
Abstract
Introduction
In many health care systems, colonoscopy is a scarce resource. 1 Patients at some facilities face long wait times for elective colonoscopy for colorectal cancer (CRC) screening,2–5 a fact that has been compounded by a simultaneous increase in demand for colonoscopy and a reduced number of available endoscopists.6,7 More recently, the COVID-19 pandemic has further reduced the availability of colonoscopy. 8
Typically, information about resource limitations is not explicitly discussed with patients, and it is unclear how their attitudes toward use of resource-limited services changes when they are given information about the impact of supply constraints in the health care system on others. It is possible that such conversations could appeal to one’s sense of altruism (an intentional act performed to benefit another person as the primary motivation). 9 Altruism has been studied in a variety of domains in health care (e.g., judicious use of antibiotics to prevent antimicrobial resistance, public health benefits of vaccinations, and cost-prohibitive treatment of hepatitis C),10–13 but not in CRC screening. This issue is of renewed relevance in the current COVID-19 recovery phase, when endoscopy units are working to reduce backlogs and there is a guideline-recommended alternative available—fecal immunochemical testing—which is not always known to patients.8,14
Using a survey of US Veterans that assessed attitudes toward low-value CRC screening cessation, 15 we further examined attitudes toward risk-based prioritization of scheduling. We hypothesized that Veterans awaiting average-risk screening colonoscopy would be willing to defer their own procedures so that higher-risk patients could be prioritized. Additionally, we hypothesized that specific factors (such as patient characteristics, beliefs about screening, and trust) would influence willingness to defer.
Methods
We performed a survey of Veterans who underwent a negative (i.e., normal) average-risk screening colonoscopy to elicit attitudes toward repeat screening colonoscopy at the Ann Arbor VA Medical Center (AAVA). The Institutional Review Board of the AAVA approved this study.
Survey Design
Survey development has previously been described. 15 Briefly, we presented each participant with a detailed, hypothetical scenario of a patient–provider clinic encounter. The scenario began with information on how and why screening is initiated at age 50 in average-risk individuals, followed by an explanation of screening cessation recommendations. The survey assessed specific aspects of CRC screening that are important to the screening decision (e.g., benefits, harms, risk stratification, supply constraints, etc.). The full instrument, available as Supplemental Material, comprised 42 questions that took approximately 15 to 20 minutes to complete.
We assessed Veterans’ attitudes toward CRC screening cessation by introducing a scenario describing low risk for CRC that included a recommendation to stop screening. Respondents answered “how likely do you think you’d be to follow the doctor’s recommendation to stop screening for colon cancer?” on a unidirectional 7-point Likert-type scale ranging from “not at all likely” (1) to “extremely likely” (7). We also examined a subgroup of questions about attitudes toward risk-based prioritization of scheduling, framed to appeal to altruism. Specifically, we asked respondents, “If you were at lower risk for cancer than other patients, would you be willing to wait up to 6 months to get your next screening colonoscopy, so that higher risk patients could be screened first?” Responses were recorded as “Definitely Yes,”“Probably Yes,”“Probably No,” and “Definitely No.”
We collected baseline information on sociodemographic and health factors, including age, gender, race, marital status, highest level of education, self-reported health status, and health literacy (using a validated scale by Chew et al. 16 ). In addition, we assessed Veterans’ trust in health care, prior experience with CRC screening, and health belief model constructs (i.e., perceived susceptibility to CRC, perceived threat of CRC, perceived effectiveness of colonoscopy, and perceived barriers to completing colonoscopy). 17
Population and Sampling
Participants were identified electronically using the endoscopic database at the AAVA. The AAVA serves as a majority tertiary care referral center for Veterans in Michigan and northwestern Ohio. We included Veterans who met the following criteria: 1) age ≥50; 2) prior complete, negative average-risk screening colonoscopy with adequate bowel preparation. Individuals were excluded if they had a personal history of adenomas, family history of colon cancer, or a personal history of inflammatory bowel disease. Surveys were mailed in April 2012, with a second mailing to nonresponders 3 weeks later. All potential respondents received a $10 gift card.
Statistical Analysis
We reported descriptive statistics (means or proportions), compared groups using the chi-squared test, and conducted multivariable ordinal logistic regression analysis to identify patient factors associated with greater willingness to wait. We adjusted regression results for age, gender, race/ethnicity, perceived health literacy, trust in physician, self-reported health status, perceived effectiveness of screening, perceived barriers to screening, and perceived threat of CRC. All analyses were performed using Stata 14.1 statistical package (StataCorp, College Station, TX).
Results
Of the 1500 surveys mailed, 85 surveys returned to sender, yielding 1415 potential respondents. Of these, 1054 completed the survey (response rate = 74%). Respondents were predominately White (86%) and male (94%). The median age was 60 to 69 years. Most patients (74%) reported their general health as either good, very good, or excellent (Table 1).
Patient Baseline Characteristics of Survey Respondents (N = 1054)

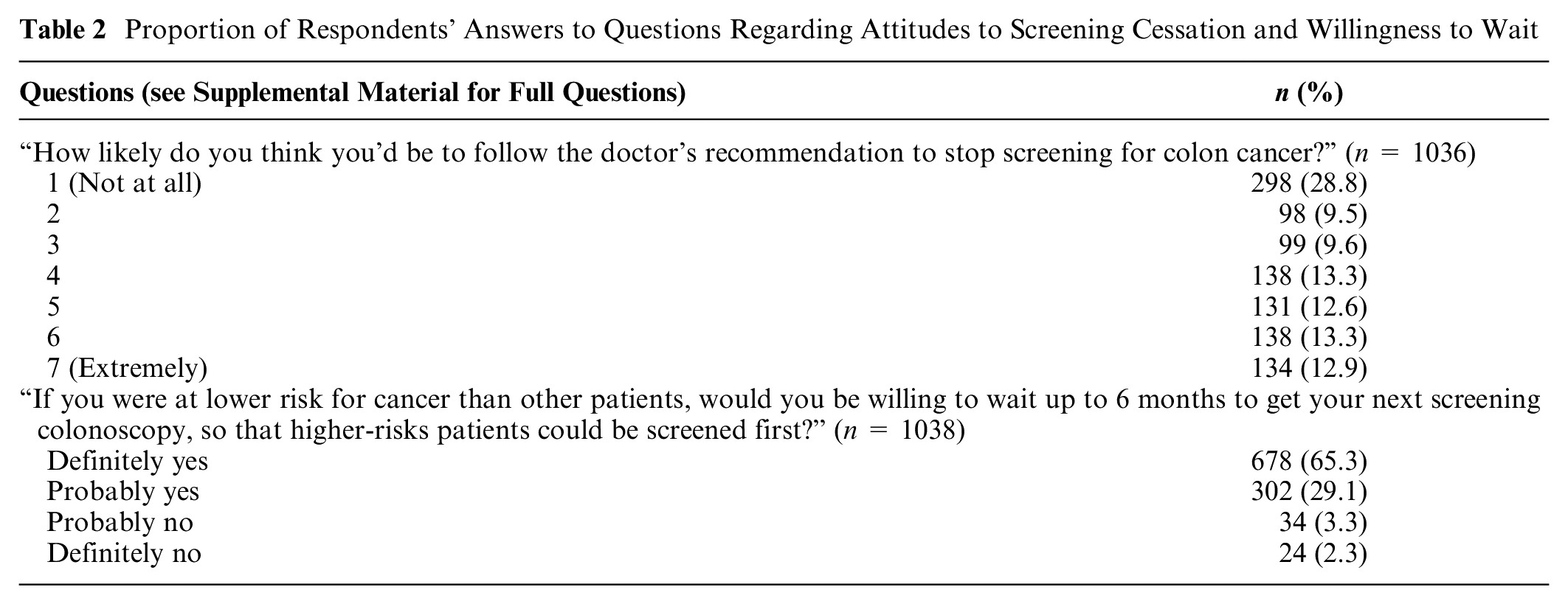
Many respondents were resistant to screening cessation, with 298 (28.8%) stating that they were “not at all likely” to stop screening (response = 1 on 7-point Likert-type scale ranging from “not at all likely” to “extremely likely”) even if a physician recommended that they stop (Table 2). Despite this, patients reported a strong willingness to delay their own colonoscopy so that another, higher-risk patient could undergo colonoscopy sooner. Specifically, 94% of respondents stated they would definitely (65%) or probably (29%) be willing to wait in order for a higher-risk peer to be prioritized (Table 2). In multivariable analysis, factors associated with greater willingness to wait were the following: 1) greater trust in physician (odds ratio [OR]: 1.39; 95% confidence interval [CI]: 1.23–1.57) and 2) greater perceived health literacy (OR: 1.25; 95% CI: 1.09–1.44). Factors associated with less willingness to wait were the following: 1) greater perceived threat of CRC (OR: 0.77; 95% CI: 0.69–0.87) and (2) identifying as Black (OR: 0.39; 95% CI: 0.24–0.62) or Latino (OR: 0.34; 95% CI: 0.16–0.72; Table 3).
Proportion of Respondents’ Answers to Questions Regarding Attitudes to Screening Cessation and Willingness to Wait
Multivariable Ordinal Logistic Regression: Factors Predicting Willingness to Wait (n = 979)

Discussion
Colonoscopy is a limited resource, and in some health care systems, these resource limitations can affect timely receipt of colonoscopy. One way to address these resource limitations is to prioritize care according to risk. But our data show that most Veterans who have previously been screened (and are therefore at low risk for CRC) are resistant to the idea of CRC screening cessation, which is consistent with prior data.18–21 Despite this general preference for ongoing screening, the majority would be willing to defer their own colonoscopy for at least 6 months so a higher-risk peer could undergo colonoscopy sooner.
To our knowledge, communication that openly discusses supply constraints and appeals to an individual’s sense of altruism in cancer screening has not been previously evaluated. Our study suggests that framing communication in this way could be persuasive, as 94% of our participants were willing to delay their own screening for someone else despite high baseline enthusiasm for screening. The impact of other factors identified in our study, such as health belief model constructs, physician trust, race/ethnicity, and health literacy, was consistent with prior literature.22–28 For example, Gupta et al. 22 found physician trust to be the strongest predictor of CRC screening completion in a low-income population. While this finding may seem contradictory to our study, it is important to note that trust may simply support willingness to follow the physician’s recommended course of action—screening completion in a screening promotional context (as in the case of Gupta et al. 22 ) or screening cessation/deferral in a screening de-intensification context (as in the case of this survey). It is not surprising that, in our study, Black and Latino patients were less likely to defer endoscopic procedures, as many institutions have historically and consistently failed to garner the trust of marginalized communities.23–25 Regarding health literacy, previous studies suggest that higher health literacy is associated with greater baseline knowledge about CRC screening, which may explain why patients with higher health literacy would be more willing to defer their endoscopy for a higher-risk peer. 26
Our study has several strengths and limitations. First, it may not be representative of the general population. However, the high response rate (74%) minimizes the potential effect of nonresponse bias. In addition, it is important to note that the “cost” of deferring a screening colonoscopy may be low/marginal for many patients. Unlike deferring or forgoing a resource-limited treatment (e.g., organ transplantation, COVID-19 vaccination), deferring a screening colonoscopy is likely to cause little clinical harm. However, it is important to also acknowledge that a substantial proportion of patients in our study deemed screening so important, that they would not stop. Likewise, we cannot isolate whether messages that incorporate altruism are more effective than other types of messages, which could be investigated in future studies using randomization. Furthermore, our study is a survey study that assesses patients’ attitudes and perceptions toward a hypothetical situation; this may or may not mimic actual behavior and is subject to social desirability bias.
In conclusion, this study suggests that despite having a strong personal interest in repeat low-value screening, patients were almost universally willing to delay their own screening colonoscopy for higher risk patients. This suggests that in some clinical contexts, patients have the potential to act as responsible stewards of health care resources and as stakeholders in health policy decisions. Ultimately, appealing to altruism has the potential to be effective in situations where scarce resources must be utilized wisely. It could also be of value in discussing screening with older adults with limited life expectancy, in whom the benefits of screening are marginal and guidelines recommend de-intensification. Future studies should assess both qualitatively and quantitatively how to best communicate with patients regarding the use of low-value screening and other health care services.
Footnotes
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Veterans Affairs (VA) Health Services Research and Development (HSR&D) Career Development Award (VA CDA 09-213-2) and grant NIDDK T32 DK062708 from the National Institute of Diabetes and Digestive and Kidney Disease funded this work. VA had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; and preparation, review, or final approval of the manuscript.
Author Contributions
Sameer D. Saini and Marc S. Piper had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
Study concept and design: Sameer D. Saini and Brian J. Zikmund-Fisher.
Acquisition, analysis, or interpretation of data: Marc S. Piper, Sameer D. Saini, Jacob Kurlander, Jennifer K. Maratt, and Akbar K. Waljee.
Drafting of the manuscript: Marc S. Piper and Sameer D. Saini.
Critical revision of the manuscript for important intellectual content: All authors.
Statistical analysis: Marc S. Piper and Sameer D. Saini.
Administrative, technical, material support, and acquisition of data: Sameer D. Saini and Valbona Metko.
Study supervision: Sameer D. Saini.