
Abstract
Introduction:
Children accessing early childhood intervention due to developmental concerns or disability may be less likely to receive regular dental care compared with the general pediatric population. This qualitative study explores the perspectives of parents and carers regarding their children’s experiences with dental services.
Methods:
A qualitative descriptive design was used to study families accessing early childhood intervention services at a community health service in Melbourne, Australia. Convenience and purposive sampling was used to recruit families of children aged 0 to 6 y. Semi-structured interviews were conducted, recorded, and analyzed using thematic analysis to explore perspectives on the oral health needs and experiences of families.
Results:
Participants included 11 parents of children aged 1.5 to 6.4 y. Parents were primarily mothers, with 1 interview including both parents and another including the father. Three themes were developed regarding child and family experiences, and 3 themes were developed relating to opportunities to improve dental care as part of early childhood intervention.
Discussion:
This study highlighted the anxiety and distress faced by children with complex needs and their families in the traditional dental environment setting. Sensory sensitivities led to avoidance of dental visits and compromise of oral health status. A holistic preventative approach emphasizing desensitization coupled with improved practitioner training in disability awareness could mitigate anxiety. Systemic barriers, including fragmented health care and inadequate support networks, further impeded access. Reforms prioritizing person-centered care are essential to address these unmet needs.
Conclusion:
This study highlighted the need for tailored resources, integrated care models, accessible services, sensory-friendly environments, and flexible approaches to dental care to improve oral health outcomes for children accessing early childhood intervention. Future research should explore these issues from the perspective of health care providers and investigate co-designed interventions to address the identified barriers.
Knowledge Transfer Statement:
The results of this study can be used to inform patient-centered approaches to dental care for children with developmental concerns and/or disability who are accessing early childhood intervention services. The perspectives of families suggest that clinicians, health services, and policymakers all play an important role in improving dental experiences for children and their families.
Keywords
Introduction
Aligned with the Convention on the Rights of the Child, health systems globally recognize the importance of supporting optimal early childhood development (UNICEF 1989; Olusanya et al 2023). The rationale for monitoring and intervening in early childhood is the potential to leverage early developmental plasticity to establish pathways to support all children to thrive (Imms et al 2024). Despite some variation, international frameworks for best practice in early childhood intervention (ECI) all have common elements, being child and family centered, inclusive, and involving community-based services. ECI services support children with variations in early childhood development, from temporary developmental concerns or developmental delay to disability. The term “developmental concerns” is nonspecific but reflects terminology used within an Australian ECI framework (Imms et al 2024). “Developmental delay” refers to delayed attainment of developmental milestones compared with the typically expected age of attainment and is often used clinically when there are concerns about a child’s development but a more specific clinical diagnosis has not been made (Choo et al 2019). Developmental disabilities are likely to continue indefinitely, requiring additional coordinated services, support, or other assistance for an extended duration or during a lifetime, and represent a subset of conditions that affect children with special health care needs (Boulet et al 2009). While ECI supports a broad range of children and families, its significance for the disability health sector has led to its inclusion as part of Australia’s Disability Strategy (Commonwealth of Australia, Department of Health 2021).
What remains less clear is how oral health fits into this broader ECI framework. Dental disease in childhood can lead to pain, infection, hospitalization, and poorer quality of life. Children with developmental disabilities may have unmet dental needs and poor access to dental services (Norwood et al 2013; Zhou et al 2017). Underrecognized or untreated dental issues can significantly affect nutrition due to difficulty chewing and swallowing, potentially leading to malnutrition (Souza et al 2018). In addition, the pain and discomfort associated with dental problems can contribute to behavioral issues, irritability, and sleep disturbances, further affecting a child’s overall well-being (Guarnizo-Herreño and Wehby 2012). Dental diseases, such as dental caries, are almost entirely preventable through optimal habits such as twice-daily brushing and reduction in sugar intake (Rugg-Gunn 2013). As early childhood is a key developmental period with implications for long-term health, establishing good oral health habits has benefits throughout the life course (Guyer et al 2009). However, this may be more challenging for families of children who require ECI due to developmental concerns and/or disability. Despite a paucity of data, there is emerging evidence that people, including children, with disability are more likely to have poor oral health (Desai et al 2001; Braúna et al 2016; Wilson et al 2019; Pradhan et al 2021). Factors, such as oromotor dysfunction, including dysphagia (difficulty swallowing) (Calis et al 2008), oral aversion (strong dislike of oral sensations), restrictive diets, or sensory difficulties with dental hygiene practices (Stein et al 2011) are some factors that may contribute to poorer oral health among children with disabilities.
This qualitative study aimed to explore parental perspectives about dental services for their children accessing ECI services due to developmental concerns and/or disabilities. This study’s specific objectives were to explore the parent’s perspectives (1) about their families’ experiences with dental services and (2) opportunities to improve dental care for children with developmental concerns and/or disabilities. The intention of the study was to identify strategies to overcome the barriers experienced by families with children with developmental concerns and/or disabilities to improve access to ongoing and timely preventive health care.
Methods
A qualitative descriptive design (Willig and Rogers 2017) was used to explore the experiences and perspectives of families of young children accessing an ECI service regarding their child’s oral health needs. This project was approved by the University of Melbourne Human Research Ethics Committee (ref No. 26759).
Families of children with developmental concerns and/or disabilities were recruited from the ECI services delivered by the Child and Family Team (CFT) at Access Health and Community, a government-funded community health service in the inner eastern/northeastern suburbs of Melbourne, Australia. Specifically, families with children receiving ECI services due to any identified developmental concerns were eligible to participate in this study. The clinicians providing the ECI services comprise allied health personnel (physiotherapy, speech therapy, occupational therapy, psychology, and music therapy) who provide support for families of children who have any developmental concern. Consistent with ECI, the CFT service does not employ specific criteria for intake and includes all children presenting with any form of developmental concern. An ECI clinician is assigned to each family as a key worker and coordinates a range of additional support services based on the individual needs of the child. Families can engage with ECI services up to 12 y of age; however, the extent and duration of engagement vary.
The inclusion criteria for the study were parents and/or legal guardians of a child aged between 0 and 6 y, with developmental delay and/or disability, who was engaged with the Access Health and Community ECI program.
The study was conducted in consultation with 4 consumer representatives, who were parents of children with developmental delay and/or disability. They contributed to the development of the project by providing feedback on participant-facing resources and the interpretation of the study findings. Three of the consumer representatives were clinicians within the Access Community and Health ECI service. Over a series of 5 meetings held between July 19, 2023, and March 26, 2024, the consumer group provided feedback about the recruitment process, participant-facing resources and the interpretation of the study findings.
Recruitment was supported by ECI key workers, who approached eligible families during their routine sessions to introduce the study and support families to access the online plain language statement and REDCap consent form. An interpreter was used to support recruitment and participation of non–English-speaking participants. Recruitment ceased at the point of saturation when no new data or themes emerged (Willig and Rogers 2017).
Parents who provided written consent completed a brief questionnaire about their demographics, their child’s health, reporting in their own words, any developmental concerns, and diagnoses relating to their child. Socio-Economic Indexes for Areas (SEIFA) deciles within Australia were extracted based on postcode as a measure of socioeconomic disadvantage (Australian Bureau of Statistics 2021). Qualitative data were collected using a semi-structured interview guide, which aimed to capture rich and detailed narratives from the parents about their child’s oral health needs and experience of using dental services (see Appendix Table 1). This guide was developed collectively by the research team, which included researchers with backgrounds in health promotion, developmental pediatrics, physiotherapy, community health, psychology, and pediatric and special needs dentistry. Verbal consent was obtained prior to the interviews, which were audio recorded and conducted online via Zoom (Zoom Video Communication). Interviews were conducted by researchers with experience conducting qualitative interviews (O.W. and A.N.F.) and lasted between 14 and 31 min (mean 24.46 min; standard deviation 5.55 min). Transcription of the recordings was done verbatim by the research team, aided by Otter.ai (Otter.ai Inc.), an online automated transcription service.
Thematic analysis (Ahmed et al 2025) was led by T.K. (a qualified researcher in dentistry) with the support of O.W. and A.N.F. (research assistants with experience conducting qualitative research in the psychological sciences). The process began by familiarization with the interview transcripts to identify initial ideas, patterns, and meanings. This was followed by the generation of initial codes from the interview transcripts to identify meaningful sections of the transcripts that addressed research objectives. The research team collaborated to iteratively refine the codebook throughout the analysis, ensuring consistency in coding and accurately reflecting the nuances within the data. Initial themes were developed by grouping codes that were conceptually related. The codebook and initial themes were reviewed and refined by the broader research team. This process ensured that the themes represented a narrative account of families’ experiences and parent’s perspectives about accessing dental services. NVivo 14 software (QSR International) was used to organize, code, and analyze the data. This inductive approach aimed to provide flexibility, which enabled a comprehensive understanding of participant experiences.
Results
Participant Characteristics
The study reached a final sample size of 11 parents (10 interviews) after a pattern of repetition was observed in the interview data. All participants were mothers, except for 1 interview that included both parents (interview 1) and 1 interview with only a father (interview 4). Participants’ children ranged in age from 1.5 to 6.4 y (mean = 4.3 y) and included both male (n = 8) and female (n = 6) children, 2 of whom (from different families) were born outside of Australia. The index of relative socioeconomic disadvantage (2021) of participants ranged between the 5th and 10th decile (within Australia), indicating a relatively low level of area-level socioeconomic disadvantage. Parents reported that their children had a variety of health conditions and developmental concerns, including 9 children with autism spectrum disorder (ASD) and 6 with developmental delay. One interview was conducted with the assistance of an interpreter. The demographics of participating parents are presented in Table 1.
Participant Demographics.
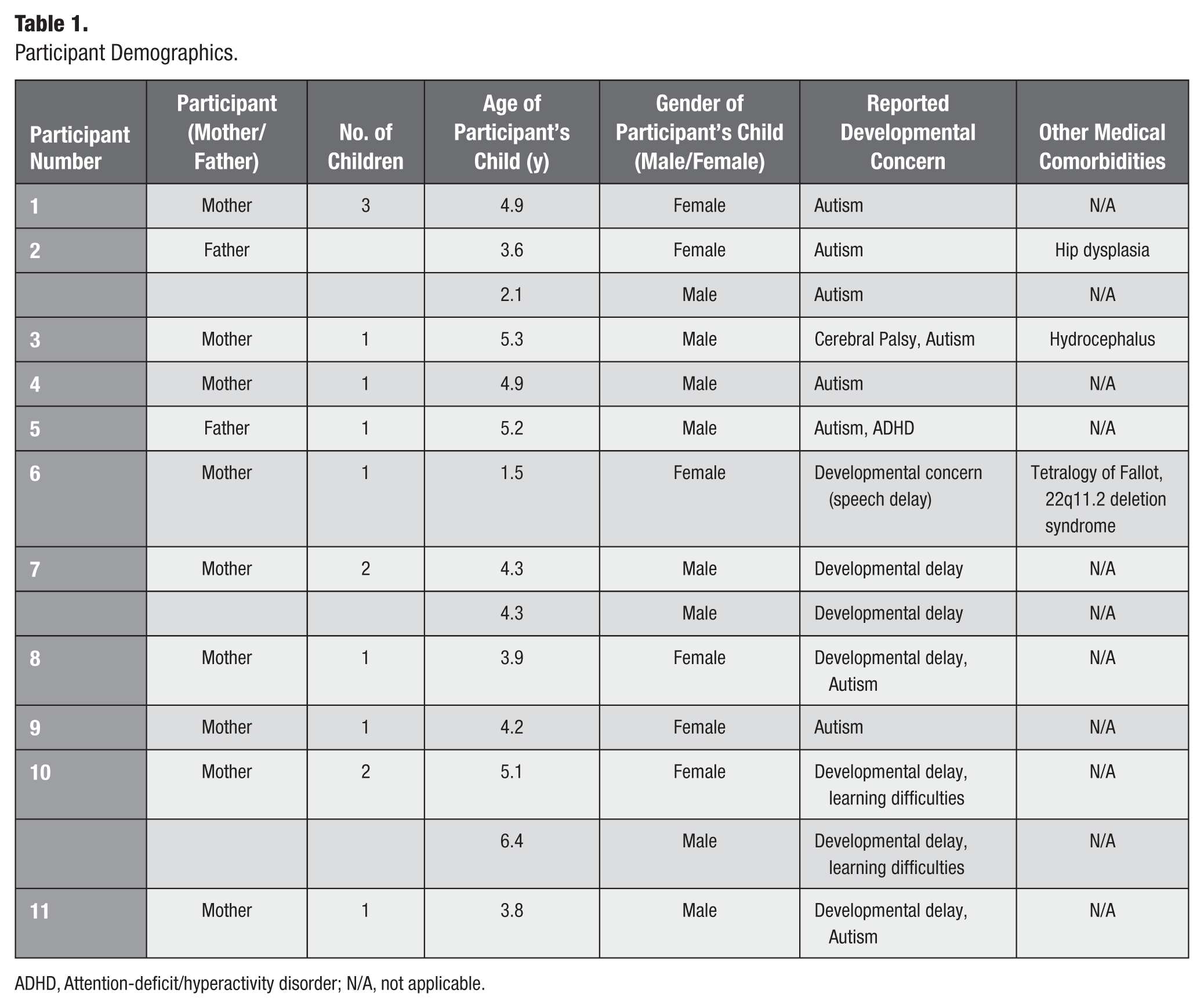
ADHD, Attention-deficit/hyperactivity disorder; N/A, not applicable.
Themes and subthemes are presented in Table 2.
Themes and Subthemes.
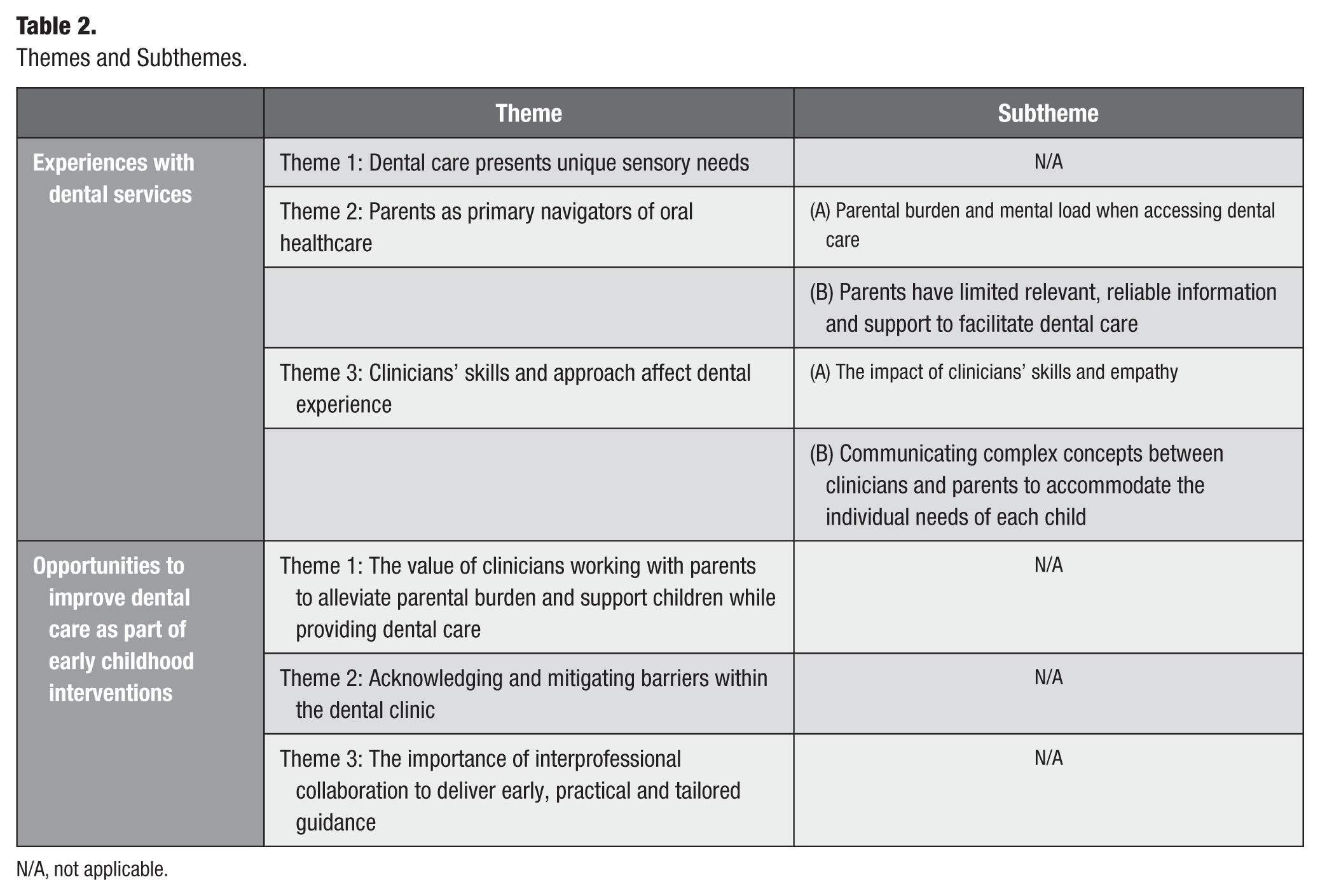
N/A, not applicable.
Experiences with Dental Services
Participants shared their experiences with dental services and the challenges facing their child and family. From this, 2 central themes were developed about their dental experiences in relation to (1) dental care presents unique sensory needs and (2) parents as primary navigators of dental care
Theme 1: Dental care presents unique sensory needs
In many cases, examples of sensory needs made basic aspects of dental care difficult. Some challenges were reported to be linked to previous medical interventions at a young age.
She was born at 28 weeks . . . had a feeding tube for the first 8 months of her life, so I think she really hates it when people interfere with her face and her mouth. (Participant No. 8)
Sensory stimuli, including sounds and tactile sensations, unique to dental care were also reported as distressing.
Usually the machinery that buzzes or hums he doesn’t like, he starts covering his ears. (Participant No. 5)
In addition to the sounds and tactile sensations related to dental services, the need to interact with unfamiliar people and environments was perceived to be particularly challenging.
In addition to her kind of ASD needs, she’s very uncomfortable with new people and in strange scenarios. (Participant No. 8)
Parents described how these sensory-related challenges ultimately necessitated general anaesthesia to facilitate essential dental treatment.
They took some, you know, photographs from a camera and not any X-rays or anything like that, just because, he was fighting it all the way. So, you know, it’s very, very difficult. And we made the decision to rather than try and get X-rays, we would just . . . have him put under surgery and have all the stuff you need to fix because they could tell what he needed roughly. So, basically, his next dental visit was a dental surgery. (Participant No. 5)
These experiences reveal children who use ECI services face unique additional challenges when attending dental services.
Theme 2: Parents as primary navigators of oral health care
Subtheme 2A: Parental burden and mental load when accessing dental care
Parents reported feelings of uncertainty in knowing how to support their child and the clinician during a dental appointment. For example, parents discussed the challenges managing their child’s behavior and stimming that occurred around the time of the dental appointment.
It’s just . . . we don’t know really how to calm him down. Because once he gets in that mood . . . there’s nothing you can do about it. . . . We’re still learning what his likes and dislikes are, but . . . everything is pretty difficult with him. (Participant No. 5)
For some parents, this resulted in feelings of anxiety and futility.
Even I get anxiety taking him to the dentist. Because I know how he would react. . . . I feel like I would just be wasting my time. (Participant No. 11)
They discussed this as an additional factor that affected prioritizing dental care, especially when they anticipated the dental visits to be futile.
It’s just I feel like we’ve got our hands full with them [children] all going through kinder or playgroup, where we don’t have a lot of time to just do stuff. . . . Because at this point we’ve got 2 kids at any given point and on weekends all 3. . . . I don’t see the point in going if they [dental practitioner] don’t know how to break it down and give her positive reinforcement every time she feels comfortable with it. (Participant No. 2)
Children often had additional medical comorbidities, heightening parental concerns of the impact of poor oral health on their child’s general health.
Because she has a heart defect . . . the heart and the teeth are related . . . that’s scary as parents being like could this potentially turn into an infection in her blood? And then we don’t catch it. And then it’s a whole another thing. (Participant No. 6)
However, despite the awareness of the importance of oral health, these additional medical conditions added to the mental load parents experience when navigating dental care for their child.
I think it [booking first dental appointment] just was sort of sitting in our brains that okay, that’s something else we needed to do . . . and you know, thinking about it, because of other health things going on. (Participant No. 3)
Navigating dental services in the face of such complex needs, within a fragmented health care system, compounded by complex referral processes led to delays in care, intensifying the burden on families.
And that’s the other thing that irked me was that it took 6 months to get it done . . . my son was in pain for 6 months . . . it was a significant period of time. . . . You know, from when we took him to when he got his appointment, you know to get fixed up. (Participant No. 5)
As parents navigated these complex needs and priorities within a fragmented health system, some reported incurring substantial cost, due to lack of funding for the dental services that was essential for their child.
It’s . . . six grand, you know what I mean. I would prefer . . . not spend six grand. . . . It’s not cheap. And private health insurance only covers a fraction of it. (Participant No. 5)
In contrast, parents who were able to access subsidized dental treatment did not experience these financial burdens.
I guess because we go through, like, hospital settings, we never really pay for anything. (Participant No. 6)
Parents are less likely to engage with dental services due to anxiety about their children’s capacity to engage and a sense of futility as they juggle many priorities to meet the complex health and developmental needs of children accessing ECI services.
Subtheme 2B: Parents have limited relevant, reliable information and support to facilitate dental care
Parents described a general lack of support in supporting their child’s oral health and navigating dental health care. In particular, parents reported challenges in locating relevant and reliable information to support their child’s oral health needs.
You don’t want to read American sites . . . I think you’re just trying to find that .com.au stuff or .gov.au stuff . . . it’s hard to find the right, accurate [information]. (Participant No. 3)
A lack of practical support and tailored guidance from early childhood health professionals they trust was commonly discussed among parents as a challenge to managing children’s oral health needs, leaving families uncertain about appropriate strategies.
I spoke to our pediatrician a little bit about it [challenges with toothbrushing]. . . . And she just said just keep trying. . . . I can get like about 3 seconds of brushing. (Participant No. 6)
Health professionals’ lack of awareness about dental services and funding schemes also affected access to dental services.
I don’t remember what the scheme is called . . . when I mentioned the scheme to my OT [occupational therapist], she hadn’t heard of this scheme before. (Participant No. 8)
Structural and informational gaps not only delayed care but also undermined support for optimal preventive oral health behaviors, highlighting the urgent need for integrated, person-centered solutions.
Theme 3: Clinicians skills and approach affect dental experience
Parents recognized the central role of the clinician in shaping their child’s experiences with dental services.
Subtheme 3A: The impact of clinicians’ skills and empathy
Some of the negative experiences shared by parents highlighted their perceptions that the clinician’s approach lacked empathy and failed to consider the support needs of children.
They don’t understand how to help calm her down, or understand how to break down her fear. They don’t know how to break down into stages. They just tried pinning her down and looking at her teeth. And she wriggles and squirms and gets extremely upset to the point where it’s completely useless. (Participant No. 2)
The clinician’s inability to accommodate the needs of their child was perceived to be due to lack of expertise or skills.
I think. . . someone with [child]’s level of autism is a little bit outside of their expertise. . . . They say they do, but . . . I didn’t really see any benefit to their expertise. (Participant No. 5)
In contrast, parents who reported positive experiences attributed these to the expertise of the clinician. The clinician’s ability to make adjustments in interactions and personalize approaches were felt to reflect additional expertise.
“[Child] also has an ASD diagnosis . . . but I’m sure they’d had experience with that. Like they were very comfortable allowing me to sit wherever I wanted. I think even the first time [child] sat on me. (Participant No. 3)
Subtheme 3B. Communicating complex concepts between clinicians and parents to accommodate the individual needs of each child
There was variability in the ways parents communicated about children’s unique needs. Some parents communicated their child’s needs with dental clinicians to facilitate clinicians’ preparation and ability to provide dental treatment.
I just wanted to make sure that they kind of know what to expect with [child]. (Participant No. 11)
Some parents expressed uncertainty about what information may be relevant to the dental setting.
I tend to sort of mention like everything because I don’t know how it relates, especially to dental. (Participant No. 3)
Some parents who did not disclose their child’s developmental concerns, delay, and/or disability described a general lack of adaptability for children in dental clinics.
There was no adaptability for children that might need that—there’s bright lights—it’s just like what an adult would go through if they went to the dentist. I don’t disclose that he’s on the spectrum beforehand, so they don’t know. (Participant No. 4)
Parents also provided examples in which clinicians’ communication was dismissive of parents’ concerns and viewed catering to their child’s additional needs as an inconvenience.
It felt like a little bit of an inconvenience. . . . It seemed like she was just trying to push us out . . . waste of time kind of thing. (Participant No. 6)
Parents perceived that experienced, skilled clinicians were empathetic and communicated well, but negative experiences were often associated with a lack of such attributes and expertise.
Opportunities to Improve Dental Care as Part of ECIs
Three key themes relating to opportunities to improve dental care were identified: (1) the value of clinicians working with parents to alleviate parental burden and support children while providing dental care, (2) acknowledging and mitigating barriers within the dental clinic, and (3) the importance of interprofessional collaboration to deliver early, practical, and tailored guidance.
Theme 1: The value of clinicians working with parents to alleviate parental burden and support children while providing dental care
Parents had clear expectations of what would improve dental experiences for their children. For example, parents described how clinicians could better interact with their child, rather than focusing only on parental interactions.
I think that a dentist should probably approach a child . . . get on their level and be like “hi what’s your name” kind of thing, as opposed to talking about the child to the parent and not acknowledging the child. (Participant No. 4)
Parents valued the opportunity for familiarization and positive reinforcement as a manner of fostering better experiences for their child.
It would be good just to get her into a room on a regular basis with absolutely no instruments . . . get her to sit on the chair a few times with positive reinforcement. Get her to look at the tools and maybe turn them on without them going near her mouth. (Participant No. 2)
Likewise, parents valued the tailored, empathetic oral health advice provided by oral health professionals, viewing it as an integral component of person-centered care.
We were trying to brush her teeth . . . it’s not like she drinks juice out of a bottle or anything. But just like having those conversations with the parents . . . to try and figure out why this is happening with this child . . . just being more personal, more playful, and maybe not so task-minded. (Participant No. 6)
Parents discussed the importance of approaches that prioritized familiarization and empathetic communication to both parents and children throughout the dental care process.
Theme 2: Acknowledging and mitigating barriers within the dental clinic
Parents discussed barriers within the dental clinic that could be addressed to facilitate effective dental care. Many parents highlighted that dental clinics were not only sensory unfriendly but were often designed for adults, highlighting a lack of consideration for the needs of children in general dental settings.
It was like just a general chair; that adult thing. There was no adaptability for children [at a general dental clinic] . . . like, there’s bright lights . . . it’s just like what an adult would go through. (Participant No. 3)
Parents contrasted these experiences with other health care experiences to demonstrate opportunities to address this in the dental setting.
There’s nothing for a child to feel comfortable . . . when we get her hip ultrasounds or a blood test, there’s teddys, and there’s pictures, and there’s a TV screen . . . all these things going on that kind of distract her from what’s happening. (Participant No. 6)
Parents suggest that designing dental clinics to suit children’s needs, or even simple adjustments to the physical environment, may reduce barriers to care for their children.
Theme 3: The importance of interprofessional collaboration to deliver early, practical, and tailored guidance
With limited information and early childhood health professional support available, parents reported a need for clear oral health guidance tailored to children with developmental concerns and disability, offering a key opportunity for further support in this area.
. . . that would be like amazing . . . having like a website, or something where you could go and, you know, see all the different ways that you can brush teeth or encourage brushing teeth. . . . I guess they could also include things about how to lessen the anxiety around brushing teeth or the sensory overload. (Participant No. 6)
Parents highlighted the potential role of other health professionals in supporting oral health, noting that the absence of early and proactive guidance often left them feeling frustrated and uninformed about how use dental services.
. . . you never get any information about that [general dental information] anywhere like I didn’t know, like, what age I have to take them for their first dental visit . . . with my daughter. We only went when she started having problems. . . . So, I wasn’t really aware of how I’m supposed to look after my children’s teeth. . . . I suppose it [general dental well-being] could go through maternal nurse, something. GP [general practitioner] or whatever. . . . Like, no one talked to me about it. (Participant No. 11)
Some parents shared their expectation that health professionals across different sectors should work more collaboratively to share reliable dental information and provide educational support.
Potentially, like more education through like maternal child health nurses . . . ours touched on it [dental care] a little bit. (Participant No. 6)
Some provided examples where this had been beneficial to them. In many of these cases, promoting a more integrated health message was crucial to parents feeling empowered to assist with meeting their child’s needs.
Yeah, well, we were pretty lucky . . . a dental person came to speak to our groups. So, she actually came, yeah, a dental person came to speak to us then. (Participant No. 3)
As children accessing ECI engage with a range of health professionals, improving interprofessional collaboration between these various professionals and dental services could greatly improve child and family experiences.
Discussion
This qualitative study explored the dental experiences of parents of young children accessing ECI services. It reinforces the importance of previously reported barriers to person-centered dental care, such as the cost and expertise of clinicians. In addition, the study provides additional rich context about the experiences of families, including the burdens that are carried by parents as they seek to support their children with high support needs. Challenges are exacerbated in the dental context because the health professionals involved in their child’s care are often unfamiliar with oral health and dental services, and health promotion resources are not tailored.
Consistent with the existing literature, parents reported concerns about the training and experience of oral health professionals. In particular, parents were disappointed by the lack of accommodations for their child’s needs. This was expressed in 2 ways: (1) parents providing examples of what they felt were inappropriate interactions with their child and (2) clinicians failing to meet parental expectations that they would provide opportunities for familiarization and desensitizations to the dental environment. Underpinning this was the fact that anxiety and distress were recurrent elements experienced by not only the children but also the whole family unit when engaging with dental care. Dental anxiety is highly prevalent among individuals with developmental concerns, ASD, and/or intellectual disability (Sahab 2017). This anxiety frequently leads to the avoidance of much-needed dental care, affecting oral health outcomes (Sahab 2017).
The findings are consistent with existing research that shows that the typical dental environment can be overwhelming for children with sensory sensitivities. This often triggers anxiety and avoidance behaviors (Sahab 2017). While often inferred, the study extends these to reveal the impact of negative dental experiences on parents and their willingness to take their children back for dental care. Of concern, it was common that parental distress and helplessness were exacerbated by the feeling of not being able to help regulate their child in preparation for the appointment and the perceived lack of acknowledgment or understanding of support needs. It is this sense of futility that understandably affected their utilization of dental services, especially given the competing demands experienced in families with a child with a disability—another challenge that was also highlighted in our study.
While the existing literature emphasizes the effectiveness of gradual desensitization and relationship building (Appukuttan 2016), the families in this study felt unsupported in this process. Instead of focusing solely on completing the dental procedure, a more holistic approach that prioritizing familiarizing children with the sights, sounds, and smells of the dental setting, alongside collaborative support with parents, could better address the child’s emotional needs. This approach can often be complicated by problem-based or symptomatic dental visits or previous negative experiences.
Parents’ perceptions of a lack of understanding of sensory needs among dental clinicians highlight the need for more focused training on disability and sensory processing, equipping clinicians with the knowledge and skills to understand and support children with these needs through neuroaffirming and trauma-informed approaches. This gap in training also underscores the need for greater access to specialists with additional expertise. Similar findings have been reported previously, with lack of training and experience consistently described as key barriers to providing quality oral health care for children with developmental delay and/or disability (Lim et al 2020; Lim et al 2021b; Lim et al 2022).
However, while parents in this study largely interpreted the lack of utilization of anticipated adaptations as a lack of training among oral health professionals, it is important to recognize that this study did not explore the views of clinicians. As with many areas of health service provision for people with disability, the research in this area is limited. This is despite the existing literature highlighting clinician-related barriers as a significant concern in delivery of dental care for patients with additional health care needs (Lim et al 2021a; Lim et al 2021b). A perceived lack of training and experience for clinicians has been reported to be a common barrier for providing dental care for patients with disability, with the main contributor being perceived lack of training and experience. However, other factors that have been described include lack of access to facilities and modalities that would enable them to adapt the care of patients and the restrictive nature of funding models (Lim et al 2021a).
Funding schemes for health services that recognize the additional resources needed to provide holistic, prevention-focused care for children with additional needs may assist with alleviating these pressures. Fee-for-service models that do not sufficiently value preventive care (eg, by limiting the number of dental checkups per year), or other adaptations required to achieve this, may be additional contributory factors. The findings of this study suggest that further research is needed to explore how parents’ expectations for their child’s dental care align with the enablers and barriers experienced by clinicians. Such research may be critical to addressing the challenges that limit the utilization of dental care for children with disabilities.
An interesting observation from this study was parents’ uncertainty about sharing their child’s diagnoses or additional needs with clinicians. Some participants did highlight that they were unaware of the detail required by dental professionals and what would affect care. However, some parents expected clinicians to be able to recognize and adapt to the needs of their child. While one aspect of this may be a reflection on health literacy and a need for wider discussion about why dental practitioners benefit from having comprehensive histories to inform approaches to dental care, it also raises concerns about whether risk of discrimination or the perception that their child would receive “less” care than another child without additional needs influenced this decision. This is a factor that should be explored in future research to ensure that perceived bias or discrimination are not contributing to the engagement of parents of children with disability with health services.
In relation to health literacy, a clear theme that was developed was the desire among parents to have access to better information about oral health and dental care to feel more empowered to address or advocate for their child’s needs. The lack of easily available resources for families with children with disability to guide their understanding of oral health, approaches to oral hygiene, and access to dental care are a significant deficiency in assisting families. Where resources are available, these need to be publicized to families of children with disability and the health care and disability workers that form part of their wider support networks to help ensure parents are able to access these supports.
Support networks, including trusted primary care practitioners, such as maternal child health nurses, general practitioners, allied health personnel and specialists such as pediatricians, may lack understanding of oral health, have limited awareness of the available dental services, and are unable to guide families effectively. This was a finding of this study, with families having quite different experiences depending on how much support they were offered. It highlights the important role of integrated ECI services in providing a model for how access to additional dental supports might be facilitated. Likewise, it demonstrates the value of investment in disability liaisons more widely in the health care sector. Given the fragmented nature of a health system that separates dental services from other health services, incorporating oral health professionals or establishing referral pathways to dental specialists through existing multidisciplinary teams could help to address the gaps in knowledge and access currently experienced by families of children with developmental delay and/or disabilities. The findings and the successful use of key workers in the study design of this project highlight the value of collaborative models of care between the oral health and disability/early childhood sectors, rather than just the reliance of families on the need to advocate for their children and their needs.
The cost of dental treatment, which is a regularly reported consideration in the Australian context (Lopez Silva et al 2021), was again reported by some parents. This demonstrates a concerning systemic barrier in the health care system for children with developmental delay and/or disabilities, who have a greater need for specialized services. Funding for such specialized services and general anesthesia is limited; while almost half of Australian children access dental services privately (Australian Institute of Health and Welfare 2023), government subsidies, such as the Child Dental Benefits Scheme, do not extend to general anesthesia (Stormon et al 2022).
This study focused on a metropolitan area of Melbourne with a relatively low area-level disadvantage, and this may limit the transferability of the findings to other families, especially where access to specialized dental care and support networks might be more restricted. In addition, the involvement of a key worker in the recruitment process could introduce selection bias as the key worker might be more likely to approach families whom they perceive as having greater oral health needs or being more receptive to participating in research.
A further limitation of this study in influencing the required changes may have been the qualitative methodology. The paucity of the available literature and data in relation to the oral health of Australian children with disability is of concern and needs to be addressed in light of the findings of this study. However, the absence of mechanisms to effectively report these disparities at the population level will mean that it will take time to demonstrate the link between poorer utilization of dental services in this population with health outcomes. In light of this, amplifying the lived experience of these families, in the absence of other data, is the true strength of this study in helping inform the urgent needs that must be addressed at several levels: the clinician, the wider dental environment, and awareness and information more widely across the health sector. Likewise, it is important to acknowledge that smaller studies such as this one have the potential to uncover nuanced challenges and localized solutions that might be overlooked in larger, more generalized research. The overall findings of this study are pivotal as they call for health system reform that emphasizes person-centered communication, fosters co-designed care plans, and acknowledges the spectrum of sensory experiences that affect dental care.
Future research should prioritize a broader geographical scope, including rural communities along with the integration of service provider viewpoints, to identify potential points of collaboration and address capacity-building needs. Longitudinal studies, with the ability to identify people with disability, would be the ideal mechanism to track the effectiveness of implementing tailored resources, interdisciplinary care models, and disability-competent training for dental professionals. However, to develop truly inclusive interventions, future research should prioritize the direct involvement of individuals with developmental delay and/or disabilities. This approach will ensure a deeper understanding of their specific needs and preferences and ensure true patient-centered care.
Conclusion and Recommendations
This study highlights a health care system that often fails to understand and meet the dental needs of families with children who have developmental delay and/or disabilities. It is evident from this lived experience shared by participants that anxiety and distress due to lack of personalized settings and services, and compounded by previous negative experiences, are large contributing factors to the use of dental services for children with disability. The emphasis on empathetic care highlights the need to prioritize the child and family’s psychological well-being and include collaborative parent–provider partnerships alongside enhanced disability competency for dental professionals. The findings also emphasize the need for tailored resources, integrated care models, accessible specialist services with appropriate financial support, sensory-friendly environments, and disability-competent dental care. Parents’ calls for more accessible dental information and proactive education and support from allied health professionals underscore the limitations of the current “one-size-fits-all” approaches and the need for personalized approaches to address the use of dental services by children with developmental delay and/or disabilities.
Author Contributions
T. Kangutkar, contributed to analysis and interpretation, drafted and critically revised the manuscript; A.N. Fernando, contributed to data collection (conducted interviews), analysis, interpretation and critically revised the manuscript; O. Walsh, contributed to conception and design, data collection (conducted interviews), analysis, interpretation and critically revised the manuscript; M. Lim, K. Milner, contributed to data analysis, interpretation and critically revised the manuscript; J. Thorpe, M. Silva, contributed to conception and design, data collection, analysis interpretation and critically revised the manuscript. All authors gave their final approval and agree to be accountable for all aspects of work.
Footnotes
Appendix
Interview Guide.
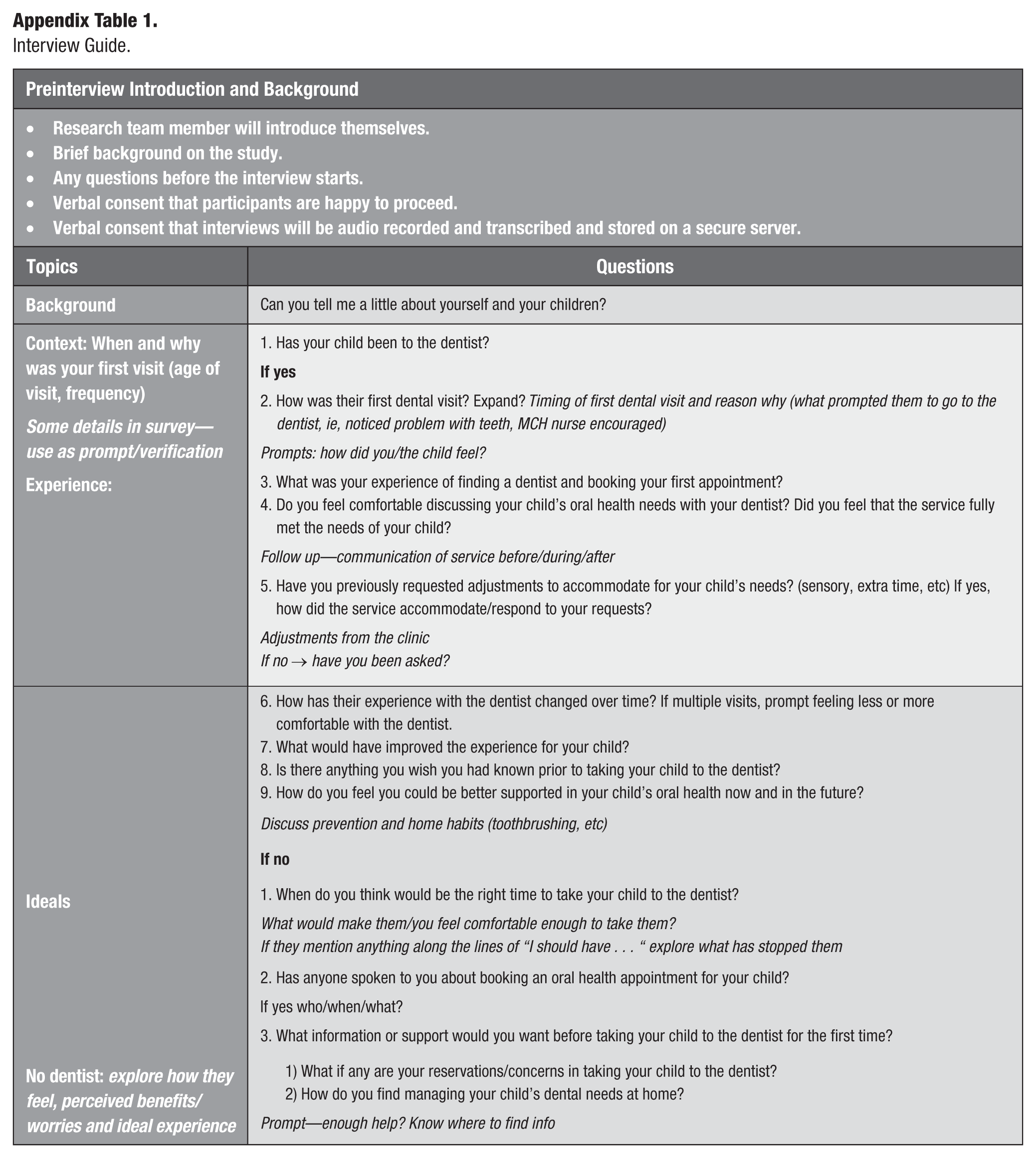
| Preinterview Introduction and Background | |
|---|---|
| • Research team member will introduce themselves. • Brief background on the study. • Any questions before the interview starts. • Verbal consent that participants are happy to proceed. • Verbal consent that interviews will be audio recorded and transcribed and stored on a secure server. |
|
| Topics | Questions |
| Background | Can you tell me a little about yourself and your children? |
| Context: When and why was your first visit (age of visit, frequency) Some details in survey—use as prompt/verification Experience: |
1. Has your child been to the dentist? 2. How was their first dental visit? Expand? Timing of first dental visit and reason why (what prompted them to go to the dentist, ie, noticed problem with teeth, MCH nurse encouraged) Prompts: how did you/the child feel? 3. What was your experience of finding a dentist and booking your first appointment? 4. Do you feel comfortable discussing your child’s oral health needs with your dentist? Did you feel that the service fully met the needs of your child? Follow up—communication of service before/during/after 5. Have you previously requested adjustments to accommodate for your child’s needs? (sensory, extra time, etc) If yes, how did the service accommodate/respond to your requests? Adjustments from the clinic If no → have you been asked? |
| Ideals No dentist: explore how they feel, perceived benefits/worries and ideal experience |
6. How has their experience with the dentist changed over time? If multiple visits, prompt feeling less or more comfortable with the dentist. 7. What would have improved the experience for your child? 8. Is there anything you wish you had known prior to taking your child to the dentist? 9. How do you feel you could be better supported in your child’s oral health now and in the future? Discuss prevention and home habits (toothbrushing, etc) 1. When do you think would be the right time to take your child to the dentist? What would make them/you feel comfortable enough to take them? If they mention anything along the lines of “I should have . . . “ explore what has stopped them 2. Has anyone spoken to you about booking an oral health appointment for your child? If yes who/when/what? 3. What information or support would you want before taking your child to the dentist for the first time? 1) What if any are your reservations/concerns in taking your child to the dentist? 2) How do you find managing your child’s dental needs at home? Prompt—enough help? Know where to find info |
Acknowledgements
We acknowledge the consumer representatives who contributed to this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Victorian Government and Department of Health Public Oral Health Innovation grant. O. Walsh was funded by the MRFF-PPHR Initiative – 2020 Maternal First 2000 Days and Childhood Health grant. M. Silva was funded by a Melbourne Children’s Clinician-Scientist Fellowship.