
Abstract
Mental health illnesses are prevalent1,2; large numbers of people are diagnosable with a mental disorder 3 and even more experience subclinical mental health symptomology.4–8 As such, it is common to encounter mental health issues in others and ourselves. When a person experiences a health symptom (e.g., feeling tired), her or his perception of what the symptom represents (B12 deficiency or anxiety) guides the treatment she or he may try (vitamins v. destressing exercise), and eventually may dictate her or his choice of health professional to visit (physician v. counselor). As this example illustrates, laypeople make many treatment decisions based on their perceptions of experienced symptoms before ever seeking a health care professional’s guidance, emphasizing the importance of understanding lay perceptions of mental health. Understanding mental health symptoms is challenging for laypeople because a single disorder can present diverse symptoms (e.g., physiological, cognitive, and affective symptoms), and a single symptom is rarely diagnostic of only one disorder (e.g., concentration problems at work could indicate depression, an attention disorder, or plain disinterest 9 ). Even recognizing a symptom as generated by a mental health issue can be difficult (e.g., 25% of emergency room patients seen for chest pain were experiencing panic attacks, not cardiac issues 10 ), with many mental health symptoms misinterpreted as manifestations of physical disorder, and vice versa.11,12
Complexities surrounding mental health issues extend to selecting treatments. Patients can choose between conventional treatment options like psychotherapy and psychopharmacological medications, as well as alternative medicine options. These broad treatment classes can be used alone13–16 and in conjunction.17–21 Each treatment type involves very different approaches to how symptom reduction is believed to occur and are often administered by very different health professionals, highlighting the complexity laypeople face in navigating mental health treatment options.
Research has begun to explore laypeople’s decisions about mental health treatment by investigating how people’s beliefs about the cause of a disorder influence decisions.22–26 Much of this work presented participants with either the label of a mental disorder24,27 or a description of a patient that provides all the symptoms needed to provide a mental disorder diagnosis.22,28 In such cases, mental disorders believed to be caused by biological factors (e.g., genetics) were rated as effectively treated by medication, whereas disorders believed to be caused by psychological factors (e.g., stress) were rated as effectively treated by psychotherapy.27–30 These preferences have been characterized as a form of mind-brain dualism in thinking about mental health treatment: disorders of the mind are best treated through therapy and disorders of the brain through medication.27,31
A limit of these previous findings is that they presuppose a clear diagnostic picture when making treatment decisions. However, in encountering the first symptoms of a mental health issue, a disorder label is not yet known and a person may not know what exactly she or he is experiencing. It is unclear how people start thinking about treatment options when symptom information is too sparse to provide a clear diagnosis.
We propose that previous findings of dualistic treatment preferences highlight a more fundamental way of thinking that suggests how people think about disease when it first presents. People have been shown outside the health domain to be inherent dualists, endorsing a separation between physically and mentally based phenomena.32,33 Applied to health, a single symptom can be judged as to whether it reflects a problem originating from a person’s body (e.g., medical problem) or from a person’s mind (e.g., mental problem). Such medical-mental attributions will not necessarily be accurate10–12 but will nevertheless be influential. We propose that in limited environments as long as the given symptoms are perceived as representing either a medical or mental issue, people will form strong preferences of the appropriate treatment to use.
In the following four experiments we tested our proposal. We measured people’s judgments of the helpfulness of psychotherapy, medication, and alternative medicine for a limited set of mental health symptoms that did not suggest a single diagnosis. Our experimental paradigm differs from previous research in that we present participants with information that does not clearly portray one disorder. We predict that even with sparse information people will form strong treatment preferences based on the type of symptoms presented. Specifically, people will endorse symptoms seen as reflecting mental problems as helped by psychotherapy and symptoms thought to reflect physical problems as helped by medication. We expand this investigation by also exploring reactions to alternative medicine, a treatment designed to target the mind and body in unison. We explored how alternative medicine’s emphasis meshes with dualistic thinking about treatment. We tested preferences for conventional and alternative treatments (Experiment 1), and how preferences change with symptom severity (Experiment 2), symptom duration (Experiment 3), and when alternative medicine is used in conjunction with other treatments (Experiment 4).
Experimental Overview
Across experiments, we used the same basic materials and design. No funding source had any role in the experiments.
Materials
We created descriptions of hypothetical people experiencing three mental health symptoms that did not suggest a single diagnosis. Each symptom was selected from a different Diagnostic and Statistical Manual of Mental Disorders (DSM) 9 disorder. We pretested the symptom sets on a group of participants (N = 113), who each rated a subset of the materials. Participants rated how likely symptom sets were to represent a mental or a medical disorder on a scale of 100 (completely a mental disorder) to −100 (completely a medical disorder), with the zero midpoint being equally likely to represent either. We conducted one-sample t tests comparing the pretest ratings for each set to zero, the midpoint of the rating scale. We categorized symptom sets as mental if their mean ratings were significantly above zero, medical if significantly below zero, and ambiguous if ratings were not different from zero (see Figure 1 for examples). Participants also rated the severity of the symptom sets on a 0 (not at all severe) to 100 (very severe) scale, and the plausibility that the three symptoms would be present at once on a scale of 0 (not at all plausible) to 100 (extremely plausible). In the main experiments, we included symptom sets receiving a mean plausibility rating of 60 or higher. We conducted one-sample t tests comparing the mean pretest severity ratings to the rating scale’s midpoint of 50, which should represent moderate severity. Symptom sets rated as significantly below 50 we categorized as low severity, significantly above 50 as high severity, and not different from 50 as moderate severity.

Example materials for Experiment 1.
In the main experiment, participants read a patient description and then made treatment judgments by answering, “For the person you just read about, how helpful do you believe ____ would be in treating this individual?” on a scale of 0 (not helpful at all) to 100 (completely helpful), with the blank replaced with each of the following treatment types: pharmaceutical medicine, mental health counseling, and evidence-based alternative treatments.* We used generic labels instead of specific instantiations of each treatment type (e.g., sertraline) to avoid participants being unfamiliar with or having strong bias concerning the specific instantiation we picked.
Basic Procedure
The experiments were administered online through the Qualtrics Survey Software. Participants first completed informed consent by reading the consent document and typing their initials into the online form. Participants then began reading patient descriptions and providing ratings. Participants read one patient description for each within-subjects condition of an experiment, with the description order randomized for each participant. The specific description shown for each condition was randomly selected for each participant from a larger set of possible descriptions shown across participants. After reading a description, participants completed the treatment judgments presented individually on the screen in a random order.
After completing the treatment judgments, participants completed a series of posttest judgments. The descriptions were re-presented and participants rated how severe, treatable, and curable the descriptions were on a scale of 0 (not at all) to 100 (extremely), as well as the medical-mental judgment from the pretest. Mean ratings for the posttest judgments can be found in Online Appendix B. Participants provided their age, gender, ethnicity/race (defined by the federal data classification on race and ethnicity), and reported their experiences with alternative medicine. Inspection of the means for the severity and medical-to-mental posttest ratings indicated that the participants perceived the descriptions as designed across experiments. The other measures were included for use in other studies and are not discussed further. Once participants moved on from an experimental screen, they were not able to revisit that screen to reread materials or change responses. Participants completed experiments at their own pace and were free to not respond to any question.
We recruited participants through the online crowdsourcing marketplace run by Amazon, the Mechanical Turk (MTurk) service. MTurk workers found the study on a list of available tasks hosted by MTurk and participated for monetary compensation on their own computer. Additional participants were assigned to the study through an undergraduate introductory psychology course at Lehigh University and participated in exchange for course credit on a computer in the first author’s laboratory. See Table 1 for participant demographics. All experiments were carried out in accordance with and approved by Lehigh University’s Institutional Review Board and Office of Research and Sponsored Programs.
Participant Demographics Across Experiments

Note: Numbers for gender, ethnicity, and race indicate percentage of total respondents selecting that category. No participants chose the additional option of “Prefer not to respond” for Gender. Participants additionally had as an option the category American Indian for race; no participants selected that identifier alone.
Data Analysis Plan
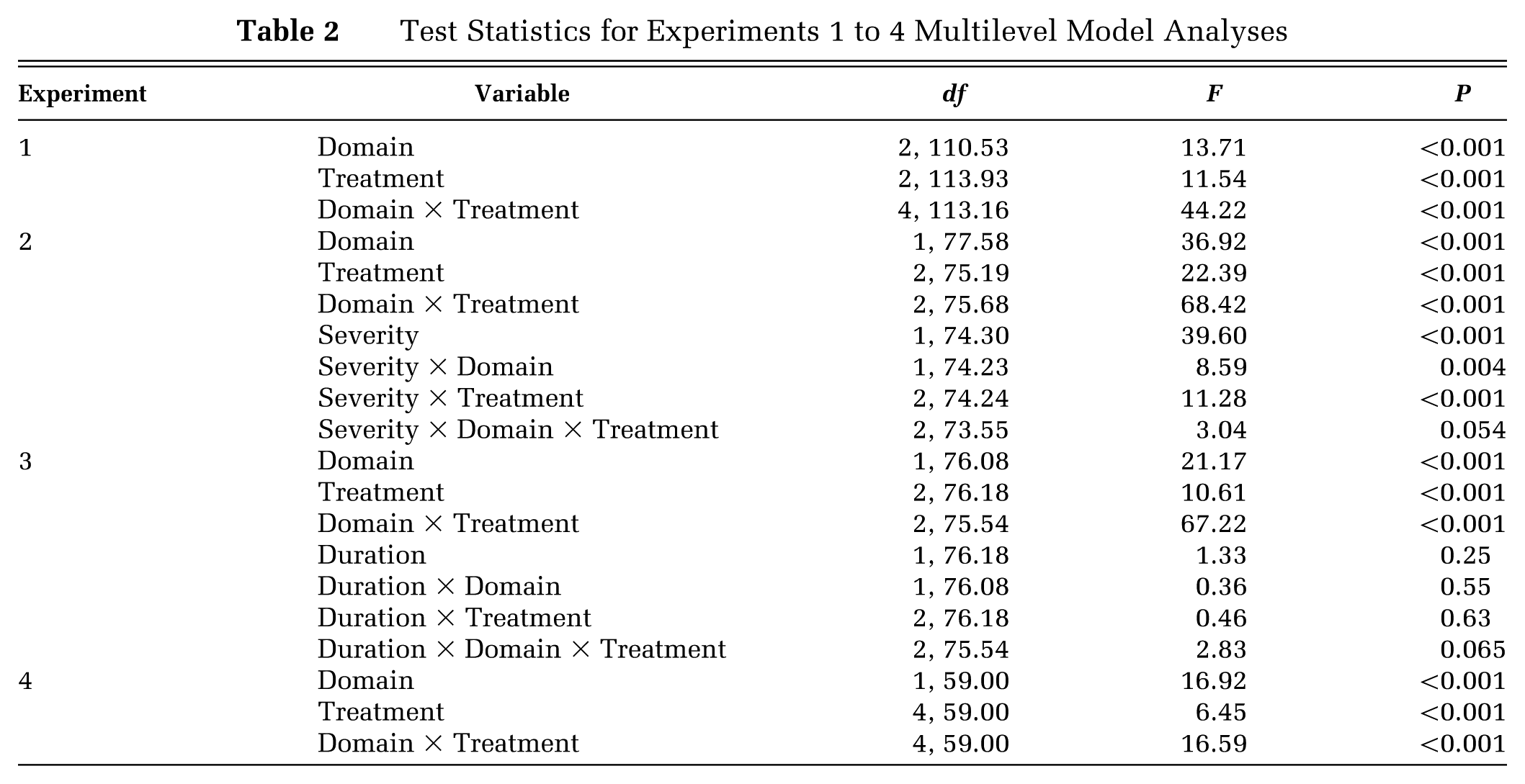
Our experiments use repeated-measures or mixed ANOVA designs. Because we did not force participants to provide responses for all questions, there were a small but notable number of missing responses.* Repeated-measures ANOVA is not an ideal statistical technique to use when data are missing. 34 To account for this, data were analyzed in each experiment using a multilevel model (MLM). Compared to the repeated-measures ANOVA approach, an advantage of MLMs is the use of maximum likelihood estimation and therefore no requirement for complete data.34,35 We entered our factors as fixed effects into the MLM models, allowing us to test the significance of the main effect of each factor and its interactions through F-tests. We present the ANOVA-style output of the MLM analyses to match the ANOVA-style design questions we are asking. Analyzing our data with traditional ANOVAs provides the same patterns of results across experiments.
Data were analyzed in the SPSS program using the repeated statement in the MIXED procedure. For each model, an unstructured covariance matrix was specified. Significant interactions were explored with simple effect analyses and, when significant, follow-up Sidak-corrected t tests conducted through the multilevel modeling procedure are presented.
Experiment 1
In Experiment 1, we explored people’s treatment judgments when limited mental health symptoms are presented that are associated with mental or medical conditions, or are not easily classified in either category.
Methods
One-hundred and fifteen people participated, 60 MTurk workers and 55 undergraduate students. We presented moderate severity patient descriptions, classified through the pretest as representing the mental domain (mean [M] = 81.9; 95% confidence interval [CI; 75.2, 88.5]), medical domain (M = −57.9; 95% CI [−42.3, −73.5]), or as ambiguously associated (M = 3.75; 95% CI [−17.9, 25.4]). Participants rated one randomly chosen case from each of the three domains.
Results
Table 2 summarizes the main effects and interaction results of our 3 (Domain: medical, mental, ambiguous; within) × 3 (Treatment type: pharmaceutical, counseling, alternative; within) multilevel model.* We found a significant interaction, which we explored within each domain (Figure 2). For medical symptoms, pharmaceuticals were rated as the most helpful, more helpful than counseling or alternative medicine, Ps < 0.001. Counseling was seen as less helpful than alternative medicine, P = 0.006. For mental symptoms, counseling was more helpful than both pharmaceutical and alternative options, Ps < 0.001. Alternative and pharmaceutical options were rated as equally helpful, P = 0.31. Finally, for ambiguous symptoms pharmaceuticals were rated as marginally more helpful than counseling (P = 0.083) and significantly better than alternative medicine (P < 0.001), with alternative and counseling ratings not differing, P = 0.21.
Test Statistics for Experiments 1 to 4 Multilevel Model Analyses
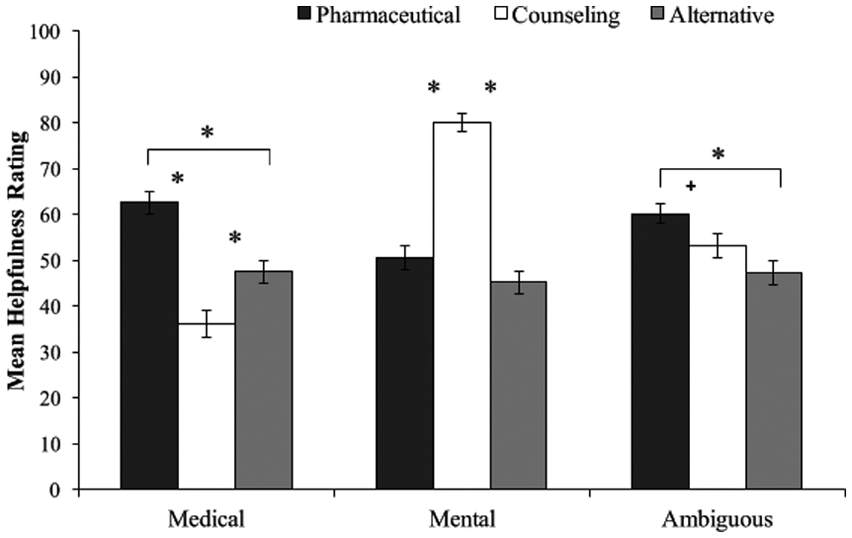
Experiment 1 mean helpfulness judgments. Error bars represent standard error. *P < 0.05. †0.05 < P < 0.1.
Discussion
Even when limited mental health symptom information is provided, people show strong treatment preferences; that is, people embrace a form of treatment dualism where counseling treats symptoms perceived as related to mental processes and symptoms that seem medical in nature are helped by medication. In the following set of three experiments we test the boundaries of these preferences.
Experiment 2
Symptom severity could change treatment preferences. If symptoms are severe enough, people may believe nothing can actually treat them. This cynical view may result in universally low helpfulness ratings, erasing any dominance of one treatment. Similarly, if people take an optimistic view, they may rate everything as helpful for severe symptoms, resulting in no differences between treatments. We examined these possibilities.
Methods
Seventy-eight people participated, including 30 MTurk workers and 48 undergraduate students. In our pretest ratings, perceived severity varied by domain: mental descriptions ranged from low to high; medical descriptions from moderate to high; and ambiguous descriptions were all rated moderately severe. We presented participants with descriptions matching the six identified domain and severity combinations. Our main comparison is between mental and medical descriptions judged as moderate (M = 52.3; 95% CI [46.5, 58.2]) and high (M = 82.6; 95% CI [77.5, 87.7]) in severity. Because the low severity mental materials cannot be compared across domains and the moderate ambiguous materials cannot be compared to other severity levels within domain, we do not discuss ratings for these materials further.
The basic procedure was modified as follows. Participants read a description and then answered the new question “Do you think that this person needs to seek treatment?” on a binary yes-no scale. We added the need-for-treatment question to check that our descriptions were seen as actually requiring treatment.* Next, participants made helpfulness ratings for that description. After rating all descriptions, participants completed the post-test questions.
Results and Discussion
Need for Treatment
Moderate (mental: 72.4%; medical: 84.6%) and highly severe (mental: 97.4%; medical: 100%) descriptions were seen as needing treatment. Exact McNemar’s tests found higher endorsement at high severity in both domains, Ps < 0.001. Endorsement did not differ between the medical and mental domains within each severity level, Ps > 0.12.
Treatment Helpfulness
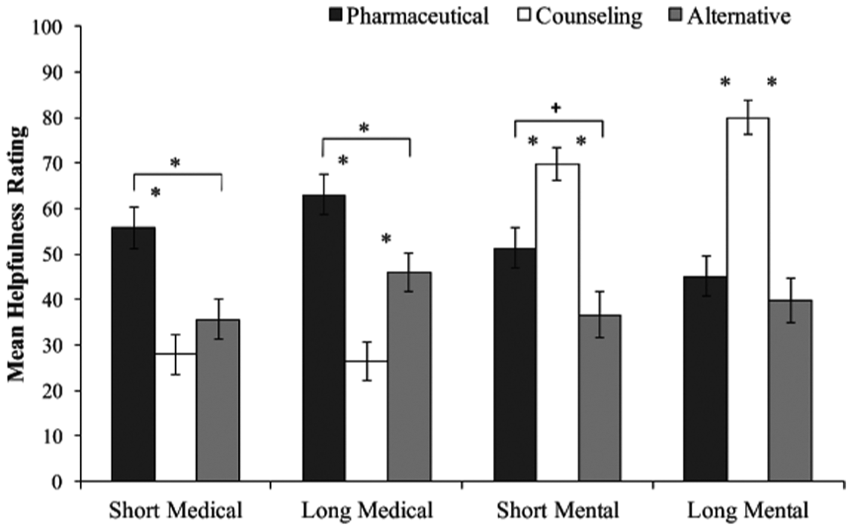
Our analysis follows a 2 (Domain: medical versus mental; within) × 3 (Treatment: pharmaceutical, counseling, alternative; within) × 2 (Severity: moderate versus high; within) design (Table 2). Overall, we found the dualistic treatment preferences of Experiment 1 across severity (Figure 3). For moderate- and high-medical symptoms, pharmaceuticals were rated the most helpful (Ps < 0.001). Alternative treatment was rated more helpful than counseling for moderate-medical symptoms, P < 0.001, and equal to counseling for high-medical symptoms, P = 0.11. For moderate- and high-mental symptoms, counseling was rated as more helpful than pharmaceuticals and alternative medicine (Ps < 0.02). Pharmaceuticals were rated equal to alternative medicine for moderate-mental symptoms, P = 0.93, but more helpful than alternative medicine for high-mental symptoms, P < 0.001.

Experiment 2 mean helpfulness judgments. Error bars represent standard error. *P < 0.05. †0.05 < P < 0.1.
A main effect of severity reflected that treatments were rated more helpful at high than moderate severity. We tested whether this pattern held within each treatment type. Pharmaceuticals (medical: P = 0.004; mental: P < 0.001) and counseling (medical: P = 0.039; mental: P < 0.001) were more helpful for high than moderate severity symptoms in both domains. Alternative medicine was rated as equally helpful at moderate and high severity for both domains, Ps > 0.6.
Experiment 3
We next tested whether symptom duration influenced treatment preferences. A symptom present for a long period of time may be seen as chronic and unlikely to respond to any treatment. Such a belief could result in rating all treatments as not helpful. Conversely, recently onset symptoms may be rated as helped by all treatments because the symptoms could be perceived as more treatable overall. However, if dualistic treatment judgments are as robust as Experiments 1 and 2 suggest, then helpfulness judgments may show the same patterns seen before regardless of symptom duration.
Methods
Seventy-eight MTurk workers made ratings for one moderate severity medical and one moderate severity mental description. We manipulated duration between subjects by adding a sentence to the end of each description that stated how long the person had been experiencing the symptoms: 2 weeks in the short duration manipulation (n = 38) and 6 months in the long duration manipulation (n = 40). All other procedures were identical to Experiment 2.
Results and Discussion
Need for Treatment
Participants endorsed treatment being needed for both medical (short: 91.9%; long: 92.5%) and mental (short: 78.9%; long: 87.5%) symptoms. Mann-Whitney U tests found these percentages did not differ by duration for medical, P = 0.92, or mental, P = 0.31, symptoms, and exact McNemar’s tests did not find differences by domain for short, P = 0.18, or long, P = 0.73, duration.
Treatment Helpfulness
Our analysis follows a 2 (Domain: medical v. mental; within) × 3 (Treatment: pharmaceutical, counseling, alternative; within) × 2 (Duration: short v. long; between) design (Table 2). Duration did not influence the treatment rated as most helpful for each domain (Figure 4). Pharmaceuticals were rated as the most helpful option for short (Ps < 0.002) and long (Ps < 0.006) duration medical symptoms. Likewise, counseling was rated the most helpful for short (Ps < 0.003) and long (Ps < 0.001) duration mental symptoms. Duration did influence differences between the less helpful options. For medical symptoms, alternative medicine was rated as more helpful than counseling for long, P < 0.001, but not short duration symptoms, P = 0.34. For mental symptoms, alternative medicine and pharmaceuticals did not differ for long duration, P = 0.77, but pharmaceuticals were marginally more helpful than alternative medicine at short duration, P = 0.080.
Experiment 3 mean helpfulness judgments. Error bars represent standard error. *P < 0.05. †0.05 < P < 0.1.
Experiment 4
In no experiment to this point was alternative medicine judged a dominant treatment option. In fact, inspecting Figures 2 to 4 highlights that alternative medicine ratings rarely differ across our manipulations. Alternative medicine’s helpfulness may be attenuated because people may not see it as standalone treatment, given that users often begin alternative treatment after initiating a conventional treatment.20,21 In Experiment 4, we tested whether alternative treatment is rated as more helpful when used as an adjunct to conventional treatments.
If people see alternative medicine as effective when it is used with conventional treatments, we should see alternative plus a conventional treatment (alternative+) options receiving higher helpfulness ratings than either individual treatment alone. Alternatively, we predict that alternative medicine’s holistic focus on mind and body may not fit with people’s dualistic beliefs that treatments target one or the other, resulting in helpfulness ratings for these combination therapies being equal to what conventional treatments can do alone.
Methods
Sixty MTurk workers read one medical and one mental moderate severity description. Participants made the same judgments as in Experiment 2, along with two additional helpfulness judgments for alternative+ options. Participants answered “how helpful do you believe some combination of Evidence-Based Alternative Treatment and a traditional ____ treatment would be in treating this individual?” with the blank replaced in one question by the pharmaceutical wording and by the counseling wording in a second question. All other procedures were as in previous experiments.
Results and Discussion
Most participants believed treatment was needed for the descriptions (medical: 80.0%; mental: 71.7%), with exact McNemar’s tests not finding a difference across domains, P = 0.36.
Our helpfulness ratings analysis follows a 2 (Domain: medical versus mental; within) × 5 (Treatment; pharmaceutical, counseling, alternative; alternative + pharmaceutical; alternative + counseling; within) design (Table 2). Pharmaceuticals were rated more helpful than counseling, P < 0.001, and alternative medicine, P = 0.089, for medical symptoms (Figure 5). Counseling was rated more helpful than pharmaceuticals or alternative medicine for mental symptoms, Ps < 0.001. Alternative + pharmaceutical ratings for medical symptoms were significantly higher than alternative alone, P = 0.002, but not higher than pharmaceuticals, P = 0.99. Likewise, alternative + counseling was rated more helpful than alternative alone for mental symptoms (P < 0.001), but not more helpful than counseling, P = 0.86. Ratings for alternative + counseling for medical symptoms and alternative + pharmaceutical for mental symptoms did not significantly different from alternative medicine alone in each domain, Ps > 0.7. Overall, alternative medicine does not boost helpfulness ratings over what a conventional treatment would receive on its own.

Experiment 4 mean helpfulness judgments. Error bars represent standard error. *P < 0.05. †0.05 < P < 0.1.
General Discussion
Across four experiments we showed that even when limited amounts of information are provided people make predictable, dualistic treatment judgments. Mental health symptoms perceived as linked to medical disorders were rated as helped by medication, whereas symptoms linked to mental disorders were rated as helped by counseling. Treatment preferences maintained regardless of symptom severity and duration. Alternative medicine was never a dominant preference, even when combined with a traditional treatment. Our findings expand previous work on treatment judgments by showing dualistic preferences when no clear diagnosis is present by just manipulating the perceived medical or mental nature of symptoms. In short, attributing a symptom to one side of this medical-mental divide elicits a dualistic treatment preference pattern.
We propose our findings can be explained by people having a fundamentally dualistic way of thinking about mental life. Dualism has been suggested as an natural bias in how we think about the world, 32 with young children36,37 and adults33,38 endorsing a differentiation between the physical body and the mind. Our findings illuminate how dualism influences health beliefs 39 by showing that our dualistic perceptions of disordered mental activity dictate the treatments we think are most useful.
Our results may illuminate one strategy for choosing between the vast numbers of treatment options modern medicine provides. Large choice sets produce more decision-making difficulty and lower ultimate choice satisfaction. 40 People may benefit by reducing the number of choices in consideration as quickly as they can. Zeroing in on only one helpful type of treatment depending on the presented symptoms may serve as an effective choice set limiter.
The limitations of our experiments suggest future research. Our participants represented a general public sample, as opposed to a sample of patients in treatment. We were interested in how people think about treatment before they enter the health care system for such treatment, and using a general public sample allows us to better assess this. Future research could measure patients, especially ones receiving care for chronic issues, to see if these dualistic treatment preferences maintain over time.
Our participants were overwhelmingly Caucasian and non-Hispanic, limiting our ability to generalize our findings across cultural groups. The perceived appropriateness of treatment and the preferred types of treatment can vary by country of origin.41,42 Within US samples, minority participants were more likely than Caucasians to believe therapy was effective and mental illness improves on its own 43 and less likely to endorse medication as useful. 44 Similarly, biological causes of mental disorders are endorsed to different extents across cultural and ethnic lines.42,45 Overall, future research should explore how differences in people’s cultural background moderates our pattern of dualistic treatment preferences.
Because our passages described hypothetical others, our findings do not directly speak to how people make judgments about their own treatment. Our research does directly address the large number of health care decisions laypeople make for others. Parents, significant others, and children of elderly parents often make treatment decisions for loved ones showing symptoms of illness. Our results suggest that how others interpret those presenting symptoms will guide which treatment they seek for their loved ones. People make different health decisions for others versus themselves, 46 suggesting future research should explore if treatment preferences differ when participants were thinking about themselves.
How do helpfulness ratings translate into selecting an actual treatment across judgment environments? People’s general preferences are not static,47,48 and being asked to think deeply about treatments 49 or defend one treatment over another before making a decision 50 could result in different judgments. More generally, future research should explore how preferences relate to actually selecting treatments in the clinical setting.
Our findings suggest several possible clinical implications. People report preferring psychotherapy over medication when asked about treating mental disorders as a general class of disorders.42,51,52 Extrapolating from our results, a preference for psychotherapy may stem from people thinking of only mentally based symptoms and, therefore, just reflect laypeople’s concepts of prototypical mental disorder symptoms. If a clinician wanted to encourage a patient to try medication for a mental health issue, highlighting physical disorder symptoms may increase the patient’s willingness. More generally, how clinicians present the different symptoms of mental health conditions should influence the treatments a patient sees as useful.
Understanding how people think about the comparative helpfulness of treatments may provide insight into adherence and the willingness to try new treatments. If one treatment is seen as dominantly helpful, a patient might continue that treatment even if the treatment was not working. In this way, a sunk cost effect53,54 or status quo bias 55 may be perpetuated because patients are unwilling to change from the perceived dominant option. However, if options were similar in perceived helpfulness, then a patient might be more likely to switch treatments. 56 Given that people will elect to defer making a choice if there is no clear best option,57–59 future research should investigate how much more helpful a treatment needs to be to be seen as a dominant choice.
Finally, our results suggest implications for how patients may think about the severity of a diagnosis. As noted in Experiment 2, we could not create plausible symptom sets that described low severity, medically associated symptoms. Overall, DSM symptoms thought to come from a medical condition were rated more severe than symptoms recognized as coming from a mental condition. This bias may influence how people experiencing different symptom presentations of the same disorder are seen. For example, a person experiencing three physical depression symptoms could be seen as having more severe depression than someone experiencing three affective depression symptoms. Providers need to recognize how people construe mental health symptoms and what that might suggest to people about the severity of their own and their loved ones’ mental health issues.
Conclusions
We demonstrated that from limited amounts of information about mental health conditions people express preferences that suggest a dualistic bias in thinking about treatment. Dualistic treatment preferences held regardless of the severity or duration of symptoms. Further research expanding our findings will help better understand the decisions people make about treatment that may greatly influence a disease’s future course.
Footnotes
Acknowledgements
We thank Lucy Napper for helpful comments on a version of this article.
All research was conducted at Lehigh University’s Department of Psychology. Financial support for this study was provided in part by a grant from Lehigh University’s Dale S. Strohl Undergraduate Summer Research Grant funds and Lehigh University’s new faculty start-up funding. The funding agreement ensured the authors’ independence in designing the study, interpreting the data, writing, and publishing the report. The following author is employed by the sponsor: Jessecae K. Marsh.
*
Half of the participants received these labels and half received descriptive versions of these options (e.g., “speaking to a mental health clinician about these issues” for the counseling option). This format manipulation did not produce meaningful changes to the patterns of results in any experiments. We collapsed across the format manipulation for our main statistical analyses. See Online Appendix A for analyses exploring the format manipulation.
*
Additionally, we screened our data to remove participants who did not respond to one third or more of an experiment’s dependent measures, removing eight participants across the four experiments. Reported participant numbers are final numbers without these participants.
*
We used the domain classifications provided by the pretest data. Using the participant provided medical-to-mental ratings to classify the stimuli for each participant into the three domains results in the same pattern of results as using our pretested classifications.
*
Believing a treatment is helpful does not necessitate believing it should be administered. For example, someone who believes counseling could help reduce stress related to a work deadline may nevertheless believe that therapy is not actually warranted.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.