
Abstract
Results of the National Lung Screening Trial (NLST) clearly document a reduction in lung cancer mortality associated with annual lung cancer screening (LCS) using low-dose computed tomography (LDCT). 1 These data, combined with results of other LCS trials, led the US Preventive Services Task Force (USPSTF) to update their LCS recommendation to a B grade, 2 indicating that LDCT-based LCS holds high certainty that the net benefit is moderate or there is moderate certainty that there is a moderate to substantial net benefit. However, in addition to this recommendation, NLST data also documented noteworthy harms associated with screening.1,3 These harms, including a combination of physical, psychosocial, economic, and opportunity costs, must be weighed against the potential benefits of screening. 4
Policy recommendations stemming from the USPSTF decision have advocated that clinicians utilize shared decision making as the recommended platform, including the discussion of benefits, harms, and unknowns of LCS and engaging in joint decision making with screening candidates. Similarly, nearly every authoritative professional and advocacy organization that has subsequently favored LDCT-based LCS implementation (e.g., American Cancer Society, 5 American Lung Association, 6 National Comprehensive Cancer Network, 7 American Association for Thoracic Surgery, 8 and others) also supported the need for informed and shared decision making, owing to the complexity of the decision to pursue LCS. The American Academy of Family Physicians contends that it is premature to support broad implementation of LCS, and so it also currently recommends that clinicians and patients use informed and shared decision making in the process of considering LDCT-based LCS for individual patients. 9
The USPSTF LCS recommendation also has a direct effect on health insurance coverage in the United States. The Affordable Care Act10,11 recommends the use of informed and shared decision making as the desired approach for addressing LCS with patients. 2 The Centers for Medicare & Medicaid Services (CMS), in taking a landmark stance regarding the implementation of shared decision making, stated that patient counseling and shared decision making are required components of the LCS process and must be documented in advance of screening to qualify for reimbursement of screening services. 12 In addition, CMS mandated that clinicians use one or more decision support tools to facilitate the decision process. The inclusion of a decision support tool into the consultation may help address noted gaps in clinician knowledge of LCS.13–15 To support the importance of this step in the screening process, CMS has added LCS counseling and shared decision making as a reimbursable preventive service benefit. 16
In support of the need for counseling and shared decision making, several studies have documented substantial deficits in patient 17 and provider13,14,18–20 LCS knowledge and awareness and that some patients have not engaged their primary care clinicians prior to pursuing screening. 21 Community-based studies of screening have shown a lack of understanding of potential harms and unknowns.21–25 Studies of clinicians have likewise shown similar concerns about knowledge of screening benefits, harms, and uncertainties13,14,18–20,22,23,26 that would challenge the ability to achieve high-quality, truly informed decisions about screening.
While the complexity of LCS decision making provides a solid justification for policy regarding patient counseling and the use of shared decision making, the CMS requirement to include decision support tools precedes the availability of LCS-specific decision aids with a base of evidence demonstrating efficacy in supporting informed and shared decisions. Funded efforts are underway to develop LCS decision aids,27–30 and under the direction of Dr. Robert Volk, the Eisenberg Center for Clinical Decisions and Communications Science has developed a series of tools that are currently in use by clinicians and patients to support informed and shared decision making concerning LCS. 31
To extend the library of decision aids that support informed and shared decision making about LCS, the investigative team developed a plan to build a decision aid (LuCaS) that incorporated conjoint analysis as the principal values clarification tool that would promote deliberation and reflection on the decision. Additionally, once embedded within LuCaS, users would receive feedback regarding the results of their conjoint exercise (e.g., relative importance, utilities, etc.) to use in subsequent decision making. However, the feedback element was not included in the current project. As a step in the process of developing LuCaS, a web-based decision support tool dedicated to supporting informed decision making about LCS, the study team developed and administered a conjoint valuation survey to elicit patient preferences about LCS and inform the development of a values clarification exercise to be embedded within LuCaS. The framework for LuCaS is derived from the Knowledge-Empowerment-Values model, which seeks to help individuals develop and apply 1) an appropriate fund of decision-relevant information, 2) applicable decision making and communication skills, and 3) clear personal preferences and values. If data support the feasibility and utility of the conjoint valuation survey, the plan was to integrate the conjoint exercise into LuCaS as the central values clarification tool.
According to International Patient Decision Aid Standards, values clarification exercises32–34 constitute a key element of decision aids and decision support tools. 35 One approach to values clarification uses conjoint analysis or discrete choice experiments 36 to provide decision makers with a strategy to consider the health choice at hand, while considering the likely tradeoffs in terms of benefits, harms, and unknowns. The major benefit of using conjoint exercises is that they emulate real-life scenarios more effectively than individual questions that do not simultaneously take into account the multiple attributes of a decision scenario. The major downside is that conjoint exercises can be time consuming and somewhat burdensome for some individuals. Previous colorectal cancer screening decision research that examined the use of conjoint exercises in contrast to rating and ranking tasks failed to identify clear benefit to the conjoint exercise in terms of decision outcomes even though conjoint methods revealed a somewhat different pattern of attribute importance scores. 37 Pignone and colleagues suggested that studies examining pre to post changes in decision outcomes, as conducted in this study, would be beneficial in evaluating the utility of conjoint and other discrete choice approaches in terms of clarifying patient preferences and supporting informed decision making. 37
The brief educational narrative and conjoint exercise used in this study was developed using data from interviews conducted with individuals at risk of lung cancer, the empirical literature on LCS, and investigator knowledge and experience regarding LCS. As shown in Box 1, the conjoint exercise included 5 attributes with 17 levels describing these attributes. Prior to implementing the conjoint exercise, the complete survey underwent cognitive interviewing38,39 to identify and correct issues that challenged effective survey administration.
Attributes (5) and levels (17) Included in the Conjoint Valuation Survey.

The primary aim of this study was to examine the impact of a brief educational narrative and conjoint exercise on decisional conflict regarding LCS decisions among individuals at high risk for lung cancer. Investigators hypothesized that the brief educational narrative and conjoint exercise regarding decision-influencing attributes involving LDCT would significantly reduce decision conflict and all its component parts. As part of a larger investigation using a nationally representative panel of individuals at high risk for lung cancer, this study employed a single-arm (pretest-posttest design) of this intervention. Participants completed a measure of decisional conflict prior to reviewing the brief educational narrative and the conjoint survey and then completed the decisional conflict measure a second time immediately after completing the conjoint survey.
Methods
The study was conducted online using the web-enabled KnowledgePanel and standardized instruments to evaluate the impact of the intervention among individuals determined to be at high risk for developing lung cancer.
Procedure
Knowledge Networks (KN) conducts online surveys using the web-enabled KnowledgePanel (a probability-based panel designed to be representative of the US population).39–42 To establish and maintain its panel of participants, KN conducts random digit dialing of telephone numbers. Persons in selected households are invited by telephone to participate in the panel, and provided with an internet appliance and connection, if needed. The KN databases include over 300 health and demographic variables describing individuals on the panel, allowing for oversampling of underrepresented groups.
The study involved surveying a national sample of English-speaking individuals 45 years of age or older who were former or current smokers with at least a 20 pack-year history and without a history of lung cancer. We targeted a population that was approximately 50% female; 25% African American and 25% Hispanic; and 25% rural dwelling. The target sample size was 200 completed surveys, using a conservative approach to the sample size estimation algorithm developed by Orme for conjoint methodology. 43 Of the 525 individuals invited to participate, 304 did not meet eligibility criteria due to an insufficient smoking history, leaving 223 who met study eligibility criteria.
Investigators developed and delivered all components of the survey to KN, including a specific description of conjoint value analysis scenarios. KN sent invitations in batches to panel members fitting eligibility criteria. In an effort to achieve the target population, the demographic characteristics of new recipients varied as respondents completed the survey. Each respondent received a $30 honorarium. All data were entered directly into databases, so missing data were limited and only due to participant refusal or early survey termination prior to completion.
Participants
Of the 223 eligible KnowledgePanel members, 210 (94%) of respondents completed the online consent procedures and became participants. Participants had a mean age of 61.69 years (SD = 8.46), reported an average smoking exposure of 39.95 pack years (SD = 20.10), and a substantial majority indicated have internet access in the home (80%). As shown in Table 1, participants reported a range of educational achievement, were approximately equally represented by females and males, and identified as having health insurance. Due to planned oversampling, 51 participants were African American (24%), and 59 participants described themselves as Hispanic American (28%).
Demographic Characteristics of Study Participants (N = 210)
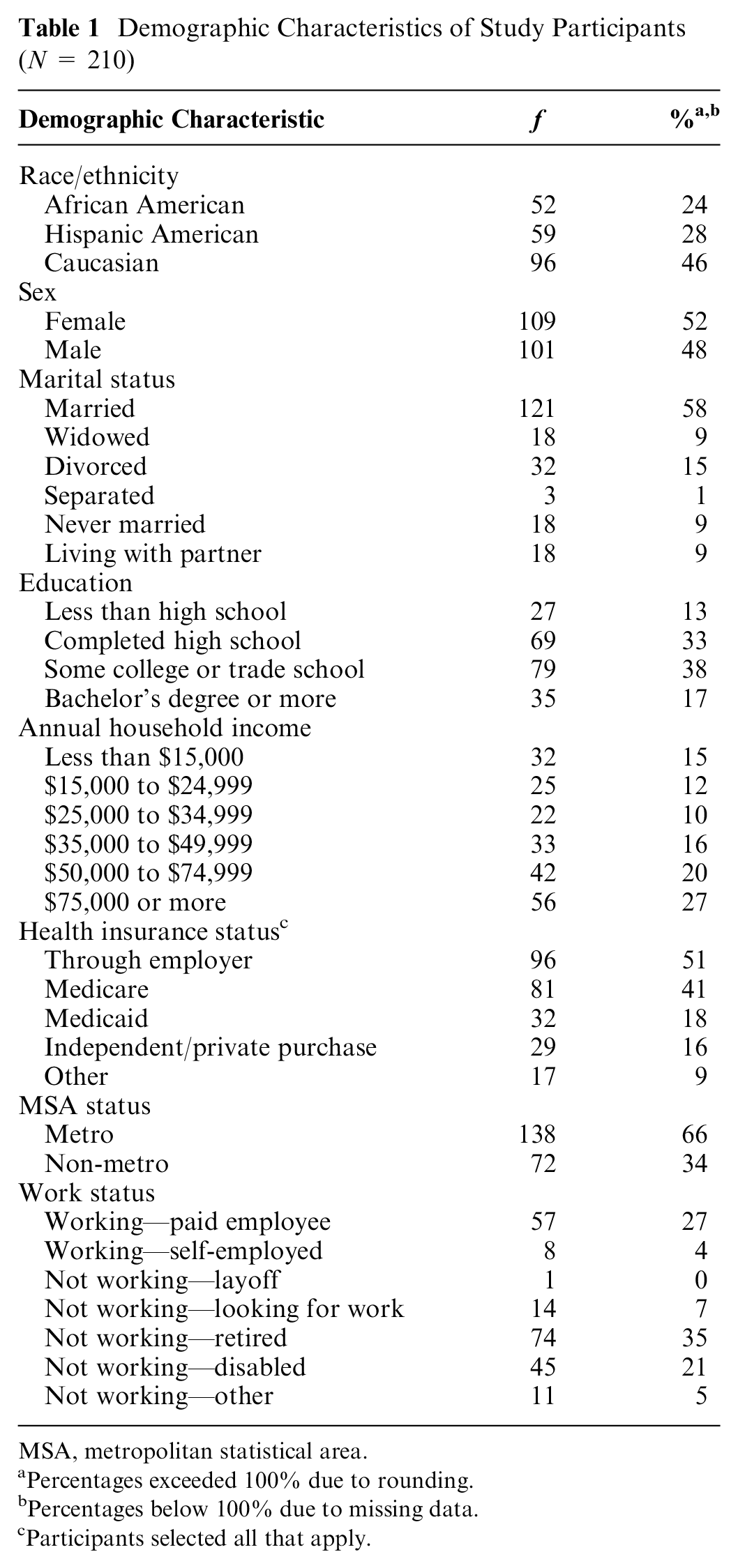
MSA, metropolitan statistical area.
Percentages exceeded 100% due to rounding.
Percentages below 100% due to missing data.
Participants selected all that apply.
Intervention
The intervention included a full-profile conjoint value analysis instrument with 22 cards/vignettes and a brief educational narrative on LCS. The conjoint exercise consisted of 5 attributes (with a total of 17 levels; see Box 1) that were developed following analysis of key informant interviews with individuals at risk for lung cancer and informed by the available research literature and the investigative team’s extensive clinical and research experience in LCS. The selection was guided by efforts to represent accurately the principal aspects of the LCS environment that would be considered in LCS choices, including benefits, harms, clinical recommendations, and environmental considerations. The final attributes included expected mortality reduction (benefit), false positive rate (harm), cost, provider recommendation, and access. After each scenario, a 9-point Likert-type ratings scale anchored by “would definitely not get screened” and “would definitely get screened” was used to assess importance scores. All respondents received the same scenarios, although the order of scenario presentation and order of attributes varied. The specific conjoint scenarios were generated using Sawtooth Software Inc. (Orem, UT). We used orthogonality, along with guidance from Johnson and Orme, 44 suggesting that individuals can answer over 20 pair-based comparisons without substantial task fatigue, as the criterion for determining the composition as well as number of the conjoint analysis tasks. In addition to the conjoint valuation survey, a brief educational narrative was provided that described the LCS decision, introduced the conjoint procedure, and defined a false positive screening result. The brief educational narrative included 410 words written at the 7.5 grade level as assessed by the Flesch-Kinkaid grade level formula. Introductory materials such as this are a vital part of preparing participants to complete a conjoint survey but may also serve as a co-intervention because they accompany the conjoint survey. See Appendix A for the brief educational narrative and the introduction to the conjoint valuation survey.
Measures
Background Characteristics
Two sources of information on background characteristics were included. Participants responded to several background questions on the PRE survey administered following consent procedures, and additional background history was available on all panel members from KN. On the PRE survey, participants responded to questions pertaining to their history of a cancer diagnosis, lung illnesses, and comorbid illness. Participants also responded to questions regarding their history of smoking and tobacco use. This set included items drawn from national surveys to assess current smoking status, years of smoking, age of smoking initiation, current average daily smoking volume, when an individual quit, quit attempts, interest in quitting, number of quit attempts lasting 3 months or longer, and nicotine dependence. Additional background data were available from their KnowledgePanel participant profile, including age, education, race/ethnicity, gender, marital status, employment status, insurance coverage, household information (e.g., size, number of adults, children, and income), internet use, health status, and geographic information about residence.
Lung Cancer Screening Awareness and Experience
On the PRE survey, participants were asked about their level of awareness and any past experience with LCS on five survey items. Specifically, the items asked about LCS awareness options, awareness of LDCT, understanding the potential benefits of LCS, and understanding the potential harms of LCS. One item asked if a health care clinician had ever talked with them about LCS. Each understanding and awareness item was measured on a 7-point Likert-type scale, and the experience item was measured dichotomously (yes/no), but a “don’t know” option was allowed.
Decisional Conflict
Participants completed a slightly adapted low literacy version (DCS-LL) 45 of the original Decisional Conflict Scale (DCS).46,47 The DCS-LL was designed to reduce literacy and time burdens among individuals completing the instrument in research settings. 45 The DCS-LL includes 10 items and employs a three response options: yes (0), unsure (2), and no (4). The full scale and subscales scores are calculated by summing responses, dividing by the number of items, and multiplying by 25. This creates scores ranging from 0 (no decisional conflict) through 100 (high decisional conflict) for the total scale and four subscales (e.g., Uncertainty, Informed, Values Clarity, and Support). Previous research has demonstrated the utility of this instrument as a reliable and valid measure of decisional conflict in a number of studies examining the efficacy of decision aids in oncology settings.45,47 The original version of the DCS-LL includes one item that combines assessment of benefits of screening and not screening and another item that assesses the potential risks and side effects of screening and not screening. Both of these items were subdivided to allow an assessment of these factors for screening and not screening separately because these were viewed as two separate and important factors related to the LCS context. Thus, the adapted version of the DCS-LL included 12 items with the two additional items loading onto the Informed subscale. 45 Estimates of internal consistency reliability were solid on the PRE (α = .89) and POST (α = .92). On the subscales, estimates of internal consistency were .80 or above for the Uncertainty, Informed, and Values Clarity subscales. However, the Support subscales internal consistency estimates were suboptimal. On the PRE survey, internal consistency was estimated to be .51, and the estimated on the POST survey was .66. Overall, the data suggested strong reliability with the exception of the Support subscale. In addition to the mean total score and mean subscale scores, cut-point scores were calculated to facilitate individual-level analyses. As recommended, a cut-point of equal to or below 25 was used as it has been associated with a higher degree of decision implementation or readiness to make a decision.46,48
Analyses
Sawtooth software was used to generate the 20 scenarios (plus 2 holdouts) embedded within the conjoint valuation survey. Holdout choice scenarios are included in the conjoint survey but are not used to calculate the results. Data from holdout responses can be used for cross-validation of conjoint results using predictive modeling. Details regarding the development and analysis of the results of the conjoint valuation survey have been reported separately. 49
Descriptive statistics were used to characterize the sample, describe participant self-ratings of awareness, understanding, and LCS experiences as well as total and subscale decisional conflict scores. Subsequently, paired t tests were conducted to test the hypothesis that the intervention would reduce decisional conflict. Additionally, McNemar’s tests were conducted after decisional conflict scores were dichotomized as >25 and ≤25 to indicate desired levels of decisional conflict in preparation for decision making. 46 Due to the use of several subscales, alpha was set at .01, and Cohen’s d was used to describe the effect size. Finally, univariate and multivariate regression analyses between demographic characteristics (including tobacco use) and change in decisional conflict scores were conducted to examine potential associations.
Results
At baseline, participants generally reported a moderate level of awareness and understanding of the benefits and harms associated with LCS. On the 7-point Likert-type scale of awareness of LCS options, the mean rating was 4.13 (SD = 2.12), and the awareness rating for LDCT specifically was 3.39 (SD = 2.12). With regard to understanding LCS benefits, the mean rating was 4.77 (SD = 1.91), but the understanding of potential harms was 3.25 (SD = 2.05), notably lower. In terms of experience, only 19% of participants indicated that they had ever spoken with a clinician about LCS (40/210).
To examine the impact of the conjoint survey and brief introductory narrative, total and subscale decisional conflict scores on the PRE and POST surveys were compared using paired t tests (Table 2). For the total score and each subscale, participants reported relatively high levels of decisional conflict on the PRE survey, followed by substantially and significantly lower decision conflict levels on the POST survey.
Decisional Conflict Scores (N = 209)

In addition to conducting group-level analyses of decisional conflict rating scale scores, individual-level analyses examined rates of participants who scored equal to or below a cut-point score of 25 (Table 2). 46 On the baseline PRE survey, 24.8% of participants had total decisional conflict scores of 25 or less. On the subscales, 29.5%, 20%, 31.4%, and 41% had sub-26 scores on the Uncertainty, Informed, Values Clarity, and Support subscales, respectively. At the POST survey, the percentage of individuals with sub-26 total decisional conflict increased to 72.7%. On the subscales, 63.2%, 73.7%, 77.0%, and 68.9% of participants had sub-26 scores on the Uncertainty, Informed, Values Clarity, and Support subscales, respectively. Based on McNemar’s test to evaluate repeated measures dichotomous data revealed statistically significant changes across the total score and all four subscales (Ps < 0.001).
Univariate regression analyses were conducted with change in the overall DCS score as the dependent variable and demographic and tobacco use characteristics (e.g., age, gender, education, race/ethnicity, income, marital status, current smoking status, and pack-year smoking history) as the independent/explanatory variables. The only significant association found was between income category and change in DCS score, with individuals in the two highest income categories having significantly larger reductions in decisional conflict (P < 0.05). To assess the robustness of this result, we subsequently ran a multivariate regression including all of the above-mentioned demographic variables (Table 3). As in the univariate results, the only significant association between demographic characteristics and change in DCS score in the multivariate analysis was that the highest two income categories continued to be significantly associated with a greater change in the DCS score relative to the lowest income category.
Summary of Univariate and Multivariate Regression Analysis for Variables Predicting Change in Decisional Conflict Scores (N = 209) a

F(15, 187) = 0.75, P = 0.709, R2 = 0.06.
P < 0.05.
Discussion
Results of the NLST have created a unique opportunity to reduce the dramatic burden of lung cancer through an evidence-based early detection program paired with effective intervention. However, implementation of LDCT screening for lung cancer is new and complicated.50–53 To address the threats to high-quality implementation, policy makers have established rigorous standards for patient counseling and shared decision making in advance of screening. To support high-quality decision making, new decision support tools regarding LCS are needed to address known gaps in patient and clinician knowledge. As part of a larger program of research, this study explored the impact of a new educational intervention and conjoint valuation survey on decisional conflict scores regarding LCS among a nationally representative sample of individuals at high risk of developing lung cancer.
Results of this observational trial demonstrated that individuals who received a brief introduction to LCS followed by a conjoint valuation survey reported large drops in decisional conflict, including all four decisional conflict subscale scores. Effect sizes ranged from 0.66 to 1.10, suggesting a pattern of (very) large effects within this uncontrolled trial. In part this may be due to limited public awareness and knowledge about LCS, but it also demonstrates that the combination of brief information sharing and in-depth exploration of key factors affecting LCS decisions had a significantly favorable impact on potential screening participants in terms of clarifying values, feeling informed, and helping prepare them to make informed choices. One other published study of a video-based decision aid has shown improvements in LCS knowledge as well as low decisional conflict following exposure to the intervention. 27 However, decisional conflict was only assessed after exposure to the intervention, precluding an assessment of change.
There was considerable individual variation in pre and post decisional conflict scores, however. While the overall group effects showed substantial reductions in decisional conflict following the intervention, approximately one quarter of the study sample had decisional conflict total scores of less than 25 (indicating a desirably low level of decisional conflict) prior to the intervention. In addition, approximately 25% of participants continued to have decisional conflict scores above 25 following the intervention. Thus, while clearly providing support for both group-level and individual-level benefits, these results show that a substantial minority of participants continued to experience decisional conflict that could impair informed decision making about LCS participation. Thus, there is likely a need for additional shared decision-making interventions that can help individuals navigate the complexities of this preventive health service choice. In particular, the largest subset of individuals appeared to experience continued uncertainty and a need for additional decision support based on subscale scores. This conclusion also provides support for the policy standard adopted by CMS, requiring documentation of a patient counseling and shared decision-making consultation prior to initiating screening. 12
In a preliminary manner, this study supports the value of the brief educational narrative and the conjoint valuation survey in reducing decisional conflict and supporting engagement with the LCS decision. The use of conjoint methods has been previously used in similar settings37,54 to facilitate preference elicitation and consideration of cancer screening although results have not consistently demonstrated their utility. 36 In this vein, the conjoint exercise can serve multiple roles: 1) provide information, 2) support deliberation and reflection, and 3) provide preference feedback, if there is a mechanism to return the results directly, which may have the most powerful impact. This study emphasized the information delivery and deliberative functions of conjoint exercises since it did not include a mechanism to provide feedback to respondents regarding the results of the conjoint. The conjoint approach has several potential advantages that support values clarification and preference elicitation. Most prominently, conjoint exercises help individuals explore relevant tradeoffs that are inherent within the potential benefits and harms associated with screening. Given the complexity of the benefit and harm equation for LCS, despite the relatively simple decision architecture (screen v. not screen) as compared to colorectal cancer screening (i.e., colonoscopy v. sigmoidoscopy v. FOBT/FIT v. not screening), the conjoint approach provides an engaging and facilitative method of clarifying values and preferences related to participation in a LCS program.
Study Limitations
Although this study was conducted with a large, nationally representative sample of individuals at high risk for lung cancer, the results should be interpreted in light of some limitations. First, because the conjoint was paired with a brief educational narrative, it is not possible to isolate the effects of the conjoint activity from the brief educational activity, nor is it possible to eliminate the possibility of other confounds. However, conjoint activities require introductory material consistent with the information we presented at the start of the conjoint activity. 37 It would be of interest to compare the effect of an educational intervention alone against an educational intervention plus conjoint exercise to gain a better sense of the relative merits of the conjoint activity. However, the data do support the viability of this intervention in the LCS context. Second, not all of the participants would be eligible for LCS based on their age and tobacco use history. However, because the purpose of the LuCaS intervention is to promote informed decision making, the strategy was adopted to educate individuals who would likely find the information of value, regardless of their eligibility. It was also not designed to promote screening; therefore, educating a larger audience, using a broader, public health approach is appropriate. Third, using a conjoint strategy is likely to be too time consuming to be employed in clinical settings, but this type of values clarification exercise could be used in decision support tools designed to prepare individuals for consultation with a clinician or perhaps for post-consultation consideration when an individual remains ambivalent about screening and wishes to continue to explore benefits, harms, and uncertainties in more detail. Fourth, the large sample size created a scenario where the study was likely to overidentify very small changes in decisional conflict as statistically significant. To address this concern, we included effect sizes measures to provide additional analytic information regarding the impact of the intervention.
Conclusions
Given the substantial plausible impact of the brief educational narrative and conjoint exercises on decisional conflict in this study, integrating conjoint approaches into decision aids for LCS may be a viable consideration. Longer administration times likely preclude the use of this particular conjoint in decision support tools in the clinical setting as consultation aids. However, conjoint survey approaches would be a better fit for individuals who are seeking information about LCS and seeking to explore the decision in greater depth before making a choice, even if conjoint results cannot be immediately analyzed and returned. Additionally, more intensive and engaging tools of this nature may help patients prepare for a high-level, yet efficient discussion with clinicians, preparing them to engage in a truly shared decision-making consultation. Conjoint exercises may be particularly helpful in the LCS context, given the complex range of benefits, harms, and uncertainties associated with this recently emerging cancer screening modality.
Supplemental Material
LCS_-_DCS_Manuscript_FINAL_R2_2019-10-22_CLEAN.rjf_online_supp – Supplemental material for Brief Education and a Conjoint Valuation Survey May Reduce Decisional Conflict Regarding Lung Cancer Screening
Supplemental material, LCS_-_DCS_Manuscript_FINAL_R2_2019-10-22_CLEAN.rjf_online_supp for Brief Education and a Conjoint Valuation Survey May Reduce Decisional Conflict Regarding Lung Cancer Screening by Jamie L. Studts, Richard J. Thurer, Kory Brinker, Sarah E. Lillie and Margaret M. Byrne in MDM Policy & Practice
Footnotes
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Support for this study was provided by a grant from the National Institutes of Health (R21CA139371) as well as assistance from the Behavioral and Community-Based Research Shared Resource Facility of the University of Kentucky Markey Cancer Center (P30CA177558). The funding agreements ensured the authors’ independence in designing the study, interpreting the data, writing, and publishing the report.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.