
Abstract
Introduction
Health literacy refers to one’s ability to access, understand, and use health information to make informed health decisions.1–4 Low health literacy has been associated with numerous health outcomes including increased hospitalizations and emergency room visits, low uptake of the influenza vaccine, medication nonadherence, poor overall health status, and even increased mortality. 5 Measuring health literacy can help researchers improve knowledge of its impact and develop interventions to mitigate its effects. However, there are many ways to measure health literacy and no universally accepted gold standard for doing so. 6 In addition, the performance of health literacy measures among younger, healthier adults has not been thoroughly explored.7,8
Many health literacy measures require interviewers to administer them in-person or by telephone.9,10 In contrast, subjective health literacy measures allow individuals to self-report their perceptions of how easy or difficult it is for them to engage with health material. 11 For example, the Single Item Literacy Screener (SILS) differentiates between limited and adequate health literacy by asking patients to self-identify how often they need help in reading instructions, pamphlets, or other written material from their doctor or pharmacy. 12 The Subjective Literacy Screener (SLS) includes three items and asks patients to self-identify how often they need help reading health materials, how often they have problems reading health materials, and how confident they are filling out health forms. 13 The brevity and ease of administering these subjective health literacy measures make them useful to include in clinic settings and/or on surveys to reduce participant burden. Both were validated against widely used objective health literacy measures.12,13
However, the SILS and SLS were developed more than 10 years ago in a middle-aged and older population, before the common use of online health information and forms.12,13 As many as 96% of hospitals and 87% of physicians report using electronic health systems14,15 for tasks such as patient communication. Health literacy measures that ask individuals how often they need help reading health information and completing health forms might not be taking into account new modes of delivery of this information. Young adults are more likely than older adults to use online sources for health or medical information. 16 They demonstrate more ease with technology, and they are more skilled at completing online forms compared to older adults. 17 A young adult population may self-report adequate health literacy skills on these measures because they respond to these measures about reading health materials and filling out health forms assuming electronic health information. Alternatively, some young, healthy adults might report lower skills if they do not have experience with health forms, instructions, or pamphlets; compared to middle-aged or older adults, they might not engage with the health care system without health conditions requiring ongoing maintenance. 18 Thus, the current wording of each measure might not discriminate between adequate and limited health literacy in younger, healthier populations.
The goal of the current study was to examine how well two commonly used subjective health literacy measures (SILS and SLS) perform in a young adult population. Because there is no “gold standard” health literacy measure, we included two measures. We chose these measures because of their strong relationship to objective health literacy measures, and their ease of administration, making them feasible to implement in research and clinical settings.19,20 We hypothesized that among young adults, a modified version of the SILS and SLS that included “online” to describe health information, health forms, and pamphlets would perform better than the original wording, or than wording specifying “paper-based.” We anticipated this relationship given the increasing use of electronic health information, which might lead to more familiarity and comfort learning about information in this manner, and the potential for more specialized or personalized information from electronic forms that can be updated and referenced over time. Specifically, we expected that the subjective health literacy measures that added “online” to their wording would be significantly associated with factors relating to health literacy (i.e., objective and subjective numeracy, electronic health literacy, comprehension, and education).
Materials and Methods
Participants
Eligible participants were English-speaking young adults ages 18 to 35, residing in the United States, with access to an internet-administered survey. The study was deemed exempt by the Human Research Protection Office at Washington University in St. Louis (Protocol Number 201906007) based on the 2018 Common Rule Exempt Categories (45 CFR 46.104) (2) Tests, Surveys, Interviews).
Procedure
We recruited individuals through an online survey sampling company, Dynata. Dynata has an actively managed pool of participants who have signed up to participate in surveys, and are incentivized with a point system that can be redeemed for rewards. Dynata recruits based on variety of demographic factors including age, gender, location, and interests. Participants received $1.25 or the equivalent value as compensation from Dynata for completing the survey. Recruitment for the current study was open for one day in June of 2019 to reach a target enrollment of 1,000 participants. The study was funded with institutional funds; no external support was received.
We randomized participants to one of three study conditions: 1) the original SILS and SLS; 2) a modified version of the SILS and SLS that added the word “online” to describe health information, health forms, and pamphlets; or 3) a modified version of the SILS and SLS that added the word “paper-based” to describe health information, health forms, and pamphlets. We included measures that we expected to relate to health literacy such as validated numeracy measures, a validated electronic health literacy scale, a knowledge assessment after participants read a short passage about genetics and skin cancer, and demographic characteristics such as age, gender, race, ethnicity, and education.
Measures
Single Item Literacy Screener
The SILS asks patients to self-identify how often they need help in reading instructions, pamphlets, or other written material from their doctor or pharmacy. 12 This measure has been validated against a widely used measure of objective health literacy (the Short Test of Functional Health Literacy in Adults [S-TOFHLA]). 21 Response options are reported on a 5-point Likert-type scale. Scores of >2 are considered limited, scores <2 are considered adequate.
The modified versions of the SILS added either the words “on paper” or “online.” The paper-wording version read, “How often do you need to have someone help you when you read instructions, pamphlets, or other written material on paper from your doctor or pharmacy?” The online-wording version read, “How often do you need to have someone help you when you read instructions, pamphlets, or other written material online from your doctor or pharmacy?”
Subjective Literacy Screener
The SLS assesses health literacy using three items. 13 This measure has strong internal reliability and was validated against the widely used Rapid Estimate of Adult Literacy in Medicine (REALM). Response options are reported on 0- to 4-point scale; scores are summed and range from 0 to 12, where higher scores indicate greater difficulty with health literacy. The modified versions asked the questions in the same way as the original, but added either the words “on paper” or “paper-based,” or “online” to the three items (Appendix A). The paper-wording version of the SLS read, “How confident are you filling out paper-based medical forms by yourself?”; “How often do you have someone help you read hospital materials on paper?”; and “How often do you have problems learning about your medical condition because of difficulty reading hospital materials on paper? The online-wording version of the SLS read: “How confident are you filling out online medical forms by yourself?”; “How often do you have someone help you read hospital materials online?”; and “How often do you have problems learning about your medical condition because of difficulty reading hospital materials online?”
Comprehension
Comprehension was assessed by providing a short passage about genetics and skin cancer risk, which was created for a young adult population. We chose this topic since it is likely unfamiliar to young adults22,23 so we could better assess knowledge learned from the passage. Five items were included to assess comprehension, with true, false, or unsure response options. The percent of correct responses were calculated, with higher percentages indicating greater comprehension. Appendix B shows the five-item measure that was informally tested with lay volunteers for clarity.
eHEALS
The eHealth Literacy scale (eHEALS) assesses consumers’ combined knowledge, comfort, and perceived skills at finding, evaluating, and applying electronic health information to health problems. 24 The eight items include response options on a 5-point Likert-type scale, from 1 (strongly disagree) to 5 (strongly agree). Scores are summed and range from 8 to 40; higher scores indicate lower eHealth literacy.
Subjective Numeracy Scale
The 8-item Subjective Numeracy Scale measures a person’s self-reported ability and comfort working with numeric information; it is scored on a 6-point Likert-type scale. Scores are summed and averaged, ranging from 8 to 48, with higher scores indicating higher subjective numeracy. This measure significantly correlates with objective numeracy scales.25,26
Objective Numeracy Scale
We used an 8-item validated objective numeracy scale 3 to measure participants’ quantitative skills. The measure requires mathematical calculations and asks participants to respond using open text. The percentage of correct responses is reported with higher percentages correct indicating higher objective numeracy.
Participant Characteristics
Participants answered questions about their age, gender, residence, language, ethnicity, race, education, income, health insurance, use of health care services, and delay of health care.27,28 Health conditions were reported by selecting all that apply from a list of the most common health conditions as described in the Medical Expenditure Panel Survey and modified from our previous work.29,30 They could also list other health conditions in an open text response field, if applicable.
Data Analysis
We included an attention-check item in the survey to preserve data quality; individuals who correctly responded to the item were included in analyses. Individuals were also included if they spent >5 minutes answering the survey, as it was not feasible to complete the survey in less than that time frame. Analyses were conducted using R software, version 3.5.2. Descriptive statistics were calculated for continuous and categorical variables. Independent samples t tests examined the relationship between the SILS and SLS and our continuous outcomes (eHEALS, comprehension, subjective numeracy, objective numeracy). Chi-square analysis examined relationships between SILS and education, and SILS and health condition status. ANOVA examined the relationship between SLS and education, and a t test examined the relationship between SLS and health condition status. Separate multivariable linear regression models examined SILS and SLS and continuous outcomes, controlling for the presence of health conditions (any v. none). Separate multivariable logistic regression models examined SILS and SLS and education, controlling for the presence of health conditions (any v. none).
Results
Of the 1341 participants who responded to the survey, 966 participants responded correctly to the attention-check item. Data from the 375 individuals that failed the attention-check question were excluded. Sixty-six individuals were excluded because they did not meet the age eligibility for the study (i.e., between 18 and 35 years). Individuals who completed the survey in less than 5 minutes (N = 52) were excluded because it was not feasible to provide meaningful answers to the survey in that timeframe. The final sample included 848 participants. Figure 1 shows a CONSORT flow diagram.

CONSORT study flow diagram.
Table 1 displays demographic characteristics of participants. Participants’ mean age was 26; 66.4% were white, 14.3% were black, 19.3% were another or multiracial. Most (61.7%) had at least one health condition. There were no significant differences in participant characteristics between randomized groups.
Participant Characteristics (N = 848)

Table 2 displays the bivariate analyses examining SILS and outcomes. Approximately the same number of participants were categorized as limited versus adequate in each condition. The original wording of the SILS related to comprehension (t = −3.04, P = 0.003), eHEALS (t = 2.09, P = 0.037), and ONS (t = −3.85, P < 0.001) but not SNS (t = −0.77, P = 0.440). The paper-wording version only related to eHEALS (t = 4.06, P < 0.001) and ONS (t = −3.02, P = 0.003) but not comprehension (t = −1.15, P = 0.250) or SNS (t = 0.94, P = 0.347). The online-wording version better differentiated between adequate and limited health literacy, relating to comprehension (t = −4.87, P < 0.001), eHEALS (t = 3.67, P < 0.001), ONS (t = −2.80, P = 0.002), and SNS (t = −2.25, P = 0.025). SILS was not significantly related to education in any of the three versions: original χ2 = 2.137, P = 0.344; paper-wording χ2 = 2.80, P = 0.246; or online-wording χ2 = 3.23, P = 0.199. SILS was also not significantly related to health condition status (any v. none) in any of the three versions: original χ2 = 1.67, P = 0.196; paper-wording χ2 = 1.91, P = 0.166; or online-wording χ2 = 0.45, P = 0.501.
Bivariate Analyses Examining the SILS Original and Modified Wording on Outcomes

eHEALS, e-Health Literacy; M, mean; ONS, Objective Numeracy Scale; SD, standard deviation; SILS, Single Item Literacy Screener; SNS, Subjective Numeracy Scale.
SILS is scored such that a higher value indicates the presence of limited health literacy.
eHEALS scores are summed; higher values indicate lower e-health literacy.
Comprehension and ONS are scored as percent correct. Higher values indicate higher comprehension and higher objective numeracy.
SNS scores are summed and averaged; higher values indicate higher subjective numeracy.
Table 3 displays the bivariate analyses examining SLS and outcomes. The original SLS performed adequately and related to comprehension (t = −0.27, P < 0.001), eHEALS (t = 0.36, P < 0.001), ONS (t = −0.24, P < 0.001), and SNS (t = −0.26, P < 0.001). The paper-wording version only related to comprehension (t = −0.133, P = 0.028) and eHEALS (t = 0.42, P < 0.001), but not ONS (t = −0.09, P = 0.125) or SNS (t = −0.06, P = 0.331). The online-wording version related to comprehension (t = −0.27, P < 0.001), eHEALS (t = 0.41, P < 0.001), and SNS (t = −0.13, P = 0.030) but not ONS (t = −0.11, P = 0.056). The SLS was not significantly related to education in any version: original F = 0.88, P = 0.549; paper F = 0.69, P = 0.741; or online F = 1.34, P = 0.207. SLS was also not significantly related to health condition status (any v. none) in any of the three versions: original t = −0.98, P = 0.327; paper-wording t = −0.55, P = 0.586; or online-wording t = 0.91, P = 0.365.
Bivariate Analyses the SLS Original and Modified Wording on Outcomes
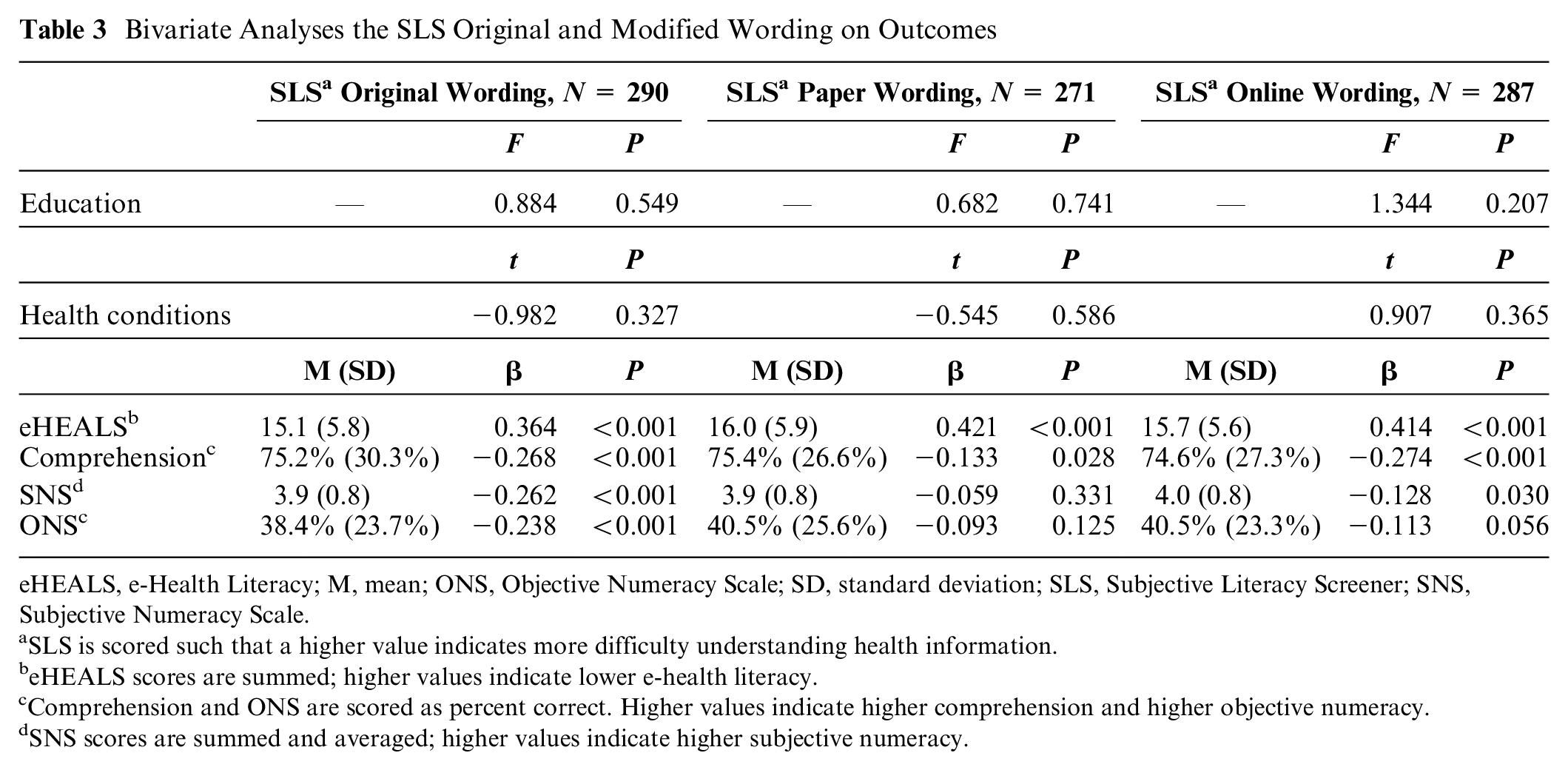
eHEALS, e-Health Literacy; M, mean; ONS, Objective Numeracy Scale; SD, standard deviation; SLS, Subjective Literacy Screener; SNS, Subjective Numeracy Scale.
SLS is scored such that a higher value indicates more difficulty understanding health information.
eHEALS scores are summed; higher values indicate lower e-health literacy.
Comprehension and ONS are scored as percent correct. Higher values indicate higher comprehension and higher objective numeracy.
SNS scores are summed and averaged; higher values indicate higher subjective numeracy.
Results did not significantly change when controlling for the presence of health conditions in multivariable analysis. Table 4 displays the multivariable results for SILS. Table 5 displays the multivariable results for SLS. Results remained the same when controlling for the presence of health conditions in multivariable analysis except the online-wording version of the SLS became significantly related to ONS when controlling for the presence of health conditions (β = −0.04, P = 0.041)
Multivariable Analyses With SILS as a Predictor of Health Literacy Measures and Education, Controlling for the Presence of Health Conditions (Any v. None)

CI, confidence interval; eHEALS, e-Health Literacy; ONS, Objective Numeracy Scale; OR, odds ratio; SE, standard error; SILS, Single Item Literacy Screener; SNS, Subjective Numeracy Scale.
SILS is scored such that a higher value indicates the presence of limited health literacy; the reference group for SILS is “Adequate health literacy.”
The reference group for health conditions (HC) is “No” conditions.
eHEALS scores are summed; higher values indicate lower e-health literacy.
Comprehension and ONS are scored as percent correct. Higher values indicate higher comprehension and higher objective numeracy.
SNS scores are summed and averaged; higher values indicate higher subjective numeracy.
Multivariable Analyses With SLS as a Predictor of Health Literacy Measures and Education, While Controlling for the Presence of Health Conditions (Any v. None)
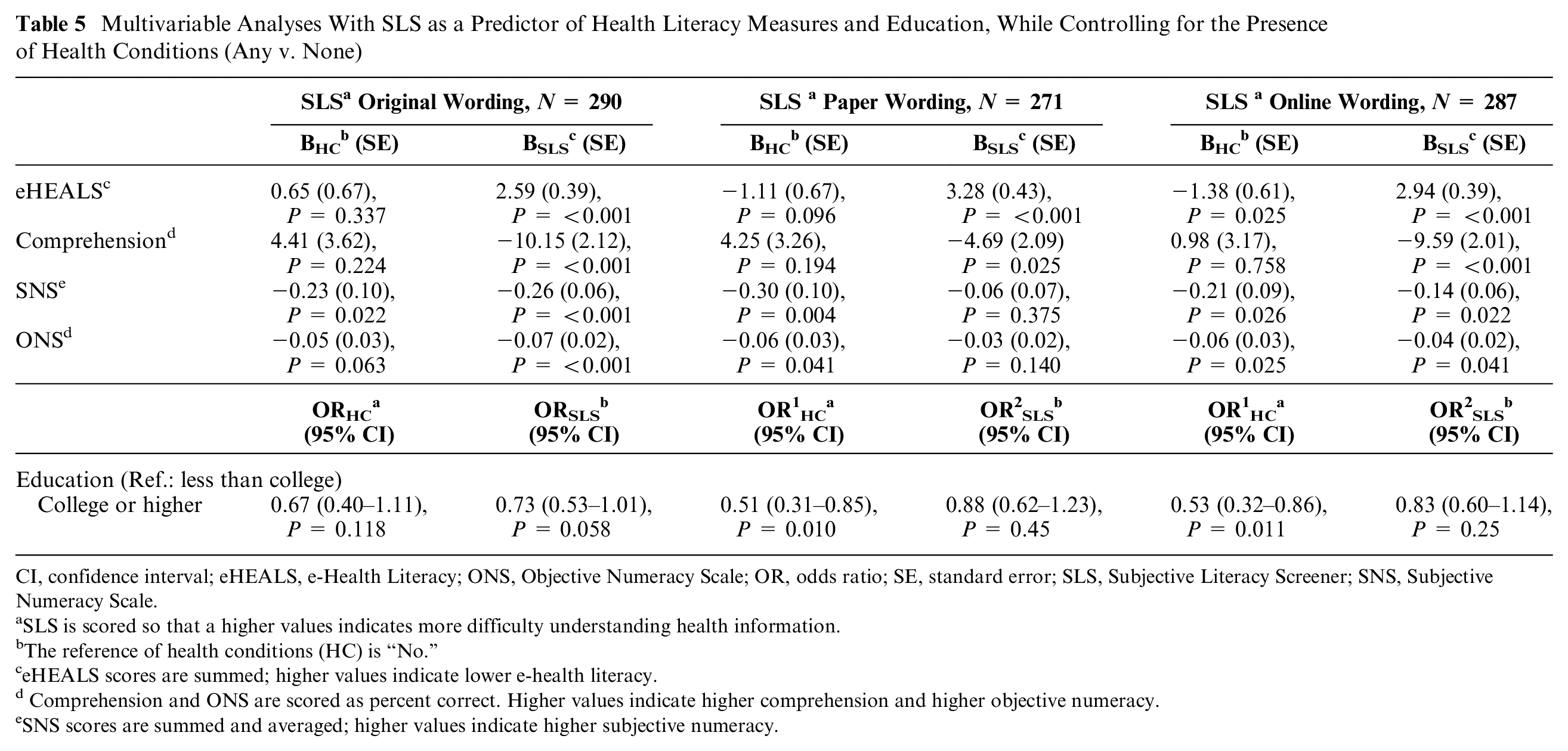
CI, confidence interval; eHEALS, e-Health Literacy; ONS, Objective Numeracy Scale; OR, odds ratio; SE, standard error; SLS, Subjective Literacy Screener; SNS, Subjective Numeracy Scale.
SLS is scored so that a higher values indicates more difficulty understanding health information.
The reference of health conditions (HC) is “No.”
eHEALS scores are summed; higher values indicate lower e-health literacy.
Comprehension and ONS are scored as percent correct. Higher values indicate higher comprehension and higher objective numeracy.
SNS scores are summed and averaged; higher values indicate higher subjective numeracy.
Discussion
This study examined how the SILS and SLS related to objective literacy, numeracy, and comprehension among young adults, and whether specifying “online” or “paper-based” wording affected these relationships. Consistent with our hypotheses, we found that young adults might interpret subjective health literacy measures differently when prompted to think about electronic or paper-based information and forms. The original versions of the measures performed adequately, relating to many of the expected outcomes. However, subjective health literacy measures that added “online” to their wording were significantly and more strongly associated with factors relating to health literacy (i.e., numeracy, electronic health literacy, comprehension) than those that added “paper-based” to the original wording.
These findings suggest that researchers should consider clearer instructions or modified wording when using subjective health literacy measures in a young adult population. Individuals might need to be prompted to think about the delivery platform through which they are receiving health information. It is possible that individuals considering online health information were thinking about searching the internet to understand health or make health decisions, whereas those thinking about paper-based health information considered forms such as intake forms or simple brochures from their clinicians’ office. Research could explore how individuals think about health material as they answer subjective health literacy questions. New or more refined measures that relate to established and validated assessments could be appropriate.
In addition, research could explore how these results apply to other age groups. It is possible that middle-aged and older adults might also interpret the measures differently than they did in the earlier measure validation studies, given the expansion of electronic health records and electronic health communication.
In this study, neither the original or modified versions of the subjective health literacy measures related to education. These results were surprising given the robust relationship between health literacy and education in other work. 31 Measuring education in this population presents challenges because many young adults are still completing their schooling. The education category that reflects their education completion at the time of the survey might not reflect their eventual education attainment. In addition, the population in our study was relatively educated overall without as much variation in educational attainment as one might expect in the larger population. However, there was variation in their numeracy skills, and as expected,19,20 health literacy and numeracy were significantly related across most of the sample when controlling for the presence of health conditions. We were surprised that health literacy and numeracy were not related at the bivariate level, though, particularly in the group viewing the paper wording. Given the complex relationship between health literacy and numeracy showing that they are related but distinct contructs,31–34 future studies could explore this association, particularly among young adults and/or those without wide variation in education.
The presence of health conditions did not relate to health literacy in our study, contrary to our predictions. It is possible that common health conditions in young adults do not require as much chronic disease management as they do among older adults, limiting their exposure to the health care system. It is also possible that among the youngest group in our study (18–26 years of age) who might be covered by a parent’s insurance, a parent completes medical forms on their behalf. Future work should consider the presence and type of health conditions and how they might impact health literacy.
Our findings should be interpreted within the context of some study limitations. We recruited an online sample from a data collection company. Those who take surveys from data collection companies might not attend to all survey questions. 35 To account for this limitation, we included an attention-check item and excluded participants who did not answer this question correctly. We also excluded those who took the survey significantly faster than would be possible if they read each question. Although the young adults were similar to the larger population in terms of race, ethnicity, and income, 36 they were relatively educated and healthy. They might have more familiarity with electronic health information since they were recruited electronically, or they might have less familiarity given that they were relatively healthy. We controlled for chronic condition status in our analyses to account for differences in health literacy based on familiarity with interacting with the health system to manage a health condition. We conducted a cross-sectional survey and cannot draw causal inferences about how health literacy or its measurement impact outcomes over time. Although most of the measures were previously developed and validated, we created a comprehension measure for this study based on previous work. In addition, individuals across groups might have answered “rarely or never” indicating that they rarely or never used health care services, rather than that they “rarely or never” had difficulty with health information. However, over 80% of the population seeks health information online, and young adults more than older adults use electronic sources for health information. 17 In addition, over 90% of our sample used health care services in the past 12 months, with no differences between groups in use. The study could be repeated in-person so that researchers could use both subjective and interview-administered objective health literacy measures to examine whether results were affected by interpretation of the items. Some individuals might have assumed that online sources of information were not sent by a trusted source such as a doctor or hospital. Future studies could include both the source of the information as well as the delivery platform in measures to test this possibility.
Conclusion
Young adults might interpret subjective health literacy measures differently when prompted to think about electronic or paper-based information and forms. Current subjective health literacy measures might not always discriminate between adequate and limited health literacy in younger populations. Results call for future research to replicate these results. If replicated, researchers could consider developing or modifying subjective health literacy measures to account for the format and delivery platform of health information. Clinicians could consider administering the improved health literacy measures to identify how prevalent limited health literacy might be in their practice. They can then use this data to ensure that their clinical materials meet the needs of their clinic population.
Supplemental Material
Appendix_A_online_supp – Supplemental material for How Do Subjective Health Literacy Measures Work in Young Adults?: Specifying “Online” or “Paper-Based” Forms Impacts Results
Supplemental material, Appendix_A_online_supp for How Do Subjective Health Literacy Measures Work in Young Adults? Specifying “Online” or “Paper-Based” Forms Impacts Results by Mary C. Politi, Courtney M. Goodwin, Kimberly A. Kaphingst, Xuechen Wang, Angela Fagerlin, Lindsay N. Fuzzell and Sydney E. Philpott-Streiff in MDM Policy & Practice
Supplemental Material
Appendix_B_online_supp – Supplemental material for How Do Subjective Health Literacy Measures Work in Young Adults? Specifying “Online” or “Paper-Based” Forms Impacts Results
Supplemental material, Appendix_B_online_supp for How Do Subjective Health Literacy Measures Work in Young Adults?: Specifying “Online” or “Paper-Based” Forms Impacts Results by Mary C. Politi, Courtney M. Goodwin, Kimberly A. Kaphingst, Xuechen Wang, Angela Fagerlin, Lindsay N. Fuzzell and Sydney E. Philpott-Streiff in MDM Policy & Practice
Footnotes
Acknowledgements
The authors would like to thank Steven Yoon for assistance with an earlier version of this work.
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Dr. Politi previously (2017–2019) received research funding from Merck on a topic unrelated to this article. The authors have no other conflicts of interest to disclose.
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research was supported in part by the enhancing undergraduate preparation for research in aging and neurological diseases (5R25NS100133-02) grant from the National Institute of Health.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.