
Abstract
Keywords
Introduction
Around 20 million people a year need palliative care worldwide; in the Netherlands, in 2017, over 100,000 people went through a palliative phase before they died.1,2 The World Health Organization (WHO) defined palliative care as “an approach that improves quality of life of patients and their families who are facing problems associated with life-threatening illness.” 3 Addressing the needs of patients and their partners/family is an important goal of palliative care. The recommended approach for making decisions in which the needs of patients and their partners/families are addressed is shared decision making (SDM).4–6 In SDM, health care professionals and patients decide the best treatment and care option together after discussing all available options, their pros and cons and personal preferences, and the circumstances of the patient.4–6 In the Netherlands, professionals are required by law to fully inform patients about all available options, risks and consequences, and become aware of the patient’s situation, personal needs, and invite the patient to ask questions.7,8
SDM in palliative care can be complicated and challenging. Patients in the palliative phase of their disease sometimes receive inpatient or outpatient hospital care, which is highly complex and preference-sensitive. 9 Additionally, emotional and psychological distress, the prospect of death, and cognitive abilities of patients (as a result of advanced age, illness, or educational level)10–12 result in patients having problems processing information.11,13 The complex and preference-sensitive care and difficulties with processing information in palliative care could lead to reduced communication and, in turn, hampered SDM. 14 Attention to SDM is therefore warranted for all patients in palliative care.
Bearing in mind the complexity of decision making in palliative care for all patients, SDM is an even bigger challenge with and for patients with limited health literacy (LHL).15,16 LHL is defined as “the limited ability to access, understand, appraise, and apply health information to make judgments and make decisions in everyday life concerning healthcare.”15–18 In Europe, almost 48% of the population experience these difficulties. 19 The estimated proportion of adults with LHL in the Netherlands is 29%. 20 Groups most at risk of LHL are semiliterate people (2.5 million in the Netherlands), people with 10 years or less of formal education, the elderly, people with low socioeconomic status (SES), chronically ill people, and first-generation migrant workers with little formal education and low SES.20–22 Nevertheless, LHL is also found in people with medium or high levels of education, indicating that LHL is determined by more factors or situational elements than only the number of educational years, and can be seen as both a trait or a state.23,24 Because of the difficulties LHL people have with health and health care information, this complicates communication in health care and, in turn, hinders SDM.25,26 As a consequence, patients with LHL are involved in SDM less often, have less favorable health outcomes, spend more time in the hospital, and have a lower medication and treatment compliance. 12
Health literacy is increasingly gaining attention in health care practice. The WHO considers it as one of the central determinants of inequality in health care. 27 Communication strategies that aim to improve communication between professionals and LHL patients include the teach-back method, chunk and check, and the use of pictures and illustrations.18,28–31 In palliative care, limited research has been carried out focusing on SDM and LHL. 29 We do know that SDM is not always used in Dutch clinical practice.32–34 Professionals want more time to communicate with LHL patients in palliative care because, in their view, time is the most important aspect for resolving the current barriers.35,36 We also know that palliative patients want to engage in SDM 37 and value good communication with their professional highly. 38 This study aimed to examine SDM in palliative care for LHL patients conducted by specialized palliative care clinicians and professionals integrating a palliative approach, and to assess these professionals’ perspectives on their own SDM.
Methods
Study Design
An explanatory sequential mixed methods design was used, in which fragments from the video-recorded consultations were used in interviews to further understand quantitative observations of SDM. Cross-sectional, video-recorded consultations were gathered. Video recordings of consultations are a valid method for examining communication between health care professionals and patients. 39 SDM was investigated by measuring the extent to which professionals involved patients in SDM, using the “Observing Patient Involvement in Decision-Making” (OPTION) 5 instrument.40–42 Sequentially, the professionals reflected on their own SDM behavior and how they thought they had involved their patients in SDM during “stimulated recall interviews.”43–46 Video-recorded consultations were used to stimulate the professionals’ recall of the outpatient consultation and to discuss the professional’s thoughts, meanings, and subjective reactions elicited by it.44,45
Setting and Procedure
Consultations in oncology, radiation oncology, pulmonary disease, and specialized palliative care departments were the setting for this study, including professionals integrating a palliative approach and specialized palliative care clinicians. These clinical areas were chosen because of the clear correlation between LHL and poorer health: asthma and chronic obstructive pulmonary disease (COPD), diabetes, cancer, cardiovascular disease, and psychological problems are significantly more common in people with LHL in the Netherlands. 16 Data were collected between April and October 2018 (RR and WvdH) as part of a larger project called “A Basic Understanding,” which aims to improve information provision and decision making with LHL patients in secondary palliative care (Appendixes 1 and 2). Four Dutch hospitals participated, located in different regions of the Netherlands (three academic hospitals and one general hospital). To protect the privacy of participants, recordings were anonymized by deleting all data that could reveal the identity of the participants. In video recordings, when expressions of names that could reveal the identity of participants were audible, the audio was deleted. The study protocol was evaluated by the Medical Ethics Committee of the Radboud University Medical Center, which exempted the study from formal ethical approval (File Number CMO: 2017-3623).
Participating hospitals appointed an employee as the local project manager—in two cases a specialized nurse and in two cases a medical specialist—functioning as the contact point for the researchers. These local project managers invited professionals in the hospital to participate. Eligible patients were preselected by the local project manager based on inclusion criteria47,48 and convenience sampling, and were informed by phone by the project manager or researcher approximately a week before the planned visit to the hospital. At that moment, the patients also received information explaining the background of the study, the purpose of the video recordings and the procedures, and contact details of the researchers.
Patients who expressed interest were approached by a researcher in the waiting room before seeing their health care professional. If patients decided to participate, inclusion criteria were checked in a private room at the hospital using a short questionnaire. The researcher asked the questions and registered the answers. Furthermore, the patients and professionals signed an informed consent form (IC) before the video recording of the consultation. To make sure that LHL patients could fully understand the patient information form and IC forms, tailored versions were created using plain language. Both were tested by a panel of the Dutch ABC Foundation (low literacy volunteers who regularly assess the understandability and applicability of texts). An unmanned video camera was installed in the consulting room, pointing at the professional, making them visible and audible on video; patients (and partners/family) were only audible. Patients received a gift voucher between 10 and 30 euros, depending on the amount of participation in the project. The video recordings were stored in a secured and locked room at Nivel; only researchers had access to them. Four to 8 weeks after the initial recording, professionals looked back at carefully selected fragments of their own consultations about SDM with a researcher (RR or WvdH). These stimulated recall interviews were conducted at their workplace.
Participating Patients and Professionals
LHL patients in this study are defined as per the definition given earlier in the introductory paragraph. 15 They are aged ≥18, have been diagnosed with cancer or COPD, and are in the palliative phase of their disease. The assessment of the palliative phase of patients for both cancer and COPD was conducted by the local project manager or professional of the participating hospital, always someone with a medical background capable of making this assessment. In this assessment, they adhered to the definition of palliative care given in the introduction. 3 The assessment of the level of health literacy of the patient was checked and determined by using a short questionnaire, asking the educational background of the patient and asking three questions indicating health literacy: “Many people find it difficult to read hospital leaflets—how about you?”“Many people find forms and filling them out difficult—how about you?” and “Do you need help filling out forms or reading leaflets?”47,48 An educational background at or lower than vocational level or less than 10 years of formal schooling, and affirmative answers to at least one of three health literacy questions indicated LHL. Patients were also included when professionals considered them to be LHL (expert opinion). This consideration prevailed the educational background and the “three question assessment” of LHL, because LHL is also found in people with medium or high levels of education and patients often hide that they do not understand health information.16,31 Therefore, patients could easily circumvent our assessment in the questionnaire. Patients were excluded from participating if they 1) did not speak the Dutch language, 2) were in the terminal phase of their disease, 3) had a severe intellectual disability, or 4) had a psychiatric problem or dementia. The professionals included were physicians and nurses who regularly conduct consultations with patients with cancer and/or COPD and discuss palliative care and/or treatment options.
Instrument and Analyses
Option 5
The OPTION 5 instrument is a reliable and valid method for investigating SDM.40–42 Five SDM items are coded on a 5-point Likert-type scale, ranging from 0 = “zero effort observed” to 4 = “exemplary effort,” as presented in Table 1. The OPTION 5 instrument includes the rating of communication by professionals and patients in the consultation related to prior conversations. 49 This means that, for instance, if a professional or patient refers to a prior establishment of goals, preferences, or decisions, this is included in the assessment of SDM. Coding was conducted using BORIS software. 50 All 40 video-recorded consultations were initially checked by one main observer (RR) on whether SDM was conducted and if SDM could be measured using OPTION 5 . Thirty-six consultations were observed by the main observer, and 25% (10 consultations) were also reviewed by a second observer (JN) to ensure reliability. Both observers had been trained to use the OPTION 5 instrument. When multiple decision-requiring issues (or index problems, as referred to in OPTION 5 ) 49 were discussed in one consultation, the main observer selected one of the issues for observations. These issues were selected for observation when a decision was needed in the relevant consultation, or when patients addressed the issue to be solved. The selected issues were communicated to the second observer. Interrater reliability between observers was calculated using Cohen’s kappa (0.80), indicating a substantial interrater agreement. 51
Observations of Palliative Care Consultations With LHL Patients Using the OPTION 5 Instrument, per Item and Corresponding Scores

OPTION 5 , observing patient involvement in decision-making instrument.
Score description: 0 = No effort (zero effort observed in the video-recorded consultation); 1 = Minimal effort (effort to communicate could be implied or interpreted in the video-recorded consultation); 2 = Moderate effort (basic phrases or sentences used in the video-recorded consultation); 3 = Skilled effort (substantive phrases or sentences used in the video-recorded consultation); 4 = Exemplary effort (clear, accurate communication methods used in the video-recorded consultation).
The total OPTION 5 score is generated by converting the scores to a 0 to 100 scale and then calculating the average. The higher the score, the higher the level of SDM. Potential determinants for applying SDM by professionals (type of disease, sex of patients and professionals, age of patients, consultation duration and the type of consultation) were analyzed using multilevel analysis [with professionals as Level 1]. All variables were added to allow an explorative analysis of any possible associations with SDM.52–55 Because of the explorative nature of our analysis, every item in the OPTION 5 instrument was additionally calculated independently. Data was analyzed using Stata version 15. 56
Stimulated Recall Interviews
Before conducting the interviews, the video-fragments used in the interviews were selected individually by two researchers (RR and WvdH), focusing on three types of occurrences in the videos: 1) the expressions of emotion by the patient, 2) potential manifestations of misunderstandings between patient and professional, and 3) elements of SDM (using the OPTION 5 protocol40,41,49). After selecting fragments, the researchers compared their findings, in which differences were resolved through discussion, leading to a maximum of three fragments to be viewed and discussed in the interviews. Interviews took place 4 to 8 weeks after the initial recording. The professionals were asked to recall the consultation and give their perspectives on communication, SDM, and other aspects that could facilitate or hinder communication with LHL patients. 57 The topic list (Appendix 3) used during the interviews was developed based on literature and experience from previous research 58 (JN, SvD). Feedback was provided on initial versions of this topic list by researchers with ample experience in researching LHL (JN, SvD, GB, RR). All the interviews were audio-recorded and transcribed verbatim (RR and WvdH). To increase credibility, all professionals conducted a member check, that is, to check the completeness of the transcripts. Participants did not provide feedback on the results of our study.
The interview transcripts were analyzed using deductive thematic content analysis. 59 All transcripts were read carefully and parts in which elements of SDM were mentioned were selected (RR). Initial codings were applied to these segments independently by one researcher (RR). These codings were reviewed and complemented by a second researcher (JN). Discrepancies between researchers were resolved through discussion, and modifications to the initial categories were made when necessary (RR, JN). All categories and patterns that emerged during analysis are illustrated by multiple quotes that were translated into English and edited, increasing readability without losing meaning or context.
Results
Sample Characteristics
Table 2 provides an overview of the medical and demographic characteristics of participating patients and professionals. Forty consultations were video-recorded, SDM was assessed in 36. Four videos were excluded, because consultations were too short, or in hindsight, the intellectual disabilities of patients were too severe. Thirty-six individual patients and 19 individual professionals participated in the video-recorded consultations. During two video-recorded consultations, two professionals participated simultaneously in the consultations. Therefore, 38 consultations were discussed with 19 professionals.
Characteristics of Patients and Health Care Professionals in the Video-Recorded Consultations, in the OPTION 5 Observations and the Stimulated Recall Interviews
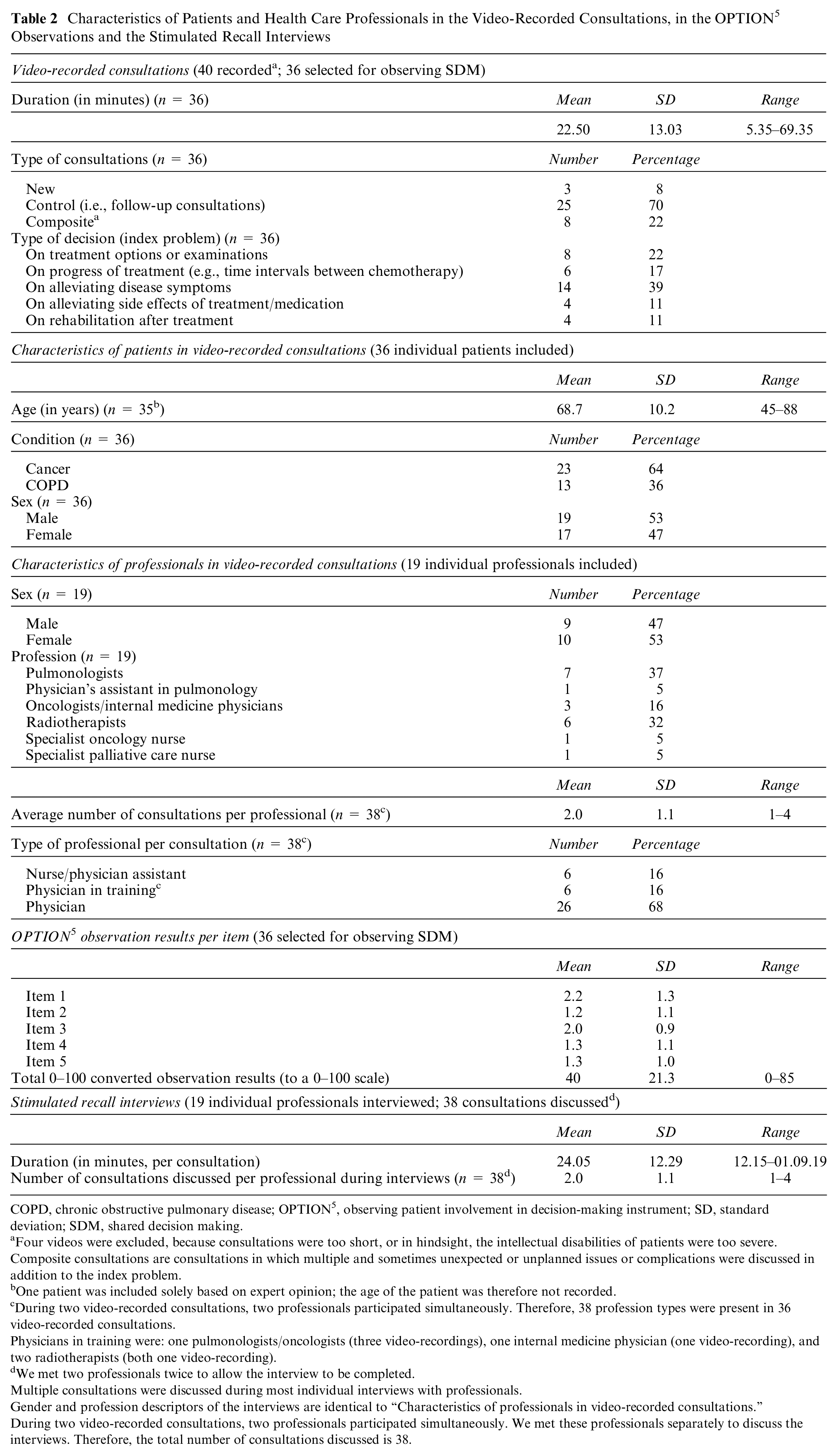
COPD, chronic obstructive pulmonary disease; OPTION 5 , observing patient involvement in decision-making instrument; SD, standard deviation; SDM, shared decision making.
Four videos were excluded, because consultations were too short, or in hindsight, the intellectual disabilities of patients were too severe.
Composite consultations are consultations in which multiple and sometimes unexpected or unplanned issues or complications were discussed in addition to the index problem.
One patient was included solely based on expert opinion; the age of the patient was therefore not recorded.
During two video-recorded consultations, two professionals participated simultaneously. Therefore, 38 profession types were present in 36 video-recorded consultations.
Physicians in training were: one pulmonologists/oncologists (three video-recordings), one internal medicine physician (one video-recording), and two radiotherapists (both one video-recording).
We met two professionals twice to allow the interview to be completed.
Multiple consultations were discussed during most individual interviews with professionals.
Gender and profession descriptors of the interviews are identical to “Characteristics of professionals in video-recorded consultations.”
During two video-recorded consultations, two professionals participated simultaneously. We met these professionals separately to discuss the interviews. Therefore, the total number of consultations discussed is 38.
SDM in Practice
The mean SDM score (0–100 score) was 40 (see Table 2). Of the OPTION scale items (see Table 1), the highest average score was observed for Item 1 (2.2; professional drawing attention to or confirming options and the need for a decision), the lowest average score was observed for Item 2 (1.2; professional reassures or reaffirms support to the patient for becoming informed or deliberate options). This indicates that the extent to which clinicians involve patients in SDM in practice lies between a minimal effort (effort to communicate could be implied or interpreted) and a moderate effort (basic phrases or sentences used).
Potential Determinants Associated With SDM
Table 3 shows the results of the multilevel analysis and the determinants associated with SDM for each OPTION 5 item. Potential determinants were the professionals themselves (on total SDM rates and individual items), composite consultations and consultation duration. Composite consultations are consultations in which multiple and sometimes unexpected or unplanned issues or complications were discussed. These consultations have a significantly higher degree of observed SDM for the total SDM rate and for Items 1 and 2. Consultation duration is significantly related to Items 1 and 3, indicating that longer consultations have a higher degree of observed SDM for these items.
Factors Associated With Shared Decision Making Observations per OPTION 5 Item and Total OPTION5a

CI, confidence interval; COPD, chronic obstructive pulmonary disease; OPTION 5 , observing patient involvement in decision-making instrument; SE, standard error.
Significant differences are printed in bold where P < .05.
Composite consultations are consultations in which multiple and sometimes unexpected or unplanned issues or complications were discussed in addition to the index problem.
Assessing Health Care Professionals’ Perspectives on Their Own SDM
To illustrate categories and patters that emerged during analyses, multiple quotes were used. Themes and quotes are presented in Table 4.
Themes and Illustrative Quotes by Health Care Professionals From the Stimulated Recall Interviews

SDM, shared decision making.
Varying Degrees of Involving Patients in SDM
In the process of involving patients in SDM, all professionals in the interviews described themselves as advisors; varying degrees of involving patients could be identified from that outlook. The most limited involvement of patients occurred when professionals only proposed one option to the patient and asked them to approve it. This is indicated in Quote 1 (see Table 4), in which a female pulmonologist reflects on a preselected video fragment from the consultation and is asked whether the decision was made together with the patient. In another variation of limited patient involvement, the professional’s proposal was framed as their preferred decision. In Quote 2, a female radiotherapist/oncologist reflects on a fragment and was asked the same question as indicated in Quote 1; whether the decision was made together with the patient. Nevertheless, some professionals who presented patients with only one option tried to involve their patients by using another question for requesting approval. In Quote 3, a female pulmonologist reflects on a fragment and was asked the same question as indicated in Quotes 1 and 2. At the other end of the gradient, one professional reported a lot of patient involvement. In this example, the patient in the video fragment asked a male pulmonologist for a medical examination that, according to the professional, was irrelevant for treatment policy, as is indicated in Quote 4.
Perceived Barriers to Involving Patients in SDM
Multiple barriers to involving patients in SDM were identified by the professionals in the interviews. The first is marked by the requirements and necessities of treatment protocols that professionals are bound to adhere to. In Quote 5, after reflecting on a fragment, a male pulmonologist is asked whether the decision was made together with the patient. Furthermore, a male pulmonologist who emphasizes his role as an expert in SDM and does not seem to support the concept of SDM also mentioned time constraints in outpatient clinical practice as barriers. These represent the second and third barriers, respectively, as indicated in Quote 6. A fourth barrier to involving patients in SDM reported by professionals is that they are unable to make patients understand the severity of their condition and, as a consequence, are unable to focus on SDM, unable to elicit the real preferences of patients, or focus on solving the wrong problems. According to the professionals, the reasons for patients’ lack of understanding were the imbalance between hope and reality and/or the patient’s conscious or subconscious denial of their condition or prognosis. In Quote 7, a male pulmonologist reports not being able to really discuss urgent matters with the patient, and therefore continues to discuss and make decisions about less important issues. In another example presented in Quote 8, and after asking a female pulmonology resident what she thought of the way the patient talked to her in the fragment, she indicated to be unable to get the patient to talk about herself and therefore found it difficult to elicit preferences for treatment. As a consequence, she had to decide while knowing too little about the patient.
Recommendations to Involving Patients in SDM
The professionals’ recommendations for involving patients in SDM were to discuss all options, to allow time for patients to talk during consultations and to think about when to involve patients in SDM. According to professionals, even when they proposed only one option to a patient and asked for their approval, treatment goals and reasons for this must be clear. Professionals reported that it is important to discuss the available options with patients thoroughly, and to make sure that decisions are made based on a mutual understanding. This is indicated in Quote 9, in which after reflection, a male pulmonologist was asked whether the decision was made together with the patient. Furthermore, during the interviews, professionals recommended mentioning and explaining all available options to patients, even when some of them were not yet applicable or necessary in the disease progression. Professionals mentioned that the reason for this is to create awareness for patients of what might come in their disease progression and to not ignore prior knowledge of patients about some of the options. According to the professionals, this could possibly encourage patient involvement in SDM at that particular moment and when options become necessary later on. In Quote 10, after reflection, a female radiotherapist/oncologist was asked whether the decision was made together with the patient, in which she demonstrates the importance of explaining to patients why options were not yet applicable. Furthermore, in order to improve patient involvement in SDM, the professionals recommended leaving enough space and time for patients to talk during the consultations (e.g., when discussing sensitive subjects such as “do not resuscitate” decisions). Last, because patients do not remain consistent in their preferences, even after the decision is made to stop offering curative treatment, the professionals interviewed recommended involving patients in SDM during all the consultations in their disease pathway. One female radiotherapist/oncologist reported that patients sometimes change their preferences when problems occur, as indicated in Quote 11.
Discussion
This study provides insights into SDM in practice with LHL patients in the palliative phase of their disease and from the perspectives of professionals. Overall, the results of this study show that SDM is applied by professionals on average to a moderate extent. Compared to SDM scores in oncological settings in the Netherlands, with an average SDM rating of 35, 34 the average SDM score of 40 in this study was comparable, showing that improvement is needed. 60 The multilevel analyses and the interviews in this study showed that SDM is implemented heterogeneously across professionals and care domains in palliative care. This demonstrates that SDM is not yet fully implemented in everyday clinical practice.
This study also found that Item 2 in the OPTION 5 instrument is the least observed item (see Table 1 for the items). Future interventions or research in this setting should focus on improving this particular element of SDM, as SDM for LHL patients is already challenging.11,13,15,16 In addition, as LHL patients are known to be more passive during SDM than health-literate patients, are less inclined to take control during the conversation and are prone to follow the advice suggested by their physician, additional support from their professional is required for effective SDM.61,62
In addition to indicating a heterogeneous implementation of SDM, the multilevel analyses showed that composite consultations and consultation duration are potential determinants for SDM as well. A higher degree of SDM was observed when additional problems or complications were discussed during the consultation. Perhaps the assessment of the additional problem or complication increases the overall involvement of the professional with the patient and, in turn, increases SDM. Also, we observed a higher degree of discussing the problem and providing information for associated options by professionals when consultations were longer. This could indicate that more time facilitates SDM. Although the interviews with professionals indicated time constraints as a barrier for involving patients in SDM, more research is needed investigating the exact role of time in SDM and additional contextual factors associated with it. 36
The interviews showed that professionals perceived SDM as proposing one option and asking the patient for their approval, which is in fact not SDM.4–6 That professionals did perceive this to be SDM underlines their limited understanding of the concept and the varied implementation of SDM in practice. This will negatively affect the application of SDM by professionals for all patients in palliative care. On the other hand, and underlining the varied implementation, some professionals offered recommendations to involving patients in SDM, such as substantiating and mentioning options, timing of information and allowing space and time. These additional recommendations could be used as best practices in future interventions or research, and could help improve the implementation of SDM for all patients.
The requirements of complying with a treatment protocol, limited support for the concept of SDM, time constraints, and the inability of making patients understand the severity of their condition were perceived barriers for involving patients in SDM. Future research should investigate the organizational and interventional opportunities hospitals have for additional training or schooling opportunities for their professionals. 63 These opportunities could increase support for SDM and enhance the ability of professionals involving patients in SDM. Also, they could enhance their ability of having deeper conversations with patients about death and dying and nonmedical aspects of palliative care.
During the observations of cancer and COPD consultations using the OPTION 5 protocol, 49 differences between the two types of diseases were found. On the one hand, COPD consultations generally involved the discussion of a more diversified range of options, focusing solely on alleviating symptoms (e.g., undergoing physical or rehabilitation therapy, prescribing antibiotics or morphine, or adopting a healthier lifestyle). On the other hand, cancer consultations generally involved the discussion of more treatment-oriented options available (e.g., deciding on immunotherapy, chemo or no treatment). From a methodological perspective, these differences made it difficult to determine an adequately uniform index-problem that is needed to assess SDM, and in turn, construct the overall assessment of SDM in palliative care consultations. Further research should elaborate on the possibility of using the OPTION 5 instrument for merging different disease- and decision-types, and the influence of this on the overall assessment of SDM. Furthermore, another difference in context emerged through the conduct of professionals in SDM: during COPD consultations, some professionals tried to improve the decisions of patients by “beneficent persuasion.” 64 For instance, they urged the patient to stop smoking or to do rehabilitation therapy. This could have influenced SDM and patient involvement in these consultations and should be investigated in future research.
An important strength of this study was assessing SDM in practice, and discussing it with professionals. Both analyses pointed in the same direction, which enhances their validity. Furthermore, real-life video-recorded consultations were collected, increasing the ecological validity of the results found in this study. Also, we focused on a hard-to-reach population of LHL patients in the palliative phase of their disease, a subgroup not yet thoroughly investigated.
Despite these strengths, some methodological considerations should also be discussed. In addition to how it is applied by professionals, SDM also depends on patient characteristics and the context of the consultation. 65 Considering this, the relatively small number of hospitals and consultations included (4 hospitals and 36 video-recorded consultations) and the explorative research design could lead to reduced external validity in our study. In future research, when assessing SDM, more hospitals and video-recorded consultations should be included to increase the external validity. Furthermore, a majority (70%) of the consultations included in this study were follow-ups. This means that patients and professionals have had prior conversations that could include elements of SDM. Although the OPTION 5 protocol includes the rating of utterances related to prior conversations by professionals, 49 it is possible that professionals forget to relate to prior consultations during the consultations included in this study. This could indicate an overall underestimation of SDM using the OPTION 5 instrument. Future research should experiment with observing SDM during multiple consultations between one patient and professional in order to more accurately assess SDM (i.e., assess SDM relevant to the different stages in the disease experience of patients 66 ). In addition, in some cases, there was discrepancy between patients’ and professionals’ assessments of the patient’s level of health literacy for including patients in this study. This could be related to the fact that LHL patients often hide that they do not understand health information because they are ashamed, or because LHL is also found in people with medium or high levels of education.16,31 When this occurred, expert opinion prevailed, yet future research is needed to investigate the validity of the opinion of the expert in assessing LHL. Also, the OPTION 5 instrument only measures the assessment of SDM by professionals in practice; it is not a comprehensive measure for the overall quality of communication. 40 Although the aim of our study was to assess SDM, and the OPTION 5 instrument is suited for this, other elements could have affected communication and should be measured as well to evaluate the overall quality. Assessing affective communication in consultations or the professionals’ responses to cues and concerns of patients, for instance, could create additional valuable understanding.10,67 Last, in future research, the time between the initial video-recording and interview should be reduced. This way, participants are better able to recall the consultation and associated perspectives on communication. We recommend to schedule interviews as soon as video recordings are confirmed.
The results of this study show that SDM is applied by professionals to a moderate extent and implementation is varied. This indicates that improvement is needed, as enhanced SDM more effectively addresses the needs of patients and improves patient autonomy and patient-centeredness for the most vulnerable in society.
Supplemental Material
sj-doc-1-mpp-10.1177_23814683211023472 – Supplemental material for Shared Decision Making in Practice and the Perspectives of Health Care Professionals on Video-Recorded Consultations With Patients With Low Health Literacy in the Palliative Phase of Their Disease
Supplemental material, sj-doc-1-mpp-10.1177_23814683211023472 for Shared Decision Making in Practice and the Perspectives of Health Care Professionals on Video-Recorded Consultations With Patients With Low Health Literacy in the Palliative Phase of Their Disease by Ruud T. J. Roodbeen, Janneke Noordman, Gudule Boland and Sandra van Dulmen in MDM Policy & Practice
Footnotes
Acknowledgements
The authors would like to thank the participating hospitals, professionals, and patients for their cooperation. We would also like to thank Wietske van der Hoeven for collecting the video recordings, Peter Spreeuwenberg for conducting multilevel analyses, and Tessera Translations (Mike Wilkinson) for the language editing.
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support for this study was provided entirely by a grant from the Netherlands Organization for Health Research and Development, Palliative Care Program—ZonMw (Palliantie: 844001403). The funding agreement ensured the authors’ independence in designing the study, interpreting the data, writing, and publishing the report.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.