
Abstract
Highlights
A patient decision aid for anterior cruciate ligament injured patients was developed based on international criteria, the current literature, and patients’ experiences and suggestions on how to optimize the decision-making process about surgical and nonsurgical treatment.
The decision aid improved shared decision making by supporting the dialog between the patient and the doctor to clarify the patients’ values concerning issues important for the treatment options.
Keywords
Introduction
Increasing numbers of people are physically active as a part of a healthy lifestyle, leading to an increase in the incidence of joint injuries. 1 In Denmark, which has a population of 5.8 million people, 5000 patients annually are expected to contact the hospital with an anterior cruciate ligament (ACL) injury. 2 However, to achieve the best treatment results for patients with an ACL injury, it is important to involve patients in decision making about treatment options to provide the treatment that matches the values, lifestyle, and conditions of the individual patient.
ACL injuries are especially common among athletes, typically resulting from a valgus–internal rotation injury to the knee. The injury leads to joint instability and thus decreased activity, unsatisfactory knee function, and poor knee-related quality of life.3–5 Historically, ACL injuries have usually been treated surgically and generally accomplished arthroscopically by use of a patellar tendon or hamstring tendon autograft. 6 Rehabilitation alone has more recently been advocated as an alternative treatment to surgery, even for people with high demands on their knee function.7–9 The highly profiled randomized clinical trial by Frobell et al. 10 demonstrated that structured rehabilitation as initial treatment for an ACL injury led to a satisfactory outcome in half of the patients.
These results have led to a worldwide shift in the treatment strategy for ACL injury. Both surgical and nonsurgical treatment are today considered viable treatment options depending on the individual patient’s preferences. In such preference-sensitive decisions, the best choice depends on how the individual patient value the risks and benefits of different treatments. As the treatment decision for ACL injury today has become more preference sensitive with 2 treatment options, there is a need for better tools to support the treatment decision after an ACL injury. In particular, patient decision aids (PDAs) can support informed choice when there is more than 1 medically suitable treatment option and the treatments have different risks and benefits for individual patients.
Shared decision making (SDM) is a key component of patient-centered care and has been defined as “an approach where clinicians and patients share the best available evidence when faced with the task of making decisions, and where patients are supported to consider options, to achieve informed preferences.” 11 PDAs are often used during the process of SDM to help patients to make informed, preference-based decisions in collaboration with the health professionals by assisting the patients to construct, clarify, and communicate the personal values they associate with the different features of the options.11–13 A systematic literature review from 2017 on the use of a PDA in SDM showed a positive effect on patient-clinician communication, and patients were more satisfied with their decision. 13 Compared with usual care, people involved in decisions feel more knowledgeable, better informed, and are clearer about their values. 13 There is growing evidence that PDA may improve preference-based decisions across a wide variety of decision contexts.
The study aimed to describe a process to develop, test, and evaluate a PDA for SDM in patients with an ACL injury to support patients to choose the best treatment option in accordance with their individual values, lifestyle, and conditions.
Methods
The study was conducted at Aarhus University Hospital in Denmark from 2015 to 2019 and included a stepwise method. 14 A subsequent evaluation was based on the questionnaire “Shared Decision Making 9 questions” (SDM-Q9,15,16 and a thematic analysis of semistructured interviews with patients and doctors. 17
Setting
The Clinic of Sports Traumatology is a section of the Department of Orthopaedic Surgery at Aarhus University Hospital. The section has a highly specialized function and is organized as a close interdisciplinary collaboration between doctors, nurses, and physiotherapists, who are all experienced specialists in ACL treatment. Each year, the department treats approximately 400 children and adult patients with cruciate ligament injury. Patients are often referred from the emergency department, where they are examined in the acute phase. The patients are summoned to the Clinic of Sports Traumatology to be diagnosed and to have a treatment plan. The treatment plan could be nonsurgical treatment with a referral to physiotherapists in a specialized rehabilitation center, or the treatment plan could be a reconstruction of the ACL followed by specialized rehabilitation treatment.
Design
The design included 6 phases: preparation, reality check, developing a prototype, repeated testing, quality assessment, and implementing the new practice (Figure 1). 14 The phases included the steps from the 2013 update of the International Patient Decision Aid Standard: prototype development and the alpha and beta testing with patients and clinicians. In the following, each phase will be presented in detail.

The 6 phases included in the design. From Jørgensen MJ, Pedersen CG, Martin HM, Lomborg K. Implementation of patient involvement methods in the clinical setting: a qualitative study exploring the health professional perspective. J Eval Clin Pract. 2020;26(3):765–76.
Preparation
The study was a part of a large-scale project at Aarhus University Hospital about patient involvement of different patient groups with mandatory implementation of methods for SDM and user-led health care. 14 In the Department of Orthopaedic Surgery, we decided to focus on patients with an ACL injury and set up an interdisciplinary project team of doctors, nurses, and physiotherapists. The status of the project was presented and discussed once a month with the other health care professionals in the Clinic of Sports Traumatology.
Reality Check
A reality check was conducted to explore the patients’ perspectives on the existing care pathway. Qualitative interviews were conducted to gain an understanding of the patients’ wishes, experiences, and perceptions of their needs for information and support. A focus group interview of 6 patients was conducted before, during, and after the treatment. Further, individual in-depth interviews were performed with 20 patients at different time points in the care pathway. Using a semistructured interview guide, patients were asked to talk about their experiences, wishes, needs, and ideas. Interviews were recorded and subsequently transcribed verbatim. In the thematic analysis, the interview data were categorized into themes based on the aspects mentioned in the interview to improve the care pathway. This study focuses exclusively on the patients’ suggestions for improvement concerning the treatment decision. When undertaking thematic analysis of the interview data, the patients’ experiences and wishes could be outlined in the following 4 points:
Most patients had difficulties in choosing between treatment options on the same day they were diagnosed, and they wished to have time to consider the options.
Patients wanted a timeline for both treatment options describing the expected functional status and recommendation on when to resume different activities.
Patients suggested an overview with short- and long-term risk and benefits of the treatment options.
Patients wanted to have the possibility to further discuss treatment options with a nurse/physiotherapist/doctor.
Development of Prototype
To meet the patients’ needs for an overview of the 2 treatment options, a prototype of a PDA was created based on the current literature as well as experiences and suggestions from patients with an ACL injury on how to optimize the decision-making process. A systematic development process was carried out inspired by the 12 criteria from the International Patient Decision Aid Standards (IPDAS) described by the Ottawa Hospital Research Institute. 12 The 12 broad criteria include a systematic development process, information on options, presenting probabilities, clarifying values, patient stories, disclosing conflicts of interest, delivering decision aids on the Internet, balanced presentation of options, use of plain language, information based on scientific evidence, and established effectiveness. 12 The project team decided to involve both patients and health care professionals throughout the process of creating a PDA.
To clarify key issues enabling a treatment decision, each health care professional in the Clinic of Sports Traumatology was asked to list all possible issues that influence a patient’s treatment decision. This resulted in 39 different issues, which were subsequently categorized into 10 issues: return to sports, complications, work possibilities, cosmetic concerns, knee function, rehabilitation, stability of knee, prognosis, graft selection, and sick leave. Then, 35 random patients were asked to prioritize these 10 issues and comment on any missing issues. Finally, the top 8 prioritized issues important for the treatment decision were identified: knee stability, possible activities of daily living, sports ability, workability, clinical results, risks, rehabilitation, and sick leave (Figure 2 in the supporting information).
For each of the eight issues, the risk and benefits of surgery versus nonsurgery were described based on a literature review. When no scientific evidence was available, best practice was described. To help patients consider and clarify which features were the most important, the 2 treatment options were presented in a table with the prioritized issues presented in a balanced way (Figure 2 in the supporting information). When the literature supported the probabilities of outcome for both treatments, it was presented in an understandable way.
Repeated Testing
The prototype of the decision aid was sent to the hospital’s communication department to improve readability and graphic layout. The improved version was evaluated by 7 patients. Some patients suggested the 8 issues supplemented with a question. For example, the issue knee stability was supplemented with the following frequently asked question: How will the treatment affect the stability of the knee? Further, within the area of daily life activities, patients wanted us to add when they may use a bike and drive a car, because this was considered important information. These revisions and some additional minor corrections suggested by the patients were included in the final version of the PDA.
The process of SDM and the associated PDA were introduced to all health professionals in the Clinic of Sports Traumatology. To assess whether both the patient and the doctor were actively involved in decision making, sharing knowledge, and preferences, a member of the project team attended a minimum of 2 consultations per doctor. After the consultation, the doctor and the team member evaluated the use of SDM and the PDA. Following these evaluations, the use of the PDA was adjusted to a feasible, standardized procedure for patient involvement.
To meet the patients’ wish for reflection time before making a decision about treatment, practice was changed in our clinic, facilitating that the patient’s decision about the treatment should not be taken before at least 1 day after the patient had been diagnosed. Together with the PDA, a guide was made for the patients on how to contact the clinic about their decision. Patients could also book an appointment to obtain additional information from a nurse, physiotherapist, or doctor. The PDA was available in both a paper version given to the patients after they had reviewed it together with the doctor and an electronic version located on the clinic’s website. Along with the website version, a video showed how the PDA would be used in the clinic to prepare the patients before their consultation.
Quality Assessment
To assess the perceived benefits and effects on patient involvement, the new procedure and the associated PDA were tested quantitatively by the SDM-Q9 questionnaire15,16 and evaluated qualitatively by patients and doctors. The SDM-Q9 questionnaire was chosen to measure whether patients experienced SDM. The questionnaire had formerly been used at the Clinic of Sports Traumatology. Some patients with an ACL injury had participated in the validation process of the Danish translation of the questionnaire. 18 The scale consists of 9 questions with 6 response categories, ranging from 0 (completely disagree) to 5 (completely agree). A high score indicates a high patient perception of SDM with the doctor. 16 Two months before and 2 months after implementation of the PDA, all patients with an ACL injury were asked to fill in the questionnaires after a consultation with a doctor. Data were analysed in Stata using a t test for comparing the mean scores for each question and the total score from all patients, who had consultations before and after implementation of the PDA.
In addition to the quantitative study, semistructured interviews were conducted with 5 randomly selected patients with an ACL injury consulting different doctors to identify the patients’ experiences of SDM after the implementation of the PDA. Patients were invited to participate at their first appointment at the clinic; all patients agreed to participate. After the consultation and a brief break to reflect on the PDA and the consultation, patients were interviewed individually (lasting 20 min on average). The interviews were subsequently transcribed, analyzed, and thematically summarized. 17
After evaluation of the SDM process and the patients’ experiences, the doctors’ experiences of using the decision aid were examined. In a focus group interview, the doctors from the Clinic of Sports Traumatology were encouraged to discuss their experiences with SDM and the use of the PDA. The interview was transcribed and analyzed to identify the perceived advantages and disadvantages with the new practice.
Implementation of the New Practices
In 2021, the PDA has been used in clinical practice for 3 years and is well implemented. The project team has reviewed the PDA according to the update procedure. This included a clarification of some of the areas and a new literature search. The reviewed PDA is shown in Figure 2 in the supporting information.
Ethical Considerations
Participants were informed orally and in writing about the study, voluntary participation, confidentiality, and anonymity; participants proved written informed consent. The study was conducted in accordance with the ethical principles of the Helsinki Declaration. All data were stored securely in accordance with the regulations of the Danish Data Protection Agency. The user-involved hospital project, including the data collection procedure for the evaluation, was approved by the Danish Data Protection Agency (J.no.1-16-02-621-14).
Results
As a result of a systematic process involving patients in every step, a PDA for patients with an ACL injury was developed and implemented in the Clinic of Sports Traumatology at Aarhus University Hospital. The SDM using the PDA was tested quantitatively by the SDM-Q9 questionnaire and evaluated qualitatively by patients and doctors.
SDM-Q9 Questionnaires
The questionnaire was fulfilled by 39 patients before and 50 patients after implementation the PDA. All adult patients with an ACL injury were invited to attend, and none declined. The patients were generally young (26 years on average) with an equal gender distribution. About one third of patients had undergone previous surgery, and nearly all patients were doing sports activities 5–6 h per week before the ACL injury occurred. No statistically significant differences were found on the demographic factors between the two groups of patients included before and after implementation of the PDA (Table 1).
Demographic Data of Patients with an Anterior Cruciate Ligament Injury before and after Implementation of the Patient Decision Aid (PDA)

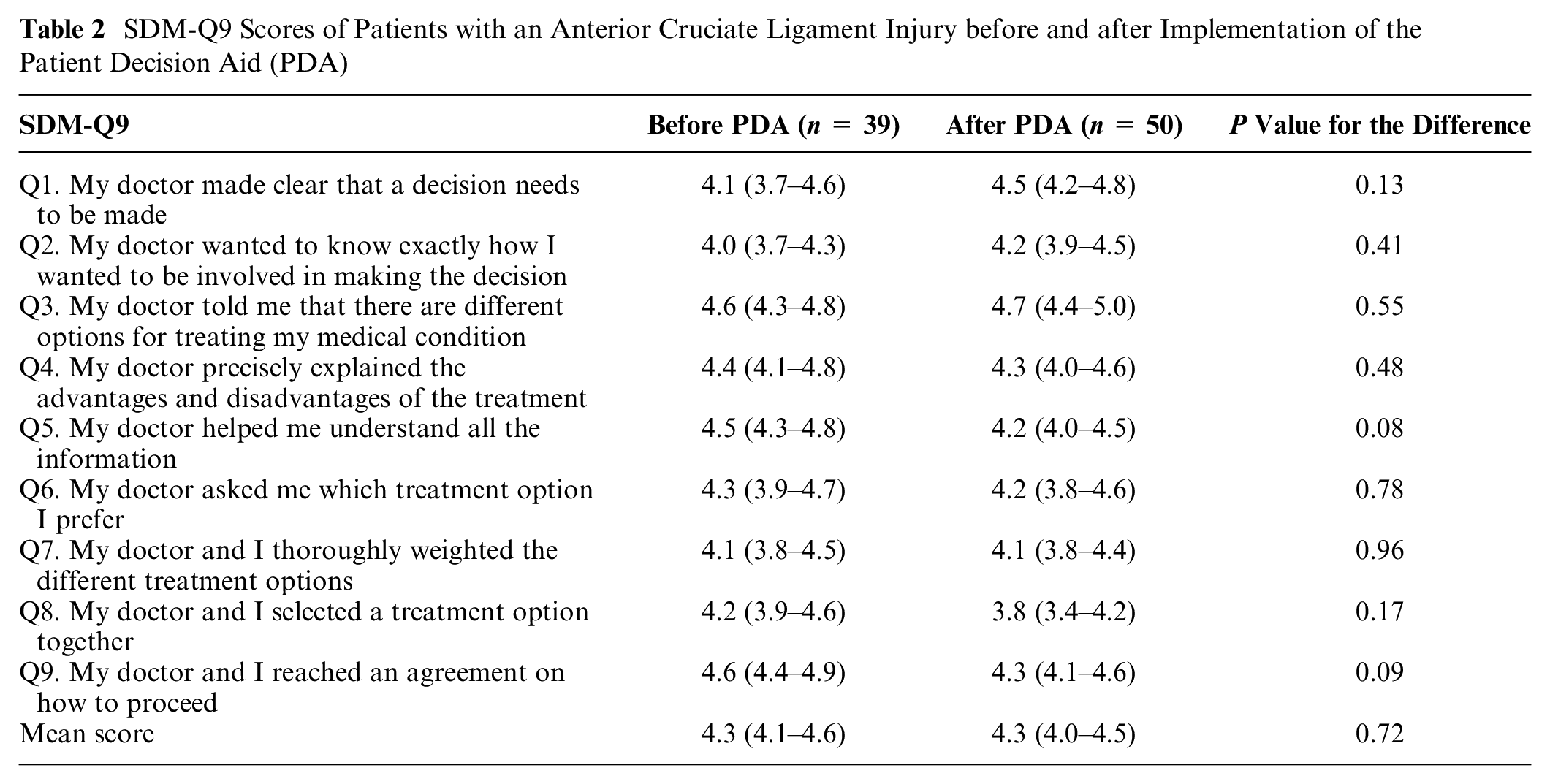
On a scale from 0 to 5, patients reported a high degree of SDM about their treatment both before (score 4.3) and after (score 4.3) implementation of the PDA (Table 2). No statically significant difference was found (P = 0.72), and the same applied to the 9 subquestions. Most patients highly agreed that “the doctor said that there were different options for the treatment” (Q3 score 4.6 before and 4.7 after), whereas the lowest, although still high, scores were found for the question “My doctor and I thoroughly weighted the different treatment options” (Q7 score 4.1 before and 4.1 after). The 2 largest differences between before and after implementation of the PDA concerned the questions “My doctor made clear that a decision needs to be made” (Q1 score 4.1 before and 4.5 after) and “My doctor and I selected a treatment option together” (Q8 score 4.2 before and 3.8 after). However, the differences were not statistically significant.
SDM-Q9 Scores of Patients with an Anterior Cruciate Ligament Injury before and after Implementation of the Patient Decision Aid (PDA)
Patient Interviews
The 5 interviewed patients evaluating the PDA were 28 years of age on average (2 women and 3 men). They were all active in sports and had a strong desire to continue with their sports. Two patients were unaware of the extent of their injury before the consultation. None of the 5 patients were prepared for a treatment decision to be made at the consultation. However, the interviews revealed that the patients perceived the PDA as a supportive and useful tool, as illustrated by these quotes from the interviews: “The PDA gives a very good overview of the 2 options, so it is easier to decide what to do,” “It [the PDA] showed what the pluses and minuses were for the two treatments,” “If only the doctor had informed me, then I think I would have forgotten most of it. So, it was really nice to take it [the PDA] home and read it again.” Furthermore, a patient expressed, “What the doctor said was also part of the decision aid. It is all very well connected.” The patients experienced that both treatment options were presented equally and also if the patient had already decided on the choice of treatment. “It was clear to me that I wanted to have surgery; I was explained about the options, but I was listened to, and I was not pressured to do just rehabilitation.” Patients experienced a high degree of autonomy, feeling that they were supported in their decision rather than being persuaded to make a particular choice.
The principles of SDM were practiced. The patients’ individual preferences of importance for the decision were discussed, and the patients felt they were involved in the decision. One patient stated, “I thought I was given some good information, and the doctor was very interested in my life, what I am doing and what sport I practice.” Another patient said, “The doctor asked me a lot. He asked what I wanted to be, whether I wanted to be a craftsman or something.” “The doctor explained very well what the decision aid was about. After our discussion, it became clear what was best for me now.” Patients felt their preferences and needs were heard: “I was very much listened to, and was asked about what I was doing, my work and my physical activity. Also, how my knee function is now, what I can and can’t do, and how loose it [the knee] is. It was a good dialogue.”
Doctor Interview
Overall, the doctors in the focus group interview expressed satisfaction with use of the PDA. They found it well implemented in the clinic and as an integral part of their consultation. The PDA was perceived as a tool that was deliberately used to guide the dialogue, clarifying the patient’s preferences, desires, and needs. “Apart from the fact that the dialogue is more systematically structured, the patient’s involvement and focus are extra clear when sitting together going through the PDA.”
Doctors reported that they used the PDA as a tool for SDM: “The decision aid is a helpful tool in the conversation. When using it, the patients are more engaged, and they are encouraged to be involved.” To guide the patient to make a decision, an introduction to the PDA was important: “An intro is needed to use the decision aid, but after this, the patient will automatically be involved in sharing information.” Reflection time was viewed as a new positive approach by the doctors; hence, the patient’s decision was made on an informed basis. “Some patients are almost shocked, when they are diagnosed, and then they do not remember much from the conversation.”
The doctors found it challenging when the choice of treatment was obvious for both the patient and the doctor, for example, surgery. In these cases, some of the doctors felt that they informed too much about an apparently irrelevant treatment. However, another doctor said, “I have seen patients who have changed their attitude about treatment, because they have gone through all the information again at home, and have become aware of some advantages or disadvantages, they did not know about.” One concern in the beginning was whether the consultation would take longer and cause a delay. However, this was not the case. One doctor expressed it like this: “I do not see there is a time problem, but rather an advantage of the systematic dialogue.”
Discussion
Using a stepwise approach, we systematically developed a PDA for SDM in patients with an ACL injury based on the IPDAS criteria. The results of the patients’ perceptions of SDM by the SDM-Q9 questionnaire showed a high level of SDM both before and after implementation of the PDA. The results from the patient interviews showed that patients experienced the PDA as a very useful tool to assist SDM. The doctors reported that the PDA improved SDM by supporting the dialogue to clarify the patients’ values concerning issues relevant for choice of treatment.
In the interviews, patients expressed that they were very satisfied with the PDA to support SDM; however, a statistically significant difference in the SDM-Q9 score before and after implementation of the PDA was not found. There may be several reasons for this finding. Looking into the subquestions in the SDM-Q9 for the 2 largest (although not statically significant) differences between before and after implementation of the PDA, it seems that the doctors are more aware of explaining to the patients that a decision needs to be made (Q1 score 4.1 before and 4.5 after implementation). On the other hand, after the PDA implementation, patients scored lower in the question of whether they decided the treatment together with the doctor (Q5 score 4.2 before and 3.8 after implementation). This may be explained by the introduction of reflection time. After the consultation, patients were told to contact the clinic about their treatment decision, which may have made some patients feel that they made the decision themselves and not together with the doctor. This could indicate a tendency for patients to feel that they had more control over the treatment decision and thus experienced a higher degree of autonomy.
In addition, the limited sample size of 39 and 50 patients before and after PDA implementation, respectively, could explain the lack of a significant difference between scores before and after PDA implementation. However, a difference less than 0.01 on a scale from 1 to 5 would not be clinically relevant, so whether the study was performed on a larger population, a significant result would probably be of minor importance. The most likely explanation of no difference is that the patients before the implementation of the PDA generally already agreed that they were involved in the decision about treatment, as shown by the high score of 4.3. The maximum score of 5 was seen in 452 answers (57%). This distribution provides a considerable ceiling effect without much variance, which reduces the possibility of studying differences. The ceiling effect is a known problem in SDM self-reported instruments.18,19 To adjust for a high ceiling effect, the response categories in the SDM-Q9 questionnaire were changed in 2010 from a 4-point to a 6-point rating scale with more extreme categories (completely disagree to completely agree) 16 . However, the ceiling effect might still be a problem. In a systematic review of studies published between 2010 and 2015 evaluating interventions to facilitate SDM, no significant changes were detected between the intervention and control groups in 4 of the 5 included studies; the identified difference in the fifth study was “small in size.” 20 As mentioned in this review, this could mean that SDM tools have deficiencies in the sensitivity to measure changes. Future studies are needed to investigate whether quantitative methods with a smaller ceiling effect could be used to test the effect of PDAs without any ceiling effect.
One of the strengths of this study was the involvement of patients and colleagues throughout the process. Using an iterative, stepwise method, the patients identified the problems they experienced concerning treatment decisions, they suggested improvements in the alpha version, evaluated all new initiatives, and tested the beta version of the PDA. 11
In fact, our process mirrored a newly described framework of user-centered design that was developed based on a previous systematic review of the design and development of 348 personal health tools. 20 The framework consists of 11 items (UCD-11) to quantitatively document user involvement in the development processes of patient-centered tools. 20 The first 5 items ask whether or not potential end users were involved in at least in 1 of the steps: 1) involved to help understand their needs, 2) involved in developing a prototype, 3) involved in evaluating prototypes or a final version of the tool, 4) asked about their opinions of the tool, and 5) observed using the tool. The next 2 items ask whether the developing process 6) had 3 or more iterative cycles and 7) if changes between at least 1 cycle were reported. The last 4 items question whether health professionals 8) were asked their opinion, 9) were consulted before the first prototype was developed, 10) were consulted between initial and final prototypes, and 11) whether an expert panel was involved. While this framework did not exist when we developed and tested our PDA, our process met all 11 UCD criteria, as described in the 8 phases in the “Methods” section.
Another strength is that the patients were interviewed immediately after the consultation following a short period of reflection and that different doctors were involved. However, as a result, the study only reflects patients’ short-term experiences and not what increased involvement in decision making means on a long-term basis. In addition, the patients were very committed and willing to participate, when invited. From information posters in the waiting room, they were prepared to be asked for participation by the staff. No one declined participation, which may also be explained by the relatively young and not seriously ill population. All health professionals in the clinic were engaged during the process by disseminating and evaluating methods and accompanying tools for SDM.
This study had several limitations. First, the project team conducted the interviews in their own department. This might have resulted in interviews being more positive and that the analysis did not sufficiently include negative aspects. Although the interviewers were committed to focusing on what could be improved, patients were generally very satisfied.
Further, one can question whether the 5 interviewed patients were representative of the relevant patient population. However, they were randomly selected and corresponded to the mean age and gender distribution in the SDM-Q9 study. We also interviewed different patients before and after development and implementation of PDA, which could support that patients’ suggestions for improvements regarding treatment decisions were expressions of the general wishes of patients with an ACL injury, as the PDA was evaluated positively by other patients in the same situation.
The developed PDA for patients with an ACL injury may positively affect the patient-doctor interaction and individual treatment decisions. The use of PDA will improve patients’ responsibility for the treatment and outcome of their knee condition, resulting in greater patient autonomy. Future research is needed that investigates the impact of a PDA in patients with an ACL injury regarding treatment choices and whether PDA improves the clinical outcome at follow-up.
The PDA can be disseminated nationally and internationally for a broader approach to increase SDM. With the successful development of a PDA for a knee condition with more than 1 relevant treatment option, a similar process could be conducted for other knee or joint conditions.
Conclusion
A systematic process involving patients with an ACL injury was successfully used to develop a PDA for SDM based on the IPDAS criteria. The SDM-Q9 questionnaire was not very suitable for this study to identify differences before and after implementation of the PDA, presumably because of a ceiling effect, with patients being very satisfied both before and after implementation of the PDA. The patients expressed in interviews that they found the PDA very supportive and useful when they had to make a treatment decision. The introduced reflection time was important for some patients. The doctors found that the PDA improved SDM by supporting the dialogue to clarify the patients’ preferences and values concerning issues important for the treatment options. Future studies are needed to investigate whether implementation of the PDA has an impact on ACL patients’ treatment choices and outcome.
Supplemental Material
sj-docx-1-mpp-10.1177_23814683221081434 – Supplemental material for Development and Test of a Decision Aid for Shared Decision Making in Patients with Anterior Cruciate Ligament Injury
Supplemental material, sj-docx-1-mpp-10.1177_23814683221081434 for Development and Test of a Decision Aid for Shared Decision Making in Patients with Anterior Cruciate Ligament Injury by Hanne Mainz, Lone Frandsen, Martin Lind, Peter Fauno and Kirsten Lomborg in MDM Policy & Practice
Supplemental Material
sj-pdf-2-mpp-10.1177_23814683221081434 – Supplemental material for Development and Test of a Decision Aid for Shared Decision Making in Patients with Anterior Cruciate Ligament Injury
Supplemental material, sj-pdf-2-mpp-10.1177_23814683221081434 for Development and Test of a Decision Aid for Shared Decision Making in Patients with Anterior Cruciate Ligament Injury by Hanne Mainz, Lone Frandsen, Martin Lind, Peter Fauno and Kirsten Lomborg in MDM Policy & Practice
Footnotes
Acknowledgements
We are grateful to all patients who participated in this study. We would also like to thank our colleagues at the Department of Orthopaedic Surgery, Clinic of Sports Traumatology, for their commitment to and support of the project. Finally, we want to thank our colleagues at the Centre for Research in Patient Involvement, Aarhus University Hospital, Denmark, for good inspiration and encouragement.
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support for this study was provided entirely by Health Research Fund of Central Denmark Region and Department of Clinical Medicine, Aarhus University, Denmark. The funding agreement ensured the authors’ independence in designing the study, interpreting the data, writing, and publishing the report.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.