
Abstract
Keywords
Throughout history and across cultures, tattoos and other methods of body modification have been used as a means of representing one’s identity to the world. Ross identified several themes in which tattoos play a role in the lives of the transmasculine community; tattoos that relate to one’s transgender identity, tattoos that serve as a means of permanence, tattoos that exist as a form of therapy, tattoos that exist as a form of storytelling, tattoos that serve as a reclamation of one’s body, and tattoos that are used as a tool of visibility. Tattoos that can relate to transgender identity include the date that the individual started testosterone or other artwork that represents significant milestones in one’s transition. Tattoos can be viewed similar to medical transitioning by some patients, as both are viewed as permanent changes to one’s body and therefore connected. 1
In addition, tattoos may serve as a permanent reminder of a person’s experience. For some patients, the act of getting a tattoo may be therapeutic. In some instances, the tattoo can symbolize a specific moment of adversity that the individual was able to overcome. In other instances, the process of being tattooed and the pain that is associated can be viewed as a cathartic experience. Some transmen have stated that their tattoos exist as a form of telling their story. These tattoos may signify an important moment in one’s life or represent loved ones who are no longer with them. For many individuals who have struggled with gender dysphoria, tattoos can often be a method of reclaiming their body and establishing a sense of control. Finally, some people may choose to have their tattoos in more visible areas, such as the forearms, as a way to portray a specific message about their identity to the public. 1
Phalloplasty Flap Options
While several phalloplasty flap options exist, the radial forearm free flap (RFFF) has emerged as the most frequently used surgical technique for phalloplasty in the transmasculine community. The RFFF phalloplasty is done as a single- or multistage procedure in which a fasciocutaneous flap is harvested from the patient’s nondominant forearm. The procedure utilizes a “tube within a tube” configuration where the ulnar aspect of the flap creates the neourethra and the remainder constructs the penile shaft. There are several reasons why the RFFF is preferred. The RFFF provides a long, predictable, and reliable vascular pedicle that has been shown to reduce the rate of complications when compared to other flaps. The tissue is quite unique because of its anatomical properties. It is not only pliable, which allows this type of design, but it also carries a robust sensory supply, which increases the possibility of establishing tactile and erogenous sensations of the neophallus. The RFFF also confers a greater degree of functionality with micturition and penetrative intercourse while providing an aesthetic result for the patient. 2 According to a systematic review, the RFFF carries the lowest rate of serious complications, such as total flap loss, of any phalloplasty flap. 3
However, despite the preferred use of the RFFF, it still has several disadvantages. There is significant morbidity associated with the donor site including an identifying scar that can be problematic for those who do not wish to be identified as transgender. Additionally, a decrease in manual dexterity, pronation at the wrist, and radial nerve sensation have been observed postoperatively in some RFFF donor arms, thus making the nondominant forearm preferable. 4 In addition, due to surgical restrictions on flap design, the surgeon’s ability to reconfigure the orientation of the flap to conceal or protect an existing tattoo is very limited.
Beyond the use of a RFFF, there are several other acceptable flap choices for phalloplasty including an abdominal flap, latissimus dorsi flap, groin flap, and anterolateral thigh flap. The abdominal flap is a pedicled flap that utilizes the epigastric vessels. This flap procedure does not include neurorrhaphy, limiting the sensation of the neophallus, and it also does not allow a tube within a tube design. In addition, the anatomic variation of epigastric vessels and limitations in functionality have rendered this flap choice less than ideal. The latissimus dorsi flap is a free muscle flap that uses the thoracodorsal neurovascular bundle. 3 While this flap provides a less noticeable scar than RFFF, the major drawback is the significantly decreased sensation 5 and poor cosmetic outcome. Groin flaps are pedicled flaps that are based off the iliac vessels. Similar to the abdominal flap, they are less than ideal given their lack of sensation and decreased functionality compared to more modern flaps. 3 The anterolateral thigh flap can be done as either a free or pedicled flap. Given the increased adiposity of the thigh, this flap is limited by the body habitus of the patient and is often reserved for patients who are not a good candidate for RFFF due to a negative Allen test (incomplete palmar arch). 6 These considerations are all in addition to the previously noted higher complication rates. 3
Aim
For some transmasculine patients, tattoos carry significant importance, and therefore, those patients may prioritize maintaining the integrity of that tattoo over a medically optimized flap choice. The aim of this study is to understand the prevalence of forearm tattoos among transmasculine patients seeking phalloplasty and how the presence of tattoos affects decision making about the donor flap. The ultimate goal is to improve the ability of patients and surgeons to engage in shared decision making around flap choice.
Methods
Participants included in the study consisted of the first 50, consecutive, adult (≥18 years of age) transmasculine patients presenting for a phalloplasty consult at Boston Children’s Hospital in Boston, Massachusetts. The presence and location of tattoos along with the motivation for preservation were assessed by review of consult notes in the electronic medical record, as were decisions about donor flap choice. For each patient, two notes were reviewed—one from the team physician and one from the team social worker—both from the initial consult. Both social work and physician notes are partially templated and include information about the dominant arm, tattoo presences, and flap choice as a matter of course. Physician notes consistently document reasons for any flap choice other than the nondominant arm, as the nondominant arm is always preferred in our Center. Maintaining this documentation is critical to managing the informed consent process.
Data were abstracted by a single reviewer into a structured abstraction table. Where data were missing from the electronic medical record, it was noted in the table. A one-tailed test of proportions was used to test the hypothesis that forearm tattoos increase the likelihood that patients will choose an alternative flap. This retrospective chart review was declared exempt by the Boston Children’s Hospital Institutional Review Board (P00031525), and no external funding was received for this study.
Results
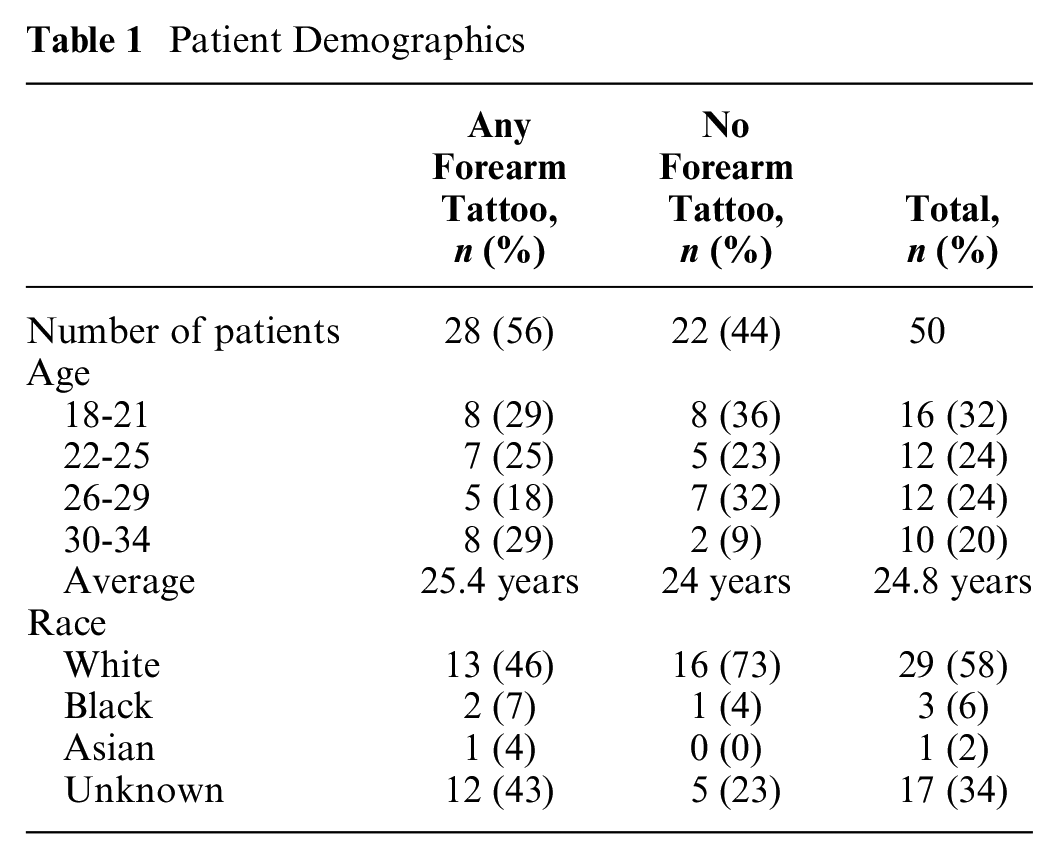
Of the first 50 patients who had a consultation for phalloplasty at Boston Children’s Hospital, the average age was 24.8 years (Table 1). Racial data were missing for approximately one third of patients, 58% were White, 6% were Black, and 2% were Asian. Fifty-six percent had a tattoo or multiple tattoos on either one or both of their forearms (n = 28). Of these patients, 75% had a tattoo on their nondominant arm (n = 21). There was no statistically significant difference in age between patients with a forearm tattoo and patients without a forearm tattoo (P = 0.31). Among patients with forearm tattoos, the presence of tattoos was noted as affecting the flap site decision for 46% (n = 13). All affected patients had at least one tattoo on their nondominant arm. Two patients with tattoos only on their nondominant arm had expressed to providers that their tattoo placement supported the use of the preferred flap, but this was not categorized as affecting flap choice.
Patient Demographics
For patients who chose a flap site other than their nondominant forearm, 46% chose a RFFF using their dominant arm (n = 6) and 54% chose an anterolateral thigh flap (n = 7). Overall, 46% of all consult patients with tattoos (n = 13) were recorded as stating that they would choose an alternative flap site due to the presence of a forearm tattoo. This was significantly higher than the 18% of patients without tattoos (n = 4) choosing an alternate flap (P < 0.01). No records from patients with tattoos indicated the desire to choose an alternative flap site was due to the visible scar of the donor site. Among the reasons for choosing an alternative flap site for individuals with tattoos, preservation of the tattoo due to personal meaning was the most common recorded reason (n = 10; Table 2, Figure 1).
Results

ALT, anterolateral thigh; RFFF, radial forearm free flap.

Sankey diagram of how tattoos affected graft choice.
Discussion
Presence of Tattoos Affecting Flap Choice
Reviewing the charts of the patients with tattoos, 46% had clinician notes indicating that the presence of their forearm tattoo(s) affected their flap site decision, either from a desire to preserve the tattoo or to prevent the presence of a tattoo on the neophallus. This led to the patients choosing either an alternative flap or using their dominant arm for a RFFF. Alternative flaps confer a potential increased risk of serious complications, such as flap loss, relative to the standard RFFF. Similarly, the use of the dominant arm in a RFFF carries an increased risk of impairing the mobility and sensation necessary for certain activities of daily life. 3
In the majority of cases, flap choice is driven by the goal of preserving an emotionally important tattoo. Ideally, providers from all disciplines working with transmasculine patients should counsel prospective phalloplasty patients on the impact of tattoo placement and on the cosmetic outcome of the neophallus early in their transition. For those who desire a meaningful tattoo, this information may help them choose an alternative location for tattoo placement. However, for patients who already have a meaningful tattoo on their nondominant arm, there is a need to engage in shared decision-making processes to help patients balance the risks of alternate flap choices with the importance of maintaining the integrity of their tattoo. Rather than imposing a hierarchical model of informed consent, shared decision making has been shown to improve patients’ sense of autonomy and satisfaction with outcomes, including with respect to gender affirming care.7,8 That is particularly important in cases like this, where nonmedical factors may lead to choices that are seen as less optimal from a medical perspective.
Use of Laser Tattoo Removal in Phalloplasty
Alternate flap choice is not always related to preservation of a meaningful tattoo. In some cases, flap choice is instead driven by the desire to not have a potentially problematic or unaesthetic tattoo appear on the phallus. For these individuals, there is some question about the feasibility of tattoo removal prior to gender affirming phalloplasty. A potential disadvantage of using laser tattoo removal prior to surgery is how the quality of the flap tissue may be affected. Unfortunately, there is a dearth of literature describing the use of laser tattoo removal in the preoperative setting for gender affirming phalloplasty.
Similarly, there is no evidence regarding the impact or feasibility of laser tattoo removal on the neophallus in the postoperative setting. One concern is trauma to the flap tissue following the photothermolysis of the ink and the resulting edema, particularly given the limited vascular supply and drainage of the neophallus. Indeed, it is unclear if postoperative laser tattoo removal would even be effective given the increased difficulty of ink clearance in locations with decreased or no lymphatic vasculature, such as the donor flap. Further studies are needed to assess both risks and efficacy of laser tattoo removal in this population.
Additionally, laser tattoo removal can pose an enormous burden with regard to both a delay in surgery and increased financial expense. One study showed that the average number of laser treatments needed to remove a tattoo was 10, with a range of 3 to 20. 9 The recommended time between laser removal sessions is 8 weeks, 10 which can result in an estimated length of removal of 6 months to several years. According to the Cosmetic Surgery National Databank Statistics by the American Society for Aesthetic Plastic Surgery, the average cost per session of laser tattoo removal is $401, 11 which based on the average of 10 sessions, can cost upwards of $4000, imposing a massive financial burden for phalloplasty patients who choose this option. This is in addition to the significant financial barriers already faced by patients, who need to complete hair removal on the flap prior to surgery, an expense that is often not covered by insurance. 12
Limitations
This exploratory study was designed to assess whether and how tattoo placement affects flap choice in transmasculine patients. Our study had several limitations. It was based on medical record abstraction rather than directly interviewing patients about their reasons for flap choice, something that could benefit from additional, qualitative research. Our population was also both relatively young and racially homogeneous. In addition, because our team only offered the options of RFFF and anterolateral thigh phalloplasty, other flap choices were not available that may have been preferable to some patients. Despite this, we believe that this study raises an important concern for how nonmedical factors can affect decision making around phalloplasty procedures. It also has important implications for practice with transmasculine patients. Our research indicates the importance of having conversations about how tattoo placement can affect long-term gender affirmation goals early in a patient’s transition—long before they present for an initial consult for gender affirming surgery. Education of primary care providers and even pediatricians may be advantageous as those providers are often not familiar with genital reconstructive options and their preoperative requirements. Tattoo artists who work with transmasculine patients may also benefit from education that forearm tattoo placement may pose a future concern for some of their clients.
Conclusion
The RFFF, harvested from the nondominant arm, is the most commonly used flap for gender affirming phalloplasty, as well as the flap associated with the fewest complications.2,3 More than half of transmasculine patients seeking phalloplasty at Boston Children’s Hospital had tattoos on either one or both of their forearms. In many instances, the presence of a tattoo on the proposed flap site led to the patient deciding to use either their dominant forearm or an alternative flap. Providers working with transmasculine patients early in their transition, especially in a primary care setting, should inform them about how tattoo placement may affect their ability to use the preferred donor flap, should they be interested in undergoing gender affirming phalloplasty in the future.
Footnotes
Acknowledgements
The authors acknowledge the work of Haley Chrisos, PA-C, in assessing and documenting the tattoo histories of these patients.
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support for this study was provided entirely by the Center for Gender Surgery, Boston Children’s Hospital. The funding agreement ensured the authors’ independence in designing the study, interpreting the data, writing, and publishing the report.
Author Contributions
Travis A. Benson performed the analysis and wrote the first draft of the paper. Elizabeth R. Boskey helped design and supervised the analysis and revised and edited the paper. Oren Ganor supervised the project and revised and edited the paper.