
Abstract
Introduction
Shared decision making (SDM) is a multicomponent process of interaction between health care clinicians, patients, and often caregivers to decide which screening or treatment option would better align with patients’ individual preferences and values.1–4 SDM should occur under conditions of uncertainty when there is no clear understanding of which screening or treatment option is superior and a health decision is preference sensitive.1,4–6
Although models for performing SDM exist, uncertainty remains about how to implement and achieve SDM in routine clinical practice.4,5,7,8 The adoption of SDM may be constrained by various health system, cultural, and practical barriers at the individual, organizational, and policy levels;2,8–10 however, it is unclear which barriers most impede the use of SDM. For example, although the most frequently cited barrier is insufficient time during a clinical encounter,2,8,10 SDM has been demonstrated to not extend the visit time necessary for usual care. 5 Patient-related barriers to full participation in SDM include insufficient knowledge about available options and the current evidence, high levels of decisional conflict, and power imbalance in the clinician-patient relationship.2,5
The most frequently cited clinician-related facilitator for successful adoption of SDM is the perception that SDM will improve patient outcomes and the clinical process. 10 Patient-related facilitators to SDM include trust in an equal clinician-patient relationship and an individualized approach where clinicians seek the patient’s preferences. 2 Patient decision support tools (e.g., patient decision aids) can be used to help clinicians and patients engage in SDM by improving patients’ knowledge regarding available options, helping them feel more informed, and clarifying their own values. 11 Decision aids may have limited effects on health outcomes since they are often used during situations of clinical equipoise in which there is no reason to expect better health outcomes from a particular screening or treatment option. 11
Approaches for increasing the use of SDM may include interventions targeting patients (e.g., patient decision aids, patient activation, question prompt lists), clinicians (educational materials, training in SDM, reminders), or both. Although many of these interventions have been tested, whether they increase the use of SDM remains uncertain. 3
The US Preventive Services Task Force (USPSTF) makes evidence-based recommendations for primary care clinicians about clinical preventive services, such as screenings, counseling services, and preventive medications. The USPSTF is committed to ongoing review and advancement of its methods and processes for making recommendations. 12 In particular, the USPSTF Dissemination and Implementation Workgroup aims to continually improve communication of USPSTF recommendations to facilitate their effective implementation and ultimately lead to better patient outcomes.13,14 The USPSTF strives to be helpful to clinicians applying its recommendations in practice, including the many USPSTF recommendations that entail engaging in SDM with patients. The USPSTF does not develop decision aids but would like to appropriately incorporate SDM principles in USPSTF recommendations and communication resources.
The Scientific Resource Center (SRC) for the USPSTF conducted this small methods project to support the USPSTF’s consideration of SDM and its efforts to help clinicians operationalize its recommendations. This project aimed to first evaluate how the USPSTF currently addresses SDM in its recommendations by identifying existing SDM frameworks that could guide which critical SDM elements to communicate in USPSTF recommendations (Aim 1) and assessing whether USPSTF recommendations address the core SDM components (Aim 2). For a more thorough appraisal of USPSTF SDM communication, we supplemented the information from SDM frameworks with experts’ perspectives on which SDM information would be most valuable for the USPSTF to incorporate into its recommendations and resources (Aim 3). Last, we developed criteria to inform the selection of USPSTF topics that would most benefit from additional communication resources to support SDM (Aim 4).
Methods
During the course of the project, a working group consisting of six USPSTF members, SRC staff, and an Agency for Healthcare Research and Quality (AHRQ) Medical Officer met regularly to discuss project methods and findings. We addressed each aim sequentially, and the workgroup reviewed and approved the proposed methods for each aim prior to their implementation.
Aim 1
To identify frameworks that could assist the USPSTF in assessing whether their existing recommendations communicate all information necessary to engage in SDM and what information to support SDM is missing from the recommendation statements, we conducted a literature scan in Ovid MEDLINE to identify existing SDM frameworks, using the following strategy:
*Decision Making/ or *Decision Support Techniques/
*Patient Participation/
“shared decision making”.ti,ab,kf.
((cooperative or cooperation) adj10 decision*).ti,ab,kf.
(patient adj5 (centered or centred or choice or autonomy)).ti,ab,kf.
((individualized or individualised) adj decision).ti,ab,kf.
We also conducted a scan in CINAHL using the heading “Decision Making, Shared,” reviewed the references of systematic reviews, and searched the websites of major decision aid and SDM guide developers.
We selected frameworks using a priori criteria that were focused on identifying frameworks most relevant to the scope of the USPSTF and project goals. The criteria specified that frameworks must be action oriented rather than theoretical or conceptual; relevant to a general primary care population instead of limited to patients with a specific condition; and focused on the patient-clinician interaction as opposed to interprofessional or organizational decision making. Most importantly, the framework needed to specify the essential SDM components to enable evaluation of USPSTF recommendations. Two SRC team members screened all identified articles against the selection criteria and reached consensus on final inclusion.
Aim 2
Although implementation of all USPSTF clinical practice recommendations involves some level of SDM, the workgroup decided this project should concentrate on C grade recommendations since these are likely to entail substantial SDM in their implementation. The definition of a USPSTF C grade is, “The USPSTF recommends selectively offering or providing this service to individual patients based on professional judgment and patient preferences. There is at least moderate certainty that the net benefit is small.” Using the USPSTF website in November 2018, we identified nine current topics with recommendation statements that included a C grade recommendation.
Some USPSTF C grade recommendations reflect the fact that the magnitude of net benefit is small so the service should be selectively offered to those at highest risk (e.g., behavioral counseling for skin cancer prevention in adults older than 24 years with fair skin types). While the population net benefit is small for these preventive services, the net benefit at the individual level varies depending on an individual’s risk and/or values and preferences. Exploration of these factors during SDM is needed to determine the magnitude of net benefit for the individual patient. We excluded these topics from the audit since the nature of the decision differs from other C grade topics. After removing three such topics, we evaluated the SDM content included in the six current USPSTF C grade recommendations that list patient values and preferences as one of the considerations for the decision about offering or receiving the preventive service: screening for abdominal aortic aneurysm (AAA) in men ages 65 to 75 years who have never smoked; aspirin for prevention of cardiovascular disease (CVD) and colorectal cancer in adults ages 60 to 69 years who have a 10% or greater 10-year CVD risk; breast cancer screening with mammography in women prior to age 50 years; colorectal cancer screening in adults ages 76 to 85 years; prostate-specific antigen (PSA)-based screening for prostate cancer in men ages 55 to 69 years; and statins for prevention of CVD in adults with a 10-year CVD even risk of less than 10%.15–20
SRC staff examined these six recommendation statements using definitions developed a priori for each of the SDM elements in one selected SDM framework; the definitions were reviewed, revised, and approved by the workgroup prior to the audit. To conduct the audit, we reviewed the entire text of the recommendation statements for the six topics and abstracted all text related to each of the SDM elements. The workgroup reviewed the abstracted text and approved the categorization of text as meeting (or not) the definition for each SDM element.
Aim 3
We engaged eight experts in SDM as key informants and solicited their input via email on 1) the most important SDM principles for clinicians to consider when engaging in SDM with patients, and 2) the most helpful SDM guidance to provide in USPSTF recommendation statements or communication resources. When selecting key informants, our objective was to collect multiple perspectives from experts currently conducting various types of research in SDM. We developed a list of potential key informants by reviewing authorship and references of recent, relevant publications in the SDM field and by soliciting workgroup member suggestions. All eight key informants have expertise and research foci in SDM, some specifically in implementation of SDM in clinical practice, others in patient engagement in decision making, and many with additional expertise in developing and evaluating patient decision aids and other SDM tools. These experts conduct SDM research in a wide range of clinical areas for which the USPSTF has recommendations, including prostate, breast, lung, and thyroid cancer. All key informants disclosed their financial and nonfinancial conflicts of interest. Some of these experts have received funding for their work (from federal agencies and companies that make products related to SDM), and many have worked together on SDM steering committees (e.g., the National Quality Partners Shared Decision Making Action Team) or in the development of various SDM frameworks or tools. Key informants were not involved in identifying or selecting SDM frameworks (Aim 1), the audit of USPSTF recommendations (Aim 2), or developing criteria to select USPSTF topics appropriate for supplementing with a communication resource to support SDM (Aim 4).
Aim 4
Communication resources to support SDM include patient decision aids, encounter tools, conversation aids, infographics, and other types of discussion guides. A preliminary step for the USPSTF’s SDM considerations is establishing a method to identify topics that would most benefit from additional communication resources to aid in implementation of recommendations. Many of these topics may be those for which patient preferences play a significant role and thus require patient engagement in decision making, but some may represent recommendations that are challenging to implement or communicate to patients.
SRC staff reviewed the text of the recommendation statement and evidence report for all USPSTF topics with A, B, or C grade recommendations to identify signals suggesting the need for a communication resource to guide discussions with patients. We included topics with A, B, and C grade recommendations because these recommend that clinicians offer a preventive service to all or some patients and therefore involve clinician-patient interaction. We looked for text indicating changes in the evidence or recommendation (often in Update of Previous USPSTF Recommendation section of recommendation statement), disconnect between the USPSTF recommendations and current clinical practice (often in Current Clinical Practice section of evidence report), potential challenges to implementing and/or communicating the recommendations (often in Implementation section of recommendation statement), and essential elements of SDM, such as uncertainties in the evidence (found throughout recommendation statement and evidence report). We abstracted all relevant text and reviewed it to identify themes, commonalities, and differences across topics, which were then used to draft criteria for selecting topics appropriate for a communication aid. We then applied the draft criteria to nine USPSTF topics with A, B, or C grade recommendations published in 2019, and the team revised the criteria to reduce ambiguity in their application.
Role of the Funding Source
This project was funded by the Agency for Healthcare Research and Quality under a contract to support the work of the USPSTF. Agency for Healthcare Research and Quality staff provided project oversight and feedback but were not involved in preparation of the manuscript for publication.
Results
Aim 1: Existing SDM Frameworks
We identified eight frameworks meeting selection criteria, all of which lay out a series of SDM steps, essential SDM elements or requirements, or physician competencies for SDM that could be used to judge the completeness of USPSTF recommendation statements.21–28 The developers of most of the frameworks acknowledge that SDM is not a linear process and the order of the steps is fluid and flexible, allowing for a two-way exchange of information and iterative deliberation.
Table 1 shows the eight identified frameworks and the SDM elements included in each. The number of elements in the frameworks ranges from four to nine; however, some frameworks collapse multiple elements into one. There is considerable overlap among the frameworks, with two elements present in all the frameworks—presenting options and eliciting patient values and preferences. Providing information on the benefits and risks (or pros and cons) of the alternatives, making or facilitating a decision, and planning for follow-up are found in all but one of the frameworks, while discussing the patient’s role in decision making is included in all but two of the frameworks. Identifying the decision that needs to be made, discussing uncertainty, and checking for understanding are addressed in fewer frameworks.
Shared Decision Making (SDM) Elements in SDM Frameworks

Some SDM elements may be less relevant to evaluating whether existing USPSTF recommendation statements communicate all key information to help inform a shared decision, for example, they are slightly downstream from the purview of USPSTF recommendations. In particular, making or facilitating a decision is the result of the SDM process and planning for follow-up occurs after the decision has been made. Leaving those two elements aside, the most comprehensive frameworks are those from Braddock et al., 21 Volk et al., 28 and Rusiecki et al. 24 After reviewing the information presented in Table 1, as well as the specific terminology used for the elements in the frameworks, the USPSTF members in the workgroup chose the Braddock framework for the audit of existing USPSTF recommendations because it is comprehensive and is attentive to the patient’s role in the decision. This model of informed decision making from 1999 outlines seven required elements based on a synthesis of the bioethics literature. The required elements are the following:
Discussion of the patient’s role in decision making
Discussion of the clinical issue or nature of the decision
Discussion of the alternatives
Discussion of the pros (potential benefits) and cons (risks) of the alternatives
Discussion of uncertainties associated with the decision
Assessment of the patient’s understanding
Exploration of patient preference
Aim 2: Audit of USPSTF C Grade Recommendations
Table 2 shows the definitions for each of the SDM elements used for the audit, and Table 3 presents the audit results. The patient’s role in decision making, nature of the decision, pros and cons of options, uncertainties, and the importance of patient preferences are included in all six recommendation statements. Prostate cancer screening is the only topic that includes all seven SDM elements. The only recommendation that explicitly refers to “shared decision making” is for initiating statins for prevention of CVD in adults with a 10-year CVD event risk of less than 10%, which states that the decision to begin statin use “should reflect shared decision making that weighs the potential benefits and harms, the uncertainty about risk prediction, and individual patient preferences, including the acceptability of long-term use of daily medication.” 18 The two SDM elements not routinely addressed in the recommendation statements are 1) identification of not screening or not initiating preventive medication use as an alternative (i.e., doing nothing as an alternative) and 2) the importance of patient understanding of the options.
Definitions for Shared Decision Making (SDM) Elements in Braddock Framework

Audit of Six USPSTF C Grade Recommendations
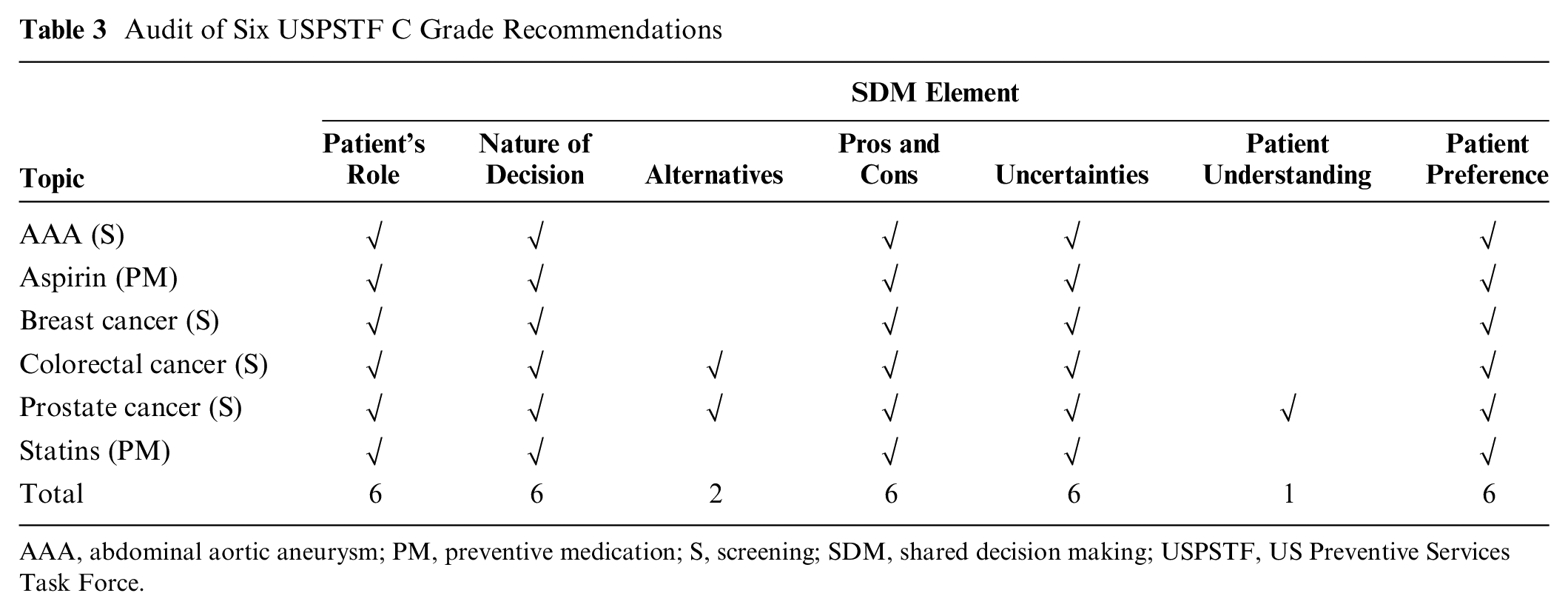
AAA, abdominal aortic aneurysm; PM, preventive medication; S, screening; SDM, shared decision making; USPSTF, US Preventive Services Task Force.
Examination of the manner in which the SDM elements are incorporated in the recommendations showed that the location of the SDM information in the recommendation statement varies widely across the six topics and none have all the SDM-relevant information in one place. All topics except for statins have a separate section in the recommendation where some of the SDM-relevant information is presented, although the title of the section differs (e.g., Implementation, Informed Decision Making). Five of the topics address areas of uncertainty in the evidence in the Research Needs section of the recommendation statement. All six topics have SDM-relevant information, especially potential benefits and harms of the service, presented throughout the Rationale, Clinical Considerations, and Discussion sections.
Aim 3: Incorporation of SDM Information Into USPSTF Recommendations
Key informants’ views of the most important SDM principles for clinicians to consider when engaging in SDM with patients overlap considerably with the SDM elements included in the audit of USPSTF C recommendations, including the patient’s role in decision making, the nature of the decision/choice awareness, the potential benefits and harms of options, areas of uncertainty, and the importance and role of patient preferences or values. However, key informants offered several suggestions for how clinicians might address these SDM elements with patients. For example, in discussions of the patient’s role in decision making, they stressed the importance of explaining why the patient’s involvement is necessary (i.e., choice awareness).29,30 Key informants specified that the discussion about uncertainties should include estimates of benefit and harm, credibility of the evidence base, precision of estimates, and applicability to the individual patient. Experts proposed that presentation of the options start with the issues that distinguish among the options, followed by a request for the patient to identify the issue most relevant to them, and ending with a discussion of how each option fares on that issue. 30 Key informants suggested that communication resources, such as decision aids, encounter tools, or conversation aids, may be helpful to patients, but only when combined with clinician discussion of the available options. 31 These SDM experts also recommended that clinicians assess decisional conflict at the beginning and end of discussions to measure patient uncertainty in choosing an option and gain insight into what additional information and support the patient may need.32,33
Many of the experts’ suggestions above point to useful information to include in USPSTF recommendation statements to support clinicians’ discussion of SDM elements, such as estimates of benefit and harm, the precision of these estimates, and the applicability of these estimates to different patient subpopulations. In addition, when asked what SDM guidance would be helpful to provide in USPSTF recommendation statements, key informants advised including a short, patient-friendly summary of 1) options, including the alternative of doing nothing; 2) key outcomes (benefits, harms, treatment burden, cost, etc.); and 3) likelihood of key outcomes. Experts responded that an indication of whether the recommendation is preference sensitive would be valuable, along with information on the range of patients’ preferences (e.g., goals, concerns, attitudes toward outcomes) from a search for preference-related evidence (e.g., patient preferences for health outcomes using quality of life measures, studies of patients’ experiences and actual decisions). 34 Several suggestions from key informants relate to communication guidance for clinicians, such as how to communicate potential benefits and harms, how to assess patients’ willingness to take medication, and how to assess whether patients feel the benefits outweigh the harms.
Aim 4: Selection Criteria for Topics to Supplement With Communication Resource
In our review of USPSTF topics with A, B, or C grade recommendations, we found six general situations that explain variation in clinical practice and could therefore identify topics most likely to benefit from a communication resource:
New recommendation or substantially updated recommendation that requires a change in current clinical practice
Challenges in identifying the right population for the service at the point of care
Narrow balance of benefits and harms at the population level
Decision about patient receipt of service heavily depends on patient values and preferences
Existing health disparities related to provision or uptake of service
Suboptimal uptake of the service
These situations represent six criteria that could guide selection of USPSTF recommendations to supplement with a communication resource.
Notably, application of these criteria involves subjectivity, especially when clear evidence to support the criteria is lacking. In addition, the importance of these criteria may not be equal, so a count of criteria met may be too simplistic to be a good indicator for topic selection. There is also some overlap among the selection criteria (e.g., decisions that depend heavily on patient values and preferences often involve challenges in identifying those at risk and show suboptimal uptake of the service). Despite these complexities in applying these selection criteria, they provide an indication of USPSTF recommendations for which clinicians may need support in engaging in SDM with patients. Two 2019 USPSTF recommendations provide examples of how the selection criteria can inform the need for a communication resource (see Box 1).
Application of Selection Criteria: Two Examples

Discussion
To support USPSTF considerations of how best to communicate SDM in its recommendations, this methods project identified essential elements of SDM from a literature scan and expert informants, evaluated the way USPSTF recommendations currently address SDM, and developed criteria that could guide the selection of USPSTF topics to supplement with a communication resource. Five SDM components are included in all six USPSTF recommendation statements that we audited—the patient’s role in decision making, nature of the decision, pros and cons of options, uncertainties, and importance of patient preferences. However, two components—identification of not screening or initiating preventive medication use as an alternative and the importance of patient understanding of the options—are not routinely communicated.
Development of decision aids is not within the scope and resources of the USPSTF; however, the USPSTF is currently considering how to incorporate the project findings into its recommendations, processes, and resources. This may include exploring ways to provide more guidance in the recommendation statement about the key things clinicians should be sure patients know before making a decision, or approaches to developing more communication resources for topics meeting the selection criteria created during this project.
Based on the assessments shown in Box 1, discussion guides for these two USPSTF topics were recently developed and posted on the USPSTF website to be used as conversation starters with patients (https://uspreventiveservicestaskforce.org/uspstf/sites/default/files/inline-files/hiv-prep-guide-2020_0.pdf and https://uspreventiveservicestaskforce.org/uspstf/sites/default/files/inline-files/breast-cancer-risk-reduction-discussion-guide.pdf).
This project has several limitations. The audit, expert recommendations, and selection criteria for communication resources were focused on clinical preventive services (i.e., screening, counseling, and chemoprevention) and the USPSTF’s scope and processes. However, they are likely applicable to any evidence-based clinical practice guidelines since SDM is vital to nearly all clinical contexts. The audit of USPSTF recommendation statements was limited to C grade recommendations that require input on patient preferences. Although implementation of C grade recommendations likely requires more SDM than those with other grades, project findings may have utility for other USPSTF recommendations but would require further investigation to determine how they apply to these topics. Last, our literature scan and screening processes for SDM frameworks may have resulted in some frameworks being missed. However, the goal was not to conduct a systematic review of SDM frameworks but to identify one comprehensive framework that fit the scope of the USPSTF and could be used to audit the SDM information included in USPSTF recommendation statements.
The findings of this project can assist the USPSTF and other clinical practice guideline developers in incorporating SDM information in recommendations and determining which topics would most benefit from additional communication resources to support clinicians in engaging patients in SDM.
Footnotes
Acknowledgements
The authors thank the following persons for their assistance with this project: Emily S. Walsh, MPH; Megan O. Iacocca, MS; Allea Martin, MPH; Debra Burch; Melinda Davies, MAIS; and Smyth Lai, MLS. They also thank Amanda E. Borsky, DrPH, MPP, who served as the AHRQ Project Officer, and the USPSTF Workgroup for their contributions to the project: Michael J. Barry, MD; Aaron B. Caughey, MD, MPP, MPH, PhD; Karina Davidson, PhD, MASc; John Epling Jr., MD, MSEd; Alex H. Krist, MD, MPH; Chien-Wen Tseng, MD, MPH, MSEE; and John B. Wong, MD. They also thank the following key informants: Juan P. Brito, MD, MSc; Glyn Elwin, MD, PhD, MSc; Dominick Frosch, PhD; France Légaré, MD, PhD; Christopher Saigal, MD; Karen Sepucha, PhD; Dawn Stacey, PhD, MScN, BScN; and Robert Volk, MD.
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded under contract HHSA290201600006C from the Agency for Healthcare Research and Quality (AHRQ) of the US Department of Health and Human Services. The authors of this article are responsible for its content. Statements in the article do not necessarily represent the official views of or imply endorsement by AHRQ or the Department of Health and Human Services. The funding agreement ensured the authors’ independence in designing the study, interpreting the data, writing, and publishing the report.