
Abstract
Introduction
Lung cancer is one of the most prevalent cancer types in both men and women, and the leading cause of cancer deaths in the United States. 1 An estimated 234,030 new cases of lung and bronchus cancer were diagnosed in 2018, and non–small cell lung cancer (NSCLC) accounted for approximately 85% of these diagnoses.2,3 Due to the asymptomatic nature of the disease in its early stages, nearly 80% of lung cancer cases are diagnosed at a late stage (stage III or stage IV), after the malignant tumor has metastasized to other parts of the body. 4 As such, patients often cycle through multiple lines of therapy in order to effectively minimize disease progression and prolong survival. 5
Given its high disease burden and high unmet need, lung cancer has emerged as a key target for treatment innovation. The last decade has been marked by the introduction of immuno-oncology (IO) therapies, a class of drugs quickly gaining significance in the treatment of cancer in general, and of NSCLC in particular. 6 Pembrolizumab is currently approved for NSCLC as combination therapy in the first-line (1L) setting for all NSCLC patients, as monotherapy in the 1L and second line (2L) setting for patients whose tumors express PD-L1, and as monotherapy in the 2L setting for all patients. Atezolizumab, pembrolizumab, and nivolumab are currently approved as a monotherapy following progression on platinum-based chemotherapy, and atezolizumab is also approved as combination therapy in the 1L setting.7–13 Several additional molecules are in the advanced stages of clinical trials. While IO-IO combinations are recognized as efficacious options, 14 they are often costly and have yet to be approved for the treatment of NSCLC. 15 Beyond clinical efficacy, however, these therapies may possess other attributes that are particularly valuable for patients relative to other combinations, for example, mechanism of action and side effect profile.
In response to the evolving NSCLC treatment landscape, studies in the United Kingdom and Europe16,17 have been published examining patient preferences for novel therapies that vary in their respective modes of administration (MOA), side effects, progression-free survival (PFS), and alleviation of disease symptoms (e.g., pain, coughing, and shortness of breath). In 2012, Bridges et al. found that PFS and symptom alleviation were most important, 16 but that patient preferences for these attributes varied among the small sample of patients surveyed based on the severity of disease symptoms patients had experienced. A discrete choice experiment (DCE) published by Mühlbacher and Bethge in 2015 asked patients about similar treatment attributes, 17 and concluded that a therapy’s ability to extend PFS and reduce tumor-related symptoms were the outcome measures most influential to a patient in the treatment decision-making process. In one study focused on NSCLC patient preferences for chemotherapies, patients reported making their treatment decisions based on the severity of side effects when therapies offered comparable effectiveness. 18 Making cancer treatment decisions requires that patient and providers make tradeoffs between multiple treatment objectives (e.g., maximizing effectiveness and minimizing adverse events/side effects), and the process evolves along with the treatment landscape. In the health care literature, six or fewer attributes are typically included in most DCEs. 19
Cancer treatment decisions are complex and patient preferences are heterogeneous. As the spectrum of innovative treatment options for NSCLC patients continues to expand, it is critical that an informed decision about NSCLC treatment reflects not only what the patient is willing to undergo but also what undergoing treatment will allow the patient to attain or avoid. This study expands on the existing literature by measuring preferences among US patients with advanced NSCLC for emerging 1L treatment regimen options using a DCE, including IO-IO, IO-chemo, and combination chemotherapy regimens. The present study may help inform and improve clinical care delivery by providing evidence for providers on the attributes of 1L NSCLC treatment that are most meaningful and salient for patients making NSCLC treatment decisions.
Methods
Survey Design
Survey design best practices 20 were employed to develop the survey instrument, which consisted of four modules: eligibility screener and treatment history, health-related quality of life (HRQoL), DCE preference elicitation, and demographics. DCEs are widely used in health economics to measure stakeholder preferences for key treatment attributes,19,21,22 willingness to tradeoff between attributes, and preference shares for particular treatment profiles.
Attribute candidates were identified based on distinguishing characteristics of emerging treatment regimen options as well as from previous NSCLC treatment preference studies.16–18 Five key factors were considered in the attribute selection process: (1) relevance of the attribute to patients’ choice of cancer treatment, (2) attribute description complexity and patient comprehension, (3) overlap or correlation with other treatment attributes, (4) relevance to the objectives of the study, and (5) variation in the attribute across currently available cancer treatments. We elicited cancer patient preferences for 1L treatment regimens over six attributes: (1) 2-year survival rates, (2) moderate to severe adverse event (AE) rates, (3) treatment delay associated with genetic testing, (4) mechanism of action (MOA), (5) subsequent treatment options, and (6) out-of-pocket cost (OOPC) per month. Table 1 describes the included attributes and their levels in detail. Mode of administration was not included because most NSCLC treatment regimens include at least one component that is intravenously administered, that is, there were no all-oral treatment regimens considered. Given that this study aimed to evaluate patient preferences over a relatively broad range of treatment options that vary significantly in their attributes and levels, and the need to balance the length of the DCE module against the study objectives, AEs were summarized in one attribute (i.e., moderate to severe AE rate/risk) rather than distinct attributes for different types of AEs with varying levels of severity, as some previous studies have done. 16
Discrete Choice Attributes and Attribute Levels
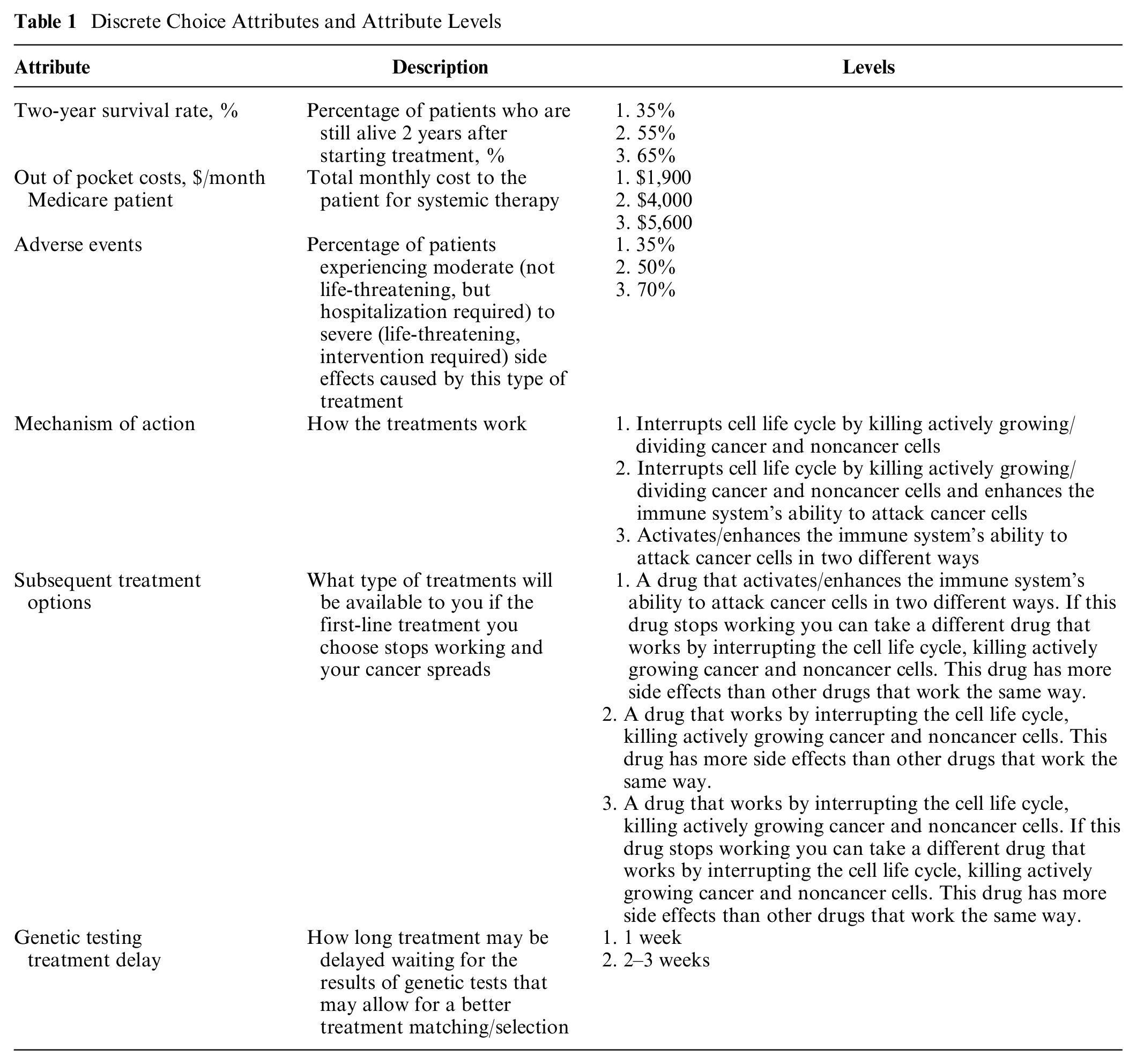
The 2-year survival rates and AE rates attributes were calibrated based on IO-IO-like, IO-chemo-like, and chemo-like clinical trial data. Weekly, monthly, and yearly OOPC of nivolumab, ipilimumab, and platinum doublet chemotherapy were derived from multiplying January 2017 wholesale acquisition costs (WAC) by dosing and length of treatment. Costs for IO-IO regimens were estimated assuming a fixed dose of 240 mg every 2 weeks for nivolumab and 1 mg/kg—or 75 mg for the average patient—every 6 weeks for ipilimumab.15,23 Costs for platinum-based combination chemotherapy regimens were based on estimates used in previous cost-effectiveness analyses. 24 Costs for IO-chemo regimens were based on the combined costs of a fixed dose of 240 mg every 2 weeks for nivolumab and the platinum-based combination chemotherapy regimen costs. Drug administration and adverse event management costs for all regimens were based on estimates used in published cost-effectiveness analyses. 25 Monthly patient OOPC was assumed to be 20% (Medicare Part B co-pay) of the total treatment cost. Two-year survival rates for IO-IO, IO-chemo, and combination chemotherapy regimens in the 1L setting were obtained from the literature.14,26 The percent of patients surviving at least 2 years using IO-IO, IO-chemo, or combination chemo as 1L treatment for advanced NSCLC was rounded to the nearest 5% to facilitate respondent understanding. AE rates were calibrated according to grade 3+ AEs reported in relevant randomized clinical trials for IO-IO, IO-chemo, and combination chemotherapies to treat advanced NSCLC in the 1L setting.7,9,14 The percentage of patients experiencing moderate to severe AEs using IO-IO, IO-chemo, or combination chemo as 1L treatment for advanced NSCLC was also rounded to the nearest 5% to facilitate respondent understanding (Table 1).
The experiment was designed and D-efficiency was estimated using the R routine Design of Experiments. 27 Based on the D-efficiency criteria, we generated a 12 × 4 block experiment design, that is, each DCE survey module included 12 choice questions and respondents were randomly assigned to one of the 4 blocks. In each question, patients faced two unlabeled treatment options (i.e., Option A and Option B) that varied across six different attributes and were asked to choose the treatment option they preferred. The optimally designed experiment contained the first unlabeled treatment option (i.e., Option A) in 12 choice sets. To create the second unlabeled option—Option B—in each choice set, we employed the algorithm developed by Street and colleagues, 28 which systematically alters the level of each attribute in Alternative A in a particular choice set to generate the attribute levels for each attribute in Option B. An example choice set is provided in Figure 1. We chose not to include an opt-out option to prevent patients choosing the opt-out option because it is the least cognitively burdensome choice, rather than reflecting their true preferences, and also because the opt-out option provides no information on tradeoffs between attributes.29,30
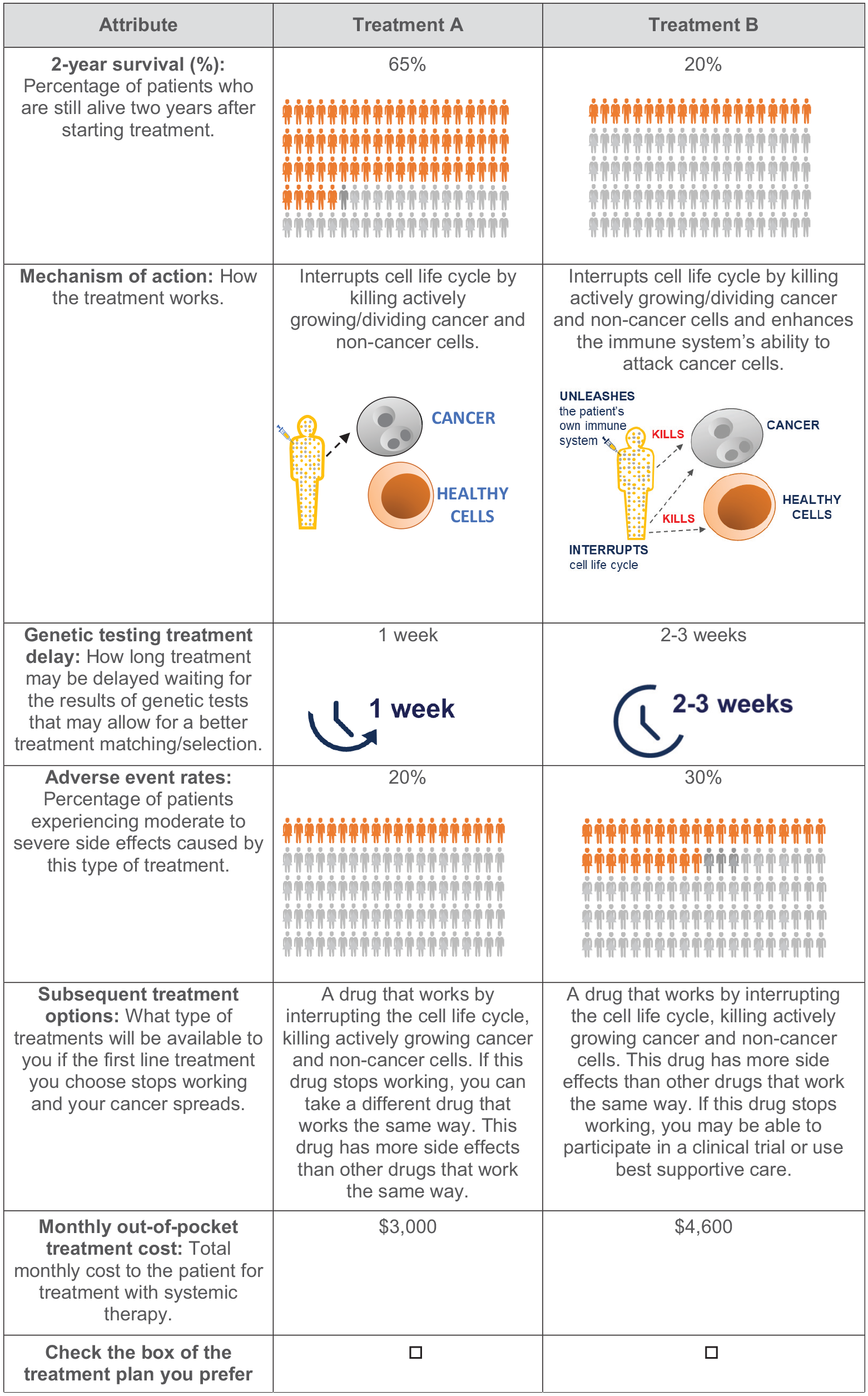
Example choice set.
Survey Population and Administration
Patients at least 18 years of age, fluent in English, with advanced NSCLC (stage III or IV), and residing in the United States were eligible for the survey. While patients in any stage of treatment (e.g., had not started treatment or currently in 2L treatment) were included to allow us to test whether previous lines of treatment influenced treatment preferences, given the objective of this study, there was an emphasis on recruiting patients who were treatment naïve, or were on first-line therapy. In addition, quotas were implemented by age and gender in an effort to reflect the nationwide advanced NSCLC statistics. 4 We aimed to have 10% of the sample be comprised of patients under 50 years of age, 60% be between the ages of 60 and 74, 30% be 75 years of age or older, and 60% be male. The web-based survey was executed in two phases: a pilot and a primary data collection. Before the primary data collection phase, four NSCLC patients participated in the pilot phase. The pilot phase was used to assess the clarity of the survey and to confirm that the survey could be completed in 30 or fewer minutes. The pilot survey was followed by a cognitive debriefing interview. Feedback from participants in the pilot phase resulted in minor editorial changes in the iconography and language used in the survey questions to improve readability.
The primary data collection phase was conducted between November and December of 2018. The objective was to have 200 NSCLC patients from across the United States complete the survey. Orme (2010) 31 suggests a minimum sample size of 94 patients for a DCE with a maximum of three levels for any attribute, two alternatives in each choice set, and a total of eight choice sets. Therefore, our target sample size of 200 patients should be sufficient to estimate the main effect parameters of the random utility model. We engaged a survey vendor to identify and recruit potential participants. Patients with NSCLC from the vendor’s panel of cancer patients received direct email invitations with a link to the survey. Participants were given $30 in remuneration for completing the survey. 32 Western Institutional Review Board reviewed and approved all study procedures (Study Number CA209-506).
Analytic Methods
Using the data collected from survey respondents, we tested for whether patients used decision rules or heuristics to simplify the treatment decision process, that is, choosing the option with the best level of one attribute (e.g., highest survival or lowest OOPC) or always choosing Option A (Option B). Patient preferences were estimated using latent-class and attribute nonattendance models, as well as model and best practices in statistical analyses. 33 The latent class model divides patients into a specified number of classes or groups with similar preferences within classes/groups and simultaneously estimates the probability of belonging to a certain preference class and patient utility weights. 34 Models with and without class membership modeled as a function of respondent characteristics were explored. Two, three, and four preference class models with and without patients who used simplifying decision rules were explored, as well as models with attribute nonattendance—that is, ignoring one or more attributes when choosing between options—for various combinations of attributes. Model fit was evaluated based on the minimum Bayesian information criterion (BIC) statistic. We estimated WTP for each attribute within each preference class and weighted preference/market shares for three 1L NSCLC treatment regimen profiles: IO-IO, IO-chemo, and combination chemotherapy. The weighted market share was calculated as the sum of the product of the within group market share and group share. Supplemental Table 2 contains details on the attribute levels used to calculate the preference shares for each regimen.
Results
Of the 2472 patients who responded to the survey invitation, 1299 (53%) were screened out based on survey eligibility criteria (1028 patients) or possible duplicate responses (271 patients). Another 434 patients (18%) were screened out because quotas for that patient type were full. Finally, 539 (22%) patients started but did not complete the survey and one patient’s data were omitted because they provided inadequate responses to several questions. Of the 199 respondents with responses adequate for analysis, a majority were male (55.0%), white (76.5%), over 40 years of age (57.5%), and had employer provided/privately purchased health insurance (66.5%). It took respondents 29.2 minutes to complete the survey, on average. More than 80% of respondents were diagnosed with stage III or IV NSCLC and 18.5% had not begun or were receiving their first line of treatment. A similar proportion (18%) were currently undergoing their second line of treatment. Twenty-five percent were in their third line of treatment and 24.5% were in either their fourth or fifth line of treatment. Finally, 10.5% were not currently receiving treatment and 3.5% were unsure. Approximately 70% of respondents reported having fair to excellent health and 50% reported that their physical health problems caused little to no limitations to their physical activity. However, nearly one in three patients reported recently experiencing severe or very severe pain. Finally, more patients with EGFR, ALK, and ROS-1 mutant tumors were recruited for this study than are routinely observed, likely due to the relatively young cohort. Selected patient characteristics are summarized in Table 2.
Characteristics of Survey Respondents (n = 199)

The treatment choice patterns of 20.6% of respondents suggested they used a simplifying heuristic/decision rule, either always chose the option with the best level of a particular attribute, or always chose the same option (e.g., Option A). Seventeen percent always chose the option with the best level of a particular attribute (e.g., the highest 2-year survival) and 4.0% chose the same option in all eight choice questions (i.e., they always chose Option A or they always chose Option B).
Figure 2 illustrates the preference class/group shares, and Figure 3 illustrates the estimated utility weights (and 95% confidence intervals) from the preferred model based on a three-class latent class model where class membership was modeled as a function of patient characteristics (sex, age, race, education, employment status, hospice/palliative care, poor self-reported health, treatment for depression, and line of treatment) that included patients who appeared to use simplifying decision rules since we cannot distinguish a priori between a simplifying decision rule and a true preference for attribute nonattendance. Fifty-three percent of patients fell into class/group one, where survival and OOPC were the most important factors in the treatment choice decision and patients were significantly more likely to choose a treatment option with longer survival and lower OOPC (“survival focused” patients). Within this group, patients were willing to pay $73 per month (P = 0.005) for a treatment option offering an additional one percentage point increase in 2-year survival. Roughly 13% of patients fell into preference class/group 2, where patients were more likely to choose the more expensive treatment option and OOPC was the only significant determinant of treatment choice (“cost-seeking” patients). Since OOPC was the only significant determinant of treatment choice, patient were not willing to pay more for treatment options with greater efficacy, lower AE risk, and so on. Thirty-four percent of patients fell into the third preference group where 2-year survival, AE risk, and treatment delay all significantly influenced treatment choice (“engaged” patients). In this group, OOPC was a marginally significant (P = 0.065) predictor of treatment choice and patients were less likely to choose treatment options with higher OOPC. This translated to marginally significant willingness to pay for longer 2-year survival ($1,344 per month per one-percentage point increase, P = 0.057) and reduced AE risk ($207 per month per one-percentage point decrease, P = 0.083). Mechanism of action and subsequent treatment options did not significantly influence treatment choices in any of the three preference classes.

Latent class model preference class shares.

Latent class model utility weights and confidence intervals by preference class and attribute. AE, adverse event; STO, subsequent treatment option; L2, level 2; L3, level 3; MOA, mechanism of action; OOP, out of pocket. Attribute levels are described in detail in Table 1.
Patients under 50 years of age (P < 0.01) and those in 1L or 2L treatment (P < 0.01) were significantly less likely to be survival focused patients (i.e., group 1) than engaged patients (group 3). Women (P < 0.05) and those with poor self-reported health (P < 0.01) were significantly less likely to be cost-seeking patients (group 2) than engaged patients (group 3; Table 3). Race and educational attainment did not significantly influence preference group membership.
Preference Group Membership Predictors a
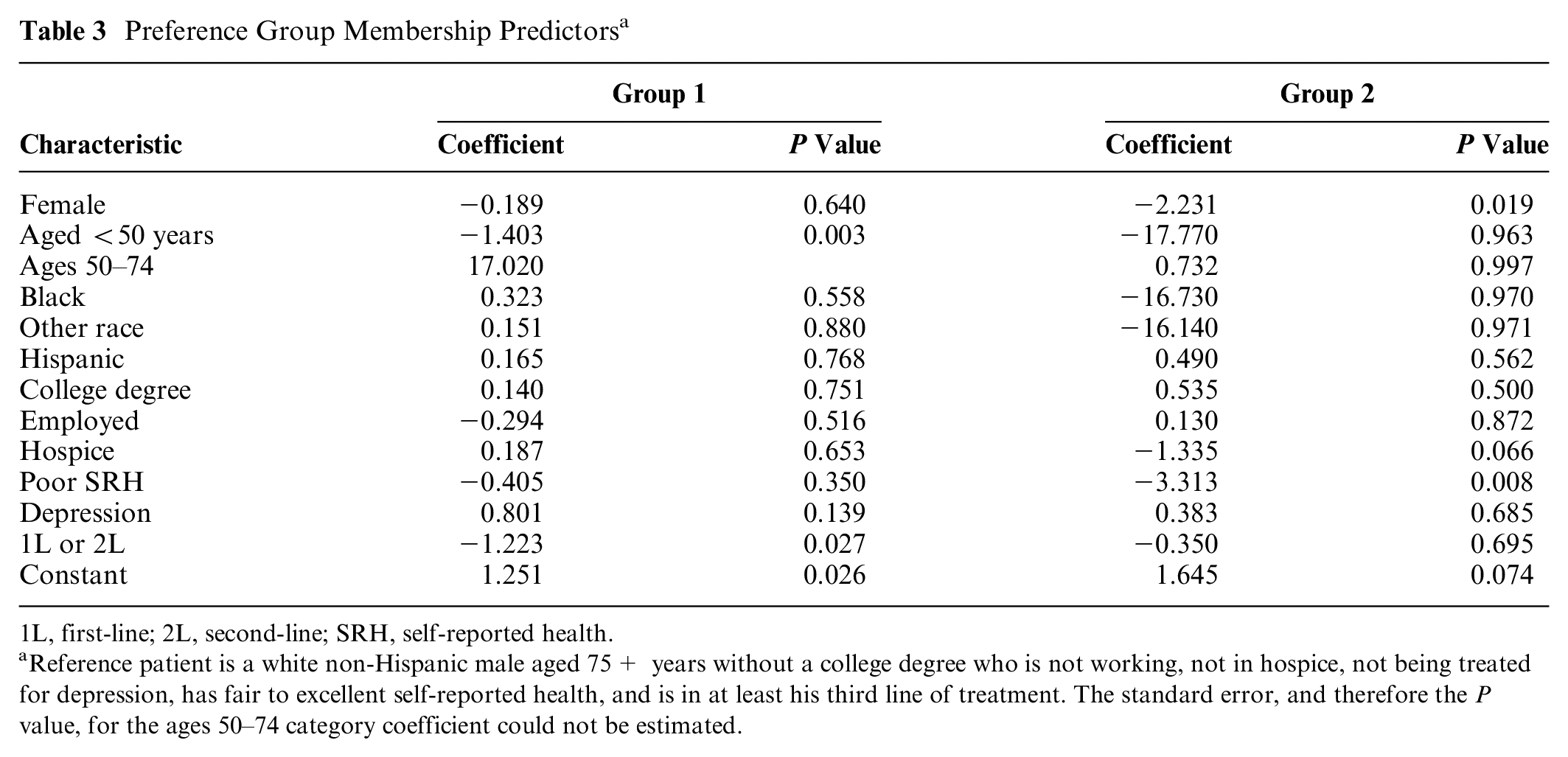
1L, first-line; 2L, second-line; SRH, self-reported health.
Reference patient is a white non-Hispanic male aged 75+ years without a college degree who is not working, not in hospice, not being treated for depression, has fair to excellent self-reported health, and is in at least his third line of treatment. The standard error, and therefore the P value, for the ages 50–74 category coefficient could not be estimated.
Table 4 contains the predicted preference shares for each 1L NSCLC treatment regimen by preference class, as well as the weighted preference shares by regimen. For example, the weighted market share for the IO-IO regimen is calculated as 53.2% = (30.9% × 53.0%) + (83.5% × 12.7%) + (76.5% × 34.3%). Overall, 53.2% of patients surveyed preferred an IO-IO-like regimen, 27.2% of patients preferred an IO-chemo-like regimen, and about one in five (19.5%) preferred a chemo-combination-like regimen in 1L. The majority of patients in the cost-seeking (83.5%) and engaged (76.5%) preference groups preferred IO-IO-like treatment regimens. On average, compared with combination chemotherapy regimens, patients were willing to pay $129 per month OOP more for IO-IO-like regimens and $90 more for IO-chemo-like regimens (Figure 4). This was largely driven by the preferences among engaged patients, who were willing to pay $399 OOP per month more for IO-IO-like regimens and $277 more for IO-chemo-like regimens.
Predicted Preference Shares by Preference Group and Regimen

The IO-IO-like regimen AE risk, OOPC per month, and 2-year survival attributes used to calculate preference shares were 30%, $6,500, and 65%, respectively. The IO-chemo-like regimen AE risk, OOPC per month, and 2-year survival attributes used to calculate preference shares were 50%, $4,000, and 55%, respectively. The chemo-like regimen AE risk, OOPC per month, and 2-year survival attributes used to calculate preference shares were 70%, $1,900, and 35%, respectively.

Predicted willingness to pay for IO-IO and IO-chemo like regimens versus combination chemo by preference group.
Discussion
Unlike much of the existing literature, which was largely conducted outside of the United States, we included OOPC as a treatment attribute in our DCE and found that more than half of patients considered the OOPC of therapy, with a small subset of patients preferring the more expensive therapy. Engaged patients (34.3%) focused on survival, AE risk, and treatment delays. The mechanism of action and subsequent treatment options attributes did not significantly influence treatment choices in any of the three patient preference groups. We found that overall, approximately 53.2% of patients preferred an IO-IO-like regimen and 27.2% of patients preferred an IO-chemo-like regimen as first line treatment for their NSCLC.
We implemented a three-class latent class model where class membership was modeled as a function of patient characteristics and patients who appeared to use simplifying heuristics were included. Women and those with poor self-reported health were less likely to focus solely on OOPC (group 2) than engaged patients (group 3). Relatively younger patients (age <50) and those in 1L or 2L treatment were significantly less likely to be solely survival focused (i.e., in group 1) than engaged patients (group 3). These results are consistent with previous studies, in which age and worse quality of life have been shown to be significant predictors of NSCLC treatment preferences.35,36 No patient characteristics were associated with a greater tendency to focus solely on cost (group 2) and socioeconomic factors like race and educational attainment did not significantly influence preference group membership.
Safety (AEs) and efficacy (as measured by survival in cancer) are the key attributes of treatment for any condition; thus, we would expect most patients to place significant weight on these attributes. Indeed, this is confirmed in previous studies of treatment preferences among NSCLC patients.16–18 The lack of focus on the subsequent treatment options in all preference groups may result from patients focusing on one line of treatment at a time for fear that they may not survive to receive subsequent lines of treatment, the cognitive burden of making choices about sequences of treatments, or both. The insignificance of mechanism of action in patients’ treatment choices may be a result of preferences for MOA being reflected in other attributes that also vary by mechanism of action, for example, efficacy and adverse event rates, and/or the complexity of the mechanism of action attribute. We leave further exploration of NSCLC patient preferences for sequences of treatment and MOA to future research.
Limitations
The DCE choice questions require respondents to make hypothetical treatment decisions by making tradeoffs between treatment attributes in a web-based survey. This exercise may be burdensome in terms of patients’ time and/or cognitively challenging. Thus, patients who are younger, more educated, more adept with technology/the internet, and/or those with relatively more time and energy may be more likely to have completed our survey. This seems likely given our patient population was younger, more likely to be Caucasian, and more likely to be fluent in English than the general NSCLC patient population. 4 Thus, our results may not be generalizable to the general NSCLC population and/or the perspectives of NSCLC patients from other socioeconomic, cultural, non-English speaking backgrounds. Also, the study only surveyed patients with self-reported advanced NSCLC, and thus the results may not extrapolate to patients with other cancers/tumor types.
Conclusion
Over the last decade, the introduction of IO therapies has significantly changed the NSCLC treatment landscape. As the spectrum of innovative treatment options for NSCLC patients continues to expand, it is critical that an informed decision about NSCLC treatment reflect not only what the patient is willing to undergo but also what undergoing treatment will allow the patient to attain or avoid. Shared decision making, which is increasingly being deployed in oncology care delivery, is a method for aligning clinical decisions with patient treatment option preferences. Treatment regimen effectiveness, risk of adverse events, treatment delays, and OOPC most influenced NSCLC patients’ 1L treatment decisions. A large majority of patients preferred an IO-IO-like followed by IO-chemo-like regimen in 1L and on average were willing to pay more for these regimens versus combination chemotherapy regimens.
Footnotes
Acknowledgements
The authors would like to thank Suepattra May-Slater, Katie Everson, Kata Bognar, and Beata Korytowsky for research support, and Christopher Nichols and Noe Marquez for assistance with designing the visual survey aids.
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Joanna MacEwan and Lauren Zhao are employees of PRECISIONheor, a research consultancy to the health and life science industries. Karen Reckamp is a Scientific Advisor to PRECISIONheor.
Komal Gupte-Singh is an employee of Bristol-Myers Squibb, which provided funding to PRECISIONheor to conduct this study. The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support for this study was provided entirely by a contract with Bristol-Myers Squibb. The funding agreement ensured the authors’ independence in designing the study, interpreting the data, writing, and publishing the report.