
Abstract
Reimbursement practices have evolved over time. Health technology assessment (HTA) represents a comprehensive approach to the evaluation of emerging and existing health care interventions. A major component of HTA submissions to public-payer drug plans are economic evaluations designed to compare competing interventions with respect to both clinical and economic consequences. Cost-utility analyses (CUAs) are a type of economic evaluation accepted by several major HTA bodies worldwide.1–3 These analyses are particularly useful for interventions or programs that not just extend life but also affect the patient’s health-related quality of life or health status. In a CUA, health state utility values (HSUVs) are used to estimate quality-adjusted life years (QALYs) and provide an estimate of both quantity and quality of life. 4 Health states may be simple or complex, defined by several factors, including disease and treatment characteristics as well as functionality and limitations. By convention, full or perfect health is assigned the maximum utility score of 1, while death is assigned a utility score of 0. Health states with negative utilities are perceived as worse than death. While HSUV estimates are inherently subjective, the general rule is to weight more preferable health states with higher utility.
Investigators can measure HSUVs using different approaches. These can be through direct measurements, such as the visual analogue scale (VAS), or through preferences elicited using probabilities or willingness to tradeoff between quantity and quality of life methods, such as the standard gamble (SG) or time tradeoff (TTO) technique. Indirect methods using multi-attribute utility-based instruments, relatively short questionnaires that require only a few minutes to complete, provide an easier alternative to these direct measures. The term indirect measure is used as individual patients do not explicitly provide preferences for their health states but rather describe their state, which is then assigned a value according to a scoring algorithm that has been developed separately with the general public or patient groups. Investigators have used both direct and indirect methods in addressing HSUV for cancer treatments. 5
Rapid progress in the field of oncology has given way to new therapies, and these treatments have made significant contributions to prolonging life expectancies or improving quality of life. 6 However, these new cancer treatments often come at high costs.7,8 As part of the drug reimbursement process in many countries, manufacturers are required to submit dossiers containing CUAs. It is recommended that HSUV inputs for these CUAs be identified through systematic literature reviews. 9 However, a cross-sectional review of 71 technology appraisals submitted to the National Institute for Health and Clinical Excellence found that out of 39 submissions that obtained HSUVs from published studies, only 31% adopted a systematic approach. 10 Moreover, even when these reviews are commissioned, the review methods and findings may not be made explicit to reimbursement agencies. Thus, the complete evidence profile for a given health state may not be clear to reviewers and their ability to make a critical appraisal of model inputs may be limited.
There are several systematic reviews of HSUVs across the cancer spectrum.11–15 However, these reviews are targeted to answer a question in a particular area of oncology. To date, no central catalogue of cancer-related HSUVs has been established. Such a resource would dramatically enhance researchers’ abilities to select and evaluate the available health utility literature in a thorough and timely manner. In the interest of the comprehensive, accountable, and transparent evaluation of CUAs in the support of oncology drug reimbursement submissions, we have developed a systematic review protocol to identify and describe published health states and HSUVs across the spectrum of oncology research. This review is part of the Health Utility Book (HUB) as described by Xie et al. 16
Objectives
The objective of this article is to present a study protocol for systematically identifying and describing the health utility literature in the field of oncology with respect to both the methods used and the estimates attained for cancer-related health states. These methods are illustrated with a pilot study in thyroid cancer.
Methods
This systematic review will be conducted in general accordance with published guidelines and good practices.17–22 Additional considerations have been made given the broad scope of the review and the anticipated volume of work. The traditional Patient, Intervention, Comparison, Outcome (PICO) statement, common to clinical research, is not typically amenable to reviews of HSUVs.17,18 Specifically, this review is not designed to collect information on any particular intervention or comparator. This protocol has been registered with the Prospective Register of Systematic Reviews (PROSPERO CRD42018095049).
Search Strategy
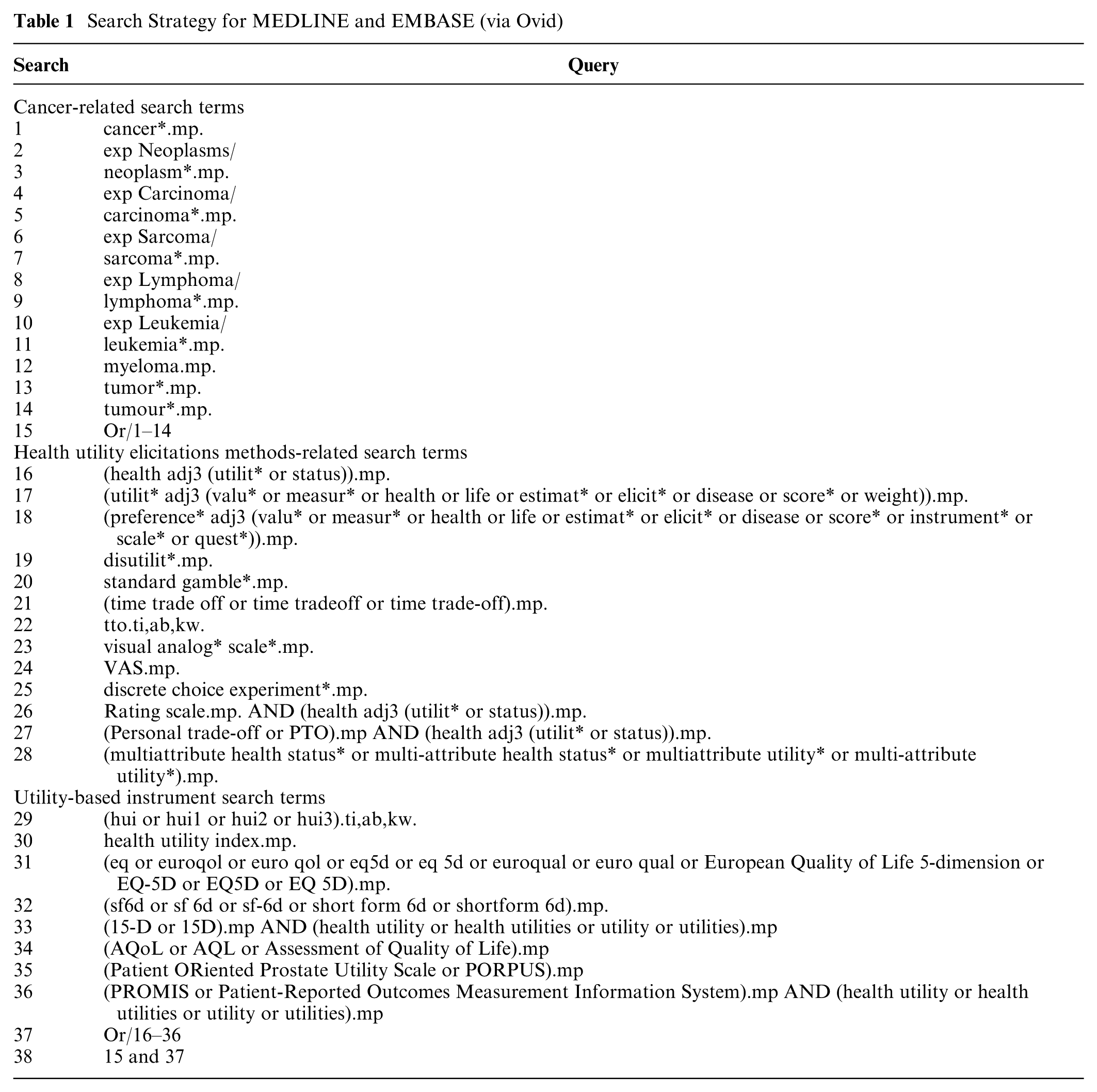
The scope of the search strategies for this review is purposefully broad. The databases to be queried include the following: MEDLINE via Ovid; EMBASE via Ovid; EconLit via EBSCOhost; and CINAHL via EBSCOhost. The search strategies were developed by reviewing published HSUV review recommendations, the strategies of published HSUV protocols, and published guidance from other sources such as the Canadian Agency for Drugs and Technologies in Health (CADTH). Specifically, we will use two categories of search terms: disease-specific queries and health state utility elicitation methodology-specific queries. To strengthen this search strategy, we added utility-based instruments as an additional search query. To validate the search strategy, we reviewed the reference lists of published systematic reviews of health utility studies and collected 28 citations (the validation set) to reflect a range of years, methods, and cancer types.23–50 The search strategies developed for the current review were tested to confirm that they successfully captured the citations included in the validation set. The strategies were then adapted to the other databases. Table 1 presents the search strategies in MEDLINE and EMBASE, which were searched separately.
Search Strategy for MEDLINE and EMBASE (via Ovid)
Study Eligibility
Inclusion Criteria
A high-level set of inclusion criteria was selected for this review. To be eligible for inclusion, a publication must meet all the following:
The publication presents the methods of a primary HSUV study, such that a study uses a direct elicitation method (e.g., TTO), an indirect method (e.g., EQ-5D), or a combination of both to elicit preferences for health states from patients or nonpatients (e.g., general public, family, caregivers, or clinicians);
The study targets cancer, cancer treatments, and/or the cancer patient population, including nonpatient respondents; and
The study reports HSUV estimates.
This review is limited to the context of patients who have been diagnosed with cancer, though studies have been published for related populations, such as unaffected high-risk individuals. No restrictions have been specified for publication date or language. In order to provide sufficient information to be used in CUAs, this review focuses only on peer-reviewed studies, excluding grey literature (e.g., unpublished studies, dissertations, conference abstracts). We anticipate that several reviews and economic evaluations, which reference HSUV literature, will be identified with the proposed search strategies. Reviewers will identify these records and the reference lists of these publications will be cross-referenced with the final list of included studies to assess the comprehensiveness of our review.
Data Collection
Study Selection
Prior to screening, duplicate publications will be identified and excluded. The titles and abstracts of all publications identified by the search strategies will be screened according to the eligibility criteria. Where unclear, reviewers will carry the record forward to the full-text screening phase. We have adopted this sensitive approach based on research demonstrating limitations in evaluating study eligibility at the title and abstract levels. 18 The full text publications of included abstracts will be retrieved and assessed for eligibility. Publications published in languages other than English will be reviewed by language-matched reviewers having a working knowledge of the language of publication. All screening will be conducted independently and in duplicate. The flow of information process, which documents the number of records retrieved as well as the number of inclusions and exclusions at each screening phase, will be summarized in a PRISMA flow diagram. 51
Based on preliminary searches, it is anticipated that a large volume of records will be retrieved through the literature search. Thus, this review necessitates the participation of multiple reviewers whose availability may change over time. As a means of promoting consistency across reviewers, we will establish a training set of 150 records purposefully chosen to represent a broad range of eligible and ineligible studies. Prior to beginning abstract screening, new reviewers will complete the training set and review their results, including reasons for exclusion, against the answer key. The complete set of publications to be screened will be divided into blocks of 1000 records. Reviewers will be assigned one block of records at a time and, upon completion, will be assigned a new, previously unscreened block. Once all blocks have been screened in single, the blocks will be reassigned to satisfy the requirement of duplicate screening. Full-text screening will also be managed using a blocking approach.
Data Extraction and Management
A complete list of data extraction items is presented in Appendix A. All data will be extracted independently and in duplicate using a similar blocking approach as described in the screening process. The reviewers who complete data extraction will review and resolve discrepancies by discussion, with a third reviewer providing arbitration, as necessary. In the case of missing data, we will attempt to contact the corresponding authors for clarification. The data extraction form has been successfully piloted. All screening and data extraction will be maintained in Microsoft Excel workbooks, which include extensive standardized vocabulary to promote consistency and ease of data extraction and reconciliation.
Data Synthesis
A descriptive summary of the findings of this review will be presented, arranged by cancer type. Health state descriptions and corresponding HSUVs from each study will be presented along with a summary of the study methodologies and respondent characteristics. At present, this review is designed to gather and describe published HSUVs. Cognizant of the assumptions that must be made, particularly when HSUVs are derived through different methodologies, we will explore different quantitative evidence synthesis approaches that have been used to pool the HSUVs in the literature. 52
Ethics and Dissemination
No ethics approval will be sought for the purpose of this review as no primary data collection will take place. All information will be identified from published studies. The completed review will be disseminated in a series of publications in peer-reviewed journals, arranged by cancer type, detailing the systematic review methodology as well as a summary of the findings. We are also in the process of seeking funding support to develop an online portal to disseminate the HSUVs identified through this review.
Pilot Review
Summary of Screening and Validation
To illustrate the systematic review process described here, we present the screening of a subset of records identified for thyroid cancer. According to data maintained by the World Health Organization (1970–2012) and the Cancer Incidence in Five Continents (1960–2007), the incidence of thyroid cancer has been increasing over the last several decades despite a falling mortality rate. These trends have been attributed to changes in the diagnosis, treatment, and exposure to risk factors. 53 However, if current trends persist, it is suggested that thyroid cancer may be the fourth most common cancer in the United States by the year 2030. 54 Despite this, our preliminary review suggested that there are relatively few published studies for health utilities for this indication.
From the complete set of records identified with our search strategy (N = 52,551), we selected a subset that contained the phrase “thyroid” in the title or abstract (n = 842). From these 842 abstracts, 31 were reviewed at the full-text screening level, and six fulfilled all eligibility criteria. Additionally, 21 economic evaluations were identified.55–75 No systematic literature reviews related to health utilities for thyroid cancer were identified. The screening process is summarized in Figure 1.
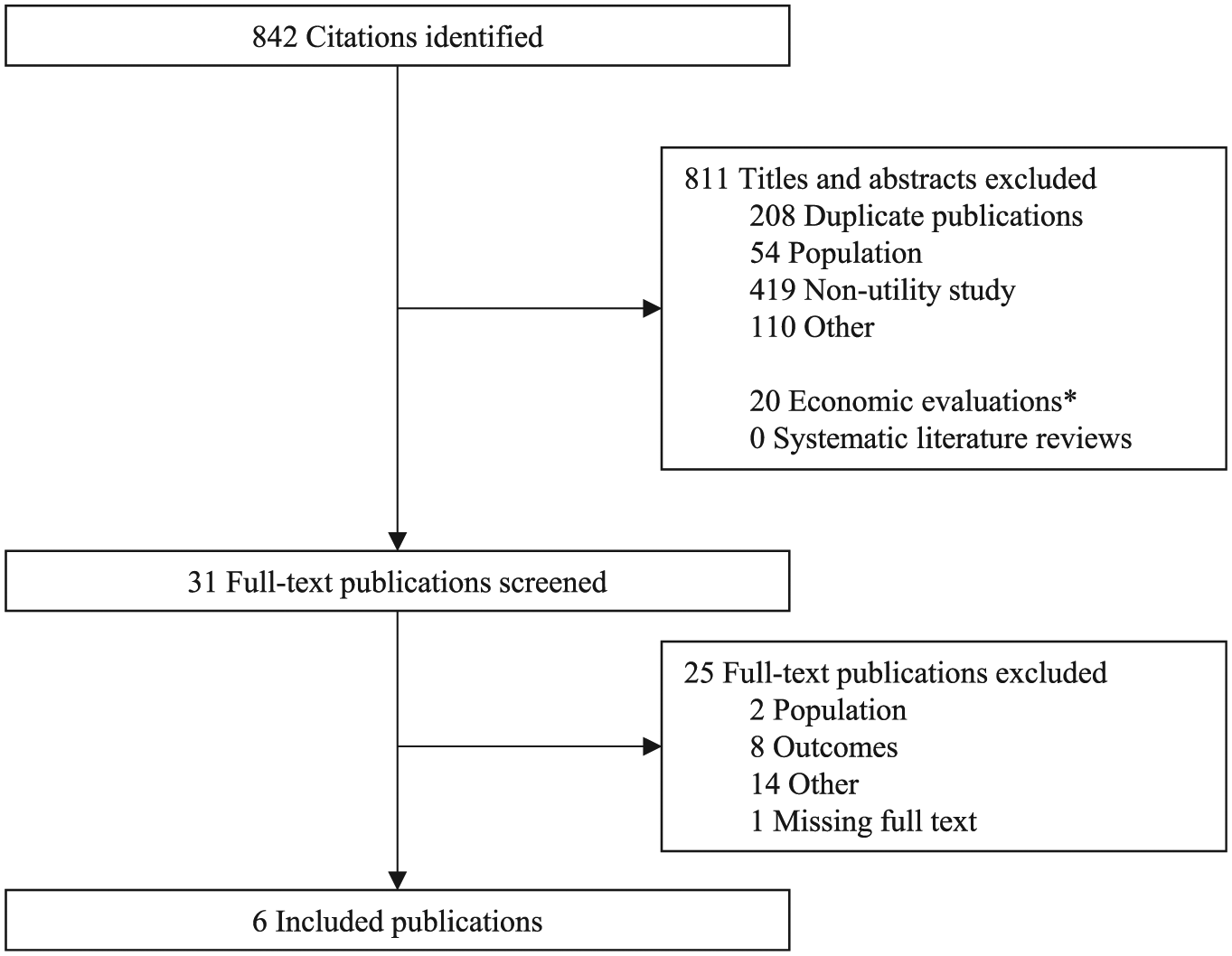
PRISMA flow of information diagram.
From the 21 economic evaluations, 35 unique citations for health utility inputs were identified. To validate the systematic review process, these were cross-referenced with the list of included studies. Of these 35 citations, 12 were in a clinical area outside of thyroid cancer, 10 lacked indexing or abstract keywords to indicate that health utility evidence was presented, 4 were published in a source not indexed in the included medical literature databases (i.e., books, websites), and 3 referenced an economic evaluation where no original health utility study was conducted. The remaining six citations were also identified through our search strategy in thyroid cancer and were reviewed for inclusion through our systematic review. However, only two of these citations were considered eligible for inclusion.62,76 While economic evaluations may contain bespoke health utility studies, they often lack indexing or keywords to identify them as a health utility study. Overall, the validation steps suggest that the literature search strategy and screening process adequately identified all relevant publications per the prespecified eligibility criteria.
Descriptive Synthesis
Characteristics of the six eligible studies are presented in Table 2. Most studies reported on health utilities collected using a single technique except for one that employed multiple methodologies (EQ-5D, SF-6D, HUI-2, HUI-3). 77 Four studies used a cross-sectional design.62,76,78,79 Respondents varied across studies, with three recruiting patients,77,79,80 two recruiting clinicians,62,78 and one recruiting members of the general public. 76 One health utility studied was conducted alongside a clinical trial. 80 However, participant characteristics were generally poorly described in the included publications. All health states were either derived for the purpose of the study or relied on patient’s own health. Adverse events or toxicities were explicitly incorporated into the health state descriptions of only one paper. 76 In the study by Choi and colleagues, 78 the impact of several cancer diagnoses, including thyroid cancer, was reported as a disutility weight. These estimates were considered eligible for inclusion in this review. A summary of the published health utility estimates, arranged by respondent subgroups and scaling method, is presented in Table 3. The health state with the highest HSUV was obtained from clinicians using the TTO for “Disease-free after thyroid lobectomy” (0.99), 62 while the lowest observed estimate was reported for “Stable disease with grade 3 diarrhea” (0.42, SD 0.29, 95% confidence interval: 0.36, 0.48) by the general public using the TTO. 76 In both studies, health state descriptions were provided by investigators.
Characteristics of Included Studies of Health Utility in Thyroid Cancer

Health States in Thyroid Cancer

CI, confidence interval; rhTSH, patients managed with recombinant human thyroid-stimulation hormone; THW, patients managed with thyroid hormone withdrawal; VAS, visual analogue scale.
Reported as disutility weights.
Discussion
Published studies that measure HSUVs are a main source of health utilities used in CUAs. These evaluations are an integral component of reimbursement submissions prepared by drug manufacturers seeking listing on public formularies. However, the selection of HSUVs, where multiple studies are available, is often left to the discretion of analysts. Thus, the lack of a systematic approach to the identification and use of published health utilities may lead to a reimbursement policy that does not reflect the preferences of the public. The current review applies a systematic approach to the identification of published HSUVs and thus affords a level of confidence to knowledge users who rely on valid information to complete economic evaluations and HTA appraisals.
Where a health utility estimate does not exist in the literature for a given condition or health state, it is common to use estimates derived for a similar condition. This was the case in several of the economic evaluations identified through our pilot review. However, it is outside the scope of our review to suggest indications that may be interchangeable.
While the proposed review is extensive in scope, there are limitations. Estimates of HSUVs coming from grey literature sources, including conference abstracts and other unpublished media, are not eligible for inclusion. According to our past experience, information provided in conference abstracts or media reports often is not sufficient to be used in CUAs. If the reporting in the grey literature changes in the future, we will revise our review to expand the search strategies and eligibility criteria accordingly. Despite this, the proposed review will culminate in a comprehensive summary of the evidence landscape for published HSUVs in oncology. Detailed study methodologies and respondent characteristics will be collected and summarized. Moreover, this review is the first component of the HUB project. 16 The publication of this review protocol is in line with the HUB project team’s goal to maintain transparency and accountability.
Supplemental Material
Zoratti_HUB_SLR_Protocol_-_Appendix_A_online_supp – Supplemental material for Health Utility Book (HUB)–Cancer: Protocol for a Systematic Literature Review of Health State Utility Values in Cancer
Supplemental material, Zoratti_HUB_SLR_Protocol_-_Appendix_A_online_supp for Health Utility Book (HUB)–Cancer: Protocol for a Systematic Literature Review of Health State Utility Values in Cancer by Michael James Zoratti, Ting Zhou, Kelvin Chan, Oren Levine, Murray Krahn, Don Husereau, Tammy Clifford, Holger Schunemann, Gordon Guyatt and Feng Xie in MDM Policy & Practice
Footnotes
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.