
Abstract
The Centers for Medicare and Medicaid Services (CMS) has mandated shared decision making (SDM) using patient decision aids for three conditions (lung cancer screening, atrial fibrillation, and implantable defibrillators). These forward-thinking approaches are in response to a wealth of efficacy data demonstrating that decision aids can improve patient decision making. However, there has been little focus on how to implement these approaches in real-world practice. This article demonstrates how using an implementation science framework may help programs understand multilevel challenges and opportunities to improve adherence to the CMS mandates. Using the PRISM (Pragmatic Robust Implementation and Sustainability Model) framework, we discuss general challenges to implementation of SDM, issues specific to each mandate, and how to plan for, enhance, and assess SDM implementation outcomes. Notably, a theme of this discussion is that successful implementation is context-specific and to truly have successful and sustainable changes in practice, context variability, and adaptation to context must be considered and addressed.
Evidence-Based Patient Decision Aids (DAs) Are Mandated but Not Widely Adopted
Patient-centered care is increasingly recognized as important for both practical and political reasons. As a primary process of involving patients directly in their care, shared decision making (SDM) is explicitly supported by the Institutes of Medicine 1 and the Affordable Care Act. 2 The Food and Drug Administration has recently begun the Patient Preference Initiative, which incorporates the patient perspective into regulatory decision making, 3 and SDM is considered part of the approval process for new drugs and devices. Recently, the Centers for Medicare and Medicaid services (CMS) has instituted requirements for SDM with the use of DAs as a condition of reimbursement for lung cancer screening, left atrial appendage closure (LAAC) device placement, and implantable cardioverter defibrillators (ICD; Table 1).4–6
Recent Policy Decisions Mandating Shared Decision Making

ICD, implantable cardioverter defibrillator; LAAC, left atrial appendage closure; LDCT, low-dose computed tomography; NVAF, nonvalvular atrial fibrillation.
DAs are evidence-based tools to potentially improve quality of patient-centered care and communication. A Cochrane review of 105 randomized trials concluded that DAs can improve patients’ knowledge, satisfaction, patient/clinician communication, increase patient involvement in decision making, and reduce patient decisional conflict and regret. 7 DAs are available in many forms including paper, video, 8 interactive web sites, 9 and even telenovelas. 10 However, despite their efficacy in controlled trials, DAs have seldom been adopted into real-world clinical practice. A recent systematic review of DA implementation identified a host of logistical barriers, including clinicians’ perception of time necessary to use DAs, lack of reimbursement, and perceived bias inherent in the DAs themselves. 11 Indeed, the lack of understanding of how to implement DAs in clinical practice has led some to call the CMS mandates premature. 12
SDM is a process in which patients and physicians collaborate to make decisions based on the best available evidence of the likelihood of risks and benefits, taking into account patient preferences. While DAs can support SDM especially in information exchange (or delivery), the use of a DA alone does not ensure that quality SDM will occur. Many DAs are publicly available, meaning that patients can review the DA independently of an encounter with a physician. Patients who review a DA may choose to decline a screening or intervention without talking to their clinicians. If a DA is used simply to fill a “checkbox” to meet the CMS mandate, and the clinician reverts to less patient-centered styles of communication without discussing patients’ preference and values, then SDM has not been achieved. Thus, a major gap exists between these mandates for DAs and real-world implementation of quality SDM—and this is a major criticism of the mandates from clinicians. 12 The goal of this article is to consider recent mandates from the perspective of the Practical Robust Implementation and Sustainability Model (PRISM) framework—to explore and address issues in translating mandates for SDM and DAs into widespread clinical practice. 13
Implementation Science as a Bridge Between Research and Practice
Implementation science can help address the gap between research and practice.14,15 Implementation science has multiple conceptual frameworks, strategies, and measures that can be utilized to plan, support implementation, enhance sustainability, and evaluate the process and outcomes of strategies to implement SDM interventions. 16 Which frameworks, implementation strategies, and assessment procedures are used depends on the problem, context, and especially the fit among the intervention, the context, and the implementation strategies. 17
The PRISM13,18 framework is a lens to clarify the issues involved in planning for implementation, and to guide efforts to evaluate SDM interventions and DAs. PRISM is an expansion of the more widely known Reach, Effectiveness, Adoption, Implementation and Maintenance (RE-AIM) framework 19 to evaluate contextual factors, process, and outcomes of efforts to translate research into practice. We selected PRISM because this framework focuses on key factors important to—and measures of—implementation success, is intuitive, and emphasizes the importance of attending to the fit between the evidence-based intervention, the implementation strategy, and how they link context to outcomes. 18
In brief, PRISM focuses attention on several key contextual factors that influence program implementation, process, and outcomes. These factors, listed in Table 2, include the following: 1) the intervention (implications for both organizational and patient perspectives); 2) multilevel recipients (both organizational- and patient-level characteristics); 3) implementation and sustainability infrastructure; and 4) external environment (including guidelines, policies, and reimbursement issues).
Contextual PRISM Domains and Related Shared Decision-Making Issues

CMS, Centers for Medicare & Medicaid Services; DA, decision aid; DOAC, direct-acting oral anticoagulant; ICD, implantable cardioverter defibrillator; LAAC, left atrial appendage closure; LAAO, left atrial appendage occlusion; PRISM, Pragmatic Robust Implementation and Sustainability Model; SDM, shared decision making; USPSTF, US Preventive Services Taskforce.
The contextual factors in PRISM are hypothesized to determine the five RE-AIM implementation outcomes discussed below (Table 3). Relying on a framework like PRISM at the initiation of an implementation experience and then using it in the planning, implementation, evaluation, and dissemination (if appropriate) phases can enhance implementation success while simultaneously advancing the science by allowing implementation strategies to be linked to larger constructs. 20 Local contexts are different, change over time, and need to be addressed with appropriate adaptations to ensure continuing fit with context and culture.21,22 This is a key tenet of implementation science and contrasts with the usual focus on complete fidelity to the original protocol and all components of the evidence-based intervention. Adaptations occur throughout the implementation process, including during the planning, delivery, evaluation, and sustainability phases 23 ; and implementation science can help understand, assess, and potentially guide such adaptations to make them more effective.
Outcomes of the PRISM Framework (RE-AIM) for Planning and Evaluation
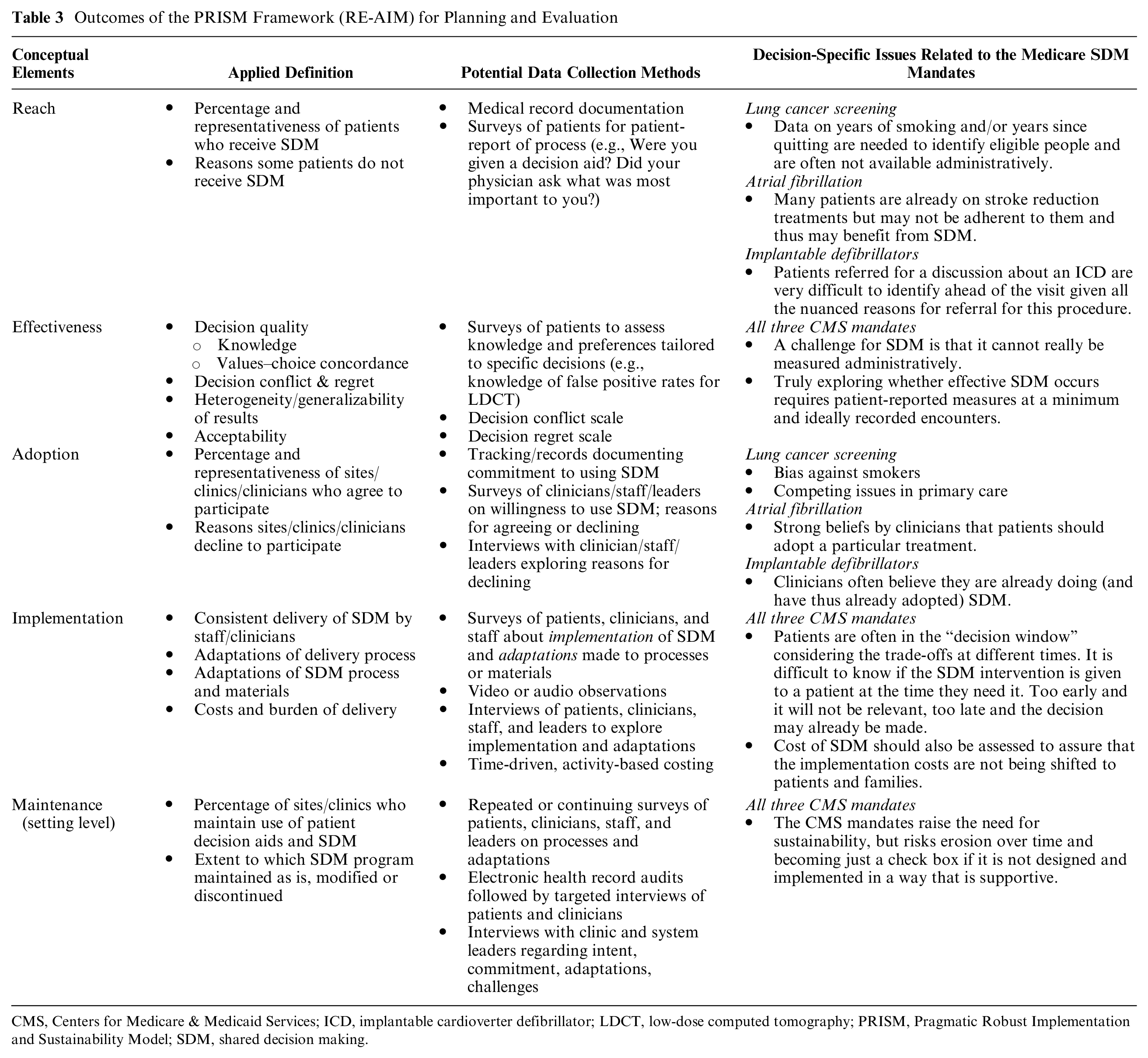
CMS, Centers for Medicare & Medicaid Services; ICD, implantable cardioverter defibrillator; LDCT, low-dose computed tomography; PRISM, Pragmatic Robust Implementation and Sustainability Model; SDM, shared decision making.
The PRISM Lens Can Enhance Success in Implementing SDM and DAs
This section illustrates how the domains of the PRISM framework can be utilized to enhance the implementation and sustainability of the recent policy mandates to utilize DAs for facilitating SDM (Table 2 and Figure 1).

PRISM logic model of implementation of a shared decision-making program.
PRISM Contextual Domain: Intervention
One important underrecognized opportunity to improve implementation is in the design of the DAs themselves and selection of DA to meet the needs of patients, clinicians, and each clinical setting. While the International Patient Decision Aid Standards Collaboration has done excellent work advancing design features to make DAs effective from the standpoint of patient education and value-choice concordance, these standards have not been translated into design features that make them feasible and easy to use in a variety of real-world clinical settings. Different decision contexts need different DA designs. 24 It is conceivable that patients may be willing to watch a longer video-based DA before a high-stakes procedure like an implantable defibrillator or a LAAC device, while they may want a much shorter, encounter-based DA to go over with their clinicians during the visit regarding a decision to take anticoagulation medications to prevent stroke or to get a test for lung cancer screening. Depending on patients’ characteristics, some patients may require assistance to use a web-based DA. Different types of clinicians providing SDM counseling to patients during the encounter have different needs, which should be acknowledged and built into DAs to enhance clinician adoption. DAs must be designed with input from all end-users and must be designed with understanding of the context within which they will be implemented. 25 From the organization’s perspective, it would be important to communicate the evidence base of offering counseling and SDM visits, and to engage clinicians in DA development or selection to help increase the readiness of clinicians to integrate counseling and SDM within their existing clinical workflow. From the patient’s perspective, it would be important to ensure that the process of counseling and SDM with the use of DA is patient centered, address patient-level barriers, and minimize the burden and costs, as well as incorporate more general health communication principles such as responding to emotions that may arise and managing uncertainty. 26 Since development of DAs itself is extensive work and involves field testing of DAs with patients and providers, peer review by patients and experts in the field who are not involved in development or field testing of DAs, thinking about development of DAs from implementation point of view and adding a few more stakeholders such as a hospital leadership or IT in this process is small additional work that will allow DAs to be widely used in a real world. DAs are living documents, and one way to defray the costs is to do some of this evaluation postimplementation allowing the DA to be adapted over time to meet the needs of end-users.
Another intervention and “fit” issue is whether adequate time for SDM discussions is built into the system. Time is one of the most frequently cited barriers to use of SDM in order to meet these mandates.27,28 Systems need to make time in already busy clinical schedules for this work or they need to empower other clinical staff such as nurses to help initiate these conversations with patients. This may be enhanced with system-wide efforts to increase SDM usage and ultimately leading to culture change. How the DAs are made available is also important. An encounter-based DA that is not easily accessible in the clinical visit is unlikely to be adopted, implemented consistently or sustained. Likewise, a self-administered DA that is difficult to access will not be used by patients prior to a visit. Limited access to DAs could be partially solved by user-centered designed health informatic support. Finally, health care systems can further support clinicians by investing in training on essential communication skills and provide feedback on the patient-centeredness of their communication strategies.
PRISM Contextual Domain: Multilevel Recipients
At the organizational level, obtaining clinical leadership and management support, instituting systems and training for clinicians, and ensuring adequate staffing is critical to enhancing the implementation and sustainability of counseling and SDM in a clinical workflow. A major barrier to implementing SDM is overcoming clinicians’ beliefs that they know how to do SDM and that they are already doing it. 27 One strategy that is often used but ineffective is telling clinicians that they are doing a poor job communicating with patients and that they should use a DA to improve their communication. 12 A better approach is acknowledging that clinicians are striving to provide excellent care to their patients and that communication can be difficult. This framing of DAs as an intervention to help and that DAs are designed support challenging discussions may be more successful. Also, direct feedback from patients regarding their preferred role in decision making and their current understanding of the decision may be additional data to help clinicians engage in SDM discussions. Furthermore, reassuring clinicians that DAs are not meant to undermine their relationship or replace discussions with their patients is also an important strategy when implementing DAs. At the patient level, individual patients have differing levels of health literacy, numeracy, internet access, or ability to utilize online patient education resources (including DAs). In addition, patients may experience vision, hearing, and cognitive issues. Therefore, the delivery of DAs and SDM visit should address these patients’ specific needs but tailoring DA to individual patient needs is challenging, and is typically not done. 29 Clinicians seeking to tailor their approach to SDM for different patients have had limited guidance. Additionally, there are usually also larger organizational-level factors such as culture, implementation climate, 30 emphasis on profit, and volume requirements to preserve the ability to perform certain procedures. These organizational concerns can also be strong influencers of whether an organization supports SDM.
PRISM Contextual Domain: Implementation and Sustainability Infrastructure
An important and unique element of PRISM is the attention to the importance of the implementation and sustainability infrastructure built into a system to increase chances of long-term maintenance. As applied to DAs and SDM, there are several structural considerations for health care systems to help create a culture supportive of SDM such as job descriptions and onboarding (for new staff to be trained in SDM), performance assessment procedures, incorporation into workflow, ongoing audit and feedback, and adequate financial and other resources that influence levels of successful implementation and long-term sustainability. Additionally, much of SDM could be easily implemented through telehealth, which is rapidly gaining traction as we adjust to the COVID-19 pandemic.
PRISM Contextual Domain: External Environment
There is an ever-increasing external pressure for the care provided to patients to be more patient-centered. 27 The increased influence of patient experience measures and the surge in the number of patient advocacy groups is strong evidence of this changing expectation of health care. 31 This shift is now represented in professional society guidelines, which increasingly call for greater inclusion of SDM in patient care. 32 Perhaps the strongest external environment motivator of implementation is linking the behavior to payment—indeed the motivation behind this article is to discuss the implementation of new CMS mandates, which require documentation that SDM has occurred for reimbursement. While clinicians reactions to these mandates has been mixed, 12 the fact that they exist has intensified the discussions about how to make SDM occur.
Specific Issues Related to Each Individual Mandate
The CMS mandates provided no discussion of implementation and organizational context or guidance on how they should be implemented. Each mandate also included unique challenges as viewed through the PRISM lens (see Table 2).
Lung Cancer Screening
CMS has mandated that patients receive counseling and SDM with the use of a DA prior to receiving a low-dose computed tomography (LDCT). The SDM visit is reimbursed by CMS separately from LDCT for lung cancer screening. The counseling and SDM visit should include several elements listed in Table 1. 4 From a PRISM perspective, this is a complicated, multimodal intervention. The first challenge unique to lung cancer screening is in identifying screening-eligible patients, as doing so requires a detailed smoking history. Building a system in a clinical workflow that accurately identifies lung cancer screening eligible patients will offset some of the burden from clinicians. Several lung cancer screening DAs have been developed; several have been evaluated and most were found to be acceptable to patients and improve decision outcomes. Some lung cancer screening DAs result in improved patient knowledge, and reduce decisional conflict.33–35 However, most studies evaluated DAs in a research setting outside of a real-world clinical workflow and these DAs likely need to be adapted and simplified for implementation in low-resource primary care settings health systems serving diverse patient populations, or in low-resource settings such as rural clinics or federally qualified health centers. CMS left the decision of which DA and how to use it in a clinical workflow to clinicians and health systems. From a recipient perspective, as patients are either current or former smokers, the counseling including tobacco cessation (or sustained abstinence) and the SDM visit should be sensitive, avoiding exacerbating smoking-related stigma and lung cancer worry in this population. Likewise, primary care clinicians are expected to play an important role in these discussions and many may not be well informed of the detailed risks and benefits of lung cancer screening. 36
Finally, from an implementation and sustainability infrastructure perspective, many primary care practices are not prepared or structured to engage in and support SDM about lung cancer screening with patients. 37 While much of the literature on SDM focuses on the primary care setting, 37 a number of alternative approaches have been considered and some have been tested. The Cleveland Clinic tested an alternate model, where primary care clinicians referred potentially eligible patients to a central lung cancer screening program to conduct the counseling and SDM visit. 38 Telephone counseling for SDM may hold promise as a way of supporting busy clinicians without burdening patients with the need for an additional visit, although CMS currently mandates that SDM occur during an in-person visit.39,40 To improve implementation of this mandate, clinicians need clarity about coverage of LDCT screening, tools for patient education, and engaging in SDM. Effective implementation toolkits and training for all frontline staff potentially involved would increase the readiness for primary care clinicians to implement SDM around lung cancer screening. 37 Incorporation of SDM into office flow and staff performance expectations would enhance probability of sustainment and allow the program to reevaluate and adopt the process when external environmental factor changes such as COVID-19 pandemic. With COVID-19 pandemic and significant uptake of telemedicine, CMS mandates of in-person SDM visit needs to be revisited and telehealth SDM counseling needs to be reimbursed to continue providing quality SDM.
Atrial Fibrillation Stroke Reduction
With respect to stroke prevention in patients with atrial fibrillation (AF), the external environment is quite strong as SDM is recommended by professional guidelines, 41 is an endorsed quality measure, 42 and is mandated by the CMS National Coverage Determination (NCD) for LAAC (Table 1). However, the state of SDM in AF is poor. Significant gaps exist in patients’ knowledge about the risks and benefits of stroke reduction options, 43 and patients often report a paternalistic decision-making process with their clinicians. 44 From an intervention perspective, there are several DAs for stroke reduction options; however, few include the LAAC device—which is the specific context in which the mandate exists. From a recipient perspective, clinicians who perform LAAC procedures have been frustrated by the mandate that the SDM discussion must occur with a non-proceduralist clinician. 12 This also creates a challenge from the perspective of multilevel recipients and the implementation and sustainability infrastructure. The NCD for LAAC explicitly states that the SDM conversation used to meet the mandate must be conducted by a “non-interventionist physician,” thereby tying reimbursement for an eventual procedure to a conversation that occurred with a different clinician. This creates a constellation of misaligned incentives and complications, including the implication that proceduralist physicians who ultimately care for patients are more likely to inappropriately guide them toward having a procedure.45,46 By alienating proceduralists, who typically oversee the operations of specialty electrophysiology and interventional cardiology practices, this requirement reduces the likelihood that the mandate would be adhered to in an earnest manner. To improve implementation of this mandate, clinicians need tools that support conversations for stroke reduction that are easy, tailored to local context, and feasible to use and implement both in primary and specialty care, and the incentive for the SDM discussion needs to be better aligned with the clinician who is actually doing the discussion as opposed to the “non-interventionist” language discussed above.
Implantable Cardioverter Defibrillators
The current NCD addressing reimbursement for ICD therapy for primary prevention of risk of sudden cardiac death involves decision-specific features which influence the design and implementation of patient decision support processes. From an intervention perspective, the requirement includes documented use of an “evidence-based” DA as part of the patient education process. While the NCD links to one such tool as an example, the language itself does not describe a list of approved DAs or a process by which to assess whether other ones are “evidence based.” From a multilevel recipient perspective, there is no agreement among clinicians that defibrillators are a preference sensitive decision—believing that the benefits in survival outweigh any harms. Consequently, using a DA risks being a “check box” on the path toward a paternalistic recommendation to perform a procedure. Patients likewise hear words like “sudden cardiac death” and may resort to making decisions based on uninformed or emotional heuristics. 47 As such, implementing this CMS mandate requires extra attention directed toward clinicians. Considering intervention and implementation and sustainability infrastructure perspectives, tools need to be designed in a way that not only helps patients make decisions but also delivered in a context so that clinicians are willing to use them and that fits their environment, staffing, and workflow.
Evaluation: RE-AIM Outcomes as Applied to SDM (Table 3)
The PRISM framework was built upon the RE-AIM framework to add the important contextual elements described above. Table 3 presents the five core concepts of the RE-AIM evaluation framework as applied to SDM. The conceptualization is relatively straightforward—the challenge lies in identifying data collection methods, data elements, and instruments that are feasible, acceptable, and support valid inferences. The PRISM elements in Table 2 are conceptualized as affecting these implementation outcomes. For instance, Reach (i.e., the number, percentage, and representativeness of patients who receive SDM) requires accurate identification of all eligible patients, and determination of whether SDM was delivered to each patient. For lung cancer screening an important eligibility criterion, pack years, is not consistently captured in the electronic health record, limiting an organization’s ability to evaluate Reach. The challenges inherent in measuring the SDM process has led some evaluators to focus solely on outcomes (see Effectiveness in Table 3). A primary focus has been decision quality, which includes both knowledge and values/choice concordance. Knowledge is typically measured using objective questions to document understanding of objective information related to the specific decision. However, there is no accepted standard defining the minimum level of knowledge or key information that the patient must understand to be considered “informed” about the decision. The measures used to assess knowledge related to a given decision vary across studies, precluding direct comparisons of DAs’ effectiveness. 48 Simply providing information is no guarantee that comprehension has occurred. Values and preferences, which are subjective, may be unstable or conflicting, making the determination of values/choice concordance more complex. Decision regret and decisional conflict are also important SDM outcomes, but patient responses on these measures may be influenced by factors other than effectiveness, such as trust in the physician or experiencing surgical complications from the medical procedure.47,49
A challenge in evaluating SDM Adoption or spread of SDM is that multiple levels must be considered: clinicians are nested within clinics which are in turn nested within organizations or health care plans, and adoption at any one level does not ensure adoption at another. Furthermore, to fully understand adoption decisions, evaluators must explore reasons for supporting or opposing adoption at each level. Evaluating Implementation is also challenging. Ideally, Implementation would be assessed by observing actual clinician-patient encounters, determining whether a DA was used, whether the clinician provided critical information (e.g., the need for annual screening), and whether the patient’s values and preferences were considered. While capturing what happens during encounters is possible, such efforts are resource intensive and often not feasible in practice. Assessing Implementation through electronic health record documentation is risky, as time constraints, reimbursement contingencies, and other factors may tempt clinicians to document that SDM has occurred even if most elements are absent, as one recent study suggests. 36 Patients can be queried about their recall of the decision-making process, but the patient-clinician relationship, memory, and other factors may influence their responses. 50 Patient surveys are more feasible than observing or recording encounters, but they still require resources. Additionally, when measuring implementation, it is also important to assess fidelity, costs, and adaptation. It is a well-documented implementation science fact that interventions are seldom if ever delivered as conducted in efficacy trials. 22 Adaptations will happen, and it is important to assess them rather than ignore them. 51 Maintenance (or sustainment) refers to sustained efforts to continue an intervention; thus, evaluation of maintenance requires repeated or continuous assessment of implementation. The methods and instruments used to assess initial adoption and implementation are also relevant for assessing maintenance. In addition, forward-looking interviews with leaders exploring commitment, intent to continue, and actual or anticipated adaptations and challenges are needed to fully understand whether efforts to implement SDM are truly successful.
Conclusion
This article stresses the importance of thoughtfully implementing and disseminating SDM interventions by considering conceptual models from implementation science. The PRISM framework emphasizes contextual factors, the importance of fit, and implementation science issues and measures in real-world applications. Having a model like PRISM can help with planning and evaluation of SDM programs and policies.18,19 PRISM is not the only IS framework that could be applied. We chose this framework because of the relative ease for nonresearchers to understand (compared to many other implementation science models) the RE-AIM implementation outcome components and because PRISM intentionally focuses on a smaller, specific set of specific contextual factors that affect the RE-AIM outcomes. Many other models exist and have been applied to SDM and DAs including normalization process theory, 52 and the Consolidated Framework for Implementation Research (CFIR). 53 This article presents one example of the promise of the more general issue of integrating implementation science and health communication disciplines into planning, execution, and evaluation of health care programs and policies.
Considering the importance of context at multiple levels is particularly important for SDM and DAs in that context varies not just among clinical settings but also across different decisions in terms of the difficulty in understanding, the urgency, and the fatefulness of the decision. 24 All of these factors can have different impacts on different implementation outcomes. Integrating SDM and implementation science provides guidance on the way to address the ubiquitous problem of lack of implementation of evidence-based SDM and on the importance of “fit” among an (SDM) intervention, the implementation setting, and the implementation strategies to deliver the intervention. This approach should be helpful for both researchers and practitioners to conceptualize, reflect on, and anticipate key contextual issues.
Future research should compare PRISM-guided implementation of SDM to implementation without such guidance to identify which PRISM elements are most important for successful implementation and suitability in which settings and at what phase in the process from planning, implementation, evaluation, sustainability, and adaptation. Additionally, DA developers should understand and address the tension between designing DAs that maximize effectiveness versus DAs that maximize pragmatic and population health issues of reach, adoption, implementation, and sustainability.20,25 As CMS considers additional mandates to support SDM, they should also consider how best to support and facilitate implementation. Notably, they should carefully consider the pros and cons of mandating specific delivery elements such as having an “independent noninterventional physician” be mandated to do the SDM as in the case of LAAC or “in-person SDM visit” as in the case of lung cancer screening. CMS could stimulate implementation by being more explicit about which subset of decisions they are considering these mandates for and what constitutes an “evidence-based” DA. Finally, CMS could assist DA developers and implementers by explicitly allowing (and reimbursing for) SDM to occur through telehealth, which has rapidly become more common as the world adjusts to the COVID19 pandemic. Indeed, given the multiple barriers to overcome, perhaps the greatest effect of these mandates so far has been to spur implementation in a way that likely would not have occurred otherwise.
Footnotes
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Knoepke is supported by a career development award from the American Heart Association. Dr. Ito FuKunaga served as a volunteer board member of the American Lung Association in Maine. The other authors have no conflicts of interest to disclose.
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support for this study was provided in part by a National Heart, Lung and Blood Institute (R01 HL136403) grant and the National Cancer Institute (P50 CA244688) grant. The funding agreement ensured the authors’ independence in designing the study, interpreting the data, writing, and publishing the report.