
Abstract
Childhood vaccinations have been highly effective in reducing the incidence of, and associated morbidity and mortality from, a range of infectious diseases. 1 To achieve herd immunity, the World Health Organization recommends that coverage of most childhood vaccinations is at least 90%, and 95% for diphtheria and measles.2,3
At the time of the research, the schedule of recommended vaccinations offered by the National Health Service in England for low risk, prescho-ol children (up to age 5 years) was 14 injections plus two orally administered vaccines given over a minimum of eight visits between 2 months and 5 years of age. In England, preschool vaccinations are routinely delivered by primary care doctors, or nurses, at primary care centers. These vaccinations are recommended but are not mandatory either before or on entry into school. Coverage of preschool vaccinations in England is generally high—nearing or exceeding the World Health Organization recommendations in most cases. 4 However, these high overall coverage rates hide wide geographical variations, with coverage of some vaccinations being lower than 80% in some areas. 4 These variations persist into school years.
This has prompted interest in exploring new ways of increasing preschool vaccination uptake. 5 One method of doing this that has received attention is offering financial incentives to parents who keep their children up-to-date with their vaccinations. 6
A recent systematic review identified only three robust outcome evaluations of parental financial incentives for preschool vaccinations. 6 All of these studies were conducted in the United States, with mixed results. On the basis of absence of evidence, the review drew no overall conclusion on the effectiveness of these interventions. Financial incentive interventions can also be controversial.7–9 This is particularly the case in contexts such as the United Kingdom where there is little experience with financial transactions for health care, and where such interventions are likely to be funded through general taxation. Given previous controversies surrounding financial incentives for health behaviours, 9 it is highly unlikely that a parental financial incentive program for preschool vaccinations would be implemented in a setting such a England—even if it were restricted to research—without first confirming that this would be acceptable to parents, and other stakeholders. 10
The best overall measure of intervention acceptability is probable take-up of that intervention (i.e., revealed acceptability). 11 However, where an intervention has not yet been implemented, the views of relevant stakeholders (i.e., stated acceptability) is the best measure of acceptability available.
Few studies exploring acceptability of parental incentive schemes for preschool vaccinations were identified in a recent systematic review. 6 Qualitative research with parents and health visitors conducted in London found they were not generally supportive of linking welfare payments to vaccination status, due to concerns about undermining parental choice. 12 In Australia, where some universally available child care welfare benefits are linked to children’s vaccination status, parents report that obtaining these benefits is not an appropriate reason for vaccinating their children. 13 These findings are supported by recent research from the United Kingdom where parental financial incentives for preschool vaccinations were interpreted as “bribes,” by both parents and health professionals, that could undermine norms of responsible parenting. 14 However, in the United States, linking welfare benefit payments to children’s vaccination status was reported as fair and motivating to the majority of parents. 15
When asked about the acceptability of parental financial incentives for preschool vaccinations, and other health behaviors, many respondents spontaneously propose a range of other methods to achieve the desired outcomes.7,9,14 In the case of preschool vaccinations, these include more flexible appointments and more accessible information about the pros and cons of vaccination.
Qualitative research can provide useful insights into what aspects of parental financial incentive schemes for preschool vaccinations are and are not acceptable and why; and how vaccination services could be made more acceptable in general. However, qualitative findings are not necessarily generalizable, and relative preferences for different aspects of the service cannot be determined. While a survey could begin to address these issues, vaccinations services are complicated, consisting of a range of different aspects, all of which can vary. Furthermore, the frequency with which parents spontaneously discussed other aspects of the preschool vaccination program that they felt could be organized better led us to believe that it might be hard to ask them to focus on acceptability of financial incentives in the absence of other potential changes to the organization of preschool vaccination services. In order to more formally explore how preferences for financial incentives for preschool vaccinations varied alongside various other aspects of organization of preschool vaccinations, we conducted a discrete choice experiment (DCE).
Discrete choice experiments offer an additional approach to investigate acceptability of interventions. We conducted a DCE with the aim of identifying relative preferences for parental financial incentives for preschool vaccinations, as well as other aspects of preschool vaccination services in England. We compared preferences of parents identified as “at high risk” of incompletely vaccinating their children with those “not at high risk.” It is particularly important to explore the preferences of parents “at high risk,” as this subgroup would probably be the primary target of any parental incentive scheme. We also considered it important to explore the preferences of parents who were “not at high risk” in order to determine the wider impact of population-wide changes in the configuration of vaccination services.
Methods
Discrete choice experiments describe interventions according to their key characteristics, or “attributes” (e.g., type of reward, value of incentive), and “levels” of these attributes (e.g., cash, shopping voucher; higher, lower values). Participants are then asked which of a small number of intervention “scenarios,” combining different levels of each attribute, they prefer. This allows relative preferences for attribute levels to be determined when comparing preferences for particular attribute levels to a reference level. DCEs are well established in health economics16–18 and increasingly used in public health.19–21 We followed best practice recommendations for conducting a DCE,22,23 collecting data from UK adults in an online survey. Ethical approval for all aspects of this study was granted from Newcastle University Ethics Committee (Reference 00748).
Identification of Attributes and Levels
We used a systematic review, 6 qualitative interviews, 14 and discussions with a project advisory group of parents and guardians of preschool children to identify attributes, and levels, of preschool vaccination programs that are likely to influence acceptability of vaccinations (see Table 1). We specifically included aspects of a parental financial incentive program in this. In all cases, all attributes and all levels chosen were realistic and plausible in policy terms.22,23
Attributes and Levels Included in the Discrete Choice Experiment

The first attribute included was “type of parental reward.” The most common types of financial incentive offered for healthy behaviors in research settings are cash rewards and shopping voucher rewards. 24 Shopping vouchers help allay common concerns that recipients will use incentives for “unhealthy” behaviors, such as purchasing cigarettes. 7 In addition to cash and shopping voucher reward levels, we also included a no reward level for this attribute. Total value of parental financial rewards were based on values used in previous research, 6 scaled across five levels from £0 to £280 (€0 to €370; US$0 to $400). A third attribute included “which parents would receive a reward.” This included targeted rewards (given to parents considered unlikely to have their child immunized) and universal rewards (given to all parents). This is based on previous research where incentives have only been offered to those parents whose children are not up-to-date with their vaccinations. 25
Qualitative interviews identified that parents felt that it could be helpful for a wider range of professionals to provide preschool vaccinations in a wider range of settings to that currently available. Based on these interviews and feedback from the parental advisory group, the attribute “type of healthcare professional administering vaccinations and location of appointments” had six levels (Table 1).
Our parental advisory group specifically identified that current information on the risks and benefits of preschool vaccinations was not optimal. Two attributes related to this were included: “how information about vaccinations is provided prior to the appointment,” which focused on mode of information delivery (written, electronic, or multimedia); and “how information on the risk of your child getting diseases is provided prior to the appointment,” which focused on whether information was in the form of number, or charts and pictures.
Parents provided substantial feedback on the limited availability and long waiting times for vaccination appointments. Two attributes on these issues were included “availability of appointments” and “waiting time at each appointment.”
Experimental Design
The combinations of attributes and levels described in Table 1 would generate 14,580 unique scenarios (6 × 3 × 3 × 2 × 3 × 5 × 3 × 3); far too many to be considered by any one individual. Instead, a D-efficient design was generated using Ngene design software (v 1.1.1). 26 This resulted in 72 experimental scenarios (“choice sets”) being required to estimate both main effects for each attribute and key interactions between attributes. However, 72 choice sets is still too many to be considered by any one individual. Thus, the 72 choice sets were randomly divided into four blocks of 18 choice sets each, with participants randomly assigned to one of these four blocks.
Each choice set of experimental scenarios was combined with a third option of “neither” (do not like either option—I would not have my child vaccinated). This opt-out option reflects policy in the United Kingdom where vaccinations are not mandatory. In all choice sets it was stated that the number of appointments required to complete the full vaccination program was eight. This is the minimum required to complete the current recommended program in England. An example choice set is provided in Figure 1.
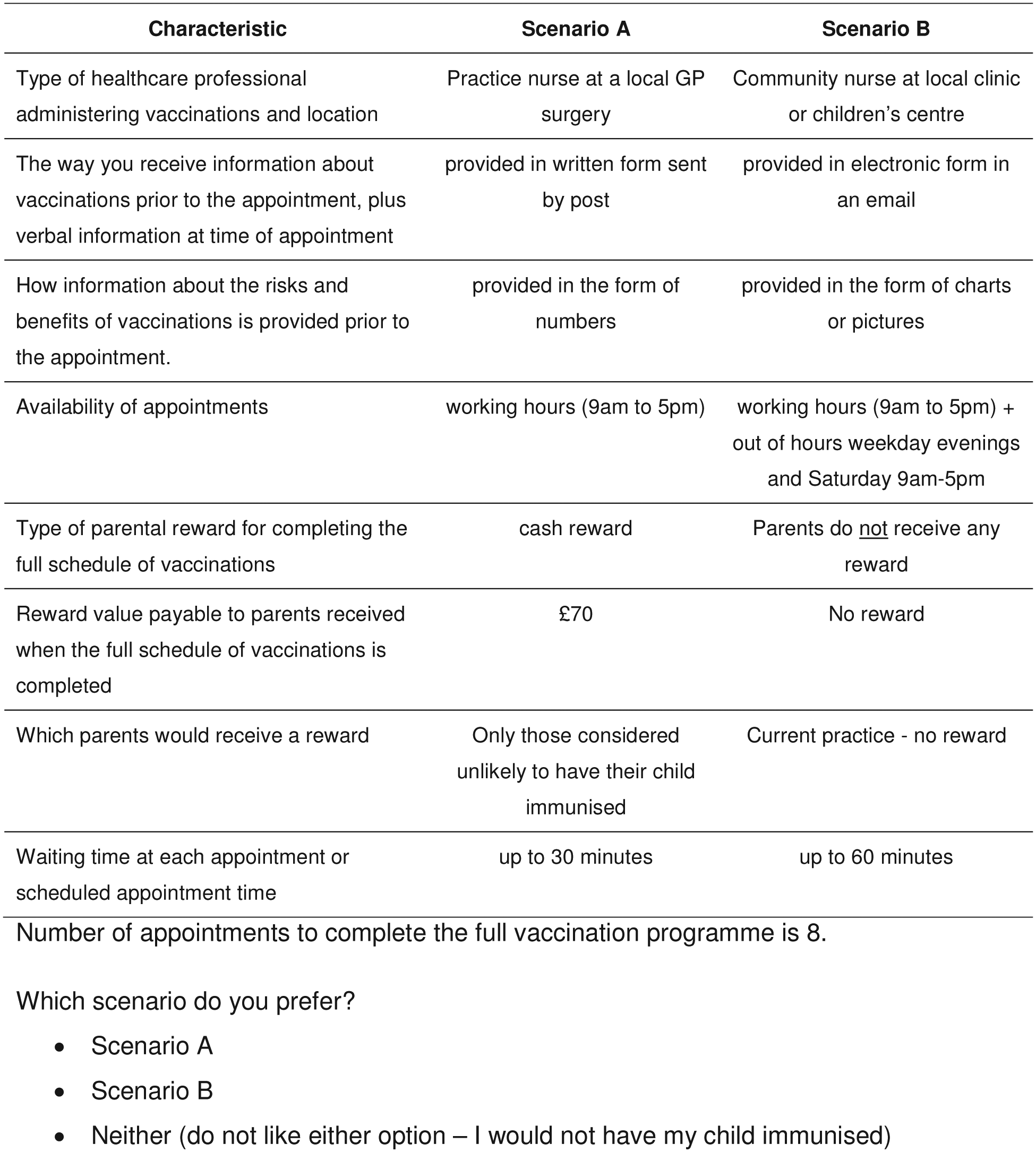
Example choice set
Choice sets were embedded in a wider questionnaire. This collected information on basic sociodemographics (in order to characterize the sample).
Pretesting and Data Collection
Pretesting was undertaken with five parents or guardians of preschool children (one male and four females) using a paper version of the questionnaire and a “think-aloud” approach. 27 This explored respondents’ understanding of the wording of questionnaire survey items, and the DCE choice task resulting in some changes to wording and layout.
Recruitment and data collection was undertaken by a market research company (ResearchNow.com) who adhered to the highest standards of market research ethics. 28 Main data collection took place via an online survey. An internal pilot analysis of the first 77 responses identified that the majority of respondents (82%) stated that they fully understood the DCE. Data collection proceeded and these 77 respondents were included in the final sample.
Participants and Sample Size
Parents or guardians who were 18 years or older, had one or more children aged less than 5 years old, who were currently residing in England, and who were members of ResearchNow’s online panel were eligible to participate in the study.
Using “by invitation” methods individuals with known characteristics were directly targeted by ResearchNow to stratify participants into one of two subsamples in terms of their likelihood of not having their children fully vaccinated. Respondents who additionally met one of the following five evidence-based criteria were used to stratify participants into a subgroup group of parents/guardians who were at high risk of not fully vaccinating their children5,29–32: live in one of the 20% most deprived areas of England (identified by Index of Multiple Deprivation 2010 score of lower super output area of residence, calculated from postcode of residence); have a preschool child with a physical or mental disability; are a single parent or guardian; are aged less than 20 years; and are the parent/guardian of more than three children (of any age). Participants that did not meet any of these five criteria were stratified into a subsample of parents/guardians who were “not at high risk” of fully vaccinating their children. ResearchNow were tasked with recruiting 250 participants within each subsample.
All participants were provided with written information on the study before taking part and indicated their consent to take part before data collection took place. As per ResearchNow’s normal procedures, participants received small (£2; ~$US3/€2.5) shopping voucher as incentives to take part.
Optimal sample size requirements for DCEs depend on knowledge of the true choice probabilities, which are not known prior to undertaking the research. 33 For this reason, DCE sample size estimates are generally based on previous research, rules-of-thumb, and budget constraints. Given the number of attributes included in the DCE, it was estimated that a minimum sample size of 400 (i.e., 200 high risk [50 per block], plus 200 not at high risk [50 per block]) would provide sufficient statistical power.
Statistical Analyses
Data were analyzed for all respondents and separately for two groups based on whether or not participants met any of the criteria for being “at high risk” of not fully vaccinating their children. Mixed logit models were used to establish whether the eight attributes presented in the choice scenarios were statistically significant predictors of participants’ preferences in either group. In all models, intercepts (alternative specific constants) and the “waiting time at each appointment” attribute were assumed to be random and normally distributed (mean and standard deviations reported); all other parameters in the model remained fixed (mean estimates reported only). Effects coding was used for all attributes with the exception of “waiting time at each appointment” and “parental reward value,” which were assumed to be linear. The level “no reward” in the attribute “type of reward” was omitted in these analyses due to multicollinearity and only additionally included in the choice sets descriptions for plausibility.
Trade-offs between attributes were considered as marginal rates of substitution (MRS) between all statistically significant attributes in the mixed logit models and the continuous variables, value of reward and waiting time. Hence, marginal willingness to accept (WTA) values were calculated in the form of a minimum monetary value that would be required as “compensation” for any change in the level of an attribute associated with losses in utility. Similarly, marginal willingness to wait (WTW) values indicate the maximum time respondents would be willing to sacrifice for any change in the level of an attribute with increases in utility. Comparing MRS values allows the relative strength of preferences for each attribute to be compared. For attribute levels with negative preferences, that is, where disutility is experienced when moving from the reference level to a different attribute level, positive WTA and negative WTW values indicate the minimum level of compensation (monetary or in terms of reduced waiting time) participants would be willing to accept to make up for the absence of the preferred reference level. For attribute levels with positive preferences, that is, where moving from the reference level to a different attribute level is associated with a utility gain, positive WTW values indicate the maximum sacrifice in terms of increased waiting time respondents would be willing to make for a level preferred to the reference level. Negative WTA estimates are included for completeness, but do not have any immediate policy implications.
Results
Complete data were collected from 521 participants—259 in the “at high risk” group and 262 in the not “at high risk group.” Characteristics of participants are described in Table 2. As would be expected from the criteria used to define “at high risk” participants, participants in this group were more likely to be single or separated/divorced/widowed, more likely to live in households with the lowest income, and less likely to live in households with the highest income, less likely to have obtained a degree, less likely to be employed and more likely to be unemployed, more likely to have a child with a disability, and had more children overall than participants not in the “at high risk” group.
Characteristics of the Sample
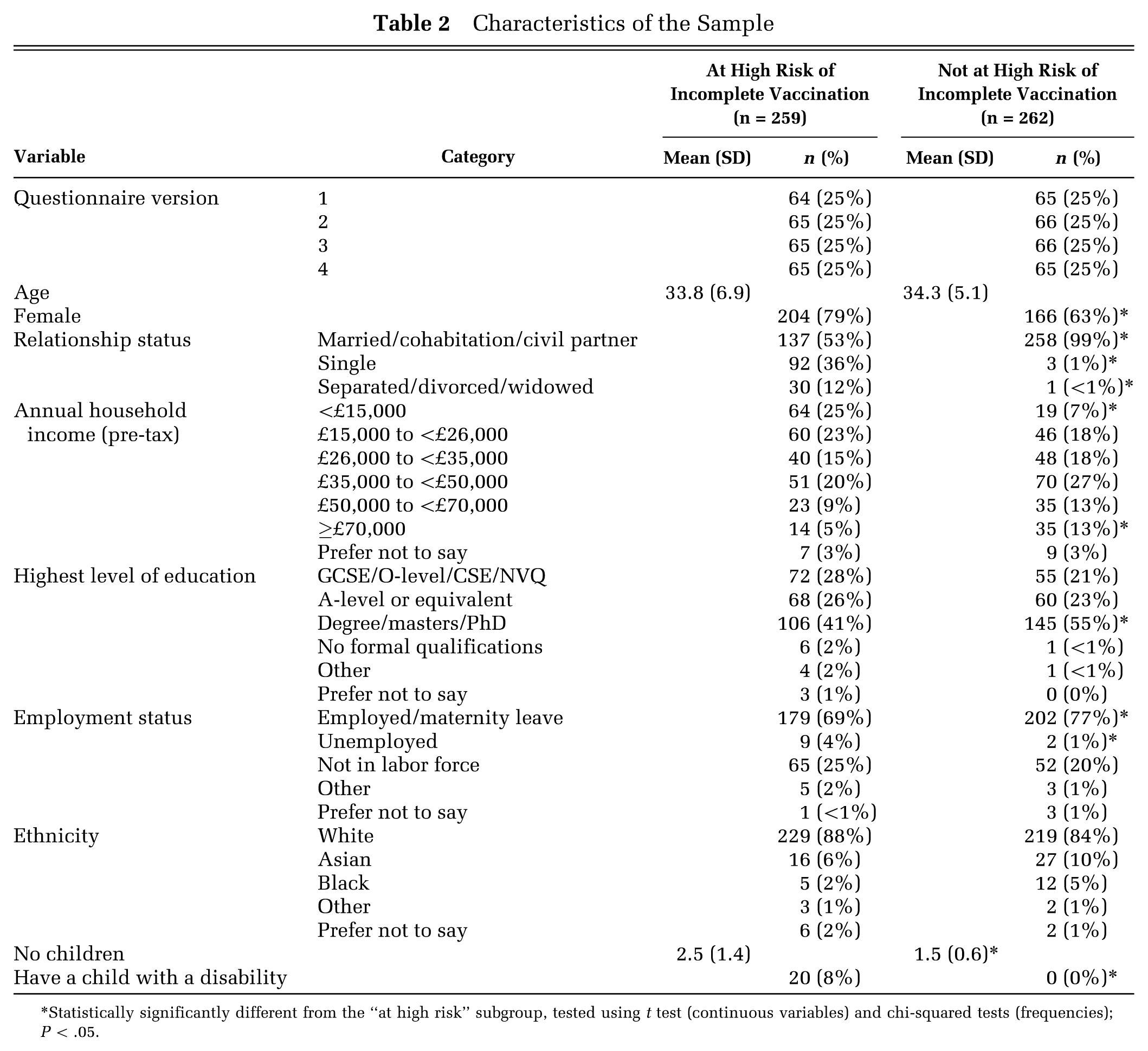
Statistically significantly different from the “at high risk” subgroup, tested using t test (continuous variables) and chi-squared tests (frequencies); P < .05.
Table 3 shows the results of the mixed logit models. Here, positive coefficients represent a positive preference (utility) associated with a particular level of an attribute compared to the reference level, whereas negative coefficients represent a negative preference (disutility). Statistically significant differences are marked, and WTA values for these calculated. Scenarios A and B were the most frequently chosen options, making up for 48% and 47%, respectively, of responses. The opt-out option was chosen for 5% of choices. Out of the 38 respondents who chose the opt-out option, the majority (n = 25) did so constantly across all choices presented to them.
Summary of Mixed Effects Logit Regression Models
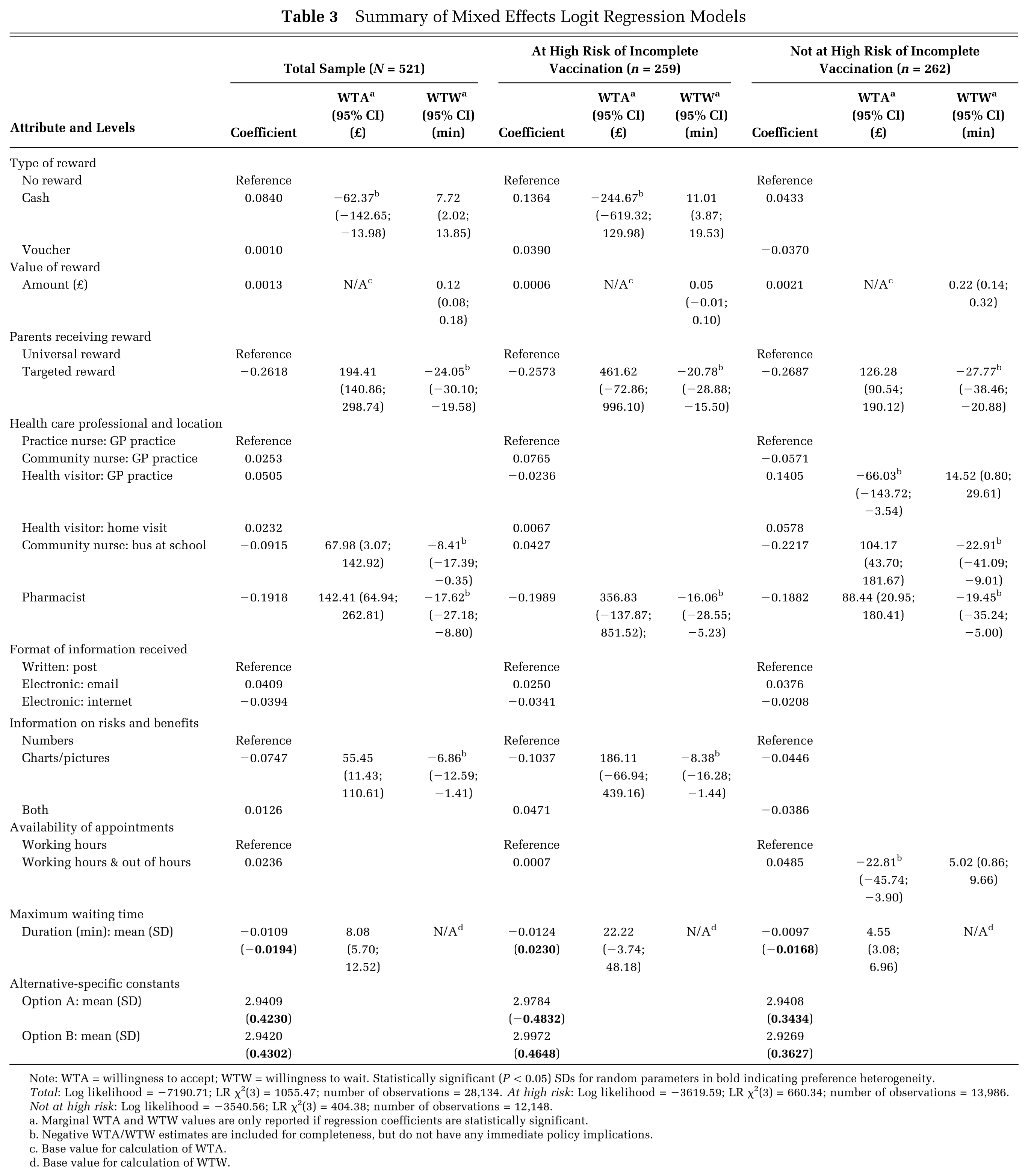
Note: WTA = willingness to accept; WTW = willingness to wait. Statistically significant (P < 0.05) SDs for random parameters in bold indicating preference heterogeneity.
Total: Log likelihood = −7190.71; LR χ2(3) = 1055.47; number of observations = 28,134. At high risk: Log likelihood = −3619.59; LR χ2(3) = 660.34; number of observations = 13,986. Not at high risk: Log likelihood = −3540.56; LR χ2(3) = 404.38; number of observations = 12,148.
Marginal WTA and WTW values are only reported if regression coefficients are statistically significant.
Negative WTA/WTW estimates are included for completeness, but do not have any immediate policy implications.
Base value for calculation of WTA.
Base value for calculation of WTW.
Participants who were “at high risk” of incompletely vaccinating their children had a significant preference for cash rewards compared to no rewards (WTA −£245). However, there was no difference in preference for voucher compared to no rewards in these participants. There was no difference in preference across any of the levels of “type of reward” in participants who were not “at high risk” of incomplete vaccination. Only participants who were not “at high risk” had a preference for higher value rewards. Both subgroups expressed a significant negative preference for targeted rewards that was substantially stronger in those “at high risk” (WTA = £462) compared to those “not at high risk” (WTA = £126).
There was statistically significant disutility associated with vaccinations delivered by pharmacists, compared to practice nurses, in both groups. This was substantially stronger in the “at high risk” group than the “not at high risk” group (WTA = £357 and £88, respectively). In the “not at high risk” group there was also a significant negative preference for vaccinations delivered by community nurses in buses located near schools (WTA = £104) and significant positive preference for health visitors providing vaccinations in the community (WTA = −£66).
There were no differences in preferences for how information on the risks and benefits of vaccination was received in either group. However, parents “at high risk” of incompletely vaccinating their children had a significant disutility associated with information in the form of charts and pictures compared to information provided as numbers along (WTA = £186).
Parents “not at high risk” had a preference for vaccination appointments being available out of hours as well as during working hours (WTA = −£23). This was not seen in those parents who were “at high risk.” Both groups preferred shorter waiting times, although this preference was stronger in those “at high risk” compared to those “not at high risk” (WTA values for each additional minute waited after 30 minutes was £22 and £5, respectively).
Discussion
Summary of Findings
This is the first DCE we are aware of that has investigated parental preferences for changes that could be made to preschool vaccination (children up to age 5 years) services. It is also the first DCE we are aware of to explore parental preferences for financial incentives for preschool vaccinations. There was no difference in preference for cash or voucher incentives compared to no incentive in those parents “not at high risk” of incomplete vaccination. Parents who were “at high risk” expressed a positive preference for cash, compared to no incentive. Both groups preferred universally available rewards, compared to those targeted at just some groups. There were also significant preferences for shorter waiting times. While parents “not at high risk” preferred vaccinations delivered by a health visitor, rather than practice nurse, at a GP surgery, there was a significant disutility associated with vaccinations delivered in other locations and by other professionals. Parents “at high risk” of incomplete vaccination preferred information on the risks and benefits of vaccinations to be provided as numbers, and not as charts or pictures.
Interpretation of Findings
Little previous work has explored acceptability of parental financial incentives for preschool vaccinations. 6 We found no difference in preference for cash and voucher incentives over no incentives in parents “not at high risk” of incomplete vaccination, and a positive preference for cash incentives over no incentives in those “at high risk.” This indicates that the acceptability of health promoting financial (cash or voucher) incentives in the context of preschool vaccinations may differ as a function of population characteristics.
Another DCE exploring preferences for financial incentives for smoking cessation, physical activity, and attendance of adults for vaccinations and screening also found that cash or shopping vouchers incentives were preferred as much or more than no incentives. 34 These findings (along with those of the current DCE) are in contrast to qualitative work and surveys, which tends to find that incentives are generally not considered acceptable.7–9,14
Differences in findings between previous qualitative work and the present DCE may reflect differences in participants, or differences in the context in which questions are asked. It is possible that DCE participants feel less inhibited by the anonymity of Internet data collection, while qualitative data are more subject to social desirability bias. Alternatively, participants in qualitative research often spend at least an hour discussing topics and so may arrive at more considered opinions than those taking part in DCEs. Further research is required to understand why findings related to preferences for financial incentives for healthy behaviors appear to consistently differ when explored using DCE versus qualitative methods.
The finding that targeted rewards were much less acceptable than universal rewards reflects some, but not all, previous findings. Some qualitative work has found that financial incentives for other health behaviors are more acceptable when targeted at “vulnerable” groups such as those living in low-income circumstances.7–9 However, other work focused on preschool vaccinations reflects the current preference for universal financial incentives. 14 A similar preference for universal incentives was found in a DCE on preferences for financial incentives across a range of healthy behaviours. 34
The positive preference for cash rewards by parents in the “at high risk” group may be attributable to their income status. Increasing value of a reward was only associated with significant utility in those “not at high risk.” Thus, the offer of any reward may be particularly salient for some (perhaps less affluent), while others are more strongly influenced by the value of the reward offered. While recipient socioeconomic position has been postulated as a determinant of effectiveness of health promoting financial incentives, with those of lower socioeconomic position being assumed to be more responsive, 8 little work has investigated this association. 24
Our qualitative work suggested that more flexibility in where vaccinations are delivered was preferred. 14 However, this was not reflected in our DCE. The DCE findings may reflect perceptions concerning which professionals have adequate training and which locations are “safe” for vaccination delivery—although it is surprising that these issues were not also raised in qualitative interviews.
There is robust evidence that graphical displays such as bar graphs and pictographs can effectively support communication of balanced probabilistic information to people irrespective of health literacy level. 35 However, parents “at high risk” expressed a negative preference for this sort of information. More research is needed to engage parents in an iterative co-design process to develop optimally acceptable and usable information that conveys robust and balanced data on the benefits and risks of vaccinations.
Implications of Findings for Policy, Practice, and Research
Our findings indicate that parental financial incentives for preschool vaccinations would be no less acceptable to parents than the current practice of not offering such incentives. If evidence emerges supporting the effectiveness of such schemes, then parental acceptability is unlikely to be a substantial barrier to implementation. However, any incentives would have to be offered universally to maximize acceptability. Similar work in relevant professionals and the wider public is required to establish how acceptable they consider such incentives—as this may also influence how easy it is to implement.
Parents, understandably, prefer shorter waiting times for vaccination appointments. Avoiding block bookings—where many people are given the same appointment time and then seen on a first come, first serve basis—is likely to help in this regard. Offering out-of-hours appointments was only preferred by parents who were “not at high risk” of incomplete vaccination, indicating that this may not have a substantial impact on vaccination uptake. Providing more flexible vaccination delivery—by a range of providers in different locations—met with mixed reactions, and furthermore, careful consideration is required before any substantial changes are made in this regard. More work is required to develop effective (in terms of communication) and accessible information of the risks and benefits of preschool vaccinations.
Strengths and Limitations of Methods
The strength of the DCE approach is that it allows relative preferences for multiple factors that may influence decision making to be explored. Moreover, we incorporated WTA terms into the analyses to facilitate the interpretation of results.
We followed best practice recommendations for conducting and designing a DCE, with combinations of attributes and levels presented in scenarios that were designed to minimize potential for bias. In order to increase the validity of our findings and reduce bias from respondents’ use of shortcuts, heuristics, or random choice, we 1) ensured scenarios were realistic and plausible in policy terms; 2) utilized best practice methods to minimize the number of scenarios presented to participants; and 3) tested the designed scenarios using a think-aloud protocol during the pretesting stages.
We were also able to compare results from two contrasting groups of parents and guardians—those “at high risk” and those “not at high risk” of incompletely vaccinating their children. In some cases preferences between the two groups were different. This indicates that the two groups cannot necessarily be combined and provides some indication of what changes to services might be particularly helpful in increasing uptake among those currently “at high risk” of not vaccinating. These nuances and differences would not have been captured in a more population representative sample. Throughout, we were careful to follow best practice guidance for the conduct of DCEs,22,23 and to ensure that the attributes and levels used were both evidence-based and plausible in policy terms.
Given the lack of empirical evidence, we did not explore differences in preferences as a function of how many criteria for being at high risk of not fully vaccinating their children parents/guardians achieved. However, we acknowledge this may have yielded a differential pattern of results and should be explored in future work in this area.
The sample was effectively a convenience sample, meaning it may not be representative. Furthermore, by using the recruitment method we did, it is not possible to determine response rates to the survey. Previous DCE research suggest that alternative methods of recruitment and data collection, such as random postal or telephone surveys associated with time and budget constraints, achieve very low response rates, which also threatens representativeness. 36 By using an opt-in panel it is possible that our results were skewed by “professional responders,” who could be assumed to be more likely to use shortcuts, heuristics, or random choice when completing questionnaires, which may reduce the quality of responses. However, recent findings indicate such responders are unlikely to represent a significant threat to validity of findings. 37
We combined health care professional delivering immunizations and the place of delivery of immunizations into one attribute. Although these may be seen as separate constructs, they are inextricably linked and this was noted by our parental advisory group. Separating them out would have imposed a prohibitive number of design constraints, which would have had negative implications for the model parameters and conclusions that could be drawn from the results.
Conclusions
We identified that universal “high value” rewards, in the form of cash payments for parents/guardians, are likely to be acceptable within populations at high risk of incomplete vaccination without any negative impact on current high uptake rates of parents/guardians who are not at high risk of incomplete vaccination. The cost of incentives could be offset by offering additional flexibility in terms of alternative community settings for vaccinations and out of hours appointments. Further work is required to develop methods of communicating risks and benefits of vaccinations that are both optimally effective and accessible to parents/guardians. Mandatory schemes may be more acceptable alternatives to incentives, and further research should investigate parental preferences for organization of such schemes.
Footnotes
This study was funded by the UK National Institute for Health Research Health Technology Assessment Programme (11/97/01). The views and opinions expressed herein are those of the authors and do not necessarily reflect those of the HTA Programme, NIHR, NHS, or the Department of Health. JA is currently funded by the Centre for Diet and Activity Research (CEDAR), a UKCRC Public Health Research Centre of Excellence. Funding for CEDAR from the British Heart Foundation, Cancer Research UK, Economic and Social Research Council, Medical Research Council, the National Institute for Health Research, and the Wellcome Trust, under the auspices of the UK Clinical Research Collaboration, is gratefully acknowledged. The funders had no role in study design, data analysis, report writing, or choice of publication. Ethical approval for all aspects of this study was granted from Newcastle University Ethics Committee (Reference 00748).