
Abstract
Background
Discordance with well-known sepsis resuscitation guidelines is often attributed to rational assessments of patients at the point of care. Conversely, we sought to explore the impact of choice architecture (i.e., the environment, manner, and behavioral psychology within which options are presented and decisions are made) on decisions to prescribe guideline-discordant fluid volumes.
Design
We conducted an electronic, survey-based study using a septic shock clinical vignette. Physicians from multiple specialties and training levels at an academic tertiary-care hospital and academic safety-net hospital were randomized to distinct answer sets: control (6 fluid options), time constraint (6 fluid options with a 10-s limit to answer), or choice overload (25 fluid options). The primary outcome was discordance with Surviving Sepsis Campaign fluid resuscitation guidelines. We also measured response times and examined the relationship between each choice architecture intervention group, response time, and guideline discordance.
Results
A total of 189 of 624 (30.3%) physicians completed the survey. Time spent answering the vignette was reduced in time constraint (9.5 s, interquartile range [IQR] 7.3 s to 10.0 s, P < 0.001) and increased in choice overload (56.8 s, IQR 35.9 s to 86.7 s, P < 0.001) groups compared with control (28.3 s, IQR 20.0 s to 44.6 s). In contrast, the relative risk of guideline discordance was higher in time constraint (2.07, 1.33 to 3.23, P = 0.001) and lower in choice overload (0.75, 0.60, to 0.95, P =0.02) groups. After controlling for time spent reading the vignette, the overall odds of choosing guideline-discordant fluid volumes were reduced for every additional second spent answering the vignette (OR 0.98, 0.97, to 0.99, P < 0.001).
Conclusions
Choice architecture may affect fluid resuscitation decisions in sepsis regardless of patient conditions, warranting further investigation in real-world contexts. These effects should be considered when implementing practice guidelines.
Highlights
Time constrained clinical decision making was associated with increased proportion of guideline-discordant responses and relative risk of failure to prescribe guideline-recommended intravenous fluids using a sepsis clinical vignette.
Choice overload increased response times and was associated with decreased proportion of guideline-discordant responses and relative risk of guideline discordance.
Physician odds of choosing to prescribe guideline-discordant fluid volumes were reduced with increased deliberation as measured by response times.
Clinicians, researchers, policy makers, and administrators should consider the effect of choice architecture on clinical decision making and guideline discordance when implementing guidelines for sepsis and other acute care conditions.
Background
Sepsis is responsible for more than 250,000 deaths and 1 million hospital admissions in the United States annually, costing more than $20 billion.1,2 When managing patients with septic shock, well-known best-practice guidelines emphasize early and adequate intravenous (IV) fluid administration. Both previous 3 and recently updated 4 Surviving Sepsis Campaign (SSC) guidelines recommend administration of at least 30 mL/kg IV fluid within the first 3 h after presentation. Compliance with SSC guidelines improves survival.5,6 Despite increasing hospital and institutional mandates for sepsis guideline compliance, however, overall concordance remains generally low,5,6 including widely variable fluid resuscitation practices.7,8
For providers, the clinical decision-making processes and rationales for choosing how much fluid to prescribe are poorly understood. One possibility is that variations in fluid resuscitation are warranted due to differences in patient conditions and disease severity and that clinicians may sometimes reasonably discount current guidelines.9,10 For example, clinicians commonly prescribe less fluid volumes to patients with comorbid conditions that increase risk for developing harmful fluid overload, such as a history of heart, liver, or renal failure.7,8
While clinical judgments based on case mix certainly contribute to variability, patient and hospital factors only partially explain frequent and potentially harmful under or overresuscitation. 8 At the bedside, resuscitation targets for individual patients are often unclear. 9 In addition, although one-half of all shock patients are volume responsive (i.e., improved cardiac output), the presence of volume overload (as measured using “static” indicators of cardiac preload such as the central venous pressure or right atrial pressure) poorly predicts volume responsiveness. 11 In other words, many patients with septic shock who have clinical evidence of volume overload may still benefit from additional fluids. This highlights the challenge and complexity of prescribing optimal fluid volumes for patients with septic shock and why many patients receive either insufficient fluid volumes early in their disease course or excessive fluid volumes throughout the entirety of their hospitalization.7,8,12-14
To assist clinicians, studies have demonstrated improved patient outcomes using “dynamic” as opposed to static measures of volume responsiveness, 11 such as a passive leg raise maneuver.15,16 These bedside tests accurately predict a positive response to fluids, are very safe, and are generally easy to perform. 17 However, clinical decision making for patients with septic shock is frequently characterized by time pressure, high stakes, and diagnostic and therapeutic uncertainty. Under these conditions, clinicians often employ intuitive thinking 18 and heuristics (mental shortcuts or rules of thumb) to make rapid decisions using immediately available information.19-22
While heuristics save time and effort and are highly useful in many clinical contexts, 23 they are accurate only most of the time. Inaccuracy among heuristics is less important when the associated harms are minimal or low. However, for highly morbid conditions such as septic shock, overreliance on intuition or heuristics in real-world clinical practice may contribute to unwarranted cumulative harms even when inaccurate just a small percentage of the time. Furthermore, clinicians may also have to choose between competing heuristics. For example, instead of prescribing the guideline-recommended ≥30 mL/kg IV fluid bolus for septic shock, some clinicians may use a heuristic to prescribe ≤500 mL if patients have a history of heart failure. As such, many patients with septic shock and certain comorbidities may be systematically underresuscitated and vice versa for patients without such conditions.
Choice architecture refers to the environment, manner, and behavioral psychology within which options are presented and decisions are made. 24 These characteristics of clinical practice environments can have significant intentional or unintentional effects on clinical decision making.25,26 Although the choice architecture is often unplanned or minimally considered, many strategies to improve clinical decision making emphasize designing the choice architecture to promote more analytical, deliberative decision making over using intuition or heuristics. 27 For septic shock, more analytical thinking could improve recall of current guideline recommendations, dissuade reliance on potentially faulty gestalt and inappropriately selected heuristics, and promote clinical decision making based on patient-specific, dynamic measures predictive of fluid responsiveness. 11 Therefore, the goal of this study was to explore whether choice architecture also affects septic shock fluid resuscitation decisions, including adherence to current fluid resuscitation guidelines. Since susceptibility to choice architecture effects may vary among individuals, 28 we also explored how physician characteristics compare between intervention groups and with respect to guideline discordance.
To test our central hypothesis that fluid resuscitation decisions for patients with septic shock are malleable in relation to the choice architecture within which they are made and not just a result of patient differences, we specifically examined the use of choice architecture to induce choice overload (COL) effects. COL delays decision making by asking individuals to consider many similar options.29,30 Although sometimes associated with decision fatigue or selecting default options, 31 greater choice improves decision making, particularly when individuals feel less certain or knowledgeable, perhaps by promoting greater analytical thinking and deliberation. 32 Therefore, we predicted that physicians asked to choose between more fluid volume options for a patient with septic shock would have longer response times and reduced guideline discordance (i.e., choosing to prescribe <30 mL/kg). Conversely, we also predicted that pressuring or abridging deliberation using a time constraint (TC) would increase guideline discordance, simulating the challenge of making rapid decisions associated with managing septic shock patients.
Methods
Survey Design Overview
We invited a large, heterogenous, and randomized sample of physicians to respond to a clinical vignette describing a patient with septic shock with an incidental history of congestive heart failure and mild lower extremity swelling. As modifications to the choice architecture, we tested the impact of COL (using an expanded set of fluid volume options) and pressured or abridged deliberation (using a TC). In the primary analysis, we compared the proportion of SSC guideline-discordant responses between these intervention groups and a time-unlimited control group. Longer response time in the electronic surveys is a validated measure of more analytical or deliberative thinking, while shorter response times are associated with more intuitive thinking.33,34 Therefore, we also examined the relationship between response time and guideline discordance. Finally, in the secondary analyses, we controlled for physician characteristics and examined whether there was effect modification associated with physician predisposition for intuitive thinking35,36 and risk tolerance.37-40
Clinical Vignette
An electronic survey instrument with a single clinical vignette was developed to measure the effect of TC and COL on clinical decision making. The vignette described a common presentation of an adult patient with pneumonia and sepsis, including a medical history of coronary artery disease and congestive heart failure. The patient was hypotensive after an initial 500-mL fluid bolus over 2 h. Physicians were asked how much IV fluid they would like to prescribe over the next hour (Figure 1). Representative examples from publicly available clinical board exam questions were used to guide vignette format and structure. To limit confounding and isolate choice architecture effects from other potential biases, we used a single vignette, simplified to omit certain patient details not relevant to treatment, such as the patient’s sex. To refine the clinical vignette and survey presentation for comprehension and ease of administration, iterative pretesting and pilot testing were performed by sampling local physicians and experts from outside institutions.
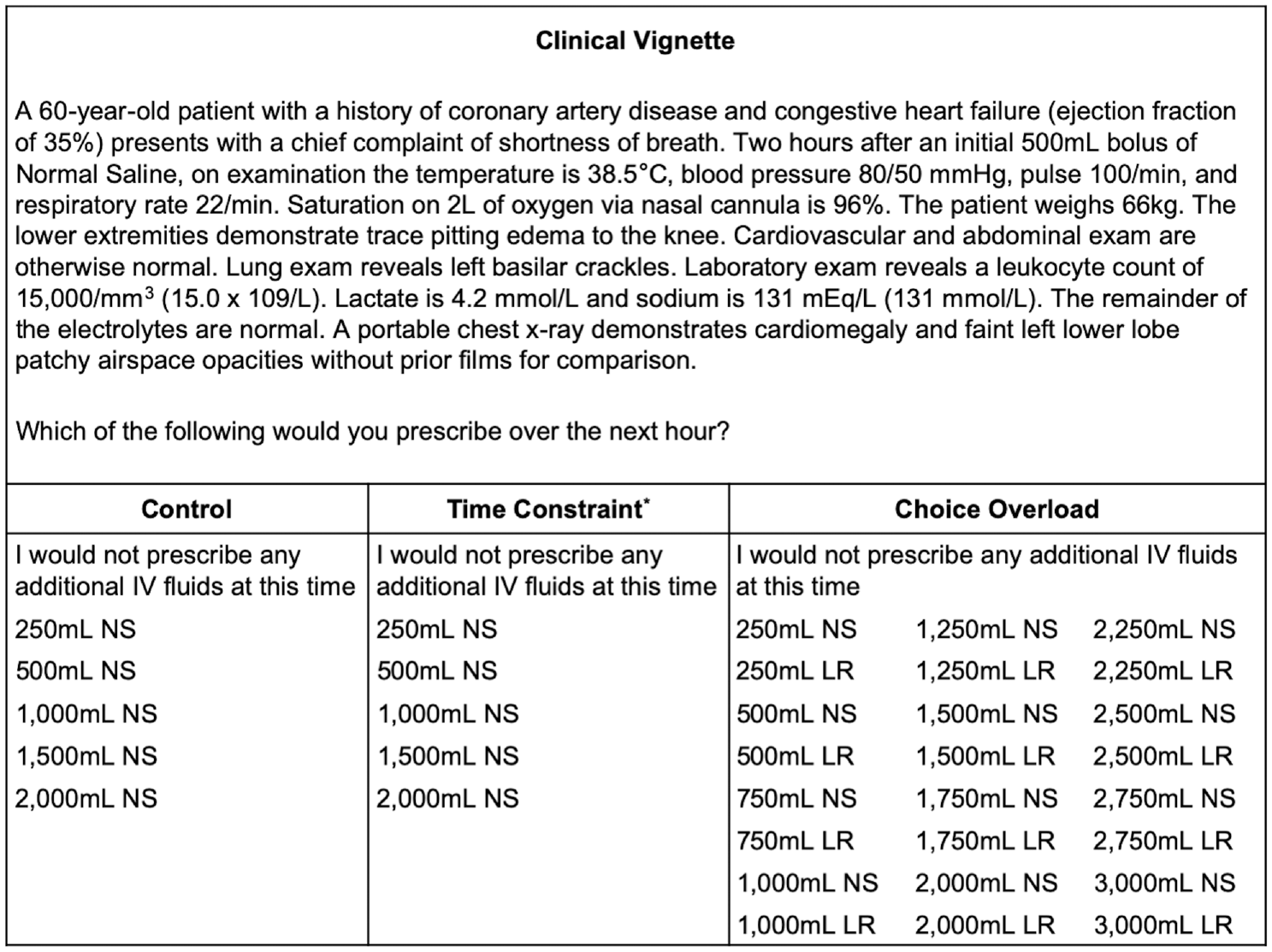
Clinical vignette and answer sets by intervention group. Respondents were randomized to each intervention in 1:1:1 fashion. All answer choices were presented in random order. NS presented as “normal saline” and LR presented as “lactated Ringer’s.” The vignette and question with answer choices were presented on separate pages. *The figure does not represent the actual display to respondents. A 10-s limit was imposed to select an answer choice. There was no limit for other groups.
Choice Architecture Intervention Groups
Three discrete answer sets were distributed to physicians in a randomized, 1:1:1 fashion. The control included 6 options for normal saline (NS) fluid volumes ranging from “I would not prescribe any fluids at this time” to 2000 mL. The TC intervention included the same 6 options, but respondents were limited to 10 s before the survey automatically advanced. If no option was selected in the allotted time, a guideline-discordant answer was scored. A warning of the upcoming TC was displayed between the vignette page and the question/answer page. The 10-s TC was determined during pretesting by measuring the average time required to read the question/answer page, which was similarly displayed after the vignette page. In-person debriefing with pretest participants confirmed there was sufficient time to read both the question and answer options. Pretest participants also confirmed pressure to make a very rapid decision when the TC was introduced. Finally, the answer set for the COL intervention was expanded from 6 to 25 options 31 with no time limit (Figure 1).
Study Population
The survey was distributed by email at 2 institutions (University of Colorado and Denver Health Medical Center) using nonprobability voluntary sampling, targeting physicians from nonsurgical specialties who manage patients with sepsis, including septic shock. The University of Colorado Hospital is a large, tertiary-care academic hospital. Denver Health Medical Center is a large, tertiary-care academic hospital that serves predominantly urban, underinsured, and immigrant populations. Physicians at both institutions hold faculty appointments at the University of Colorado School of Medicine.
The sample frame included residency/fellowship and faculty distribution lists from the departments of medicine, emergency medicine, pulmonary and critical care medicine, and cardiology at both institutions. Surveys with partial responses or response times of <5 or >500 s were excluded to account for respondents who did not read the vignette/answer choices or had an unrelated interruption while answering the vignette. Using a 2-sample means test (comparing to control) and data for response time from pilot testing (n = 43), the estimated minimum sample size was 51 in TC and 55 in COL to achieve a power of 80% with a 2-sided confidence interval of 95%. Participation was anonymous, and the Colorado Multiple Institutional Review Board approved the study protocol. A consent form was clearly displayed in the electronically distributed request to participate in the survey.
Measures and Outcomes
The primary outcome was discordance with SSC fluid resuscitation guidelines, 3 determined for the purposes of this study by choosing <1500 mL NS or lactated Ringer’s (LR) to complete an initial 30-mL/kg bolus within the first 3 h after presentation. Time spent (in seconds) responding to the clinical vignette was also measured. Total response time (total time) was defined as time spent on the vignette description page (read time) in addition to the question/answer page (answer time). For TC respondents who did not answer in the allotted time, an answer time of 10 s was assigned and added to their respective read time to provide the total time.
Other exploratory outcomes included self-reported acute stress (measured using a validated, single-item 1 = lowest to 10 = highest response-scale41,42) and confidence (measured on a 1 = not at all confident to 5 = completely confident Likert-type scale). These were measured immediately after answering the clinical vignette. Various individual characteristics may affect the susceptibility to choice architecture effects. 28 Therefore, physician characteristics were compared between intervention groups and by guideline discordance. Responses to the following validated cognitive and psychological scales were measured in randomized order and are further described in the supplementary materials: Cognitive Reflection Test35,36,43 (CRT), Jackson Personality Inventory Risk-Taking Subscale37,38,44 (JPI-RTS), and Malpractice Fear Scale37-40,45,46 (MFS). Respondents were also asked to identify the SSC 2016 initial fluid resuscitation guidelines. Demographic data included level of training, specialty, experience managing patients with septic shock in the past 90 and 365 d, age, gender, race/ethnicity, and type of device used to complete the survey (mobile or personal computer). Relative risk of a guideline-discordant answer in TC and COL compared with control was expressed as either rate ratios or hazard ratios (HRs).
Statistical Analysis
The Kruskal-Wallis test was used to examine the relationship between guideline discordance and all 3 intervention groups. To compare the proportion of guideline-discordant responses for each intervention group, 2-sided binomial probability testing was used to evaluate whether guideline discordance in TC and COL differed significantly from the control. Accordingly, the proportion of guideline-discordant responses in the control group was used as the expected distribution.
Wilcoxon–Mann-Whitney test was used to compare response times between TC or COL and control. A Bonferroni correction was used for multiple comparisons when applicable. Multivariate linear and logistic regression models were developed to analyze the relationship between response times and guideline-discordant versus guideline-concordant responses. For the linear regression model, the dependent variable was answer time, whereas the independent variable was an indicator variable for guideline discordance. Read time was included as a covariate in both linear and logistic models to control for potential differences in time spent reading the clinical vignette. Because answer time was artificially constrained in TC according to the study design, linear regressions were performed using combined data from the time-unlimited groups (COL and control) and separately from the time-limited group (TC). For the logistic regression model, guideline discordance was the dependent variable, whereas answer time was included as a continuous independent variable, controlling for read time and the intervention groups. Indicator variables for intervention group and guideline discordance were generated using dummy coding and included as the independent variables, with either the control group or a guideline-concordant option used as the reference category in respective analyses.
Based on the theoretical premise that intuitive thinking and heuristics are associated with faster decision making, 18 multiple time-to-event analyses were performed to examine the relative risk of guideline discordance based on exposure to a TC or COL. Because choice architecture effects on decision making could vary depending on response time, in addition to analyses examining the proportion of guideline-discordant responses, we also examined the risk of guideline discordance over time. The rate of choosing a guideline-discordant fluid volume option in each intervention group was calculated for every 10 s spent cumulatively reading and answering the clinical vignette (i.e., total time). The relative risk of guideline discordance in TC and COL compared with control was then determined using Mantel-Haenszel rate ratios. This analysis was then repeated using every second of answer time (as opposed to total time). Descriptions of unadjusted and adjusted Cox proportional hazards regression models; effect modification related to the CRT, JPI-RTS, and MFS; and separately developed Fine-Gray competing risk regression models are described in the supplementary materials.
The survey was developed and administered using Qualtrics (Qualtrics, Seattle, WA, USA), and statistical analyses were performed using Stata v14.2 (StataCorp, College Station, TX, USA). Variables are reported as means (s) or medians and interquartile ranges (IQRs). Test statistics are included where applicable. Model covariates are reported as HRs or odds ratios (95% confidence interval [CI], P value).
Results
Respondent Characteristics
A total of 189 of 624 (30.3%) physicians completed the survey, with an additional 65 of 624 (10%) partial responses. Seven of 189 (4%) respondents were excluded for answering the vignette in less than 5 s or more than 500 s. There was even randomization into the control (10%, n = 64), TC (9%, n = 56), and COL (10%, n = 62) groups. Partial responses (P = 0.26) or exclusions (P = 0.28) were similar between groups (Figure 2). Physician demographic dispersions were reflective of the population at both institutions; most were 31 to 40 y old (49%, n = 89) and male (59%, n = 108). Most were also attending physicians (54%, n = 98), were general internists/hospitalists (53%, n = 97), and had relatively infrequent experience managing patients with septic shock in the past 90 d (0 to 10 patients, 54%, n = 99) and 365 d (0 to 25 patients, 42%, n = 77). However, 167 of 189 (88.5%) physicians accurately identified the SSC initial fluid resuscitation guidelines. There were no significant differences between the intervention groups (Table 1).

Physician enrollment and stratification. Vignette time is equal to the sum of time spent on vignette page in addition to question and answer page. Percentages are the percentage of total distribution.
Respondent Demographic Characteristics by Choice Architecture Intervention Group

PGY = postgraduate year.
P values for overall category comparisons by intervention groups calculated using Kruskal-Wallis H test.
Includes hospital medicine/hospitalist.
Experience managing patients with septic shock.
Impact of Choice Architecture Interventions on Guideline Discordance
The distribution of fluid volumes selected for each intervention group in response to the clinical vignette are presented in the supplementary materials (Supplementary Figure S1). Using the Kruskal-Wallis test, there was a statistically significant overall relationship between choice architecture interventions and guideline discordance (χ2 = 11.49, df = 2, P = 0.003). Assuming the control group’s probability (64.1%, 51.3%, to 75.1%) using the binomial probability test, the proportion of guideline-discordant responses was increased from predicted in TC (78.6%, 65.5% to 87.6%, P = 0.03) and reduced in COL (48.4%, 36.0%, to 61.0%, P = 0.01).
Differences in Response Times between Choice Architecture Intervention Groups
Using the Wilcoxon–Mann-Whitney test, the total time was reduced in TC (45.8 s, IQR 38.3 s to 56.6 s, z = 5.076, P < 0.001) and increased in COL (94.2 s, IQR 73.0 s to 142.6 s, z = −2.80, P = 0.005) compared with control (71.5 s, IQR 52.6 s to 100.6 s; Figure 3A). Similarly, answer time was reduced in TC (9.5 s, IQR 7.3 s to 10.0 s, z = 9.29, P < 0.001) and increased in COL (56.8 s, IQR 35.9 s to 86.7 s, z = −4.721, P < 0.001) compared with control (28.3 s, IQR 20.0 s to 44.6 s; Figure 3B). The significance of the results was unchanged after Bonferroni correction for multiple comparisons. There was no difference in read time between TC (37.3 s, IQR 28.3 s to 49.5 s, z = −0.50, P = 0.62) or COL (34.5 s, IQR 22.99 s to 50.66 s, z = 0.87, P = 0.39) and control (34.6 s, IQR 28.49 s to 44.58 s).

Response time decreased with time constraint and increased with choice overload. (A) Total time represents time spent reading and answering the vignette. (B) Answer time represents time spent on the question/answer page. Differences were significant when time constraint and choice overload groups were compared with control and with each other. ▪▪▪ = median, - - - = 25th and 75th percentiles.
Relationship between Response Time and Guideline Discordance
Linear and logistic regressions were performed to further analyze the relationship between answer time and guideline discordance. In the time-unlimited groups (C and COL), the average answer time was 30.5 s (8.3 s to 52.7 s, P < 0.001) higher in COL than control after controlling for read time and guideline discordance. Controlling for read time, the average answer time among physicians who chose a guideline-discordant option was 40.3 s (−62.3 s to −18.4s , P < 0.001) lower than those who chose a guideline-concordant option. For the TC group, there was no difference in answer time between guideline-discordant or concordant responses (−0.4 s, −1.5 s to 0.9 s, P = 0.59). Overall, physician odds of choosing a guideline-discordant response were reduced for every additional second spent answering the vignette (OR 0.98, 0.97 to 0.99, P < 0.001) after controlling for read time and the type of choice architecture (C, TC, COL).
Finally, the rate of choosing a guideline-discordant option for every 10 s of total time was 0.08 (0.05 to 0.12) in the control group, 0.25 (0.14 to 0.44) in TC, and 0.07 (0.05 to 0.10) in COL. The relative risk (using rate ratios) of guideline discordance was higher in TC (2.07, 1.33 to 3.23, P = 0.001) and lower in COL (0.75, 0.60 to 0.95, P = 0.02) when compared with control. The relative risk of guideline discordance per second spent answering the vignette (i.e., answer time) was also higher in TC (21.84, 11.88 to 40.17, P < 0.001) and lower in COL (0.66, 0.52 to 0.84, P < 0.001) when compared with control. The relative risk of guideline discordance by intervention group as measured using rate ratios, unadjusted hazard ratios, and adjusted hazard ratios is summarized in Table 2. Results from Cox proportional hazard models, including measures of effect modification for the CRT, JPI-RTS, and MFS, are further described in the supplementary materials (Supplementary Table S1, Figures S2–3).
Summarized Relative Risk of Guideline Discordance by Choice Architecture Intervention Group a
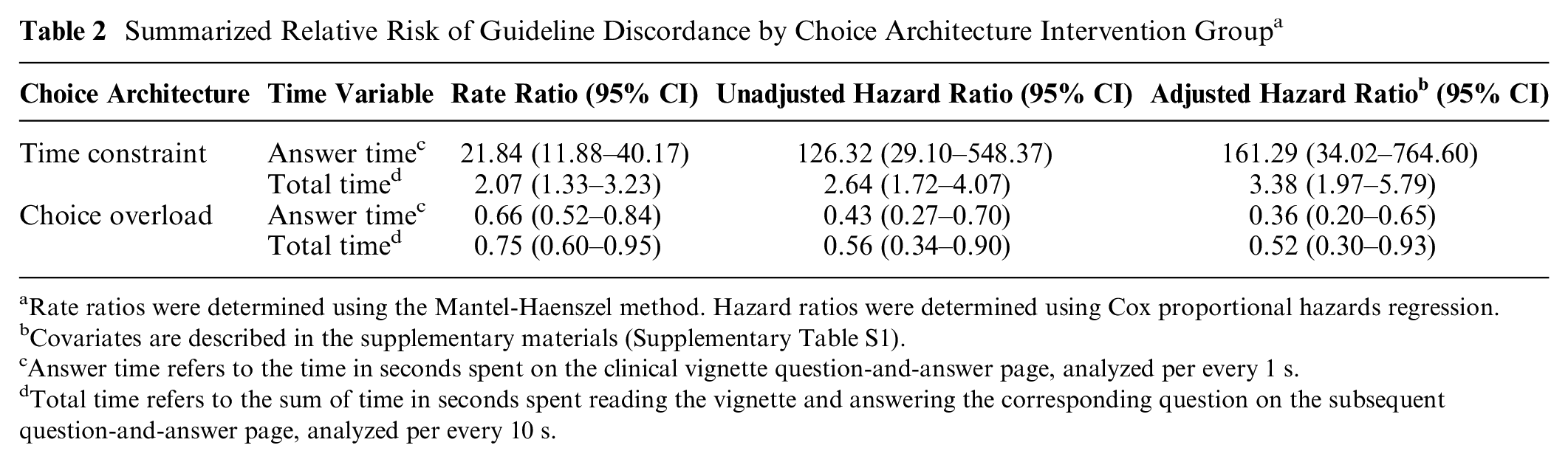
Rate ratios were determined using the Mantel-Haenszel method. Hazard ratios were determined using Cox proportional hazards regression.
Covariates are described in the supplementary materials (Supplementary Table S1).
Answer time refers to the time in seconds spent on the clinical vignette question-and-answer page, analyzed per every 1 s.
Total time refers to the sum of time in seconds spent reading the vignette and answering the corresponding question on the subsequent question-and-answer page, analyzed per every 10 s.
Exploratory Outcomes
Neither risk tolerance scale was associated with guideline discordance in any of the intervention groups, and none of the scales was associated with response time. After adjusting for intervention group, accurate identification of SSC initial fluid resuscitation guidelines conferred the largest increase in odds of having higher self-reported acute stress (OR 2.39, 1.08 to 5.30, P = 0.03), while reporting complete confidence in the selected answer to the vignette was associated with the largest decrease (OR 0.01, 0.00 to 0.06, P < 0.001; Supplementary Table S2). Stress compared with control was lowest in COL (5 v. 3.5, respectively, P = 0.002) with no significant difference in TC (4.5, IQR 3 to 6, P = 0.23; Supplementary Figure S4A). Median confidence was 3 (IQR 2–3) with no significant differences between intervention groups (H[2] = 2.75, P = 0.25; Supplementary Table S3). Mean CRT score was lower in TC among those who chose a guideline-discordant answer (1.98, s = 0.14, P = 0.007) compared with those who did not (2.42, s = 0.19; Supplementary Figure S5). Further results of measured cognitive and psychological physician characteristics are described in the supplementary materials.
Discussion
Among physicians provided unlimited time to respond to a septic shock clinical vignette, faster decision making was associated with failure to prescribe SSC-recommended IV fluid volumes (≥30 mL/kg). Presenting more fluid volume options (i.e., COL) slowed responses and decreased the overall proportion and relative risk of guideline discordance. In contrast, a TC increased the proportion and relative risk of guideline discordance. These findings persisted after controlling for time spent reading the vignette and for physician cognitive, psychological, and demographic characteristics. While examining decision making in dynamic clinical contexts has inherent challenges, these data support our central hypothesis that physicians are susceptible to choice architecture effects when prescribing fluids for patients with septic shock, warranting future investigations in real-world settings.
Findings from this study are consistent with previous studies demonstrating low SSC guideline concordance, associations between physician characteristics and variable clinical practices, and deviations in clinical decision making associated with intuitive thinking, heuristics, cognitive bias, 24 and choice architecture in other clinical conditions and circumstances.22,47 Adding to the existing literature, these findings also suggest that the response time may be an important predictor, marker, or endpoint for evaluating intentional and inadvertent choice architecture effects. There are credible theoretical constructs that support mechanisms by which response time may affect the risk of guideline discordance. Dual process theory describes intuitive (system 1) and analytical (system 2) thinking, 18 the use of which may be governed by implicit detection of response conflicts.48,49 Mechanistically, COL may have reduced guideline discordance via an associated increase in the number of potential sources of decisional conflict,49,50 as indicated by increased time spent answering the clinical vignette. For example, if a physician was intuitively cued by their existing heuristics or biases (e.g. priming 24 or availability bias 24 ) to prescribe fluid boluses of 500 mL or less for patients with a history of heart failure, the presence of a 250-mL option and both NS and LR options promotes conflict between similar choices. Pausing to resolve these conflicts may provide increased opportunity for deliberation and an analytical override that may also explain why acute stress was lower in the COL group despite having to consider more options. Paradoxically, accurate knowledge of SSC guidelines more than doubled the odds of physicians reporting higher acute stress, potentially due to conflict between opposing heuristics for managing patients with both sepsis (more fluids) and heart failure (less fluids to avoid volume overload) when guidelines are known.
In our secondary analysis of the effect modification in the COL group, the risk of guideline-concordant fluid prescribing was relatively higher among physicians with greater risk tolerance. One possible explanation is that risk-tolerant physicians at baseline may be less likely to seek out disqualifying information (e.g., search satisficing 24 ) or consider alternative choice options resulting in practice variation.37,38,51,52 The magnitude of effect of COL is therefore amplified in these individuals by promoting increased deliberation. In this study, however, risk tolerance was not associated with response time. More studies are needed to better understand the mechanism and role of risk tolerance on clinical decision making.
Conversely, a mandatory TC may have increased the risk of guideline discordance by inhibiting conflict recognition or deliberation. 53 Notably, physicians who chose a guideline-discordant answer in the TC group were more predisposed to intuitive thinking, as measured by the CRT. Questions on the CRT are designed to elicit an intuitively obvious but incorrect response. Respondents with lower CRT scores tend to accept the intuitive response more frequently. Accordingly, when pressured by a TC, guideline discordance may be partially explained by some physicians’ propensity to accept an initial intuitive response.
CRT scores were not associated with response times, however. Another possibility is that deliberation was not possible due to the TC, implying that some physicians employed the wrong heuristic or that the heuristic to prescribe less fluids to patients with a history of heart failure was more influential. In fact, it is theorized that expert decision makers rely on intuition or “gist” more often but do so more efficiently and accurately than nonexperts do. 54 It is also possible that other unmeasured cognitive processes may have occurred in response to each choice architecture intervention. For example, the inclusion of more choice options may also have functioned as a memory cue, prompting respondents to recall guideline-recommended fluid volumes. This study was not designed to evaluate the independent mechanisms by which COL affects decision making. However, reduced guideline discordance in the COL group suggests that the presentation of more choice options in some clinical contexts may help improve clinical decisions. Lastly, it is important to state that optimal resuscitation targets may be unclear, 9 and some decisions to prescribe guideline-discordant fluid volumes for patients with sepsis may be valid or reasonable. 55 This alone would not explain differences in response time and relative risk for guideline discordance observed across randomized intervention groups.
Findings from this study have potential clinical implications, particularly toward understanding unwarranted variation in clinical decision making and toward designing effective interventions, decision aids, and policies that increase guideline-adherent sepsis care. For example, only a few strategies to encourage deliberation have been rigorously tested or proven effective in clinical contexts, including cognitive forcing strategies and metacognition.56,57 Effect modification associated with physician cognitive and psychological characteristics observed in this study may help explain nonuniform susceptibility to these interventions. Moreover, intuitive thinking and heuristics can be favorable in some clinical situations. Rather than discouraging them, clinical contexts, which, in particular, are the most effective interventions to improve decision making, might augment the choice environment to promote using the right heuristic at the right time. These types of interventions are referred to as “boosts” in behavioral economics.23,58 There may also be a role for educational interventions that promote more appropriate automatic cognitive processing and decision making, such as through repeated practice and simulation. 59 Finally, modifying choice architecture to increase or decrease response time may serve as a novel framework for designing and assessing quality improvement and patient safety interventions, including in the management of sepsis and other acute care conditions. It is important to emphasize that we did not attempt to determine whether clinicians made the correct fluid resuscitation decision, since this remains up for debate,9,10 but whether they would make different decisions when exposed to varying choice architecture.
Despite adjusting for physician cognitive, psychological, and demographic characteristics, survey-based studies using clinical vignettes may not approximate real-world decision making. Accordingly, we interpret our results as proofs of concept that support further studies in actual clinical settings. Because of the study design using electronic surveys, we also were not able to further explore physicians’ rationales for their responses. For example, it is possible some physicians deliberately chose a guideline-discordant option because they disagree with the existing sepsis resuscitation guidelines or believed they did not apply to the patient described in the clinical vignette. In addition, the proportion of guideline-discordant options was lower in the COL group compared with control. If physicians were choosing at random, this could explain why guideline discordance was reduced. However, several findings suggest physicians were not randomly deciding. First, respondents in the COL group spent significantly longer than control answering the vignette. This implies that respondents at least considered the options, perhaps even more so.33,34 Furthermore, in the supplementary materials, we describe the nonnormal distribution of responses. Instead, there was clustering around certain fluid volumes in increments of 500 mL. Of the respondents, 55 of 61 (90%) chose either a 0-mL, 500-mL, 1000-mL, 1500-mL, or 2000-mL option. No respondent chose a fluid volume greater than 2000 mL, also suggesting that decisions were not random. Excluding the 6 options greater than 2000 mL that received no responses, 10 of 16 (62.5%) would meet criteria for guideline discordance, which approximates the proportion of guideline-discordant options in the control group (4/6, 67%). Lastly, while there were an equal number of options for NS or LR, the proportion of respondents choosing an LR option was significantly lower than predicted assuming a 50% probability.
Other limitations include a survey response rate that was relatively low but similar to some of the highest response rates among existing survey studies of physicians.60,61 Also, we scored a guideline-discordant response for those in the TC group who did not choose a fluid volume option in the allotted time. We selected this approach because, in clinical contexts, the ultimate outcome of not choosing a fluid volume to prescribe in a meaningful amount of time is equivalent to choosing to prescribe no fluid volumes, which would be discordant with current guidelines. However, results may have differed with a longer TC, and we cannot be sure why these individuals did not provide a response. Finally, the study was also performed at 2 nongeographically distributed academic institutions, limiting generalizability.
A major strength of our study is that we compared the effects of choice architecture interventions on both response time and guideline discordance, adding to the significance of the findings by exploring potential mechanisms of actions that are closely linked to validated theoretical constructs in cognitive psychology and behavioral economics. However, this study was meant to be a hypothesis-generating proof of concept with important implications for future studies examining real-world clinical decision making and for development of interventions or policies meant to increase guideline adherence when applicable. Further investigation of actual practice is needed to define and corroborate the mechanistic association between choice architecture, response time, deliberation versus intuitive thinking and heuristics, and clinical decision making. Qualitative companion studies are needed to examine mental models and contextual factors driving clinical decisions more closely in real-world and real-time settings. Lastly, findings from this study also warrant validation in future large-scale, geographically distributed, multi-institutional analyses.
Conclusion
TC and COL increased and decreased, respectively, the proportion and relative risk for failure to prescribe guideline-recommended IV fluids using a septic shock clinical vignette. Although physicians may sometimes rationally discount current guidelines, choice architecture may affect fluid resuscitation decisions for patients with septic shock. Clinicians, researchers, policy makers, and administrators should consider these effects when implementing guidelines for sepsis and other acute care conditions.
Supplemental Material
sj-pdf-1-mpp-10.1177_23814683221099454 – Supplemental material for The Impact of Choice Architecture on Sepsis Fluid Resuscitation Decisions: An Exploratory Survey-Based Study
Supplemental material, sj-pdf-1-mpp-10.1177_23814683221099454 for The Impact of Choice Architecture on Sepsis Fluid Resuscitation Decisions: An Exploratory Survey-Based Study by Jason N. Mansoori, Brendan J. Clark, Edward P. Havranek and Ivor S. Douglas in MDM Policy & Practice
Footnotes
Acknowledgements
We would like to thank all who participated in this study.
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support for this study was by NIH/NCATS Colorado CTSA grant No. UL1 TR002535 and NIH Clinical and Translational Research Training Program T32 grant No. HL0070-85. Contents are the authors’ sole responsibility and do not necessarily represent official NIH views. The funding agreement ensured the authors’ independence in designing the study, interpreting the data, writing, and publishing the report.
Authors’ Note
Work was performed at Denver Health Medical Center and the University of Colorado Anschutz Medical Campus. Some of the study results have been previously reported at the American Thoracic Society International Conference, San Diego, California, May 2018.
Availability of Data and Materials
The data sets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.