
Abstract
Background:
The aim of this study was to determine whether dental providers wrote fewer prescriptions for opioid-containing medications and more prescriptions for non-opioid analgesics after taking a continuing education course that targeted both knowledge about an American Dental Association–endorsed guideline on the management of acute dental pain and challenges in shared decision-making.
Methods:
The implementation strategy comprised a prerecorded 1-h video continuing education course and supplementary materials that were previously shown to increase knowledge about shared decision-making. Using propensity score matching, we matched 420 dentists and dental specialists who took the continuing education course to 4,200 providers who had not. We used regression analyses to compare learners with their propensity score–matched controls on their change in opioid prescribing and change in non-opioid analgesic prescribing from the 6 mo before to the 6 mo after course completion.
Results:
Providers who took the continuing education course decreased the number of opioid prescriptions they wrote by 0.60 prescriptions more than providers who did not take the continuing education course (B = −0.60; 95% confidence interval [CI] −1.07, −0.13; t = −2.50; P < 0.01). Among providers who decreased their prescribing by 3 or more prescriptions, a greater percentage took the continuing education course. There was no difference in non-opioid analgesic prescribing between providers who took the continuing education course and providers who did not (B = −0.10; 95% CI −0.87 0.68; t = −0.25, ns).
Conclusion:
Equipping dental providers with skills in shared decision-making to use in conversations with patients about approaches to acute pain management may enable them to decrease the number of opioid prescriptions they write more than providers who are not exposed to these skills.
Knowledge Transfer Statement:
The results of this study can be used by groups and organizations seeking to improve dental providers’ adherence to the guideline on managing acute dental pain following simple and surgical tooth extraction or toothache.
Keywords
Dentists and dental specialists prescribe medication to manage acute pain for a number of conditions including having a tooth removed or having a dental infection. For managing acute or postoperative dental pain, American Dental Association (ADA)–endorsed evidence-based clinical practice guidelines recommend nonsteroidal anti-inflammatory drugs (NSAIDs) or a combination of NSAID and acetaminophen as first-line therapy (Carrasco-Labra et al 2023, 2024). If opioids are indicated, then short-acting opioids in combination with an NSAID or acetaminophen can be considered for up to 3 d (Carrasco-Labra et al 2024). With few exceptions, opioids are not recommended to manage acute dental pain. Nonetheless, in 2022, more than 7.4 million patients filled more than 8.9 million opioid prescriptions prescribed by US dentists and oral and maxillofacial surgeons (Zhang et al 2023). Each filled prescription increases the patient’s risk of misuse and opioid use disorder (McCabe et al 2013), and 54% of patients fill but do not completely consume their prescribed opioids (Maughan et al 2016), increasing the risk of non–medically related use or misuse. Thus, approaches are needed to assist providers in adopting the guidelines and evidence-informed dentistry.
Current approaches to encourage providers to reduce their reliance on opioids include requiring prescribers to participate in state prescription drug-monitoring programs and to complete training in pain management. Approaches also include increasing providers’ knowledge of guidelines through educational channels. In addition to the lack of knowledge about the guidelines, however, other barriers to reducing opioid prescribing exist. Based on our formative research and framed by the COM-B model of behavior change (Michie et al 2014), some providers report challenges in communicating with patients about pain management strategies (Yan et al 2022). This is a problem of capability, which can be addressed by implementation strategies that build provider communication skills, such as training. Without exposure to strategies that build communication skills, providers may default to practices with which they are familiar, such as prescribing pain relief medications that contain opioids and not engaging in shared decision-making with the patient. Previously, we showed that a continuing education (CE) course we developed increased providers’ knowledge of shared decision-making skills to use with patients when discussing approaches to pain management (Polk et al 2024).
The aim of this study was to determine whether dental providers wrote fewer prescriptions for opioid-containing medications after taking a CE course that targeted both knowledge about the ADA-endorsed guideline and barriers in patient communication (Polk et al 2024) and whether they wrote more prescriptions for non-opioid analgesics.
Methods
Human Subjects Protection
The University of Pittsburgh Institutional Review Board determined that evaluating the effect of the CE course on change in providers’ opioid prescribing was exempt because it involved an educational test (Exemption 45 CFR 46.104(d)(2)) and because it was secondary research for which consent was not required (Exemption 45 CFR 46.104(d)(4)). This study followed the STROBE guideline (von Elm et al 2008) and was exempt from ethics review and informed consent; however, participants received an introductory script.
Study Design
We conducted an analytical observational study using regression analysis with propensity score matching. Our estimand was the average treatment effect on the treated (ATT). Our causal question was, “How would opioid and non-opioid analgesic prescribing in those who took the CE course have differed if they had not taken the course?”
Implementation Strategy
The implementation strategy comprised a prerecorded 1-h video CE course and supplementary materials. The CE course covered 4 domains: epidemiological information about opioid use in the United States, guideline-concordant information about managing acute dental pain, skills in shared decision-making with patients, and skills in how to incorporate a guideline into clinical practice.
As a part of the shared decision-making skills, the course introduced a conversation aid for use with patients. Several aspects of the conversation aid are novel. First, although most conversation aids compare only 2 choices, ours enabled multiple comparisons (ie, rows in Appendix Figure 1), which is needed for decision making to manage acute dental pain. Second, the conversation aid displayed information about practical issues associated with each treatment option (ie, columns in Appendix Figure 1). For pain medications, these include high risk of misuse or substance use disorder among adolescents; central nervous system effects (eg, dizziness, drowsiness), which could affect the patient’s ability to drive a car or go to work; and gastrointestinal effects (eg, nausea, vomiting, constipation), which some patients may find intolerable. The conversation aid enables patients to make a decision that both aligns with their values and preferences and is informed by the best available evidence, presenting information in a format patients can understand and clinicians can use.
Materials supplementing the course were also available via Internet links. Guideline-specific resources included links to the systematic reviews on which the guidelines were based, the conversation aid, and chairside clinical decision guides for use by the provider. In addition, Internet links were included to resources describing the safe disposal of drugs, substance use screening, how to talk to children and adolescents, and how to find the providers’ states’ prescription drug monitoring database.
The ADA launched the CE course and supplementary materials on their CE learning management system (Aptify, v. 6.0, CommunityBrands) in July 2022. The course was freely available to anyone, including people who were not members of the ADA, and learners could obtain 1 ADA CERP credit.
Participants
We adopted several approaches to recruiting providers to take the CE course (see Polk et al 2024 for more details). Initially, from July 2021 to April 2023, we recruited in Alabama, Arizona, Colorado, Montana, and Oregon because those states had high rates of opioid prescribing and represented diverse geographic regions of the country. In each of these states except Montana, dentists are required to complete CE on substance use, pain management, or opioids to get or renew their dental licenses (ADA 2025). The Association for State and Territorial Dental Directors connected us to the state dental directors in these states, who guided us in how best to promote the CE course to dental providers in their states. Based on their guidance, the ADA prepared promotional materials, which were shared with the state dental directors, state dental associations, and dental societies in December 2021. In July 2022, the ADA emailed all dental providers in the 5 states with a link to the course. In December 2022, the ADA developed and distributed promotional materials demonstrating the effectiveness of the course in increasing knowledge, based on the change in pretest and posttest scores. In April 2023, the ADA promoted the course to all ADA members nationwide. Thus, study participants were not limited to the 5 states initially selected.
Data Sources
CE course pretest
Prior to completing the CE course, learners completed a pretest on the Qualtrics platform. Variables used in this study included the date when the learners took the CE course (i.e., their index date) and their unique National Provider Identifier (NPI). For a description of the pretest and posttest see Polk et al (2024).
IQVIA LRx dataset
The IQVIA LRx dataset is a commercially available longitudinal dataset that contains approximately 92% of all dispensed outpatient prescriptions in the United States, including prescriptions dispensed without insurance reimbursement (ie, cash pay). Each prescription in LRx includes the drug name, dose, formulation, number of doses dispensed, date dispensed, patient demographics, and the publicly available NPI for the prescribing provider. The IQVIA variables used in this study included the USC level 3 codification (usc_lvl3_cd) and description (usc_lvl3_desc) and NPI.
Centers for Medicare and Medicaid Services National Plan and Provider Enumeration System (NPPES) downloadable file
The Centers for Medicare and Medicaid Services NPPES file contains demographic (ie, sex and specialty, including orofacial pain) and practice (ie, address, sole proprietor status, single- or multispecialty group) data for all US providers, including those who do not provide treatment to Medicare or Medicaid patients. The data are freely available for public use. We restricted the IQVIA LRx dataset to prescriptions written by dentists and dental specialists who practiced in a US state. Variables used in this study included NPI, sex, state where the practice is located, and specialty.
Data Analysis
To increase the likelihood that we were identifying participants who did not drop out before taking the CE course, from the CE course pretest, we identified the NPIs of learners who completed at least 80% of the pretest. We chose 80% because that is a common threshold for CE course tests to count toward CE credits. Learners were not required to take the CE course pretest. We linked these NPIs to the IQVIA LRx dataset and identified providers who had prescribed a medication containing an opioid at least once in the 6 mo before or 6 mo after the date on which they took the CE course (ie, their index date). This included prescriptions written from January 2022 through December 2023. From the NPPES dataset, using the NPI, we obtained providers’ sex, specialty, and geographic region. We used these variables to group learners into 186 unique groups and determined the range of index dates for each group. We matched providers who did not take the CE course by their sex, specialty, and geographic region to one of the unique groups of learners. We assigned providers who did not take the CE course to a randomly selected, synthetic index date from the range of index dates of learners in the same group (sampling without replacement).
We calculated sums of the number of opioid prescriptions, non-opioid analgesic prescriptions, and total prescriptions (this includes opioids, non-opioid analgesics, and other medications such as antibiotics) each provider wrote in the 6 mo before taking the CE course (or their synthetic index date). To calculate proportions, we divided the number of opioid prescriptions (or non-opioid prescriptions) each provider wrote in the 6 mo before the CE course by the total number of prescriptions each provider wrote in the 6 mo before the CE course. Starting with all prescribers included in the IQVIA dataset from 2017 to 2023, we removed prescribers who did not live in the US states, were not dental providers or dental specialists, who did not fall into 1 of the 186 demographic groups, and who had not prescribed an opioid in the 6 mo before or after the index date.
To calculate the outcome variables, we quantified change in opioid prescribing (or non-opioid analgesic prescribing) per provider by subtracting the sum of the number of opioid prescriptions (or non-opioid analgesic prescriptions) they prescribed in the 6 mo before they took the CE course from the number of opioid prescriptions (or non-opioid analgesic prescriptions) they prescribed in the 6 mo after they took the CE course (ie, post – pre), creating a change score. By taking post minus pre, a number greater than zero indicates that the prescribing increased and a number less than zero indicates that the prescribing decreased.
Next, we calculated propensity scores using 3 instrument variables that have been shown to be associated with taking CE courses (Langelier et al 2021) and 4 confounding variables that have been shown to be associated with both taking CE courses (Langelier et al 2021) and opioid prescribing (Khouja et al 2024) and matched each provider who took the CE course to 10 providers who did not. Instrument variables included the providers’ sex, geographic region of practice (ie, Northeast, South, Midwest, and West), and specialty. Confounding variables included number of opioid prescriptions written in the 6 mo before taking the CE course, number of non-opioid analgesic prescriptions written in the 6 mo before taking the CE course, proportion of total prescriptions that were opioids in the 6 mo before taking the CE course, and proportion of total prescriptions that were non-opioid analgesics in the 6 mo before taking the CE course.
We characterized prescribing using descriptive statistics. We used a regression modeling framework to estimate the main effect of exposure to the CE course on both change in opioid prescribing and change in non-opioid analgesic prescribing. To control for the confounding effects of prescribing volume and prescribing proportion, we included as covariates the number of opioid prescriptions written, the number of non-opioid analgesic prescriptions written, the proportion of opioid prescriptions written, and the proportion of non-opioid analgesics prescriptions written. All covariates characterized prescribing in the 6 mo before taking the CE course or synthetic index date. All continuous variables were centered at the mean. We also analyzed high-volume opioid prescribers by examining the top 10% of prescribers (Nataraj et al 2019) in our matched data set. We used a t test to evaluate changes in opioid prescribing by CE course status.
Results
Applying the inclusion criteria resulted in 63,193 providers in the IQVIA dataset, 420 of whom had completed at least 80% of the CE course, and 4,200 of whom were propensity score matched providers who had not (Fig). Among learners, 39.5% (420/1,062), prescribed at least 1 opioid in the 6 mo before or 6 mo after they took the course. Among controls, 35.3% (62,773/177,932) prescribed at least 1 opioid in the 6 mo before or 6 mo after their synthetic index date. Combining learners and propensity score–matched controls, 52.9% (2,445/4,620) providers prescribed at least 1 non-opioid analgesic in the 6 mo before or 6 mo after their index date or synthetic index date.

Selection diagram of dental providers and dental specialists.
Compared with providers in the pool from which matches were drawn, learners were more likely to be women (37.6% versus 28.1%), less likely to be general practice dentists (45.7% versus 55.5%) and more likely to be specialists (16% versus 6.9%), less likely to be from the South (30.0% versus 39.7%), and more likely to be from the West (42.6% versus 30.6%; Table 1). Prior to taking the CE course, learners and propensity score–matched controls wrote similar numbers of opioid and non-opioid analgesic prescriptions, and the proportions of opioid and non-opioid analgesic prescriptions they wrote were similar. Propensity score matching reduced the standardized mean differences between the groups on the 3 treatment variables and all but 1 of the 4 confounding variables, bringing all values well below the 0.20 threshold for a small effect.
Descriptive Statistics and Standardized Mean Differences for Study Variables.

ATT, average treatment effect on the treated; IQR, interquartile range; SD, standard deviation; SMD, standardized mean difference.
Learners and propensity score–matched prescribers were included in the study if they did not write an opioid prescription in the 6 mo before the index date but did write at least 1 opioid prescription in the 6 mo after the index date. There were 81 learners and 780 matched prescribers who did not take the CE course meeting this definition. The learners wrote 1 to 6 opioid prescriptions in the 6 mo after their index dates. In the 12-mo period around their index dates, they wrote 1 to 23 non-opioid analgesic prescriptions and 1 to 88 total prescriptions. Among the 780 matched prescribers who did not take the CE course meeting the definition, only 7 exceeded 6 opioid prescriptions in the post–index date period. In the 12-mo period around their synthetic index dates, they wrote 1 to 93 non-opioid analgesic prescriptions and 1 to 205 total prescriptions.
Effect of the CE Course on Opioid and Non-opioid Analgesic Prescribing
We examined the effect of taking the CE course on the change in the number of opioid prescriptions written from the 6 mo before to the 6 mo after the index date. After adjusting for confounders, providers who took the CE course decreased the number of opioid prescriptions they wrote by 0.60 prescriptions more than providers who did not take the CE course (B = −0.60; 95% CI −1.07, −0.13; t = −2.50; P < 0.01; Table 2). Among providers who decreased their prescribing by 3 or more prescriptions, a greater percentage took the CE course (Table 3). After adjusting for confounders, there was no difference in non-opioid analgesic prescribing between providers who took the CE course and providers who did not (B = −0.10; 95% CI −0.87, 0.68; t = −0.25, ns; Table 4). Models without the confounders yielded the same results.
Regression Results for Change in Opioid Prescribing as a Function of Exposure to the CE Course, Controlling for Confounders (n = 4,620).
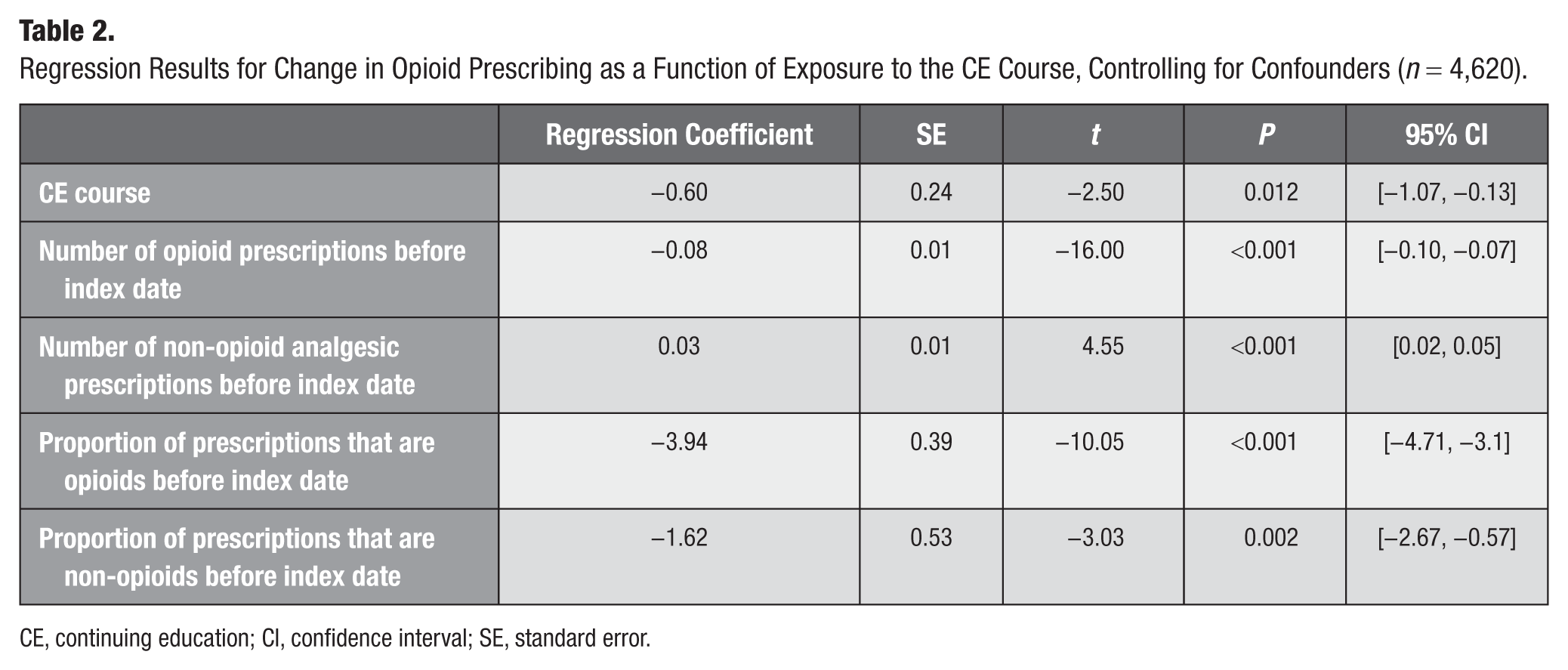
CE, continuing education; CI, confidence interval; SE, standard error.
Number and Percentages of Dental Providers and the Change in the Number of Opioid Prescriptions They Wrote from the 6 mo before the Index Date to the 6 mo after the Index Date.

Regression Results for Change in Non-opioid Prescribing as a Function of Exposure to the CE Course, Controlling for Confounders (n = 2,445).

CE, continuing education; CI, confidence interval; SE, standard error.
This analysis includes only dental providers who prescribed at least 1 non-opioid analgesic in the 6 mo before and 6 mo after the index date.
Post Hoc Descriptive Analyses of High Opioid Prescribers
See Appendix Figure 2 for the cumulative frequency distribution of opioid prescribing of learners prior to taking the course. The top 10% of prescribers among the learners and propensity score–matched controls wrote at least 15 opioid prescriptions in the 6 mo before the index date. Due to ties, this group consisted of 45 learners and 441 controls. In this high-prescribing group, learners reduced the number of opioid prescriptions they wrote by 6.1 prescriptions, and those who did not take the CE course reduced the number of opioid prescriptions they wrote by 3.7 prescriptions, on average (Table 3). This difference was not significant (P = 0.19).
Discussion
Over the 12-mo observation period and after accounting for pre-CE course opioid and non-opioid analgesic prescribing volume and proportion, providers who took the CE course reduced the number of opioid prescriptions they wrote by more than half a prescription more than providers who did not take the CE course. There was no difference between learners and controls in change in number of non-opioid prescriptions, however.
The ATT indicates that for providers who were treated (ie, chose to take the CE course), taking the CE course caused more than half a prescription greater decrease in opioid prescribing compared with the decrease in opioid prescribing by providers who did not take the CE course. This is consistent with our hypothesis. Among providers who decreased their prescribing by 3 or more prescriptions, a greater percentage took the CE course. Although our sample size was too small to draw definitive conclusions, the direction of effects suggests that even high prescribers may reduce their prescribing following exposure to the CE course. To determine the clinical significance, future research should evaluate changes in rates of opioid-related adverse outcomes (Gewandter et al 2021).
Although we hypothesized that providers who decreased their opioid prescribing might increase their non-opioid analgesic prescribing, we did not observe this behavior. The findings with respect to non-opioid analgesic prescribing may be conservative, however. Although providers may choose to write a prescription for non-opioid analgesics, patients are also able to and prefer to (Preshaw et al 1994; Arcury et al 2009; Dawson et al 2023) obtain them over the counter. Thus, it is possible that some unknown number of patients took unprescribed non-opioid analgesics that they obtained over the counter. These unprescribed medications were not captured in our analysis, which could have resulted in an undercounting of a shift to this approach to pain management.
Education interventions, such as CE courses, are not powerful interventions (Eaton et al 2011; Bailey et al 2020). Although knowledge is necessary for behavior change, it is often not sufficient. According to the COM-B model of behavior change (Michie et al 2011), in addition to knowledge (ie, capability), providers also need opportunity and motivation to change their behavior. For example, it has been shown that the motivation of emergency medicine providers to reduce their opioid prescribing is decreased by their concerns that their patient satisfaction scores will go down if they do not prescribe opioids (Penm et al 2019). We designed the CE course to address motivation in several ways. We included information about the superior pain management of NSAIDs and acetaminophen compared with opioids, and we provided learners training in communication and shared decision-making skills. Both of these aspects may have alleviated providers’ concerns about patient satisfaction. Thus, it is possible that the combination of education in the guideline recommendations and training in communication and shared decision-making skills increased both providers’ capability and their motivation and enabled the providers to reduce the number of opioid prescriptions they wrote.
Asynchronous online CE courses have several advantages. Once they have been developed, typically they are inexpensive to deliver. They can be delivered at scale; our CE course reached learners across the United States, including high prescribers. And generally, learners find them both familiar and acceptable. Future research should compare the CE course’s reach, effectiveness, and cost with those of more intensive interventions.
Overall, only about a third of dental providers wrote prescriptions for opioids, and among those who did, almost all wrote fewer than 16 opioid prescriptions in the 6 mo before or after their index date or synthetic index date. Most of the opioid prescriptions were written by the top 10% of opioid prescribers. Future research should be powered to examine the opioid prescribing of these high prescribers.
This study has several strengths. We used propensity score matching and the ATT approach to causal inference, which strengthened our ability to draw causal conclusions. We were able to match each provider who took the course to 10 who did not, which increases the precision of our estimates. We also examined prescribing behaviors out to 6 mo after the providers took the CE course, enabling us to include any persistence or fade out of changes in prescribing behavior (Bailey et al 2020). Assuming that a provider’s approach to managing acute dental pain becomes a habit, it is likely that the decrease in opioid prescribing that we observed will persist. It has been shown that the median number of days it takes for a habit to form is 66 d (Lally et al 2010). Thus, it is possible that those providers who reduced their prescribing formed a new prescribing habit and may maintain the reduced prescribing. Finally, we included prescriptions written before the guideline was released, which increases our confidence that the results were due to exposure to the CE course and not exposure to the guideline.
The study has some limitations as well. Because we could not randomly assign dental providers to take or not take the CE course, self-selection bias may have occurred. This bias would lead us to conclude that the CE course was more effective in changing prescribing behavior than it actually was. To eliminate this source of bias completely, random assignment would be necessary. We attempted to address this source of bias by using propensity score matching. That the standardized mean differences on the instruments and confounders were negligible and that there was little difference in the results of the analyses with and without the confounders included suggest that our propensity score matching resulted in little residual confounding. The possibility remains, however, that unobserved provider characteristics may have biased our findings.
In addition, we were unable to measure the patients’ preferences with respect to managing their dental pain. It may be that using shared decision-making skills, providers prescribed opioids to patients who preferred opioids. We have shown that although most patients prefer nonprescription and non-opioid analgesics, patients are more willing to accept opioids when they believe their pain will be severe (Dawson et al 2023). Relatedly, we did not know patients’ contraindications and the dental procedures associated with the prescriptions. Thus, an unknown percentage of the prescriptions may have been for patients for whom NSAIDs or acetaminophen were contraindicated or for conditions other than simple or surgical tooth extraction or toothache, for which there are no evidence-informed clinical practice guidelines.
Finally, our data were not normally distributed. However, our analytic strategy was robust to the nonnormality. In addition, it is possible that some providers completed at least 80% of the pretest but did not complete the CE course. It is possible that some providers took the CE course and were classified as controls because they did not complete the pretest. We have no way of evaluating these possibilities. These limitations have the effect of making our analyses more conservative.
In sum, we found that a CE course that improved learners’ shared decision-making knowledge led to a greater reduction in the number of opioid prescriptions they wrote compared with controls, but the CE course did not increase non-opioid analgesic prescribing. Future research should examine whether the effect of the CE course on change in opioid prescribing is mediated through providers’ use of shared decision-making skills with their patients and whether the effect of the CE course varies depending on the dental procedure the patient receives.
Author Contributions
D.E. Polk, contributed to conception and design, data analysis and interpretation, drafted and critically revised the manuscript; A. Carrasco-Labra, contributed to conception and design, data interpretation, critically revised the manuscript; N.H. Shah, N. Mukhopadhyay, contributed to conception and design, data analysis and interpretation, critically revised the manuscript; K.J. Suda, contributed to conception and design, data interpretation, critically revised the manuscript. All authors approved the final version of the manuscript and agreed to be accountable for all aspects of the work.
Footnotes
Appendix
Appendix Figure 1 displays a conversation aid dental providers and adult patients can use when engaging in shared decision-making around managing the acute dental pain resulting from a simple or surgical tooth extraction. In the upper left, the condition and population to which the conversation aid applies are listed. In the upper right, there is a graphic depiction of the amount of acute dental pain to expect and the number of days to expect it. The rows present different pharmacologic approaches to managing acute dental pain. The first column describes the conditions in which each row is appropriate. The second column describes how the medication can be obtained. The third column lists the name and dose of the medication. The fourth column lists the maximum daily dose. The fifth column presents a graphic depiction of the strength and hours of pain relief from a dose. The sixth column presents a graphic depiction of common side effects and caution indicators. Similar conversation aids were created for adults managing the pain of toothache when definitive treatment is unavailable and for children following simple or surgical tooth extraction and toothache when definitive treatment is unavailable. All conversation aids can be obtained for free at https://www.ada.org/resources/research/science/evidence-based-dental-research/pain-management-guideline.
Appendix Figure 2 demonstrates that in the 6 mo prior to taking the continuing education (CE) course, the opioid prescribers in the 0 to 90th percentiles of number of prescriptions written prescribed fewer than 16 prescriptions. The prescribers in the 90th to 100th percentiles prescribed between 16 and 120 prescriptions and accounted for 65% of the number of prescriptions written. Furthermore, the range of the number of prescriptions written was greater among the prescribers in the 90th to 100th percentiles than among the prescribers in the 0 to 90th percentiles.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was financially supported by grant U01FD007151 from the US Food and Drug Administration (FDA) of the US Department of Health and Human Services. The contents are those of the authors and do not necessarily represent the official views of, nor an endorsement by, the FDA, Department of Health and Human Services, the Department of Veterans Affairs, the US government, or of IQVIA or any of its affiliated entities. The statements, findings, conclusions, views, and opinions contained and expressed in this article are based in part on data obtained under license from IQVIA (source: LRx, January 2022 to December 2023, IQVIA). All rights reserved.
Data Availability
The data cannot be shared. This is because they are commercially available. They are not available except by purchase from the company.