
Abstract
Background:
Cardiovascular disease (CVD) is highly prevalent, affecting 1 in 6 Australians. Tooth loss has consistently been associated with an increased risk of CVD, influenced by social determinants of health as well as effects on chewing function and diet. However, there is little evidence regarding the role of diet in the relationship between tooth loss and CVD. This study aimed to determine the impact of retaining a functional dentition (minimum of 20 teeth) on the risk of incident CVD and the role of diet in this relationship.
Methods:
This prospective cohort study recruited Australian women from the 1946 to 1951 cohort of the Australian Longitudinal Study on Women’s Health. Tooth loss and diet quality were assessed from survey 5 (2007) and incident CVD from linked data over a 17-y follow-up period (2024). Cox proportional hazards models were used to estimate hazard ratios (HRs) and 95% confidence intervals (CIs) adjusted for known risk factors (age, sociodemographic, lifestyle, and medical history factors).
Results:
A total of 8,306 women, average age 58.5 ± 1.5 y, 69.2% with a functional dentition, were included. Over the 17-y follow-up period, 1,432 (17.2%) women developed incident CVD. The presence of a functional dentition was associated with a lower risk of incident CVD compared to women with a nonfunctional dentition, 15.5% versus 21.1%, respectively (HR = 0.83; 95% CI, 0.74–0.93). A greater proportion of women with a functional dentition had a high-quality diet score compared to those with a nonfunctional dentition (42% vs. 36%,
Conclusion:
Although tooth loss negatively impacts diet quality, dietary changes alone do not explain why tooth loss is a marker of incident CVD, and loss of a functional dentition should prompt cardiovascular prevention action.
Knowledge transfer statement:
This study demonstrates that loss of a functional dentition in women increases the risk of developing cardiovascular disease, independent of changes in diet quality. Policymakers and clinicians should promote cardiovascular preventive action for women with significant tooth loss.
Introduction
Cardiovascular disease (CVD) is a prevalent health condition, representing 32% of all deaths globally (World Health Organization 2025b). In Australia, 1 in 6 people self-report that they live with CVD, representing almost 18% of the total Australian population (Heart Foundation 2025).
Oral diseases are also highly prevalent, affecting nearly 3.7 billion people globally (World Health Organization 2025a). Untreated, oral diseases such as tooth decay and periodontitis can lead to the loss of teeth. In Australia, the proportion of adults with significant tooth loss increases with age from 0.7% in 15- to 34-y-olds to 46% in those aged 75 y or over (Do and Luizzi 2019). Longitudinal studies conducted globally have demonstrated a consistent association between tooth loss and CVD even after adjusting for sociodemographic factors and chronic conditions such as diabetes and hypertension. These studies have shown that tooth loss is associated with an increased risk of CVD, including CVD disease-related mortality (Liljestrand et al 2015; Joshy et al 2016; Lee et al 2019; Shen et al 2024), with a dose-dependent relationship between tooth loss and CVD (Joshipura et al 1996; Lee et al 2019). Importantly, evidence indicates a bidirectional relationship between tooth loss and hypertension, which is a key risk factor for CVD (Xu et al 2022). While diet quality, specifically fruit and vegetable intake, has been shown to mediate the association between tooth loss and accelerated aging (Xu et al 2023), very few studies have considered the role of diet in the association between tooth loss and CVD.
The mechanisms by which tooth loss affects the risk of CVD relate to inflammation (Aoyama et al 2018) and compromised chewing function (Moynihan 2007). Periodontitis, a chronic inflammatory condition of the supporting tissues of the teeth, is triggered by oral bacteria (Meyle and Chapple 2015). In addition to localized oral inflammation, periodontitis results in systemic inflammation and is associated with elevated levels of circulating inflammatory cytokines such as C-reactive protein (Aoyama et al 2018), thereby increasing the cardiovascular risk profile (Yusuf et al 2020). In terms of chewing function, as teeth are lost and the dentition becomes nonfunctional, individuals alter their food choices, selecting softer foods that are often low in protein and fiber (Kossioni 2018). A functional dentition required to maintain satisfactory chewing performance is defined as the presence of a minimum of 20 natural teeth (Do and Luizzi 2019) (a complete dentition consists of 28–32 teeth).
Poor diet quality contributes to an increased risk of CVD-related mortality (Dong et al 2022), while an increased intake of both protein and fiber has been reported to reduce the risk of CVD (Qi and Shen 2020; Reynolds et al 2022). As such, the loss of a functional dentition may compromise diet quality and thereby increase the risk of CVD. Therefore, an important question is whether the association between tooth loss and CVD is impacted by diet quality.
The primary aim of this study was to determine the association between retaining a functional dentition and the risk of incident CVD in a prospective cohort study of Australian women and to investigate the role of diet in this relationship. Secondary aims were to investigate the impact of dentition status on diet quality and the association between diet quality and incident CVD.
Methods
Study Population
This prospective cohort study used data from the Australian Longitudinal Study on Women’s Health (ALSWH), collected from over 40,000 women in 3 age groups randomly selected in 1996 from the Medicare database (Dobson et al 2015). All Australian residents have universal access to Medicare. For this study, data from the 1946 to 1951 cohort of women who answered survey 5 in 2007 when they were aged 56 to 61 y (n = 10,638) were used as our initial sample as it was the first time a question on tooth loss was included in the surveys. Demographic data not available in survey 5 (2007), including income and education level, were obtained from surveys 3 and 1, respectively. The ALSWH survey program has ongoing ethical approval from the Human Research Ethics Committees (HRECs) of the Universities of Newcastle and Queensland (approval numbers H076-0795, 2004/HE000224, respectively) for the 1946 to 1951 cohort. The ALSWH also maintains institutional HREC approvals for external record linkage. The study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology guidelines.
Primary Endpoint
The primary endpoint was incident CVD assessed using data obtained from the Common Conditions from Multiple Sources (CCMS) dataset, which is derived from surveys and linked with external health record collections, including the National Death Index, Medicare Benefits Schedule, Pharmaceutical Benefits Scheme, hospital admissions, and National Aged Care data (Dobson et al 2015). CVD included ischemic heart disease (IHD) and stroke as defined by the 10th revision of the International Statistical Classification of Diseases and Related Health Problems (ICD-10). The codes, which are also used for national reporting of IHD, included ICD codes 120–125 and 410–414, as well as ICD codes 430–438 and 160–169 for stroke. Fatal CVD was defined as a death caused by IHD or stroke. Incident CVD was defined as the first occurrence of either a diagnosis of CVD (from survey data) or a cardiovascular event (from linked data) during the 17-y follow-up period. This follow-up commenced from each participant’s date of submission of survey 5 and continued until April 2024. Participants were excluded from the analysis if they had preexisting CVD identified through either survey 5 or CCMS data linkage prior to that time or if they opted out of the CCMS data linkage.
Primary Independent Variable
The primary independent variable was the self-reported number of teeth, assessed using data from survey 5. Dentition status was categorized as functional (≥20 teeth and at least 10 teeth in each arch) and nonfunctional (<20 teeth or ≥20 teeth with <10 teeth in 1 arch). The remaining dentition was further segmented as “≥20,” “10–19,” “1–9,” or “no remaining teeth” to understand the dose–response relationship. Participants with missing tooth information were excluded from the analysis.
Wearing dentures, which was self-reported in survey 5, was also used as an independent variable. Denture use was categorized as functional dentition (≥20 teeth and at least 10 teeth in each arch and no dentures) or nonfunctional dentition (<20 teeth or ≥20 teeth with <10 teeth in 1 arch) with or without dentures.
Diet Quality
Dietary information was collected using a shortened version of the Dietary Questionnaire for Epidemiological Studies version 2 (DQES) (Giles and Ireland 1996), which was administered to all participants in survey 5. The original DQES v2 had a 10-point frequency scale, which participants used to report their habitual consumption of 74 foods and beverages over the previous 12-mo period. Details of the DQES have previously been presented (Giles and Ireland 1996), and the survey has been validated (Hodge et al 2000). The shortened version uses a 3-point frequency scale for most questions except for questions on dairy, meat, and fish, which use a 5-point frequency scale.
Diet quality was determined using the Australian Recommended Food score (ARFS) (Collins et al 2015), which is calculated by summing points within the subscales for a total of 74 points: vegetables (/22), fruits (/14), protein foods (/14), grains (/14), dairy products (/7), fats (/1), and alcohol (/2). Foods are given 1 point for a frequency of more than once/week. Higher values correspond to a healthier diet quality. The AFRS was categorized into quintiles based on the distribution of the scores. Quintiles 1 to 3 were categorized as “low quality” and quintiles 4 to 5 as “high quality.” Missing diet values on the survey were recoded to zero for up to 4 items. Participants with missing values for more than 4 items were considered to have incomplete data and excluded from the analysis.
Covariates
Covariates were prespecified based on established CVD risk factors and obtained from survey 5. They included age, area of residence (defined as urban cities, inner regional, outer regional, remote, very remote), socioeconomic status, and education status (defined by the Socioeconomic Indexes for Areas [SEIFA] index of socioeconomic disadvantage and the SEIFA index of education, respectively; both which were defined as either high [above the median cut point] or low [below the median cut point]). Health-related variables included body mass index (BMI; continuous variable), smoking (defined as never, ex-smoker, and current smoker), and diabetes and hypertension, both of which were categorical.
Statistical analysis
All statistical analyses were performed using R software (version 4.4.0; R Core Team 2024), and P values of less than 0.05 were considered statistically significant unless stated otherwise. Continuous variables are presented as mean ± SD and categorical variables as numbers and percentages. Data excluded and missing are described, and we compared baseline characteristics in women with and without data on teeth and/or diet information to assess the potential for selection bias.
Kaplan–Meier survival curve was constructed to examine the association between dentition status and incident CVD (with no teeth used as the reference). Time-to-event data were defined as the duration from survey 5 to the first occurrence of CVD. Hazard ratios (HRs) were calculated from Cox proportional hazards models, and data were adjusted for all prespecified covariates.
The primary analysis used Cox proportional hazards models to estimate HRs and their 95% confidence intervals (CIs). Model 1 was unadjusted, model 2 was adjusted for all prespecified covariates, and model 3 was further adjusted for diet quality.
To investigate the relationship between dentition status and diet quality and to explore the influence of denture use (based on the response to the question “Do you wear an upper/lower denture?”) on the relationship between dentition status and diet, log binomial analysis was used to calculate risk ratios (RRs) and their 95% CIs. Models were adjusted for all covariates. Further analyses examined the relationship between diet quality as a continuous variable or defined by fruit and vegetable intake only and incident CVD using proportional hazards models to calculate HRs and their 95% CIs.
Patient and Public Involvement
Patients were not involved in the research process of this study.
Results
After exclusions, the final sample included 8,306 participants (Fig. 1) with an average age of 58.5 ± 1.5 y. Women with a nonfunctional dentition had an average of 10.7 ± 7.6 teeth, while women with a functional dentition had an average of 26.8 ± 2.9 teeth. Compared to women with a functional dentition, women with a nonfunctional dentition were more likely to reside in a regional area (66.9% vs. 54.1%) and less likely to be in the top 2 quintiles for education status (37.9% vs. 57.3%) and socioeconomic disadvantage (39.6% vs. 56.3%). Health-wise, those with a nonfunctional dentition had a higher mean BMI (28.4 ± 5.9 vs. 26.7 ± 5.1) and were more likely to have diabetes and hypertension (8.1% vs. 4.2% and 30.2% vs. 24.0%, respectively). Most of those with a nonfunctional dentition had their teeth replaced with dentures (86.4%). Compared to women with a nonfunctional dentition, women with a functional dentition were more likely to have a diet score in the top 2 quintiles (42.0% vs. 35.6%), indicating a higher diet quality (Table 1 and Appendix Table 1). Missingness for all covariates was less than 2%. Diet variables were normally distributed, and data for the number of teeth were not normally distributed. The proportional hazards model assumption was visually assessed by checking for parallelism in the log-minus-log Kaplan–Meier plot for each covariate. No substantive departures were detected. The association between SEIFA disadvantage and education was not associated to a level that would induce multicollinearity (Kendall’s tau of 0.64 and variation inflation factor of 1.7).
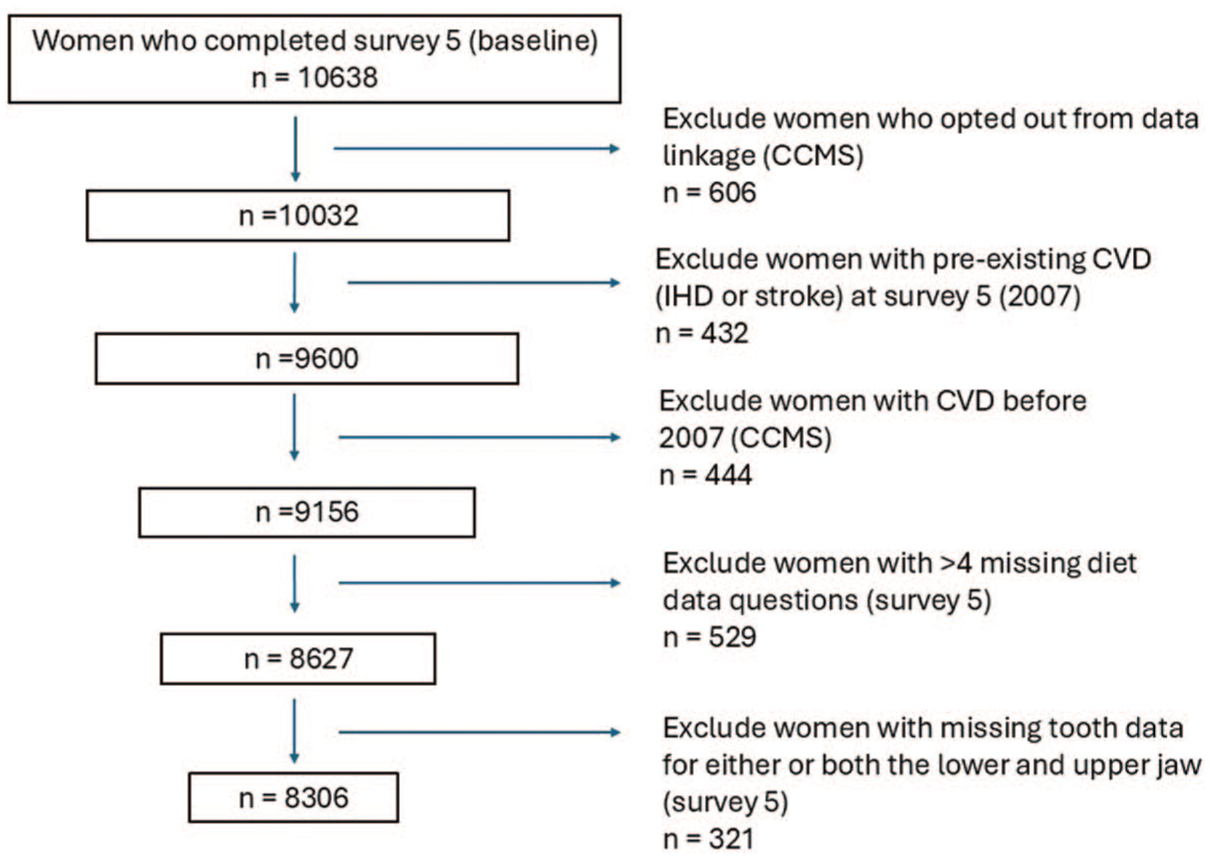
Participant selection flow diagram. Common conditions from multiple sources (CCMS), cardiovascular disease (CVD), and ischemic heart disease (IHD).
Population Characteristics.
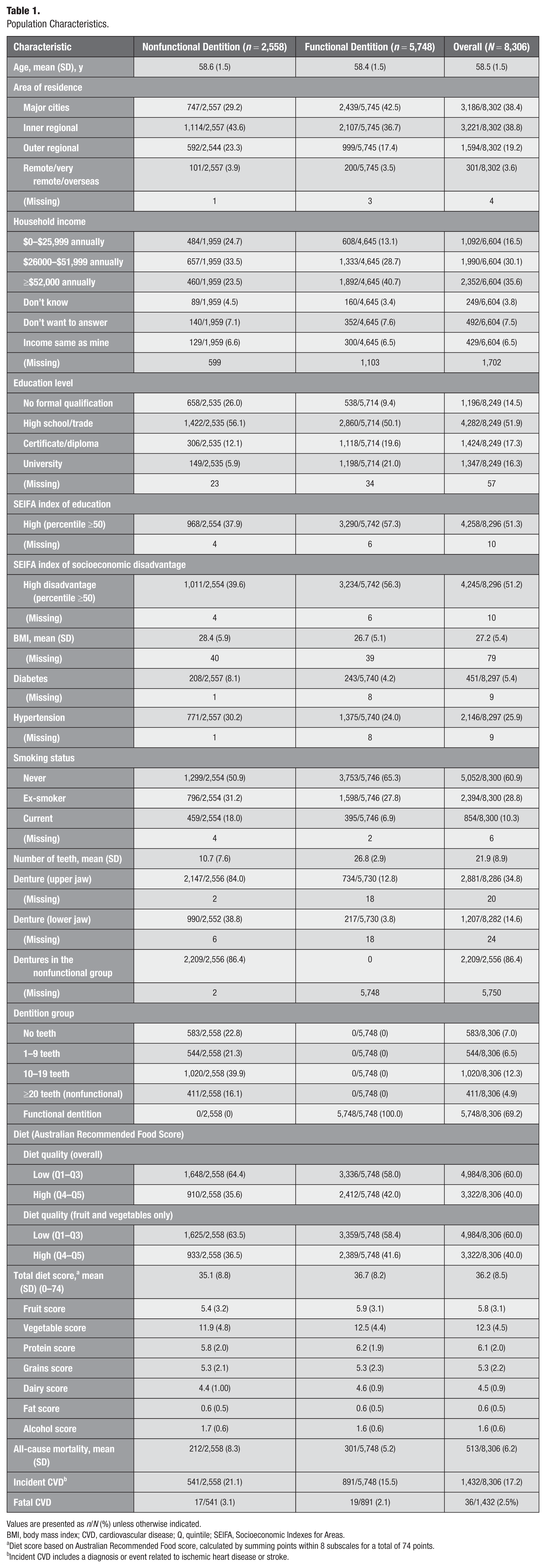
Values are presented as n/N (%) unless otherwise indicated.
BMI, body mass index; CVD, cardiovascular disease; Q, quintile; SEIFA, Socioeconomic Indexes for Areas.
Diet score based on Australian Recommended Food score, calculated by summing points within 8 subscales for a total of 74 points.
Incident CVD includes a diagnosis or event related to ischemic heart disease or stroke.
Compared to the study population analyzed, women with missing diet and tooth data were older (58.6 ± 1.5 vs. 58.5 ± 1.5, P = 0.001), more likely to live in a rural or remote location (70.3 vs. 61.6, P < 0.001), more likely to have a low income (21.2% vs. 16.5%, P < 0.001), and have no formal educational qualification (26.6% vs. 14.5%, P < 0.001). However, there were no differences in the prevalence of diabetes (P = 0.07), hypertension (P = 0.12), incident CVD or fatal CVD (P = 0.2) (Appendix Table 2).
Over the 17-y follow-up period, 513 (6.2%) women died from all causes, 36 of whom died due to fatal CVD. A total of 1,432 (17.2%) women were diagnosed with CVD (IHD or stroke) or had a cardiovascular event (including fatal CVD).
Women with a nonfunctional dentition developed CVD earlier and at the 17-y endpoint had a higher rate of incident CVD (Fig. 2). A functional dentition was associated with a lower risk of incident CVD in the adjusted model (HR = 0.83; 95% CI, 0.74–0.93; P = 0.001). Adjusting for diet quality (high or low) did not attenuate this association (HR = 0.82; 95% CI, 0.73–0.92; P < 0.001; Table 2 and Appendix Table 3). The relationship between the number of teeth and incident CVD suggested a dose–response relationship, with the HRs for incident CVD decreasing as the number of retained teeth increased (Fig. 3).
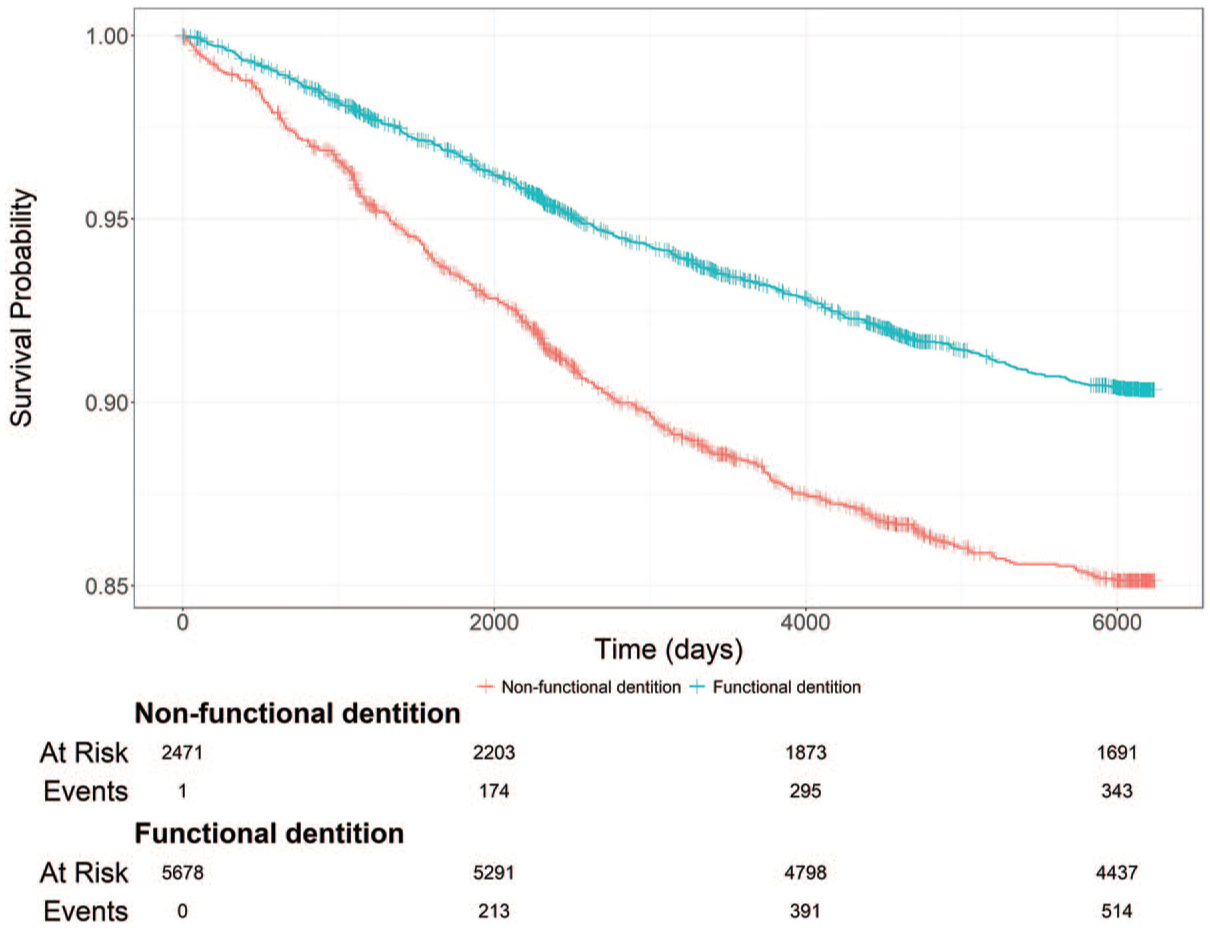
Kaplan–Meier curve of incident cardiovascular disease across time (in days). The number of participants at risk of incident cardiovascular disease over the 17-y follow-up period is shown in women with a functional dentition compared to women with a nonfunctional dentition.
Associations between Dentition Status and Incident Cardiovascular Disease among Middle-Aged Australian Women (n = 8,306).
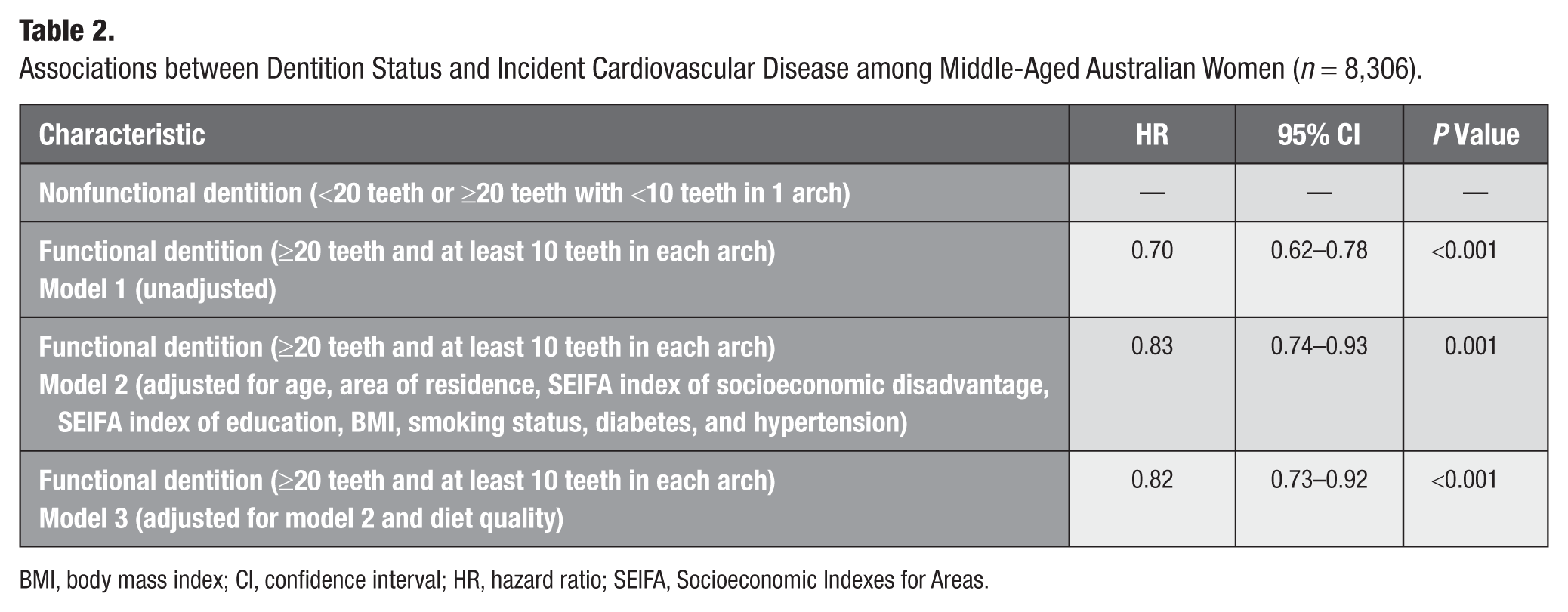
BMI, body mass index; CI, confidence interval; HR, hazard ratio; SEIFA, Socioeconomic Indexes for Areas.
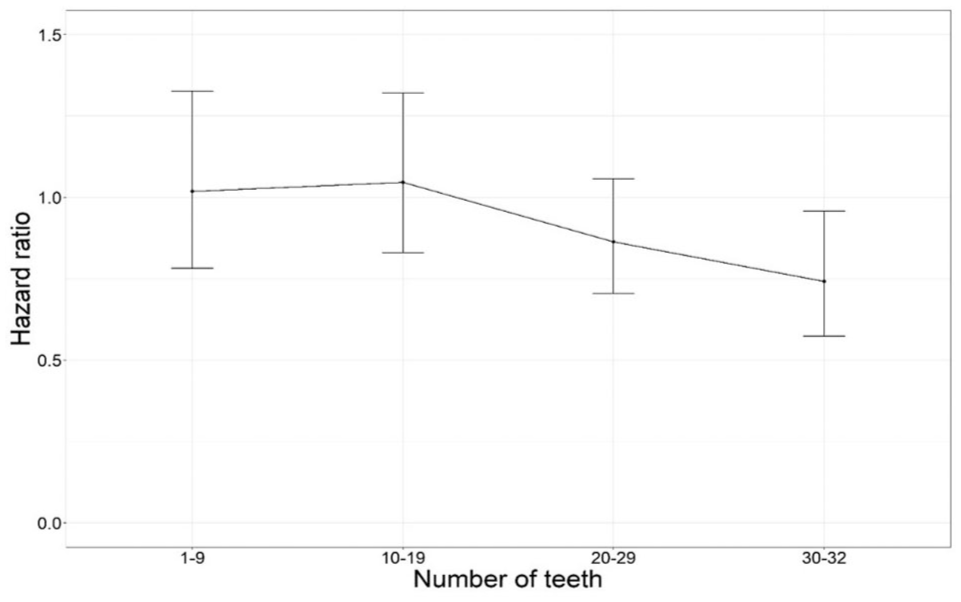
Association between the number of teeth and risk of incident cardiovascular disease. The reference group is women with no teeth. Hazard ratios are calculated from Cox proportional hazard models and data adjusted for age, area of residence, SEIFA index of socioeconomic disadvantage, SEIFA index of education, body mass index, smoking status, diabetes, and hypertension. SEIFA, Socioeconomic Indexes for Areas.
A functional dentition was associated with a higher diet quality (RR = 1.12; 95% CI, 1.06–1.20; P < 0.001). The relationship between dentition status and diet quality in those with a nonfunctional dentition was similar in women with dentures (RR = 0.89; 95% CI, 0.83–0.95; P < 0.001) and without dentures (RR = 0.91; 95% CI, 0.78–1.05; P = 0.22; Appendix Tables 4 and 5).
Although not significant, high diet quality was related to a higher risk of incident CVD (HR = 1.11; 95% CI, 1.00–1.24; P = 0.06), and while this suggests a small increase in risk, the association is marginal and likely reflects residual confounding or chance. Further context is provided in the Discussion.
There was little evidence of association between the other measures of diet (total diet score as a continuous variable or diet score restricted to fruit and vegetable intake) and incident CVD (HR = 1.00 [95% CI, 1.00–1.01], P = 0.63; HR = 1.09 [95% CI, 0.97–1.21], P = 0.14), respectively (Appendix Table 6).
Discussion
This study found that retention of teeth as part of a functional dentition was associated with a lower risk of future CVD. While retention of teeth was also associated with higher diet quality, adjusting for diet quality did not attenuate the relationship of teeth retention to future CVD. This finding was consistent when diet quality was restricted to fruit and vegetable intake. This suggests that diet quality is not the only pathway by which oral health, as measured by retention of teeth, is associated with CVD. It also specifically lends strength to the evidence that maintaining a functional dentition is an independent marker of better cardiovascular health and that poor dentition is a marker of poor cardiovascular health among women.
The findings in this study that women with a nonfunctional dentition have a higher overall incidence of CVD (21.1% vs. 15.5%) are consistent with the growing body of evidence that reports that the loss of teeth is associated with an increased risk of hypertension (a key risk factor for CVD) (Xu et al 2022), CVD (Lee et al 2019), and CVD-related mortality (Beukers et al 2021; Lee et al 2019; Shen et al 2024). Similarly, the dose–response relationship reported in this study, which showed that the risk of CVD decreased as the number of teeth increased, is also consistent with the literature (Lee et al 2019; Liljestrand et al 2015). An Australian study with a 6-y follow-up reported that tooth loss was a risk marker for incident CVD-related hospitalization (Joshy et al 2016). Very few studies, however, have analyzed the impact of diet on the association between tooth loss and CVD. A study in male health professionals investigating the association between tooth loss and coronary heart disease, adjusted for fiber and carrot intake, reported a very slight attenuation in the relationship (Joshipura et al 1996). A longitudinal study in the United States (Shen et al 2024) included diet quality, defined by the Healthy Eating Index (HEI) as a covariate, along with other established covariates, in an analysis of the association between tooth loss and cardiovascular mortality and reported lower diet scores in those with ≥10 missing teeth (Shen et al 2024). Importantly, although studies consistently report that the loss of teeth increases the risk of CVD with a dose-dependent relationship (Lee et al 2019; Shen et al 2024) and that the number of teeth retained is associated with a lower risk of CVD-related mortality (Beukers et al 2021; Shen et al 2024), they do not specifically report the association between the retention of a functional dentition (minimum of 20 teeth) on CVD risk.
In this study, women with a functional dentition were more likely to report a higher diet quality. These findings align with previous research indicating that the loss of a functional dentition impairs chewing function (Lahoud et al 2023) and that tooth loss is associated with changes in food selection (Kossioni 2018), resulting in reduced intake of dietary protein and fiber, as well as lower overall diet quality as measured by the HEI (Shen et al 2024). Interestingly, the presence of dentures did not change this relationship, indicating that dentures did not improve diet quality. This finding may relate to the absence of data on whether dentures restored the functional dentition (10 occluding pairs) or whether they were comfortable to wear, both of which directly influence masticatory function.
Diet quality has been shown to be associated with CVD (Dong et al 2022), and although not significant, this study found an 11% increase in incident CVD for those with a high-quality diet. This was unexpected. However, the difference in diet scores between the groups was very small (nonfunctional 35.1 [8.8] vs. functional 36.7 [8.2]), which suggests that both groups had very similar diets. Similarly, a previous study involving the same cohort using diet data from surveys 4 to 8 to investigate the relationship between diet quality and several noncommunicable diseases, including diabetes mellitus, coronary heart disease, hypertension, asthma, cancer, and depression, failed to find an association between diet quality and coronary heart disease (Hlaing-Hlaing et al 2021). The self-report bias of the diet survey, the use of the shortened diet survey, and the fact that we did not specifically examine whether participants had a cardiovascular healthy diet and whether their diet changed over time may explain the association between diet and CVD reported in this study. Studies that have shown associations between diet and cardiovascular health have demonstrated the relationship based on cardiovascular healthy diets such as the Mediterranean diet (Martínez-González et al 2019) and the Dietary Approaches to Stop Hypertension (DASH) diet (Appel et al 1997).
Poor diet quality has been suggested as a key mechanism by which tooth loss leads to the increased risk of CVD (Moynihan 2007). However, this study’s findings indicate that the nutritional pathway alone involving dietary changes may not explain the association between tooth loss and incident CVD. Tooth loss is primarily a consequence of untreated periodontal disease and tooth decay. Thus, systemic inflammation from underlying oral diseases may be a key driver of this association (Aoyama et al 2018) and may also explain the other indicators of poor metabolic health, such as higher rates of hypertension, increased BMI, and diabetes noted in women with a nonfunctional dentition in this study.
Strengths and Limitations
The study is a prospective study with 17 y of follow-up of a national sample of women, and although findings are not generalizable to men, there are fewer women represented in previous studies (Joshipura et al 1996; Lee et al 2019; Vedin et al 2020), and this study contributes to providing evidence for women. However, the women in the ALSWH tend to be healthier and of higher socioeconomic status (Dobson et al 2015); therefore, our study may underestimate the association between dentition status and incident CVD. Furthermore, despite prespecified confounder adjustment, unmeasured or imperfectly measured behavioral factors (e.g., diet, alcohol, activity) may still influence the observed associations.
Diet and tooth loss information were collected using self-reported surveys, which introduces the potential for information bias (Althubaiti 2016). Participants may inaccurately or deliberately under- or overreport the diet and tooth information, resulting in self-reporting bias and possible misclassification. Additionally, 13% of the dataset was excluded because of missingness (tooth and diet information), which could have caused selection bias. Participants with missing diet and tooth data were older, more likely to live in a rural or remote location, more likely to have a low income, and less likely to have a formal education. However, there were no differences in the rates of diabetes, hypertension, incident CVD, or fatal CVD. The analyses were unable to explore the role of systemic inflammation in the relation of dentition status and CVD, as inflammatory marker data were not collected, but this would be important to examine in future studies. As the shortened instrument used to collect dietary information has not undergone validation against the original DQES, the results should be interpreted with caution and have limited comparability with studies using DQES-derived measures. Additionally, other measures of diet quality, such as the Mediterranean diet or DASH diet, could not be analyzed as survey 5 did not collect the necessary data to calculate these measures.
Conclusions
In this cohort study of 8,306 middle-aged women followed for up to 17 y, the presence of a functional dentition was associated with a reduced risk of incident CVD and higher diet quality. The findings argue for both earlier interventions to maintain functional dentition and the recognition that the loss of a functional dentition may be a marker of poor future cardiovascular health and prompt cardiovascular prevention action.
Author Contributions
S. King: contributed to conception and design, data acquisition, analysis, and interpretation, drafted and critically revised the manuscript; S. Marschner: contributed to design, data analysis and interpretation, critically revised the manuscript; D. Quintans: contributed to analysis, critically revised the manuscript; A. Gibson: contributed to conception, drafted and critically revised the manuscript; C.K. Chow: contributed to conception and design, data interpretation, critically revised the manuscript. All authors have their final approval and agree to be accountable for all aspects of work.
Supplemental Material
sj-docx-1-jct-10.1177_23800844261444275 – Supplemental material for Tooth Loss and Cardiovascular Disease: A 17-Year Australian Cohort Study
Supplemental material, sj-docx-1-jct-10.1177_23800844261444275 for Tooth Loss and Cardiovascular Disease: A 17-Year Australian Cohort Study by S. King, S. Marschner, D. Quintans, A. Gibson and C.K. Chow in JDR Clinical & Translational Research
Footnotes
Acknowledgements
The research on which this article is based was conducted as part of the Australian Longitudinal Study on Women’s Health by the University of Queensland and the University of Newcastle. We are grateful to the Australian Government Department of Health, Disability and Ageing for funding and to the women who provided the survey data.
The CCMS datasets are produced as part of the Australian Longitudinal Study on Women’s Health by the University of Queensland and the University of Newcastle. We also acknowledge the following:
• The Australian Government Department of Health, Disability and Ageing for providing MBS, PBS, and Aged Care data and the Australian Institute of Health and Welfare (AIHW) as the integrating authority
• The Data Linkage Unit at the Australian Institute of Health and Welfare (AIHW) for undertaking the data linkage to the National Death Index (NDI)
• The Centre for Health Record Linkage (CHeReL), NSW Ministry of Health and ACT Health, for the NSW Admitted Patients and Emergency Department Data Collections, and the ACT Admitted Patient Care and Emergency Department Data Collections
• Queensland Health as the source for Queensland Hospital Admitted Patient and Emergency Data Collections and the Statistical Analysis and Linkage Unit (Queensland Health) for the provision of data linkage
• The Linkage, Data Outputs and Client Services teams at Data Linkage Services Western Australia, as well as the Data Custodians of the WA Hospital Morbidity and Emergency Department Data Collections
• SA NT DataLink, SA Health, and Northern Territory Department of Health for the SA Public Hospital Separations, SA Public Hospital Emergency Department, NT Public Hospital Inpatient Activity, and NT Public Hospital Emergency Department Data Collections
• The Department of Health Tasmania and the Tasmanian Data Linkage Unit for the Public Hospital Admitted Patient Episodes and Tasmanian Emergency Department Presentations Data Collections
• Victorian Department of Health as the source of the Victorian Admitted Episodes Dataset and the Victorian Emergency Minimum Dataset and the Centre for Victorian Data Linkage (Victorian Department of Health) for the provision of data linkage
The authors thank Professor Graham Giles and Professor Roger Milne of the Cancer Epidemiology Centre of Cancer Council Victoria for permission to use the Dietary Questionnaire for Epidemiological Studies (Version 2), Melbourne: Cancer Council Victoria, 1996
The authors also thank Ms Haeri Min for assisting with data programming
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Data Availability
ALSWH survey data are owned by the Australian Government Department of Health, Disability and Ageing, and due to the personal nature of the data collected, release by ALSWH is subject to strict contractual and ethical restrictions. Ethical review of ALSWH is by the Human Research Ethics Committees at the University of Queensland and the University of Newcastle. Deidentified data are available to collaborating researchers upon formal approval by the ALSWH Data Access Committee. The committee is receptive to requests for datasets required to replicate results. Information on applying for ALSWH data is available from https://alswh.org.au/for-data-users/applying-for-data/. In addition, linked administrative data have been provided by third parties (see details here https://alswh.org.au/for-data-users/linked-data-overview/linked-data-sources/). In order for these linked data to be accessed through ALSWH, every data user must be added to the applicable Data Use Agreements and Human Research Ethics Committee protocols. Details of the HREC protocols covering the use of linked data are listed here (![]() ).
).
A supplemental appendix to this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.