
Abstract
Keywords
Newborn bloodspot screening (NBS) is a clinical intervention that aims to identify children who may have a serious inherited condition early in their lives. By screening and taking action only a few weeks after birth, the quality and length of life of children with the conditions can be significantly improved. Newborn bloodspot screening programs (NBSPs) are established in many developed countries. 1 Recent advances in screening technologies, in particular the adoption of tandem mass spectrometry, have dramatically increased the number of conditions that can be effectively and economically screened for, with some US states now screening for more than 50 conditions. 1
The national NBSP in England screens more than 600,000 babies each year for nine inherited conditions. 2 In 2015, the NBSP expanded from five to nine conditions with the addition of maple syrup urine disease, isovaleric acidemia, glutaric acidemia type 1, and homocystinuria to the existing phenylketonuria, congenital hypothyroidism, cystic fibrosis, sickle cell disease, and medium chain acyl coenzyme-A dehydrogenase deficiency. Participation in the NBSP is offered to all parents in the United Kingdom, typically when their child is between 5 and 8 days old, and operates using an informed consent model. 3
Midwives represent the key group of health care professionals involved in providing the NBSP with two core roles: 1) the screening sample takers and 2) a source of information about screening. One of the main goals of screening, as stated by the NBSP, is “to minimise the adverse effects of screening, including anxiety, inaccurate information and unnecessary investigation, and to provide reassurance to the majority of parents whose babies are thought not to be affected.” The NBSP has recognized that communication of accurate information to parents is necessary and has developed guidelines on informed choice and communication. Previous studies have suggested that parents may experience anxiety on receipt of positive, false-positive, or carrier results from screening,4–6 and comprehensive information provision has been shown to be an effective way of preparing parents and mitigating such worry.
Given the recent expansion of the English NBSP and potential for subsequent program growth (an “expanded” NBSP), the quantity and type of information required by parents to make an informed decision about screening could change. 7 Given their role and experience in providing NBS information, understanding midwives’ beliefs about what information helps parents to make decisions about screening may help develop information provision in an expanded NBSP. As midwives have experience of delivering information to a wide variety of individuals, their experience may provide a different insight into the best design of NBS communication than could be elicited from parent preferences.
Stated preference studies are survey-based instruments that allow the elicitation of preferences for aspects of a service. Discrete choice experiments (DCEs) are a commonly used method to quantify the stated preferences of a defined population for a health care service or intervention.8,9 DCEs are underpinned by the theory that individuals value a service because of the component parts (attributes; each with specified levels) of the service rather than viewing the service as a whole. 10 By showing participants different hypothetical services, described by a set of attributes, which vary in the levels attached to those attributes and asking them to choose their preferred service, the relative preferences for the specific attributes can be calculated using regression-based analysis. Conjoint analysis (CA) surveys are a related, but different, type of stated preference survey that use rating or ranking rather than a choice-based approach. 11
Three published DCEs have examined preferences in the context of NBSPs. Miller and others 12 elicited public preferences for attributes of an NBSP, finding that the clinical benefits of the service were most important followed by avoidance of false-positive results and overdiagnosis. Hendrix and others 13 examined the preferences of Black and low-income families, an underrepresented section of society, regarding the storage and use of dried bloodspot samples for research. Furthermore, other types of preference valuation studies have also been previously used in the field of newborn bloodspot screening to value the avoidance of false-positive results 14 and a test for spinal muscular atrophy. 15
Understanding parents’ preferences for information is important in tailoring the intervention to meet the needs of the service users. A published preference study, using a hybrid design, aimed to identify parents’ preferences for the process of information provision alongside the outcome of screening in parents’ ability to make a decision about screening. 16 Two designs were used to identify preferences for information in a program screening for nine conditions, reflecting the current NBS program in the United Kingdom, and a hypothetical program screening for 20 conditions. This study found that all of the 11 types of information about screening identified were perceived to improve parents’ ability to make a decision about screening regardless of the program size. Parents stating preferences for a nine-condition NBS wanted to receive information early in pregnancy, but those completing the survey presenting a 20-condition NBS preferred information after 20 weeks of pregnancy. Both groups disliked receiving information after the baby had been born.
It is, however, also important to understand the perceptions of midwives who provide the information on a day-to-day basis to families from diverse backgrounds may also be informative in guiding the development of information provision. To date, no study has been conducted to quantify midwives’ preferences regarding NBSP information provision. This study aimed to quantify midwives’ preferences for the types of information that should be provided to parents in a nine-condition screening program and their views on how this information should be provided.
Methods
An online stated preference survey (see Online Appendix 1) was used to identify midwives’ preferences. Ethics approval was obtained from the University of Manchester Research Ethics Committee (Reference 13198). The online survey used a hybrid CA and DCE approach designed to identify which process and outcomes of newborn screening information provision were perceived by midwives to improve parents’ ability to make a decision about screening and to compare and contrast these preferences against the way in which information is currently provided in the English NBSP. Such hybrid models have previously been used in health and transport economics and allow the valuation of a large number of attributes that would be cognitively demanding if they had all been included in a traditional DCE.16–22 Hybrid experiments have been shown to produce similar estimates to DCEs containing all of the attributes and levels.19,20 The design used in this study was similar to the published hybrid stated preference survey used to elicit the preferences of parents for the process and outcomes of NBS information provision. 16
This hybrid study involved the linking of two subexperiments: a CA and a DCE. The DCE was used to value midwives’ preferences for the process of providing information in an NBSP. One of the attributes represented the effect of information on parents’ ability to make a decision about screening. As this attribute is subjective, the CA sought to understand what types of information affected parents’ ability to make a decision. The use of this mutual attribute allowed the comparison of relative preferences for types of information and the way in which such information is provided. The study design followed published guidelines.23,24
The Study Sample
The relevant study population was midwives working in the context of the NBSP. The study sample from this population was identified using Royal College of Midwives (RCM) facilitated contact with the heads of midwifery units in the United Kingdom. Due to difficulties in determining optimal sample sizes in DCEs, a pragmatic sample size of 150 midwives was set as the recruitment target based on the number of individuals recruited in previous maternity based DCEs and the research team’s experiences of recruiting midwives for other studies.25–27
Identifying Attributes and Levels
A range of methods was used to inform the selection and framing of attributes and levels for the CA and DCE sections. An initial list of attributes was identified by a systematic review of existing DCEs (n = 58) of maternity services, screening, diagnostic testing, and genetic testing. This review was based on a recent larger review of the DCE literature.28,29 Eleven attributes were identified that related to the types of information parents might want regarding screening, for example, how long they will need to wait for results. These attributes formed the CA task. Two attributes related to the way in which information was provided and were included in the DCE. To validate the attributes in the CA, existing information materials were examined to identify any additional types of information.3,30,31 Consultation with NHS-NBSP experts (n = 3) and semistructured interviews with midwives (n = 29), parents (n = 20), and NBSP regional quality assurance managers (n = 7) were also used to validate the attributes. Following these consultations and interviews, no additional attributes or levels were found. The draft set of attributes and levels were piloted in think aloud cognitive interviews 32 with registered midwives before finalizing. The final list of attributes for the CA and DCE are shown in Tables 1 and 2, respectively.
Attributes and Levels in the Conjoint Analysis

Each attribute had two levels (present or absent) in the design.
Attributes and Levels in the Discrete Choice Experiment

Categorical attributes that were effects coded.
Continuous attributes.
Experimental Design
The use of an appropriate experimental design ensures that the attributes and levels included in a stated preference survey are combined in such a way that accurate coefficient values, and therefore preferences, can be estimated from the rating/choice data. The CA was designed using an orthogonal main effects design, allowing the value that midwives place on different types of information to be estimated independently of the other types of information. 33 Each participant was required to answer six CA questions from a possible 24. For the DCE, NGene version 1.1.2 34 was used to create a D-efficient design with zero priors. Some combinations of attributes, such as high costs with Internet- or app-based information, were prevented from occurring together to improve the realism of the choice sets. Each participant in the DCE was randomized to answer one of four blocks of 10 questions to reduce the number of questions that each respondent answered.
The Survey
Training materials were included at the start of the survey to describe the purpose of the study and explain the attributes used. Respondents were also asked to watch a video embedded into the online survey that explained the role of an NBSP and why information provision may be important. They also received detailed information about how to complete each type of question they were shown. These types of questions were divided into five sections in the survey.
Section 1: The Effect of Information Provision on the Ability to Make Decisions About NBS
Respondents were asked to complete six CA questions each that asked them to consider a scenario in which some types of information were offered to parents and some types were not and some not given to parents. Figure 1 shows an example CA question. Respondents then had to rate how easy or hard they thought it would be for parents to make a decision about NBS given the type of information provided. They provided answers on a 5-point scale ranging from “It would be very hard to make a decision about screening” to “It would be very easy to make a decision about screening.” The framing of the CA questions allowed the effect of each type of information on the ability to make a decision to be identified.

Example of a question in the conjoint analysis
Section 2: Choosing the Best Way to Receive Information About NBS
In this task, respondents completed 10 DCE questions that asked them to choose what they perceived to be the best way for parents to receive information about screening from two possible scenarios or alternatively choosing that parents receive no information about NBS (see Figure 2). An opt-out was included to allow participants to choose to receive no information if neither of the presented alternatives were attractive to them. The framing of the DCE questions allowed the respondents’ preferences for the balance between process attributes, reflecting how to give information, with an outcome attribute (ability to make an informed decision). The DCE was linked with the CA through the attribute “ability to make an informed decision” that was the rating scale used in the CA questions.

Example of a question in the discrete choice experiment
Section 3: Making a Decision About NBS
Respondents were asked to state, using the standardized measure “Patients’ Preference for Control (PPC),” 35 how much involvement they believed parents should have when making the decision about whether a child was screened as part of an NBS program. There were seven possible responses grouped into three categories of possible decision involvement defined by Entwistle and others 36 : Passive, Active, and Collaborative. Examples of potential answers ranged from “I prefer that the midwife tells the parent what to do” (labelled as passive) to “I prefer that the parent make the decision without any information or recommendation from the midwife” (labelled as active) with “I prefer that the midwife and the parent make the decision together” (collaborative).
Section 4: Attitudes to Health Information
Respondents were asked a series of questions about how they use information to make decisions about their own health. These questions were taken from the Health Information Orientation Scale 37 and aim to measure the degree to which an individual would engage with health information and/or experience apprehension when dealing with health information. 38
Section 5: Background
The fifth section of the survey asked respondents to answer up to nine questions about themselves. These questions covered aspects such as gender, age, marital status, education, ethnicity, and whether the participant had previous children. Questions were also asked to determine how easy or hard respondents found the CA and DCE tasks and whether they had based their choices on a subset of attributes in the DCE, for example, whether midwives had only used one attribute to choose between the alternatives.
Recruitment
An email containing brief details of the study, a link to the online survey, and a participant information sheet was sent to heads of midwifery via the RCM who were asked to forward the email to their midwife groups. The first 100 midwives to complete the survey were emailed a £10 Amazon voucher as a “thank-you” for completing the survey. A Public Health England mailing list was also used to target screening coordinators. The primary inclusion criteria were that the midwives were currently registered to practice in the United Kingdom and were RCM members. In order to verify this, midwives were asked to supply their RCM registration number. This inclusion criterion may have excluded some midwives who were registered but not members of the RCM trade union. However, the alternative strategy of collecting midwives’ Nursing and Midwifery Council numbers would have resulted in the storing of data from which midwives could be identified. Midwives’ consent to take part in the study was assumed by their completion of the survey.
Survey Administration
Sawtooth Software SSI Web version 8.3.10 39 was used to create an online survey that was hosted on a secure university web ever. Sawtooth Software creates an excel spreadsheet in which participants’ responses were stored before being downloaded to a secure desktop computer. The email inviting participation in the survey was sent in November 2015, and data collection lasted for 1 month until December 2015.
Data Analysis
Responses to the questions in the “Making a decision about NBS,” “Attitudes to health information,” and “Background” sections of the survey were analyzed using descriptive statistics. The data elicited in the CA and DCE exercises were first analyzed separately. The CA data were analyzed using an ordered logistic regression model with cluster-adjusted standard errors to control for the panel nature of the data. 40 This model was used to identify the effect of each type of information on the perceived ability of parents to make a decision, which was coded on a 5-point scale from −2 (it would be very hard to make a decision) to 2 (it would be very easy to make a decision). The independent variables in the CA were coded as dummy variables such that the constants represented ability to make a decision in the absence of information, thereby aligning with the opt-out choice in the DCE.
The DCE data were analyzed using a conditional logistic regression model. This model was used to predict the effect of the presence of the different attributes and levels on the probability that a profile would be chosen, which was coded as either a “1” (for a chosen profile) or a “0” (if the profile was not chosen). The “ability of parents to make a decision” and “cost” were each coded as continuous variables in the main data analysis. In addition, a secondary analysis was conducted defining the attributes as categorical variables using effects coding to determine whether they exhibited nonlinearity. The “how” and “when” information is provided attributes were treated as categorical variables using effects coding in all analyses. This coding means that the results must be interpreted as relative to an “average” program of information provision rather than a specific base case. 41 The probability of a participant choosing the “no information” option was accounted for by using an alternative specific constant. 42
The conditional logistic regression model relies on the independence of irrelevant alternatives (IIA) assumption. The use of an opt-out choice in a DCE can violate this assumption as can be shown by drawing on an example presented by Ryan and Skåtun. 43 If a respondent has an increased probability of chosen Service A in the DCE then there should be an equal and proportional decrease in the probability of choosing both Service B and Service C. However, Service B is a service in which information is provided, and in Service C no information is provided and respondents may only directly choose between Service A and Service B. As such changes in the probability of choosing Service A may actually only affect the probability of choosing Service B, which could violate the IIA assumption. To test for potential violations of the IIA assumptions, a nested logistic regression was also conducted. This approach models participants’ choices as an initial choice between opting in or out to the service and a secondary choice between Services A and B if they chose to opt in. As part of the nested model a value (called tau [τ]) is estimated, which represents the degree of independence between the available choices in the model. If this value does not differ significantly from 1, there is insufficient evidence to suggest the IIA assumption has been violated and a standard conditional logistic regression can be used.
In this study, cost was used as a value attribute but the estimated monetary values were labelled as marginal rates of substitution (MRS) rather than marginal willingness to pay (WTP). There were still potential issues in the calculation of these MRS. The absolute values of the estimated MRS for each of the attributes and levels may have been biased due to the assumed linearity of the cost attribute, which was shown to not be valid especially for the highest levels assigned to cost. However, the relative ordering of the estimated MRS, which represents the relative contribution of each attribute to preferences, will not be affected by nonlinearity. As such the estimated MRS still provide a useful means of comparing between the relative preferences for the attributes and levels in the design and allow a link between the results of the CA and DCE. However, it would not be appropriate to use the estimated MRS to reflect marginal WTP and use them in other contexts such as in a cost-benefit analysis of different information provision approaches.
To calculate the MRS values for attributes in the CA, reflecting the types of information, the results from the two regression models (ordered logistic and conditional logistic) were linked. First, each information attribute was sequentially turned “on” while leaving the others “off” to identify the impact on parents’ ability to make a decision of each attribute. This value was multiplied by the estimated coefficient for parents’ ability to make a decision from the DCE. In turn, this value was then divided by the negative value of the coefficient for cost to obtain an MRS value for the information attribute. Further details regarding the linking of the subexperiments can be found in the technical appendix found in Wright and others. 16
Bootstrapping was used to generate confidence intervals for the MRS estimates for the types of information.16,22 To do this, the analysis was conducted 800 times, each on a sample of midwives randomly drawn from the original sample of 134 respondents with replacement.
Results
One hundred and thirty-four midwives completed the online survey. It was not known how many midwives received the email invitation, and it was not possible to calculate a response rate. The characteristics of the sample are summarized in Table 3. Only one participant was male and 98% (n = 131) of the midwives were between the ages of 25 and 64 years. The midwives worked in a range of settings, including the community (n = 69), hospitals (n = 46), and midwife-led units (n = 16). Most midwives were either a salary grade six (65%) or seven (24%). The mean survey completion time was 27 minutes.
Sample Characteristics
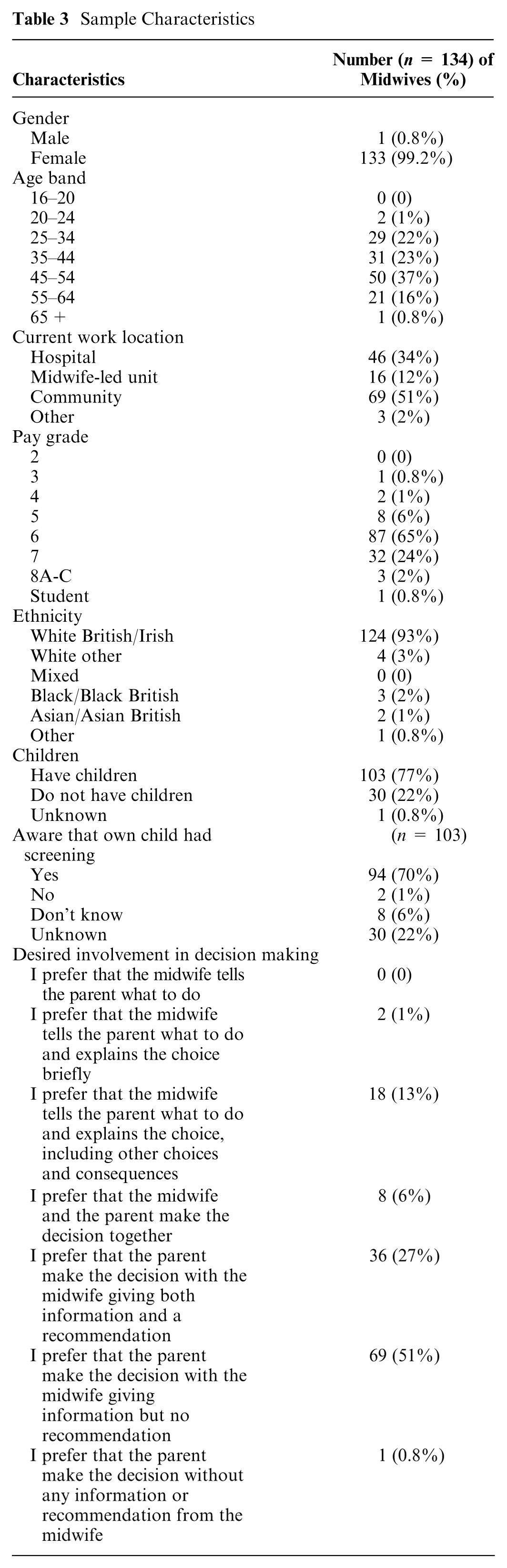
When asked about their views about how involved parents should be in decision making about whether their child should be screened in an NBSP, the modal response was that parents should make the decision with information from the midwife but no recommendation (n = 69, 51%). Regarding the three defined categories in the PPC, the majority of midwives thought that parents should have a level of decision making falling within the “active role” category (n = 106, 79%), while only 15% (n = 20) thought that the midwife should make the decision with the parent taking a “passive role.”
The results from the preference data are presented in three sections: 1) what information midwives perceive to help parents make a decision about screening, 2) how midwives believe information should be provided to parents, and 3) linking these preferences to determine the relative importance of each set of attributes. The midwives were asked how difficult they found answering the CA and DCE tasks. For both tasks the modal answer was that the questions were “easy” to answer.
Preference Results
What Information Helps Parents Decide Whether Their Child Should Have NBS?
Table 4 shows the results of the analysis of the CA data. Every type of information, with the exception of the possibility of receiving false-positive results, was perceived by midwives to be able to significantly increase parents’ ability to make a decision about whether their child should be screened as part of the NBSP. Each of the estimated coefficients was statistically significant at the <.001 level with the exception of the possibility of receiving false-negative results, which was significant at the <.05 level. Midwives perceived that the two types of information which most improved parents’ ability to make a decision were the names of the conditions being screened for and the way in which the sample is taken. Alongside the possibility of false-positive and false-negative results, informing parents about how test results would be received was perceived to be of a lower value by midwives.
Results of Ordered Logit Regression of Conjoint Analysis Data With Generated Marginal Rates of Substitution
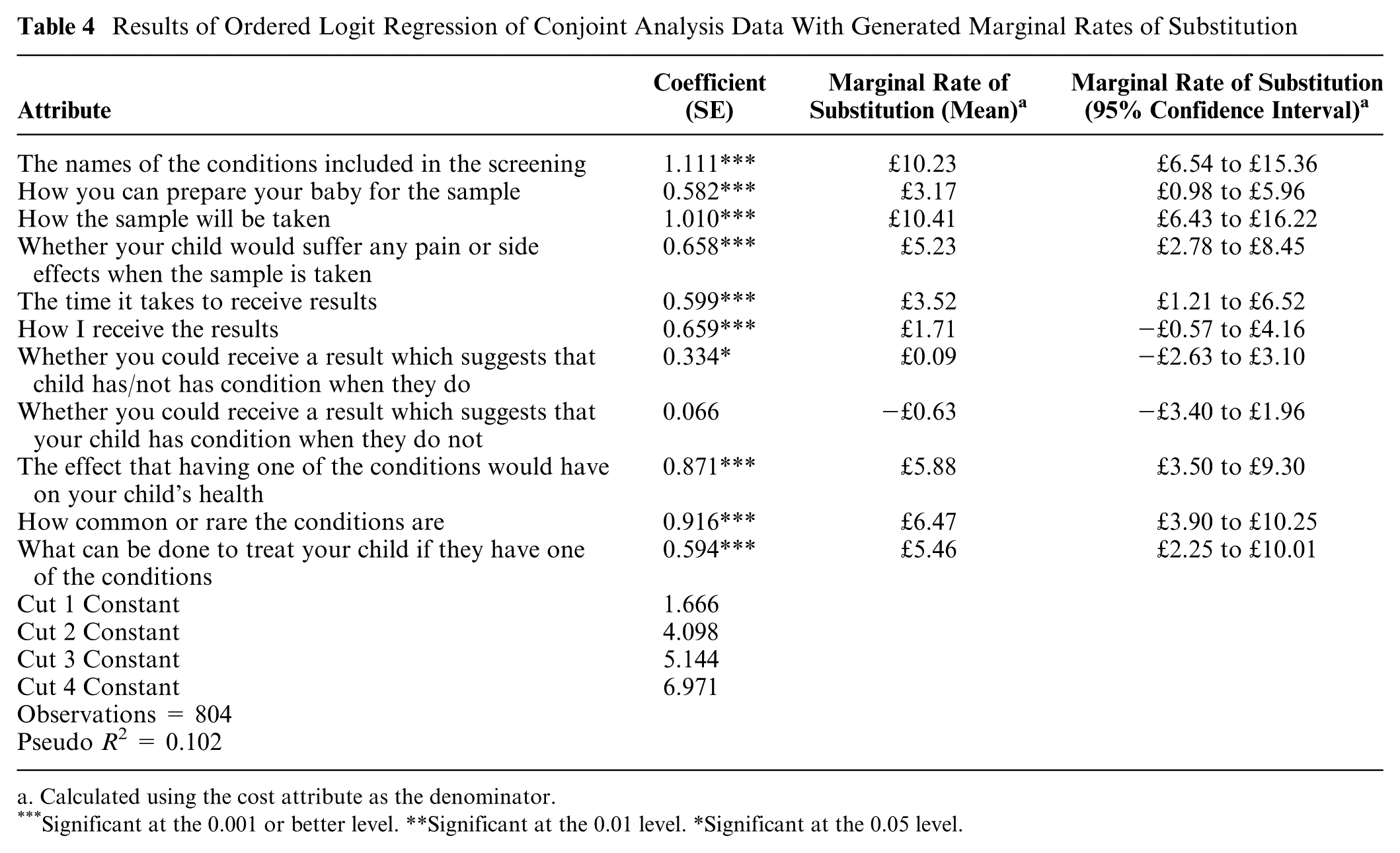
Calculated using the cost attribute as the denominator.
Significant at the 0.001 or better level. **Significant at the 0.01 level. *Significant at the 0.05 level.
How Information Should Be Provided to Parents
The results of the nested logistic regression suggested that the IIA assumption was not violated and that a conditional logistic regression would be appropriate (τ = 0.76, P = 0.2350). The results of the conditional logistic regression analysis of the DCE data are presented in Table 5. Initially, to test for nonlinearity in the ability to make a decision and cost attributes, these were analyzed as categorical variables. The cost attribute showed evidence of nonlinearity, with midwives disproportionately more likely to choose options that had a cost of £5. As the cost attribute was assumed to be linear in the main analysis, the MRS estimates may be biased and care should be taken with their use.
Results of the Conditional Logit Analysis of Discrete Choice Experiment Data With Generated Marginal Rates of Substitution

Calculated using the cost attribute as the denominator.
Significant at the 0.001 or better level. **Significant at the 0.01 level. *Significant at the 0.05 level.
Midwives’ choices revealed that the best times for parents to receive information was either late in pregnancy (MRS = £13.57; 95% confidence interval [CI] = £2.44 to £26.16) or on day 3 (MRS = £11.77; 95% CI = £1.23 to £22.61). The midwives believed that information should not be given before 20 weeks of pregnancy (MRS = −£23.29; 95% CI = −£36.43 to −£11.66). With regard to the mode of information provision, midwives preferred that this was provided in an individual discussion (£12.52; 95% CI = £2.79 to £22.60) and that parents should not receive the information from the internet (−£10.67; 95% CI = −£22.41 to −£0.78).
When asked if they had used a subset of the attributes to choose between the profiles, 40% of the midwives said that they had. Of these midwives, 65% stated that they had used the when information is given attribute, 53% used the how information is given attribute, 59% used the parents’ ability to make a decision attribute, and 37% used the cost attribute. This supports the evidence from the test of nonlinearity which suggested that midwives use heuristics when assessing the cost attribute.
The Relative Importance of the Content of Information and the Way in Which It Is Provided
Table 4 presents the MRS values that were generated for the information attributes in the CA when the results of the separate regression analyses were combined. All of these MRS values were statistically significant with the exception of the possibility of receiving false-positives or false-negatives and how results are received. The magnitude of the MRS values for information such as the names of the conditions (£10.23; 95% CI = £6.54 to £15.36) and how the sample is taken (£10.41; 95% CI = £6.43 to £16.22) show that midwives placed a significant weight on the content of the information that is provided to parents.
Discussion
This survey-based study quantified the preferences of midwives for providing information to parents within a nine-condition NBSP with respect to designing communication such that it maximizes parents’ ability to make a decision about screening. DCEs are used extensively to explore health-related preferences8,9 and have previously been used in the field of maternity to identify public and patient preferences for a range of interventions, including antenatal screening for Down’s syndrome, 44 general obstetric care, 45 and home versus hospital birth. 46 The survey reported in this article was the first to quantify midwives’ preferences for information provision as part of an NBSP. Furthermore, this study adds additional support to other published examples for the use of a hybrid design of stated preference study, using CA and a DCE, to effectively identify preferences for large numbers of attributes.16–22
To facilitate informed decision making, midwives perceived that parents needed a range of information about NBSP. Among these types of information were the names of the conditions being screened for and details about how the sample would be taken. Midwives did not think that parents’ decision making would benefit from knowing that false-positive or false-negative results would be possible. While a previous study of parents’ preference for NBS information found that information about false-positive results did help decision making, such information was among the lowest ranked in terms of importance. 16 Previous research has suggested that repeat tests following false-positive results and inadequate samples may be a significant cause of anxiety in parents during the screening process.4–6 Further research is required to determine why midwives and parents may place a low value on information about repeat tests when such results can cause significant anxiety.
The survey also suggested that a sample of practicing midwives believed that parents should make the decision about whether their child should be screened, with the midwife providing information but no recommendation. This is not consistent with current policy, which suggests that a recommendation in favor of screening should be given, and this position has also been found to be preferred by parents.16,30 Previous studies have highlighted a conflict may exist between the aims of maximizing the uptake and benefits of screening and ensuring that parents make a free and informed decision about screening, 47 and this study may provide evidence that midwives are not comfortable with these dual objectives.
When comparing the preferences of service providers (midwives) and users (parents), it is not clear whose preferences should take precedence when using the information to change current practice. In the United Kingdom, information is currently given after the baby is born and it is less likely to be given late in pregnancy. 30 Midwives had a preference for providing information in the third trimester of pregnancy, which is consistent with two published studies48,49 but contradicts the findings from the study that used the same hybrid design in a sample of parents who expressed a preference for information early in pregnancy. 16
Another published study identified that providing this information early in pregnancy may result in parents losing the leaflet or forgetting the information by the time a decision must be made about screening. 50 This contradictory information introduces a challenge for policy makers about whether to change existing approaches to the timing of information provision and suggests a need to be clear whether the preferences of service users or service providers should be used.
This study had some limitations. The results of this study only reflect the preferences of the recruited sample of midwives. The sample of midwives who were recruited for this study (n = 134) was smaller than the targeted sample size. Previous maternity based DCEs have varied significantly in sample size, ranging from 78 participants 45 to 877 participants. 51 However, previous studies have focused on the preferences of members of the public or pregnant women. Samples of health professionals have been shown to have lower response rates to DCEs than patients 52 and comprise a smaller population than the public. Both of these factors may be implicated in our difficulty with recruitment.
The estimated MRS from this survey cannot simply be interpreted a WTP for a unit change in each attribute. Midwives were asked to act on behalf of parents and make a judgement about the acceptable level of cost for gaining information. The difficulty in judging acceptable levels of cost for others may be one of the reasons why relatively few midwives (37%) stated that they used cost to decide between profiles.
There were further potential issues with the interpretation of the estimated MRS, which relied on using a cost attribute that did not exhibit linearity. This means the absolute values of the estimated MRS for each of the attributes and levels were likely to be biased due to the absence of linearity. However, it was valid to compare the relative values of the estimated MRS within this study. The estimated MRS still provided a useful means to create a quantifiable link between the CA and DCE by allowing the comparison of the relative values of each attribute and level. However, it would not be appropriate to use the estimated MRS in other contexts such as in a cost-benefit analysis of approaches to provide information in an NBSP.
The method used to link the CA and DCE relied on the assumption that the standard errors associated with the attributes and levels in each task were independent. 22 In other words, the choices in one task must be independent of the attributes and levels appearing in the other. The estimated MRS values represent averages taken from bootstrapping the analysis with 800 replications. In theory, the analysis should account for heterogeneity in the preferences of midwives. 23 Midwives with different characteristics, such as years of work experience, may have different preferences for information provision. However, it was not feasible to take account of heterogeneity due to the small sample size and use of the hybrid CA-DCE design. This is because it is unclear how the two subexperiments could be linked when they are divided into different samples. To date no hybrid DCE had addressed the inclusion of heterogeneity in the analysis.16–22
Conclusion
This study has quantified the preferences of a sample of practicing midwives for the content and process of information provision regarding an NBSP that reflects the current nine-condition program used in the United Kingdom. The results suggested that midwives perceived that moving antenatal information provision to later in pregnancy may improve parents’ ability to make a decision about screening and emphasis should be placed on providing information in an individual discussion. Further research, using observational methods, should be undertaken to investigate the potential cost implications and impact on outcomes of altering existing information provision, particularly given the continued potential for expansion of the UK NBSP.
Footnotes
Acknowledgements
The authors would like to thank the midwives who participated in this study. Thanks also go to Dr. Ewan Gray who provided advice regarding the design and analysis of this study.
This work was funded by the National Institute of Health Research Health Technology Assessment Programme Project Number 11/62/02. This article presents independent research funded by the National Institute for Health Research (NIHR). The views expressed are those of the authors and not necessarily those of the NHS, the NIHR, or the Department of Health.
Supplementary Material
Authors’ Note
This work has previously been presented at the 36th Annual North American Meeting of the Society for Medical Decision Making (“Developing a Stated Choice Experiment to Understand Preferences for Information Provision in an Expanded Newborn Bloodspot Screening Programme”) and the 37th Annual North American Meeting of the Society for Medical Decision Making (“A Stated Choice Experiment to Investigate Preferences for Information Provision in Newborn Bloodspot Screening Programmes”).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.