
Abstract
Introduction
The US Preventive Services Task Force (USPSTF) recommends mammography screening biennially for women aged 50 to 74 years but states that the current evidence is insufficient to assess the balance of benefits and harms of screening mammography in women ≥75 years since none of the randomized trials of mammography screening included these women. 1 The USPSTF further notes that if mammography is offered to women ≥75 they should be made aware of the uncertainty of benefit (e.g., chance of avoiding breast cancer death) and potential for harm (e.g., chance of false positive tests, overdiagnosis).1,2 Overdiagnosis is a particularly concerning harm of mammography screening since 30% of screen-detected tumors in women ≥70 are estimated to be overdiagnosed. 2 The risk of overdiagnosis rises with age due to increasing competing mortality risks and because breast cancer tends to have more favorable biologic characteristics with age.2,3 Yet many women ≥75 are offered screening without being informed of possible harm. 4 Primary care clinicians (herein referred to as PCPs) may offer screening to women ≥75 because they find shared decision making around mammography challenging due to patient enthusiasm for screening, because overdiagnosis is a difficult concept to explain, and because these discussions may lead to uncomfortable conversations about patient life expectancy.4–10
To help inform women ≥75 of the potential benefits and harms of mammography screening, investigators developed a workbook decision aid (DA) for women ≥75. 11 The DA, written at a sixth-grade reading level, includes information on breast cancer risk factors, life expectancy, competing mortality risks, screening outcomes, and a values clarification exercise. It is available at ePrognosis.ucsf.edu 12 and was found in an independent review to be high quality based on International Patient DA Standards (IPDAS). 13 In a PCP-clustered randomized clinical trial (RCT) that included 546 women ≥75 seen by 137 PCPs practicing at 1 of 11 primary care practices (9 in Massachusetts [MA], 2 in North Carolina [NC]), receipt of the DA in the waiting room before a primary care visit led to women ≥75 being more knowledgeable of mammography’s benefits and harms and to 9% fewer women being screened; 87% of women found the DA helpful. 14
The next step is to prepare for DA implementation in practice. Prior work suggests that clinicians need to recognize the usefulness of a DA for it to be successfully implemented and the IPDAS recommends field testing DAs with clinicians.15–17 Despite this, few trials of patient DAs have assessed clinicians’ perspectives. 18 Therefore, to inform implementation of the mammography DA, we aimed to learn PCPs’ perspectives on the DA’s acceptability (palatability), appropriateness (fit), and feasibility (workability). These three outcomes are included in Proctor and colleagues’ Implementation Outcomes Framework and may be assessed to inform how best to introduce a DA into practice. 19
Methods
Design and Setting
PCPs (physicians and nurse practitioners) whose patients had participated in the mammography DA’s RCT were sent a web-based questionnaire to learn their perspectives on the DA’s acceptability, appropriateness, and feasibility, regardless of their randomization arm. The DA trial has been described previously.14,20 In brief, 546 women 75 to 89 years old from 137 different PCPs practicing at 1 of 11 primary care practices participated. Nine practices were in the Boston area (one academic internal medicine, one academic geriatrics, seven community-based practices from two different health systems) and two were in Chapel Hill, NC (one academic internal medicine and one academic family medicine practice); see Supplementary Table A1 for more details on each practice. Once the first patient for each PCP agreed to participate, the PCP was randomized to the intervention (the DA) or to the control arm (a home safety pamphlet). All subsequent patients for each PCP received the same intervention. On average, four patients participated for each PCP. Before a visit, PCPs were sent a copy of the DA or home safety pamphlet and were informed that their patients would be coming in early to read study materials. So as not to add burden, PCPs were not required to complete any training to use the DA; however, PCPs randomized to the intervention were sent a link to a 3-minute video example of a PCP discussing mammography with an older woman plus five PowerPoint slides on shared decision making around mammography screening with women ≥75 in case some PCPs sought training; four PCPs accessed this information during the trial. To avoid contamination of the trial, PCPs were asked to participate from May 2017 to October 2018 after all of a PCP’s patients that participated in the trial had completed follow-up (18 months). The study was institutional review board approved at the Beth Israel Deaconess and University of North Carolina Medical Centers.
This research was supported by NIH/NCI (R01CA181357).
For the current study, PCPs were sent a link to a secure web-based questionnaire; a link to the DA was embedded within the questionnaire and the DA was also sent as an attachment to the study’s invitation email. Three attempts were made to reach PCPs by email. PCPs that did not respond were mailed a paper copy of the questionnaire with a stamped and preaddressed envelope for return. PCPs were informed that their participation was voluntary, their decision to participate would not affect their employment, they could withdraw any time, their responses were confidential, and that a $50 check would be mailed to them in appreciation for participating. PCPs were required to indicate their consent before completing the questionnaire. Current contact information was sought for PCPs who had moved or retired.
Data Collection
The study questionnaire, available in the appendix (see Supplemental Material), asked PCPs about the importance of shared decision making around mammography screening with women ≥75 (from strongly agree to strongly disagree on a 5-point Likert-type scale), whether they engage women ≥75 in shared decision making around mammography screening, and whether these women want to participate in shared decision making (from never to always on 5-point Likert-type scales). Then PCPs were asked about the DA’s acceptability including its length, amount of information, balance, and format; whether its use would be appropriate including whether it would help their patients make more informed and/or value-laden decisions; whether they would recommend it; and whether they had other good resources to support this decision. PCPs were also asked about the DA’s feasibility including whether it would save them time, whether they would need training to use the DA, who should deliver the DA, and the feasibility of different delivery methods (e.g., how likely would it be for a medical assistant to give the patient the DA before a visit on a 5-point Likert-type scale from very unlikely to very likely). PCPs were also asked open-ended questions on how to improve the DA and barriers and facilitators to its use. Moreover, PCPs were asked their specialty, years in practice, number of patients seen weekly, time allotted for a physical, and their sociodemographics. The questionnaire was cognitively tested by seven PCPs not included in the trial.
Analysis
The study was designed to be descriptive. However, in exploratory analyses, chi-square tests were used to examine whether PCPs’ perspectives on the DA varied by their trial randomization assignment and/or by their region since among patients the DA’s effects varied by region. 14 In MA, where 72% of women in the control arm were screened during follow-up, DA use was associated with 13% fewer women being screened. In NC, where only 22% of women in the control arm were screened during follow-up, DA use was associated with 2% more women being screened. 14
We also conducted a qualitative content analysis to identify themes in PCPs’ open-ended comments about the DA.21,22 Two investigators (MAS, MK) independently reviewed all of participants’ open-ended comments to identify themes; code discrepancies were resolved by consensus. 23 Direct quotes and participants’ study identification numbers were used to illustrate themes. This research was supported by NIH/NCI (R01CA181357). The funding source had no role in the study.
Results
Figure 1 demonstrates PCP recruitment flow. Of 137 PCPs whose patients participated in the DA trial, 13 had changed practices, 3 had retired (contact information could not be found for 1 PCP who had moved and 1 who had retired), 2 had left primary care before the PCP survey was initiated, 37 never responded to attempts at contact, 2 declined participation, and 80 participated (78 completed the web-based questionnaire and 2 completed a paper questionnaire). PCP participants were similar to nonparticipants with regard to site, race, number of women ≥75 in their panel, and randomization assignment; however, participants were more likely to be female and non-Hispanic White (Supplementary Table A2). Of the 80 PCP participants, 52 (65%) were female, 35 (44%) had been randomized to the trial’s DA arm, 55 (69%) practiced in an academic setting, and 24 (30%) practiced in NC (Table 1). There were no significant differences in PCP characteristics by randomization arm (Supplementary Table A3). PCPs from NC were more likely to be family medicine physicians, to have less time allotted for Medicare Annuals, and were more likely to report using DAs in practice than MA PCPs (Table 1). In exploratory analyses, there were no significant differences in PCPs’ perspectives of the DA by randomization arm; however, differences were found by region. Therefore, in the tables, outcomes are presented overall and by region.
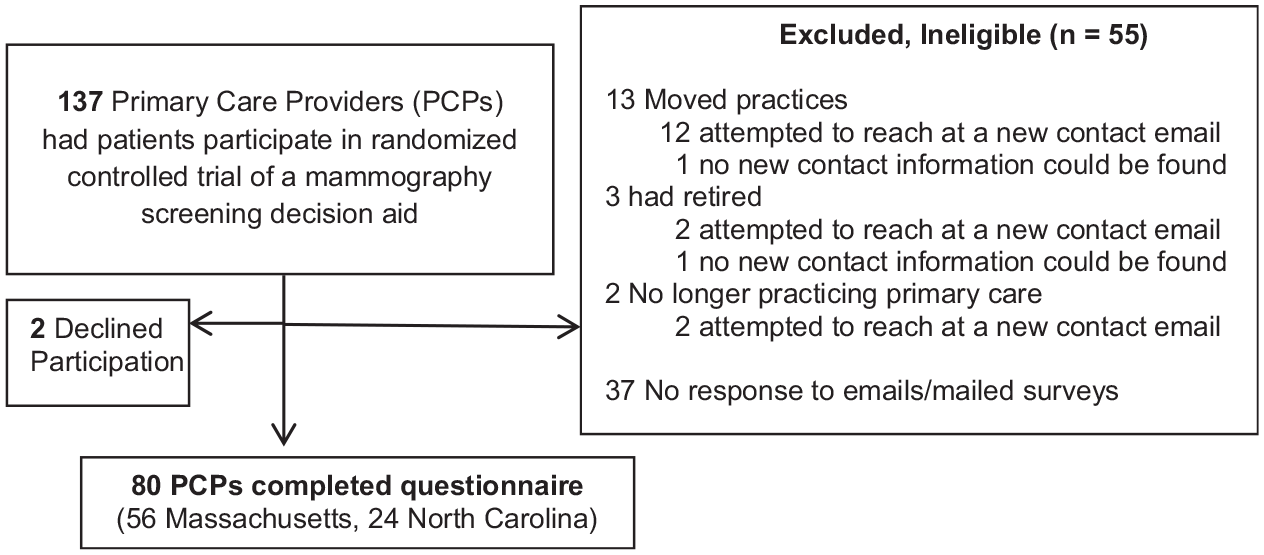
Participant study flow diagram
Primary Care Provider (PCP) Sample Characteristics Overall and by Region (n = 80)
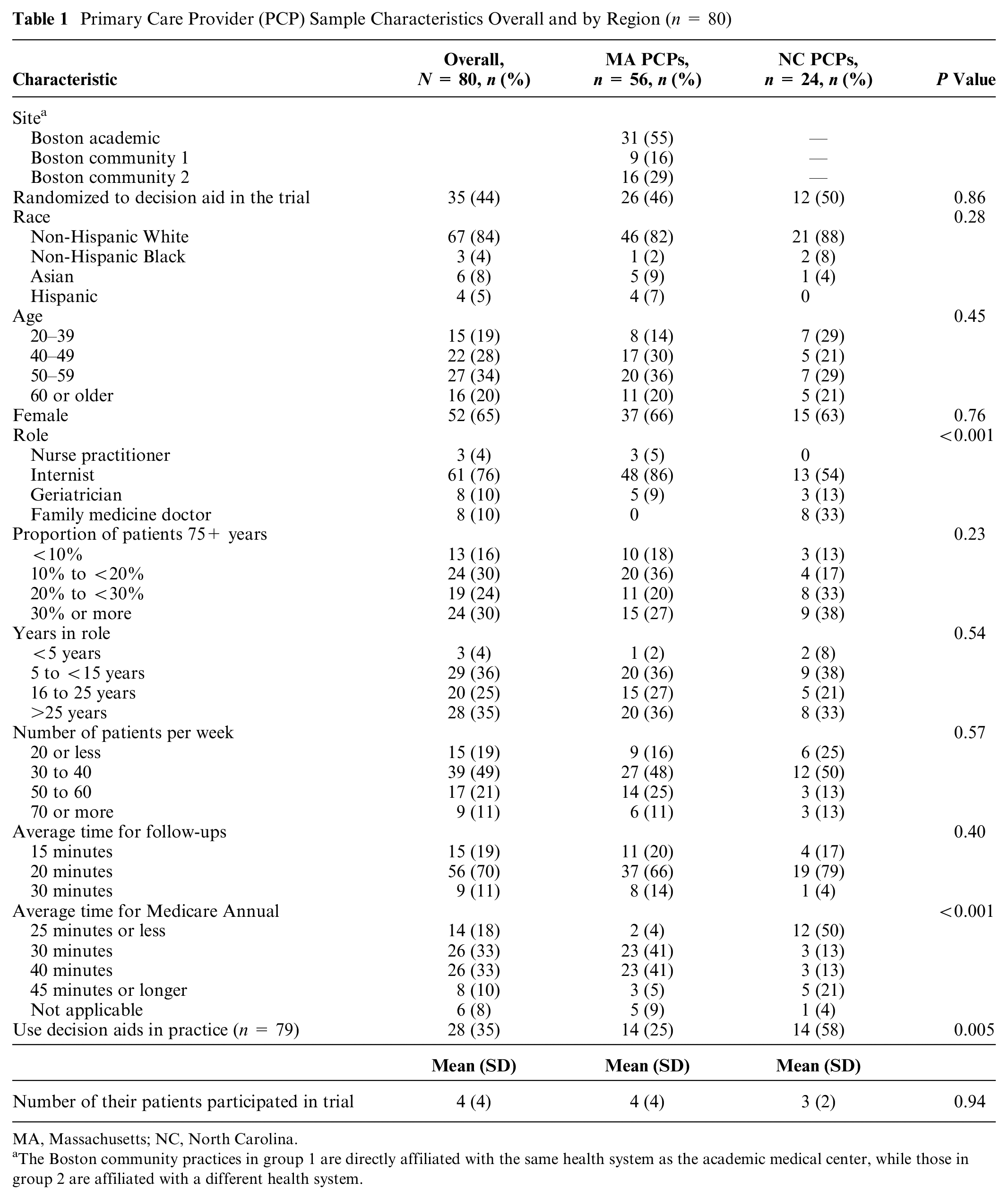
MA, Massachusetts; NC, North Carolina.
The Boston community practices in group 1 are directly affiliated with the same health system as the academic medical center, while those in group 2 are affiliated with a different health system.
Shared Decision Making
The majority (n = 69, 86%) of PCPs thought that involving women ≥75 in shared decision making around mammography screening was extremely or very important (Table 2); however, PCPs in NC tended to be less likely to feel this way (75% in NC v. 91% in MA, P = 0.03). Most PCPs (n = 49, 61%) reported that they engaged women ≥75 years in shared decision making around mammography screening frequently, 54 (68%) felt that women ≥75 years wanted to participate in shared decision making around mammography screening, and 60 (75%) felt that doing so would result in fewer women choosing screening.
Primary Care Clinicians’ Perspectives on Shared Decision Making on Mammography Screening With Women 75+ Overall and by Region (N = 80)

MA, Massachusetts; NC, North Carolina; PCP, primary care physician.
Acceptability
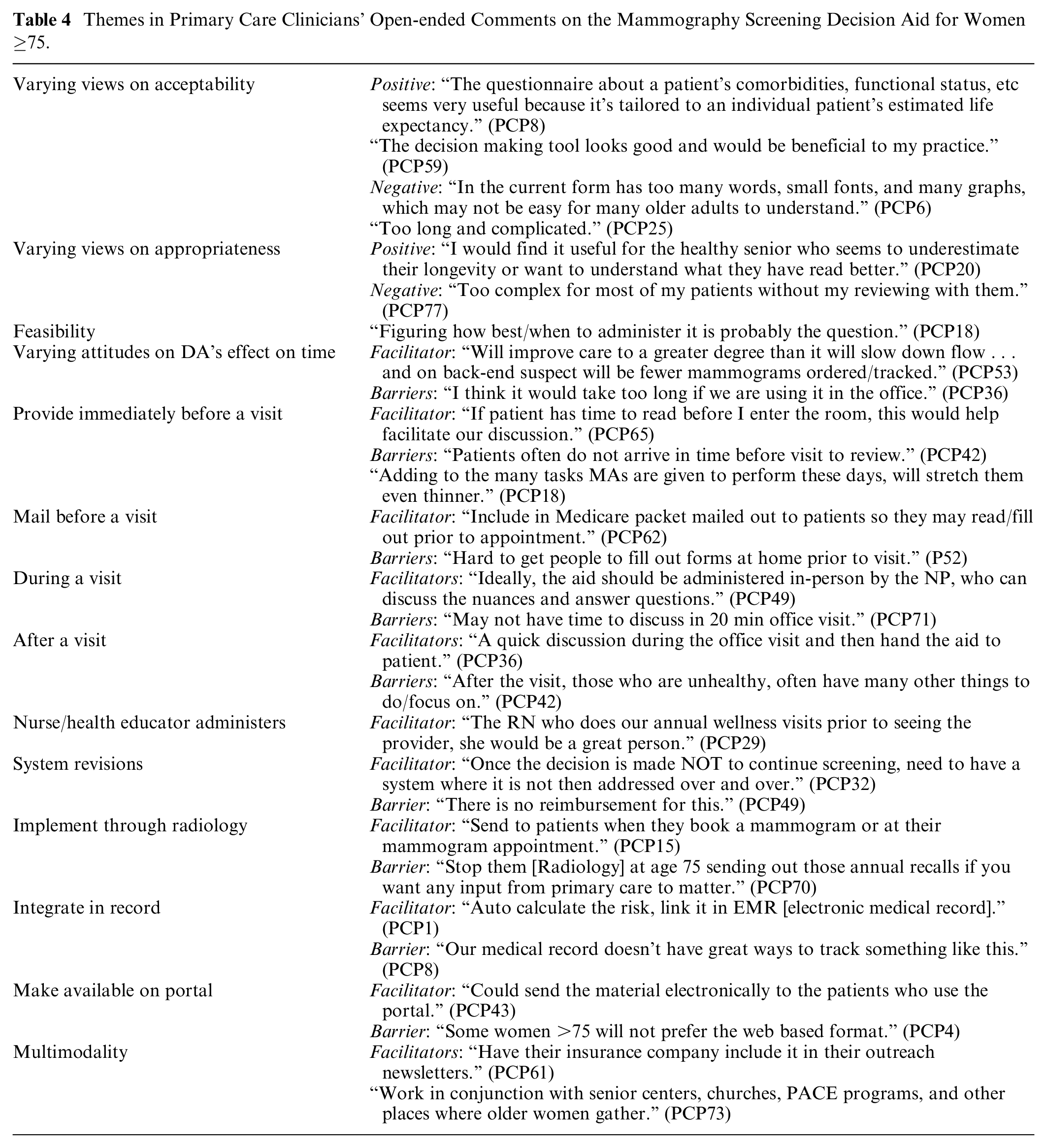
Half of PCPs thought the amount of information in the DA was just right while the other half thought there was too much information (Table 3). Forty-eight (60%) felt that the DA was too long; however, PCPs did not agree on what information could be cut from the DA (Supplementary Table A4). PCPs preferred that the DA be available on paper (n = 25, 31%) or both on paper and the web (n = 49, 61%). While 50 PCPs (63%) thought the DA presented a balanced view of mammography’s benefits and harms, 22 (28%) thought it was slanted away from mammography and 7 (9%) thought it was slanted toward mammography. In open-ended comments, PCPs noted that the DA “seemed appropriately slanted, by presenting data that there is a high risk a false positives and a low chance of saving a life” (PCP8). Overall, PCPs perceptions of the DA’s acceptability varied (Table 4). Some viewed the DA positively, “Love it! Can’t wait to use it” (PCP38), while others felt it was “too complex” (PCP17), that “it could be made more visually attractive” (PCP71), and that there should be a “longer v. a shorter version” (PCP12) based on patient literacy.
Primary Care Clinicians’ Perspectives on the Decision Aid Overall and by Region (N = 80)

DA, decision aid; MA, Massachusetts; NC, North Carolina; PCP, primary care physician.
Themes in Primary Care Clinicians’ Open-ended Comments on the Mammography Screening Decision Aid for Women ≥75.
Appropriateness
The majority of PCPs (70/79, 89%) thought the DA was somewhat or very helpful, that it would complement their usual approach to mammography screening in older women (n = 68, 85%), and that using the DA would result in their patients making more informed (n = 70, 88%) and value-laden screening decisions (n = 65, 81%; Table 3). Fifty-five PCPs (70%) would recommend the DA. Few (8%, 6/74) felt that they had other good resources to support this decision. In open-ended comments PCPs views varied on the DA’s appropriateness (Table 4). For example, some felt the DA “would be most helpful for those with poor health but who nonetheless continue to wish to have screening” (PCP42), while others wanted data to “show me that women want this” (PCP74).
Feasibility
Few PCPs (n = 13, 16%) thought DA use would save them time. Eighteen (23%) thought that PCPs should primarily be responsible for delivering the DA, while others thought that medical assistants (n = 34, 43%), nurses (n = 13, 16%), or other staff (n = 14, 18%) should deliver the DA (Table 3). In order of likelihood of success, PCPs felt that it would be most likely for a medical assistant to deliver the DA to patients before a visit, then for patients to be mailed the DA before a visit, and then for a health educator to review the DA with a patient. Few PCPs thought that it would be likely for a practice assistant to give the DA to patients after a visit, that it be sent through a patient portal, or that patients receive it from breast imaging. About half of PCPs (49%) thought it would be feasible for PCPs to deliver the DA during a visit.
In open-ended comments (Table 4) PCPs noted that “the best approach is to hand the aid out in advance of an appointment” (PCP10) via “email or on the web or to provide in the waiting room” (PCP26) especially with “Medicare wellness” forms (PCP7). PCPs also noted the need for systems to record when the DA was used and to document a patient’s decision to stop screening, “Once the decision is made not to continue screening, need to have a system where it is not then addressed over and over” (PCP32). PCPs also noted barriers to using the DA including competing demands during a visit, the “overwhelming number of prevention issues that need to be discussed during a wellness visit” (PCP25), that it can be challenging to get patients to complete forms prior to a visit, and that some women ≥75 may have trouble accessing a patient portal. PCPs also expressed concern that the DA would lead to more patient phone calls or emails. However, several PCPs felt that the DA “could help facilitate discussion and speed up decision making” (PCP29). Others noted that discussing the DA “was worth it” (PCP38) and “may save them time on the back end because of having fewer mammograms to track” (PCP53). Most PCPs (n = 50, 71%) reported that they would like some training to use the DA and generally preferred a presentation or to watch a video rather than reading an instructional workbook.
Discussion
PCPs from primary care practices in Massachusetts and North Carolina felt that shared decision making around mammography screening with women ≥75 years is important, valued by patients, and leads to older women making more informed screening decisions. PCPs also reported that use of a mammography screening DA for women ≥75 was appropriate in that it would help their patients make more informed and value-laden decisions and felt that they had few other resources to support these decisions. However, they varied on its acceptability, as many PCPs felt the DA was too long and would be challenging for women with low health literacy to use. Last, while PCPs felt that several methods for delivering the DA would be feasible, most felt that it would be most feasible for medical assistants to give patients the DA before a visit. Most PCPs also wanted some training to use the DA.
While DAs have been shown to increase patient knowledge and involvement in medical decisions, their use in practice is low. 24 Cited barriers include limited time during visits, competing agendas, difficulty identifying appropriate patients for use of a specific DA, low health literacy, and a perceived lack of need.25–30 PCPs in our study noted some of these barriers in planning for implementation of our DA, but still most felt that it would be helpful to their patients, would help their patients make higher quality screening decisions, and would be feasible for medical assistants to provide to patients before a visit. While PCPs felt the DA was too long they did not agree on what information could be cut. The DA was designed to be comprehensive to include what many PCPs find important when deciding whether to continue mammography screening after age 75, but a PCP could remove a page or pages of the DA that they thought were unnecessary to shorten the DA before giving it a patient. Despite PCPs’ concerns about the DA’s complexity, 78% of patients in the DA trial felt that its length was just right or even too short. 14 Also, 84% of patients found the DA helpful regardless of their educational attainment and 97% with a high-school degree or less reported understanding most or all of the DA’s information. 31 Notably, these patients are the very patients that PCPs in the current study see. However, the DA was designed for patients to read before a visit and not to support clinician counseling during a visit, which may explain these discrepancies. Increasingly, easy-to-use web-based conversation aids are recommended to support clinician-patient shared decision making during a visit. 32 Based on study findings, investigators plan to develop a conversation aid to support shared decision making around mammography screening between PCPs and women ≥75 during a visit. To inform the content of the conversation aid, investigators are using simulation model output on the possible benefits and harms of screening women ≥75. 33
As recommended by IPDAS, the mammography DA was written at a sixth-grade reading level using low literacy principles and uses large font, bullet points, short sentences, and includes illustrations; yet, many PCPs were still concerned about its literacy level. 34 Therefore, investigators have recently developed and pilot tested an even lower literacy mammography DA for women ≥75 years. 35 The modified DA (also available at ePrognosis) is shorter than the original DA and does not use pictographs since older women with low health literacy who evaluated the original DA found the pictographs difficult to understand. 36 There is some debate about whether pictographs actually lead to more accurate interpretation of risk information for patients with low numeracy. 37 While additional research is needed on how best to support shared decision making for low literacy populations, some experts recommend that patients be offered skills training in shared decision making and others recommend decision coaching.38,39 Studies examining the added effectiveness of decision coaching to patient decision aids alone are needed particularly in low literacy populations. 40
While training programs for clinicians have been developed on shared decision making in general, few such programs have been implemented and few trainings have been developed for the use of specific DAs.41,42 Our DA was developed in the hopes of reducing PCP workload; thus, the DA trial did not mandate PCPs be trained on DA use. 20 However, 77% of PCPs in the current study reported wanting some type of training to use the DA. Few PCPs watched an optional video training during the DA trial, suggesting a more interactive training may be needed. Successful clinician trainings generally require modeling and role playing in addition to didactics.43,44 To support training, investigators have published example scripts for PCPs to use to engage women ≥75 in shared decision making around screening. 45 Furthermore, experts realize that shared decision making in the confines of primary care needs to be brief. Elwyn and colleagues developed a three-step model for shared decision making: 1) introducing that there is a choice, 2) describing options which may be supported by the use of patient decision aids, and 3) helping patients explore their preferences and make decisions. 46 Caverly and Hayward promote everyday shared decision making which encourages clinicians to qualitatively weigh the benefits and harms of a decision in 1 to 2 minutes. Their model includes use of patient DAs, like ours, outside of visits to support brief everyday shared decisions. 47 To further prepare women for decision making at age 75, PCPs could let women know before age 75 that at age 75 guidelines recommend shared decision making around whether to continue screening.
Although the majority of PCPs regardless of region felt that SDM around mammography screening was important, PCPs in NC were less likely to feel this way than PCPs in MA. Receipt of mammography screening is more frequent among older women in MA than in NC. 48 While DAs on average add 2.5 minutes to clinic visits, PCPs in NC may not feel that they need to spend extra time or resources engaging women ≥75 in shared decision making around mammography screening when most of their patients have already chosen to stop being screened. Since the risk of harm from screening relative to the chance of benefiting increases with rising age and comorbidity burden, choosing not to readdress this decision seems reasonable. 2 The findings suggest that the DA may be most helpful in areas where screening among women ≥75 is common.
There are several limitations to this study. This was a small, descriptive study. The majority of PCPs practiced in an academic setting (69%) and/or in Massachusetts (70% v. 30% from North Carolina) limiting generalizability. Twenty-seven PCPs (34%) practiced in the same large academic internal medicine practice as the principal investigator; however, there were no significant differences in perceived helpfulness of the DA by site. PCPs were approached for this study on average 590 days (±196 days) after their last patient participated in the trial; therefore, some PCPs were no longer reachable. Reassuringly, nonparticipants were similar to participants with regard to many factors; however, PCP participants were more likely to be female and non-Hispanic White. Some PCPs may have been more motivated to participate since their patients participated in the RCT; however, 56% of PCPs had been randomized to the trial’s control arm so the survey was the first time these PCPs learned of the DA.
Our findings may be useful for designing and implementing this and other DAs for older adults. Specifically, PCPs preferred that the DA be available in a shorter and longer version for patients with different health literacy levels to use, that it be available both on paper and on the web, that it be delivered to patients before encounters and that PCPs receive training to use the DA. PCPs also recommended that electronic medical records be modified to include space for documentation of DA use and any decision made.
Supplemental Material
sj-docx-1-mpp-10.1177_23814683221074310 – Supplemental material for Primary Care Providers’ Perceptions of the Acceptability, Appropriateness, and Feasibility of a Mammography Decision Aid for Women Aged 75 and Older
Supplemental material, sj-docx-1-mpp-10.1177_23814683221074310 for Primary Care Providers’ Perceptions of the Acceptability, Appropriateness, and Feasibility of a Mammography Decision Aid for Women Aged 75 and Older by Mara A. Schonberg, Mary Beth Hamel, Roger B. Davis, Maria Karamourtopoulos, Adlin Pinheiro, Michelle C. Hayes, Christina C. Wee and Christine Kistler in MDM Policy & Practice
Footnotes
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support for this study was provided entirely by a grant from NIH/NCI (R01CA181357). The funding agreement ensured the authors’ independence in designing the study, interpreting the data, writing, and publishing the report.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.