
Abstract
Objectives:
This study examines the relationship between prior incarceration and dental insurance trajectories throughout older adulthood.
Methods:
A nationally representative sample of adults aged 55 y and older who participated in the 2012–2020 Health and Retirement Survey was analyzed (n = 6,383). Group-based trajectory modeling was used to identify distinct patterns of dental insurance coverage across the 8 survey waves. Multinomial logistic regression was used to assess the association between prior incarceration and dental insurance trajectory group membership.
Results:
Four dental insurance trajectories were identified: persistent dental insurance (30.0%), intermittent high insurance (16.4%), intermittent low insurance (20.4%), and no insurance (33.3%). Bivariate analyses revealed that formerly incarcerated older adults were significantly more likely to be in the intermittent low dental insurance (relative risk ratio [RRR] = 2.31, 95% confidence interval [CI] = 1.67–3.20) and no dental insurance (RRR = 1.51, 95% CI = 1.09–2.11) groups relative to the persistent dental insurance group. Covariate-adjusted models that accounted for sociodemographic, health, and economic covariates found a significant association between prior incarceration and membership in the intermittent low dental insurance group (RRR = 1.48, 95% CI = 1.03–2.11).
Conclusions:
Formerly incarcerated older adults were less likely to have consistent dental insurance coverage over time. Additional research is needed to understand why formerly incarcerated individuals are less likely to have consistent dental insurance over time and what policy and programmatic responses may increase access to dental care coverage for this population.
Knowledge Transfer Statement:
This study shows that formerly incarcerated older adults are more likely to experience periods without dental insurance over time. These findings can inform efforts by dental care providers, policymakers, and community health programs to improve dental care access by expanding insurance coverage and tailoring oral health services to meet the needs of individuals with incarceration histories.
Introduction
Regular dental care is essential for maintaining both oral and overall health (National Institute of Dental and Craniofacial Research 2021; Borrell et al. 2023). Preventive oral health care is particularly important in older adulthood given the elevated risk of dental diseases and tooth loss alongside aging (Meyerhoefer et al. 2021). For instance, about 1 in 5 adults aged 65 y and older experience untreated cavities (Dye et al. 2015), nearly 7 in 10 are affected by periodontal disease (Eke et al. 2015), and most cases of oral and pharyngeal cancers occur in older adulthood. (Silverman 2001; Hashim et al. 2019). Even so, approximately one-third of adults aged 65 y and older report not visiting a dental provider in the past year (Kramarow 2019), and studies find that not having dental insurance is a key barrier to accessing dental care services for older adults (Manski et al. 2010; Vujicic et al. 2016; Willink et al. 2016; Kramarow 2019). Notably, national statistics show that dental insurance coverage declines alongside age, with 52.2% of adults aged 18 to 64 y reporting having dental insurance (Blackwell et al. 2019), compared with 34.3% for those aged 65 to 74 y, 22.3% for those aged 75 to 84 y, and 19.9% for those aged 85 y and older (Kramarow 2019). Accordingly, understanding the factors associated with dental insurance patterns across older adulthood holds important implications for improving dental care use and oral health across the life course.
Increasingly, research has highlighted the role of incarceration as a critical driver of health inequities (Wildeman and Wang 2017; Novisky et al. 2025) and a factor that has adverse effects on dental care access and oral health over the life course (Kulkarni et al. 2010; Testa and Fahmy 2020; Talbert and Macy 2022; Testa and Fahmy 2022; Testa, Mungia, Lee, et al. 2024; Zhao et al. 2024). In particular, recent studies have also documented the consequences of incarceration for dental care use (Testa, Jackson, et al. 2024; Testa et al. 2025) and increased risk of edentulism (Testa, Mungia, Neumann, et al. 2024) among older adults. Notably, research also finds that the relationship between prior incarceration and lower dental care use is explained by not having dental insurance and lower socioeconomic status (Testa and Fahmy 2020; Testa, Jackson, et al. 2024). The impact of incarceration on later-life oral health disparities is of critical importance, considering the United States has the highest incarceration rate in the world (Fair and Walmsley 2021) and has experienced rapid growth of older incarcerated adults over time (Williams et al. 2012), resulting in an estimated 1 in 15 older adults who have been previously incarcerated (Garcia-Grossman et al. 2023).
Studies among adult populations from earlier in the life course show that a history of incarceration is associated with a lower likelihood of health insurance in general, despite formerly incarcerated individuals having greater health care needs (Testa and Porter 2023; Zhao et al. 2023). Even so, there is limited research examining how incarceration influences patterns of dental insurance status, especially across older adulthood. The insurance disparities among formerly incarcerated populations may be even greater in the case of dental insurance, which is not considered an essential benefit under public health insurance plans that formerly incarcerated persons often rely upon, including Medicare and Medicaid (Jolin et al. 2024).
Using data from a nationally representative sample of older adults in the Health and Retirement Study (HRS), the current study investigated the relationship between prior incarceration and trajectories of dental insurance coverage across older adulthood. We hypothesize that older adults with a history of incarceration will be characterized by trajectories of lower and less stable dental insurance throughout older adulthood.
Methods
Data are from the HRS, an ongoing, nationally representative, longitudinal panel study of aging in the United States, funded by the National Institute on Aging and administered by the University of Michigan. The HRS collects biennial data on the health, economic status, and social circumstances of adults aged 50 y and older (Sonnega et al. 2014). In 2012 and 2014, the HRS included questions about incarceration history in a leave-behind questionnaire (LBQ) that participants completed and returned by mail. Half of the sample received the LBQ in 2012, with the remaining half participating in 2014. The 2012 LBQ data included respondents aged 53 y and older, while the 2014 data reflected those aged 55 y and older. To estimate the trajectories of dental insurance, the current study used biennial data from 2012 (the first year of the LBQ) to 2020 (the most recent data available), resulting in a sample size of 6,383 respondents. Details of the selection of the final analytic sample are provided in Appendix A. The study was approved by the University of Texas Health Science Center at Houston Committee for the Protection of Human Subjects (#24-0823). Further details about the HRS data are available at https://hrs.isr.umich.edu.
Measures
Dependent variable
Dental insurance is measured using the 2012, 2014, 2016, 2018, and 2020 HRS surveys from a question asking respondents, “Do you have any insurance that covers your dental bills?” (yes or no) (Manski et al. 2010).
Independent variable
Prior incarceration is measured in the 2012 and 2014 LBQ from a question asking, “Have you ever been an inmate in jail, prison, juvenile detention center, or other correctional facility?” (yes or no) (Garcia-Grossman et al. 2023).
Covariates
Models include covariates for sociodemographic characteristics measured using responses from the 2012 HRS, which ensures time ordering that covariates are measured prior to the start of dental insurance trajectories. Covariates include respondent age (55–64, 65–74, 75–84, or 85+ y), self-reported race/ethnicity (Hispanic, non-Hispanic Black, non-Hispanic other race, or non-Hispanic White), biological sex (male or female), marital status (married, widowed/divorced, or never married), educational attainment (less than high school, GED, high school graduate, some college, or college and above), veteran status (yes or no), and whether a respondent had reported having health insurance (uninsured or insured). To account for health-related factors, we include a control variable for self-reported health (excellent, very good, good, fair, or poor) and whether a respondent had reported edentulism (i.e., loss of all upper and lower teeth) (yes or no). Wealth is measured as the net value of all nonhousing financial assets (including stocks, mutual funds, trusts, checking and savings accounts, money market accounts, bonds, and other savings) after subtracting total debts. Based on this measure, respondents are grouped into quartiles, with higher quartiles representing greater wealth (i.e., the first quartile represents the lowest 25% of wealth within the analytic sample, while the fourth quartile represents the highest 25%).
Statistical Analysis
Group-based trajectory models (GBTMs) were estimated to identify distinct latent patterns of dental insurance throughout older adulthood. The GBTM is a semiparametric longitudinal latent-class method that determines whether clusters of individuals follow similar patterns over time of a behavior of interest (i.e., having dental insurance). Specifically, GBTM examines heterogeneity in longitudinal behavioral patterns and probabilistically assigns individuals to mutually exclusive groups based on their observed data (Nagin 2005). In the current study, GBTM models were estimated using the “traj” package in Stata version 18 (Jones and Nagin 2013).
Given that the dental insurance was a binary measure, we used a logistic link function to estimate the probability of dental insurance use at each time point, covering ages 55 to 90 in the 2012–2020 HRS (ages were top coded at 90 to ensure adequate cell sizes for analysis). To select the optimal number of trajectory groups, we began by estimating a 2-group model and added additional groups until the model fit no longer improved. As each additional group was added, we assessed model fit using the Bayesian information criterion and the transformed Bayes factor to determine the optimal number of trajectory groups. After selecting the optimal number of trajectory groups, we then altered the functional form of each trajectory (e.g., constant, linear, quadratic, or cubic) to identify the model that best represents the underlying data (Nagin et al. 2024). The final model selection considered statistical fit and practical factors such as parsimony and ensuring each group had a sufficient sample size (Nagin 2005). Given the age of the HRS sample, trajectories were estimated using an extension of GBTM to account for nonrandom attrition (see Appendix B) (Haviland et al. 2011).
Following the estimation of the trajectory models, each respondent was assigned to the trajectory group for which they had the highest probability of membership. After classifying respondents to a given trajectory group, we used multinomial logistic regression to examine the relationship between prior incarceration and dental insurance trajectory group membership in both bivariate and covariate-adjusted models. Analyses were adjusted for survey weights (llbwgtr), clustering (raehsamp), and stratum (raestrat) information using the syv command in Stata.
Results
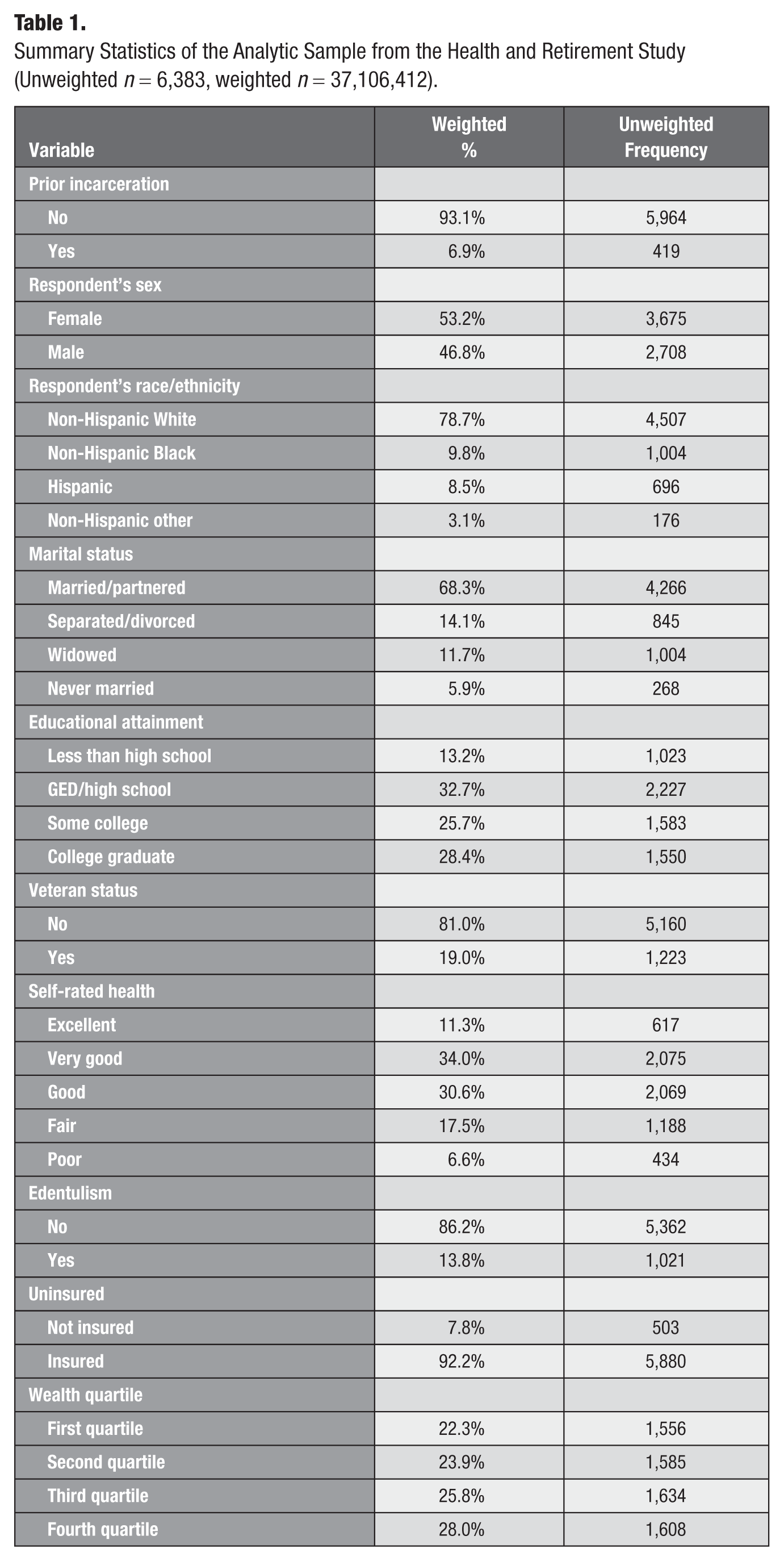
Table 1 provides the weighted percentages and unweighted frequencies for the analytic sample. Overall, 6.9% of respondents (n = 419) reported prior incarceration. The sample composition was 46.8% (n = 2,708) male, 78.7% non-Hispanic White (n = 4,507), 9.8% non-Hispanic Black (n = 1,004), 8.5% Hispanic (n = 696), and 3.1% non-Hispanic other race (n = 176). Summary statistics of the sample stratified by the 4 dental insurance trajectory groups are provided in Appendix C.
Summary Statistics of the Analytic Sample from the Health and Retirement Study (Unweighted n = 6,383, weighted n = 37,106,412).
The Figure shows the results from the GBTM models of dental insurance trajectories. The optimal model identified was a 4-group solution comprising 2 cubic categories and 2 constant categories. Details of the model fit provided in Appendix D indicate that all groups had an average posterior probability exceeding the recommended threshold of 0.70, and the odds of correct classification recommended value of 5 (Nagin 2005). While these groups represent latent constructs, descriptive labels were assigned to facilitate the interpretation of the results.
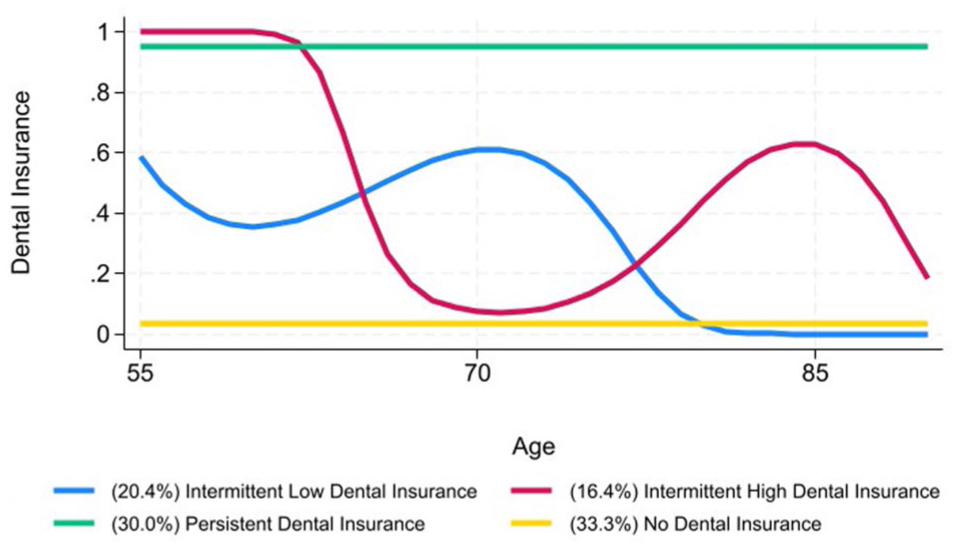
Results of the group-based trajectory model of dental insurance in the 2012-2020 Health and Retirement Study survey (N = 6,383).
The Figure provides the results of the GBTM analysis of dental insurance trajectories. The largest group, no dental insurance, includes 33.3% of the sample and is characterized by individuals who do not have dental insurance throughout older adulthood. Next, persistent dental insurance includes 30.0% of the sample and includes respondents who consistently have dental insurance throughout the observation period. The intermittent low dental insurance group includes 20.4% of the sample and is characterized by individuals with a lower probability of dental insurance, which fluctuates between 0.40 and 0.60 between ages 55 and 75 y and then declines and reaches a probability of zero by approximately age 80 y. Finally, the intermittent high dental insurance group includes 16.4% of the sample and contains respondents who consistently have dental insurance from ages 55 to 62 y, with the probability of having dental insurance steeply declining to approximately zero by age 70 y. This pattern likely represents the loss of dental insurance as many individuals exit the workforce in their early to mid-60s. However, dental insurance levels start increasing again in the mid-70s until approximately age 85, when they sharply decline.
Table 2 presents the multinomial logistic regression analysis estimating the association between prior incarceration and dental insurance trajectories. Across all models, “persistent dental insurance” is set as the reference category. The bivariate results in panel A show that formerly incarcerated individuals have a significantly higher relative risk of membership in the intermittent low dental insurance (relative risk ratio [RRR] = 2.31, 95% confidence interval [CI] = 1.67–3.20) and no dental insurance (RRR = 1.51, 95% CI = 1.09–2.11) groups relative to the persistent dental insurance group. After adjusting for covariates in panel B, the results show a statistically significant association between prior incarceration and membership in the intermittent low dental insurance trajectory remains (RRR = 1.48, 95% CI = 1.03–2.11).
Multinomial Logistic Regression of Dental Insurance Trajectories on Prior Incarceration (Unweighted n = 6,383, Weighted n = 37,106,412).
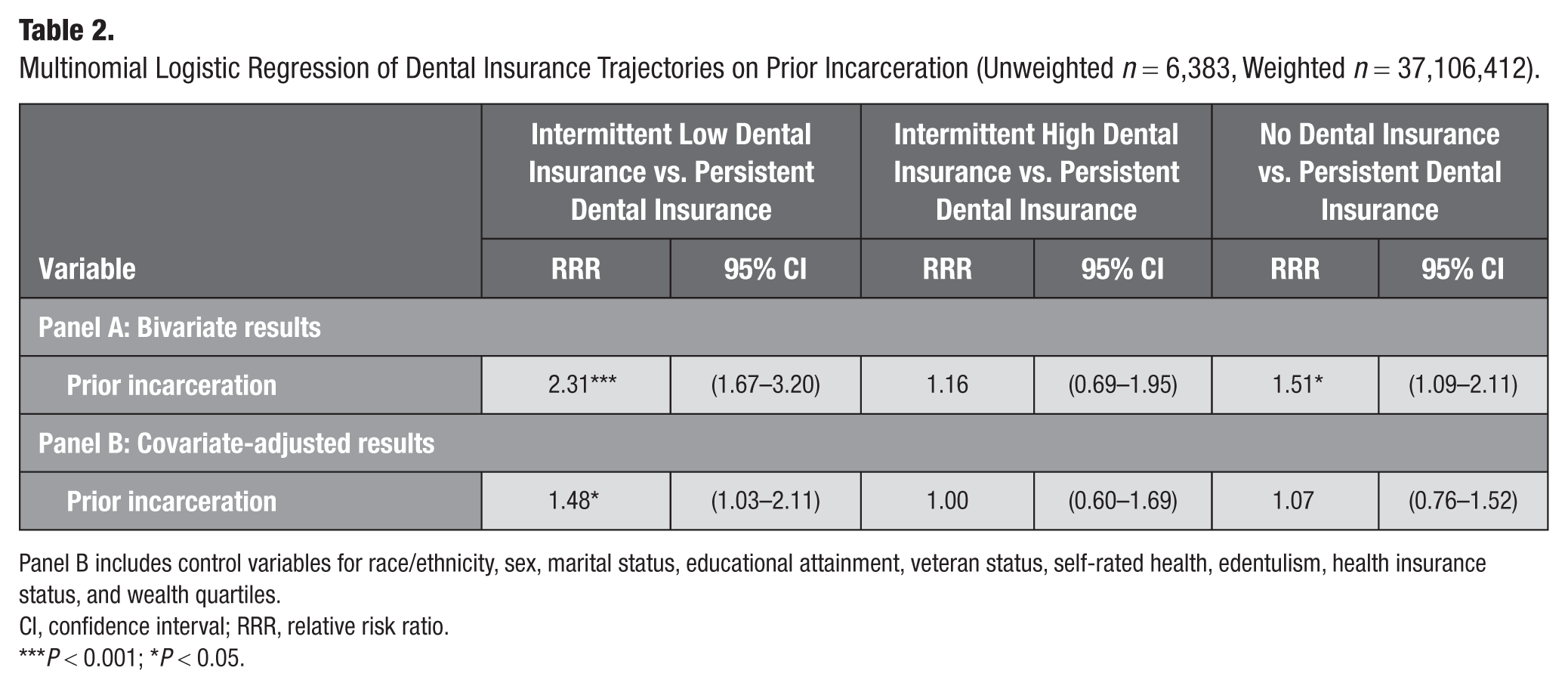
Panel B includes control variables for race/ethnicity, sex, marital status, educational attainment, veteran status, self-rated health, edentulism, health insurance status, and wealth quartiles.
CI, confidence interval; RRR, relative risk ratio.
P < 0.001; *P < 0.05.
Supplementary Analyses
Supplemental analyses were conducted using a question on the duration of incarceration, which asked respondents: “In your entire life, how much time in total have you been detained in a jail, prison, juvenile detention center, or other correctional facility?” (less than 1 mo, less than 1 y, between 1 and 5 y, more than 5 y). The responses were grouped into 3 categories: (a) never incarcerated, (b) less than 1 mo, and (c) more than 1 mo (Garcia-Grossman et al. 2023). The results reported in Appendix E show, in a bivariate analysis, that incarceration durations of less than 1 mo (RRR = 1.89, 95% CI = 1.24–2.88) and greater than 1 mo (RRR = 3.29, 95% CI = 2.02–5.38) are associated with a higher relative risk of membership in the intermittent low dental insurance group compared with the persistent dental insurance group. In addition, more than 1 mo of incarceration duration is associated with a higher relative risk of membership in the no dental insurance group than the persistent dental insurance group (RRR = 1.97, 95% CI = 1.23–3.14). After including covariates, the results show no significant associations between length of incarceration and dental care use trajectories. In part, the non–statistically significant associations in these models may be due to small cell sizes and greater statistical error across the incarceration length categories compared with the binary measure.
Discussion
To the authors’ knowledge, this study is the first to examine the relationship between prior incarceration and dental insurance status throughout older adulthood. The findings yielded the following conclusions. First, the GBTM model demonstrated that dental insurance patterns across older adulthood followed 4 distinct trajectories. About one-third of the sample consistently reported not having dental insurance throughout older adulthood; approximately one-third maintained consistent dental insurance over time. The remaining participants exhibited fluctuating trajectories, alternating between periods of having dental insurance coverage and periods of noncoverage.
Second, the findings from the multinomial logistic regression model showed that individuals with a history of incarceration were more likely to exhibit trajectories characterized by intermittent low dental insurance. These findings are consistent with prior research that has found that formerly incarcerated individuals are less likely to have health insurance compared with those without a history of incarceration (Testa and Porter 2023; Zhao et al. 2023). However, these findings extend the prior literature by providing the first estimates to our knowledge that focus explicitly on the relationship between prior incarceration and dental insurance status.
Taken together, that older, formerly incarcerated adults have lower and less stable dental insurance over time is important, considering that prior studies have found that older, formerly incarcerated adults are at a higher risk for endentulism (Testa, Mungia, Neumann, et al. 2024) and that the association between prior incarceration and lower dental care use is, in part, due to not having insurance (Testa and Fahmy 2020; Testa, Jackson, et al. 2024). Accordingly, these findings from the extant research suggest that increasing dental insurance coverage may be a means to improve dental care uptake, and in turn oral health, among formerly incarcerated persons.
The findings also have implications for policy and practice to increase dental insurance among formerly incarcerated persons. One potential avenue may be through expanding public insurance benefits to include more comprehensive dental insurance coverage. Currently, Medicare does not provide benefits for routine dental coverage (Simon and Giannobile 2021). Indeed, as of 2019, approximately 47% of Medicare beneficiaries did not have dental insurance (Freed et al. 2021). Notably, Medicare beneficiaries who obtained dental services paid an average of $874 out of pocket, with 1 in 5 spending more than $1,000 annually (Freed et al. 2021). Medicare reforms to include dental care coverage thus hold the potential to reduce the financial burden of care, increase coverage rates, and ultimately improve access to dental care for formerly incarcerated persons (Simon and Giannobile 2021). Moreover, studies have also documented that more generous state Medicaid policies are significantly associated with dental care use for low-income older adults (Singhal et al. 2021). These findings align with prior research suggesting that health care reforms, such as those through the Affordable Care Act and Medicaid expansion, have improved dental care use among formerly incarcerated adults (Testa, Mungia, Lee, et al. 2024). Thus, the findings also point to the potential for Medicaid reforms that extend dental benefits for older adults as a potential avenue to increase dental insurance and dental care uptake for this population (Singhal et al. 2021).
In the absence of comprehensive policy changes, Another potential strategy to increase the use of dental care for uninsured formerly incarcerated persons is integrating dental services into transitional clinics that provide low-cost or free health care to formerly incarcerated individuals (Shavit et al. 2017). Of note, in 2024, the Health Resources and Services Administration awarded nearly $52 million to 54 health centers to enhance access to primary care for individuals transitioning from incarceration to the community (Health Resources and Services Administration 2024). However, despite the connection between prior incarceration and oral health conditions such as periodontitis (Testa, Jackson, Gutierrez, et al. 2024) and edentulism (Testa, Mungia, Neumann, et al. 2024), transition clinics focused on providing oral health services were absent from this effort. Moving forward, investments in community transition dental clinics serving formerly incarcerated individuals, including focusing on formerly incarcerated older adults, may be an opportunity for improving access to oral health care for those without dental insurance.
Limitations
This study has limitations that future research could address. First, the measure of prior incarceration in the HRS lacks detailed information, such as the timing of incarceration within the life course and the frequency of incarceration. Second, the measure of dental insurance is also limited, as it does not capture the source of insurance or why respondents lack coverage. Because we cannot observe dental insurance status before entry into the HRS, we cannot determine whether a respondent was without dental insurance before incarceration. Third, the sample in the current study was adults aged 55 y and older (i.e., persons born between 1921 and 1958). Accordingly, the cohort demographic and socioeconomic characteristics differ from those of the broader U.S. adult population. Moving forward, future research should replicate these findings using alternative datasets encompassing a wider range of age groups. Finally, the reliance on self-reported data introduces the potential for recall errors or social desirability bias, which could affect the accuracy of the findings. Future research can replicate the study findings through administrative data that include records of objective information on prior incarceration and dental insurance status among older adults. In addition, future qualitative and mixed methods studies would also be valuable to understand why formerly incarcerated individuals are without dental insurance.
Conclusion
This study advances research on the link between incarceration and dental well-being by providing the first analysis of the relationship between prior incarceration and patterns of dental insurance over time. Considering that formerly incarcerated older adults were less likely to have consistent dental insurance over time, the findings highlight the need for targeted policies and programs improving dental insurance and dental care uptake for formerly incarcerated individuals to reduce oral health inequities within this population.
Author Contributions
A. Testa, contributed to conception and design, data acquisition, drafted and critically revised the manuscript; L. Mijares, contributed to design, critically revised the manuscript; D.B. Jackson, contributed to conception, drafted and critically revised the manuscript; V. Maroufy, contributed to conception, critically revised the manuscript; R. Samper-Ternent, contributed to conception, critically revised the manuscript; A.C. Neumann, contributed to conception, critically revised the manuscript; R. Mungia, contributed to conception, critically revised the manuscript; K.T. Ganson, contributed to conception, critically revised the manuscript; J.M. Nagata, contributed to conception, critically revised the manuscript; T. Oates, contributed to conception, critically revised the manuscript. All authors gave final approval and agree to be accountable for all aspects of the work.
Supplemental Material
sj-docx-1-jct-10.1177_23800844251387559 – Supplemental material for Prior Incarceration and Dental Insurance Trajectories throughout Older Adulthood
Supplemental material, sj-docx-1-jct-10.1177_23800844251387559 for Prior Incarceration and Dental Insurance Trajectories throughout Older Adulthood by A. Testa, L. Mijares, D.B. Jackson, V. Maroufy, R. Samper-Ternent, A.C. Neumann, R. Mungia, K.T. Ganson, J.M. Nagata and T. Oates in JDR Clinical & Translational Research
Supplemental Material
sj-docx-2-jct-10.1177_23800844251387559 – Supplemental material for Prior Incarceration and Dental Insurance Trajectories throughout Older Adulthood
Supplemental material, sj-docx-2-jct-10.1177_23800844251387559 for Prior Incarceration and Dental Insurance Trajectories throughout Older Adulthood by A. Testa, L. Mijares, D.B. Jackson, V. Maroufy, R. Samper-Ternent, A.C. Neumann, R. Mungia, K.T. Ganson, J.M. Nagata and T. Oates in JDR Clinical & Translational Research
Footnotes
Acknowledgements
This research uses data from the Health and Retirement Study, which is sponsored by the National Institute on Aging (NIA; grant NIA U01AG009740) and is conducted by the University of Michigan. No direct support was received from the NIA for this research. Alexander Testa and Luis Mijares had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: A. Testa, D.B. Jackson, V. Maroufy, R. Samper-Ternent, and A. Neumann were supported by the National Institute of Dental and Craniofacial Research via grant R03DE033486.
A supplemental appendix to this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.