
Abstract
Introduction:
The effects of racism, oppression, and colonization in Australia are reflected in the inequitable experience of chronic kidney disease (CKD) among Aboriginal and Torres Strait Islander peoples. Despite having the highest incidence of CKD, Aboriginal and Torres Strait Islander people have the lowest rate of kidney transplant, with poor oral health commonly being an obstacle to receiving a transplant. This research reflects the exploratory phase of a larger project aimed at maximizing oral health outcomes for Aboriginal and Torres Strait Islander people living with CKD in Australia through the provision of culturally secure dental care.
Methods:
The present research uses reflexive thematic analysis to analyze qualitative data from yarns, interviews, and focus groups with dental, renal, and Aboriginal and Torres Strait Islander stakeholders to generate a conceptual understanding of equity at the nexus of oral health and kidney health. NVivo software was used for organizing data and an inductive line-by-line coding approach.
Results:
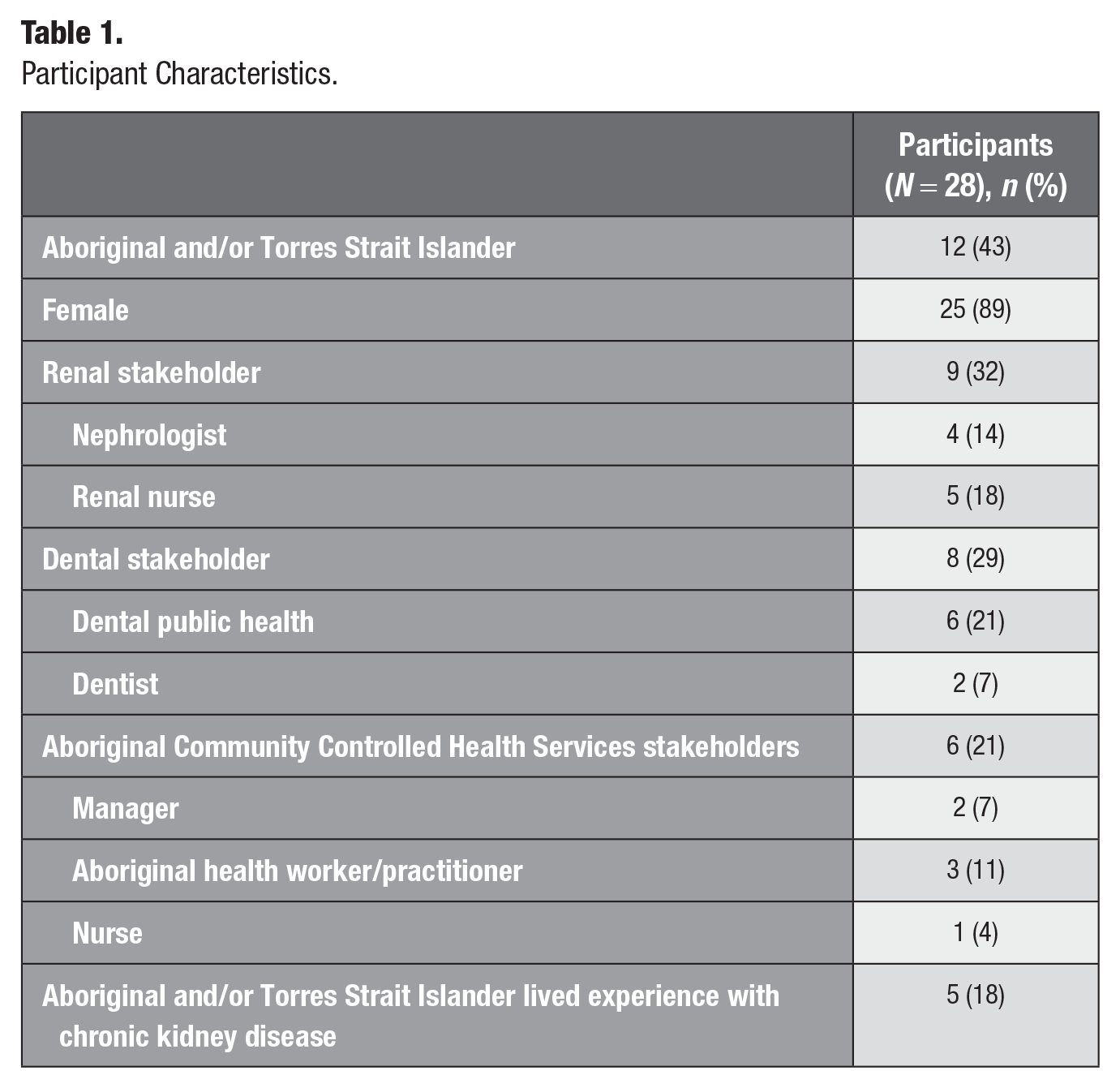
Twenty-eight stakeholders participated; 12 of the stakeholders identified as Aboriginal and/or Torres Strait Islander, and most were female. Factors at the nexus of oral health and CKD included the continuous effects of colonization, the centrality of cultural security for improved care, as well as several challenges and opportunities at a system level. Challenges included the luxury of oral health access, limited health care team involvement in oral health pathways, high-intensity engagement with medical systems, and no communication between dental and renal teams. Opportunities identified included the role of integrated care, cross-discipline knowledge sharing, Aboriginal and Torres Strait Islander leadership, clear referral pathways, prevention, and assistance with navigating the oral health system.
Conclusion:
We argue that collective responsibility for the oral health of Aboriginal and Torres Strait Islander people living with CKD is required for improved health and eligibility for kidney transplant. Cross-discipline collaboration is required to overcome the rigidness of the current colonial and biomedical model that silos oral health and CKD.
Knowledge Transfer Statement:
The siloed approach to management of oral health for Aboriginal and Torres Strait Islander peoples with chronic kidney disease results in low knowledge sharing and communication across chronic disease management teams and can prevent kidney transplantation. Collective responsibility for oral health within this context is required to ensure that just and equitable access to kidney transplant can be achieved.
Introduction
Living with a chronic disease poses unique challenges that require targeted and supportive services. For Aboriginal and Torres Strait Islander peoples in Australia, and indeed Indigenous peoples globally, these challenges are further compounded by the additional effects of racism, oppression, colonization, marginalization, intergenerational trauma, and the sociocultural determinants of health (Hughes et al. 2018; Kelly et al. 2022). Aboriginal and Torres Strait Islander people in Australia often experience the effects of illness, including chronic kidney disease (CKD), more frequently and at younger ages than non-Indigenous Australians (Australian Institute of Health Welfare 2013; Hoy et al. 2016; ANZDATA Registry 2021). Despite experiencing a higher incidence rate of kidney failure, Aboriginal and Torres Strait Islander people are less likely to be wait-listed for a kidney transplant (ANZDATA Registry 2021). This inequitable experience of CKD is directly related to colonialism, which continues to be sustained by current biomedical, social, and political structures (Cundale et al. 2023; Hughes et al. 2023). There has been increasing recognition of and progress toward Aboriginal and Torres Strait Islander community leadership for improved kidney care models that fulfill cultural and clinical needs (Hughes et al. 2018; Kelly et al. 2022; Tunnicliffe et al. 2023). Critically, this leadership must be extended to fields related to the management of CKD, including oral health (Poirier, Hedges, et al. 2023; Poirier, Sethi, et al. 2023).
A bidirectional relationship between CKD and oral health exists (He et al. 2023). In Australia, Aboriginal and Torres Strait Islander people living with CKD have previously exhibited more indicators of poor oral health than the general population (both Aboriginal and Torres Strait Islander and non-Indigenous) (Kapellas et al. 2021). Increased experiences of poor oral health for someone living with CKD are evidenced by changes in an individual’s teeth, bone, oral mucosa, salivary glands, periodontium, and tongue (Wahid et al. 2013; He et al. 2023); these changes have been attributed to metabolic, immunologic, endocrinologic, and uremic imbalances (Souza et al. 2008; He et al. 2023). The ramifications of poor oral health go beyond dental implications for patients, as optimal oral health is a requirement for kidney transplant. Systemic manifestations of oral infective and inflammatory environments can potentially influence the success of transplantation (He et al. 2023). Therefore, poor oral health can delay eligibility for transplantation or, in some cases where care is not available or inaccessible, prevent individuals from receiving a kidney transplant (National Kidney Foundation 2024). Aboriginal and Torres Strait Islander individuals living with kidney failure face unique barriers to maintaining oral health, in addition to a plethora of existing barriers such as racism and access issues (Poirier, Soares, et al. 2023), due to the demanding schedule of dialysis, whereby individuals are required to have 3 to 4 appointments approximately 4 to 6 h in length each week.
Managing the health needs and associated care of CKD, and particularly at the stages of kidney failure, is complex, involving several specialists across different services. In South Australia, dialysis provided through the public sector is typically hospital based, which often forces relocation of Aboriginal and Torres Strait Islander people to urban centers where dialysis facilities are available. This displacement from one’s country, community, culture, and family has significant implications for one’s spiritual, social, and emotional well-being (Conway et al. 2018). As part of the care team, Aboriginal health workers/practitioners (AHW/P) at Aboriginal Community Controlled Health Services (ACCHS) support patients living with CKD through provision of transport to appointments, counseling, and management of other comorbidities (such as type 2 diabetes). Dental services for adults are primarily provided by the private sector in Australia, although a means-tested public dental system is accessible for some individuals. A large proportion of Aboriginal and Torres Strait Islander adults are eligible for public dental services, and disclosure of chronic disease status increases the priority of appointments, thereby reducing most wait times. Unfortunately, the impermanence and availability of services, required copayments, complexities of arranging appointments, and the commonality of experiences of racism create complex challenges for Aboriginal and Torres Strait Islander peoples (Poirier, Hedges, Smithers, et al. 2022). Due to the critical role of oral health in the journey of CKD for Aboriginal and Torres Strait Islander peoples and the complexity of care management in this context, we aimed to gather diverse narratives regarding experiences in accessing and facilitating dental care for Aboriginal and Torres Strait Islander individuals living with CKD to answer our research question: What is the current state of culturally safe oral health services for Aboriginal and Torres Strait Islander people living with CKD in South Australia?
Methods
Decolonizing Methodologies
The work presented herein was framed by decolonizing methodologies and therefore grounded in an awareness of settler colonialism in Australia and struggles for individual and collective sovereignty related to colonial marginalization from dominant culture of Aboriginal and Torres Strait Islander peoples (Corntassel 2012; Tuck and Yang 2012; Laird et al. 2021). In this work, dominant culture is understood to be aligned with biomedical and colonial values and health systems. Due to the colonial forces attempting to limit Aboriginal and Torres Strait Islander sovereignty, strengths and successes in asserting sovereignty were centered and championed among participants, governance, and project team members. In the context of CKD and oral health, this meant challenging statements about limitations of health systems presented as fixated or factual during interviews, sharing stories of successes from other places as realistic alternatives, and continually being guided by leadership and governance groups with lived experiences. By foundationally understanding the structural role of colonialism within biomedical systems, we chose to use the term cultural security rather than cultural safety in this piece to bring attention to the overwhelming demand that structural forces place on the well-being of those living with CKD. As defined by Nyangumarta professor Juli Coffin, cultural security demands system-level changes that formally inform care provision for Aboriginal and Torres Strait Islander peoples, rather than informally informing care (cultural safety) or being positioned as best practice (cultural competency) (Coffin 2007). In approaching this work from a decolonial standpoint, we recognize that we still rely on colonial processes for findings to have translatable impacts, particularly in the chronic disease context. We also recognized Indigenous health research will never be entirely “decolonized,” as research itself is a process built on colonial foundations; however, we contend that there remains an ethical compulsion to create space and drive Aboriginal and Torres Strait Islander–led decolonizing research pursuits (Laird et al. 2021; Hedges et al. 2023).
Positionality Statement
It is critical to acknowledge the assumptions one brings to research due to their inextricable impact on interpretation and analysis of data (Braun and Clarke 2021; Poirier, Haag, et al. 2023). As such, we would like to position our team in relation to the work presented herein. The authorship team is led by a senior Aboriginal researcher and consists of 3 non-Indigenous researchers, including the first author, who have had the privilege and honor of engaging with Indigenous communities across Australia and Canada for more than 10 y in the oral health space. The project was governed by 2 reference groups, one specific to the oral health research and the other composed of Aboriginal and Torres Strait Islander people with lived experience of CKD (Owen et al. 2023). These governance groups ensured that the approach, design, implementation, and evaluation of the project was grounded in Aboriginal and Torres Strait Islander knowledges and decolonial methodologies (Smith 1999).
Study Design
The present data derive from an intervention aimed at improving access, provision, and delivery of culturally secure dental care for Aboriginal and Torres Strait Islander people living with CKD in South Australia. The project took place across 3 regional areas (Whyalla, Ceduna, Coober Pedy) and the Adelaide metropolitan area (Fig. 1). The protocol of the intervention and its methods have been published (Sethi et al. 2022). This project resulted from community consultations and discussions around the unique oral health gaps and challenges for individuals living with CKD. This project was governed by 2 advisory groups, 1 specific to oral health and 1 specific to CKD, both groups comprised entirely of Aboriginal and Torres Strait Islander people with vast experiences in these areas. Governance groups provided leadership over project design, methodological approaches, and evaluations; this included review of qualitative stakeholder guides and quantitative patient questionnaires, analyses, and publications, among other decision making. Both groups were established prior to this project, within their respective research groups, meaning that this project provided an opportunity for inclusive partnerships that have extended beyond the duration of this project, resulting in collaborations and learning opportunities (Anderson et al. 2022; Hedges et al. 2023). Advocacy work born out of the relationships established across governance groups (Poirier, Hedges, and Jamieson 2022) has become more formalized with the establishment of a cross-disciplinary alliance that is working to have a dental team co-located at an Adelaide-based dialysis unit.

Map of South Australia highlighting project sites.
The project was divided into 3 phases: the exploratory phase, intervention phase, and evaluation phase. The primary goal of the exploratory phase was to determine what structures and support services are currently in place to ensure the provision of culturally secure oral health care for Aboriginal and Torres Strait Islander patients with CKD and to identify opportunities to strengthen oral health service provision for these patients. Secondary goals of the exploratory phase included ascertaining the current state of culturally secure oral health services for Aboriginal and Torres Strait Islander people with CKD and potential opportunities to strengthen oral health services for this population (Sethi et al. 2022). Ethical approval for this project was received from the Aboriginal Health Council of South Australia (04-21-936) and the University of Adelaide Human Research Ethics Committee. All participants provided informed written consent. This study is reported in alignment with the Standards for Reporting Qualitative Research guidelines (O’Brien et al. 2014) (Appendix 1).
Sample
Purposive recruitment, or snowball sampling (Fereshteh et al. 2017), was used for the stakeholder discussions during the exploratory phase to identify a diverse sample of stakeholders, given the complexity of chronic disease management. Inclusion criteria for this component of the project included stakeholders who were older than 18 y of age with experience in the navigation, provision, or lived experience of renal and dental care for Aboriginal and Torres Strait Islander people living with CKD. Specifically, Aboriginal and Torres Strait Islander people with lived experience of CKD, representatives from ACCHS, dental services, renal nursing teams, and nephrologists were invited to participate. Participants were initially contacted by the research team via email and were invited to follow up if they were interested in participating.
Method
A combination of yarns, semi-structured interviews, and focus groups was used to accommodate the variation of stakeholders included in this project. Qualitative guides were initially made for oral health stakeholders and Aboriginal and Torres Strait Islander stakeholders and then were tailored per the remaining stakeholder positions (Appendix 2). Where participants held multiple positions (i.e., Aboriginal health worker and lived experience of CKD), multiple sections of the qualitative guide were discussed. Discussions were focused on system-level characteristics of oral health services for Aboriginal and Torres Strait Islander peoples. All discussions included topics related to current oral health pathways, culturally secure provision of care, challenges specific to CKD in relation to oral health, and potential opportunities to strengthen services for Aboriginal and Torres Strait Islander people living with CKD. Discussions took place in ACCHS, hospitals, offices, coffee shops, and via teleconference to accommodate the varying locations and positions of stakeholders.
While understanding that decolonizing methodologies necessitate unsettling the colonial project, which includes Western research (Smith 1999; Tuck and Yang 2012), we recognize the use of semi-structured interviews and focus groups with non-Indigenous stakeholders in this project as a limitation on our uptake of decolonizing methodologies due to constraints of working within the health system of CKD and oral health. Semi-structured interviews used open-ended questions in a systematic way that permits participants to diverge from topics, as appropriate (Irvine et al. 2013). Open-ended questions were followed up with both scripted and unscripted probes to enhance data captured within each interview and focus group (McIntosh and Morse 2015). Interviews were conducted by both an Aboriginal (J.H.) and non-Indigenous researcher (B.P.), oftentimes in tandem, ensuring all participants felt secure during the discussions and that all perspectives were captured. When working with Aboriginal and Torres Strait Islander stakeholders and patients, relational yarning was defaulted to by the lead Aboriginal researcher (J.H.) prior to commencing formal data collection. Relational yarning is a practice termed by the research group that refers to yarns that naturally occur in prioritizing core values of respect, relationships, advocacy, reciprocity, time, and gratitude. These resulting yarns are not necessarily central to the research project aims, but we understand them as essential to relational and ethical processes (Poirier, Hedges, and Jamieson 2022). This approach created a yarning environment where J.H. and participants led discussions and B.P. prompted only if any topic areas from the qualitative guide had not yet been discussed. Yarning is a reciprocal practice that facilitates information sharing and negotiations that aligns with Aboriginal and Torres Strait Islander ways of knowing, being, and doing. Yarning demands 2-way, engaged interactions in which all parties are learners and knowers, reducing power associated with “researcher” and “participant” identities (Bessarab and Ng’Andu 2010; Geia et al. 2013; Barlo et al. 2020).
Analysis
Reflexive thematic analysis was used to analyze stakeholder interview data (Braun and Clarke 2006, 2019, 2021). Reflexive thematic analysis, as outlined by Braun and Clarke, embraces the notion of researcher subjectivity, which enables the organic identification of themes. The primary author (B.P.) has worked in partnership with communities included in this project for more than 3 y and conducted all interviews alongside Aboriginal (J.H.) and non-Indigenous (S.S.) members of the research team. Familiarity with data happened consecutively throughout data collection and prior to beginning analysis; interviews and transcripts were listened to and read over again multiple times. Audio recordings were transcribed verbatim by a local small business, recommended by one governance member. Understandings and assumptions developed during the familiarity process were discussed extensively with the senior Aboriginal researcher (J.H.) prior to initiating analysis. Throughout analysis, discussions with both governance groups were had to tease out some of the concepts being identified, and at the completion of analysis, findings were shared for feedback. An inductive approach to analysis was used, and themes grounded in the data were identified through line-by-line coding with NVivo 12 software (QSR International Pty Ltd. version 12.6.1) and without a structured codebook to provide space for engaged interpretation of data. After coding all transcripts, data were revisited, and similar codes were then aggregated during multiple rounds of iterative thematic development.
Results
In total, 28 stakeholders participated in 15 interviews, 5 yarns, 1 focus group, and 1 yarning circle. Stakeholders belonged to 1 of 4 broad categories, including renal, dental, ACCHOs, and lived experience with CKD. Twelve of the stakeholders identified as Aboriginal and/or Torres Strait Islander, and most were female (Table 1). The continuous effects of colonization were highlighted as a key contextual influence on the oral health experiences for Aboriginal and Torres Strait Islander people living with CKD. Similarly, the centrality of cultural security was deemed necessary for the provision of improved care. Several challenges within the current system were identified, such as the low priority of oral health in the CKD journey as well as a number of opportunities for provision of improved care, including cross-discipline knowledge sharing (Fig. 2).
Participant Characteristics.

Conceptual model of factors at the nexus of oral health and chronic kidney disease for Aboriginal and Torres Strait Islander peoples.
At a structural level, the continuous effects of colonization created confounded complex medical needs. Trauma related to colonial impacts significantly affected health care utilization: I think trauma is a barrier. Things that have happened in the past have created some fear and anxiety around going to the dentist or getting a check-up . . . a lot of discussion happens in community, so if there is a bad experience that is then shared within the community and then that creates a barrier for people who actually need to access the dentist to not access the dentist. (Dental stakeholder)
Factors related to social determinants of health further affected oral health: Even access to toothpaste and toothbrush, SA dental service does a lot of [oral health] promotion, but it’s still difficult and when you’ve got limited budget, and you spend $10, do you buy a toothbrush, or do you buy bread or milk for the family. (ACCHS stakeholder)
Complex priorities also affected the understanding of oral health in relation to overall well-being.
Where health is in the priorities when you’re just trying to make sure you’ve got housing and food, protecting the family, but when it comes to health and you have a raft of comorbidities and other health concerns at the emergency treatment stage, just even understanding the importance of oral health and where it fits within general health is challenging. (Dental stakeholder)
Colonial and biomedical systems constrained the effective co-development of care plans.
We’ve got to talk about colonization. We have to talk the truth about truth in this country. And we have to understand how the health care system was built on systemically racist infrastructure, these systems were set up to exclude First Nation peoples, we were invisible? (CKD lived experience stakeholder)
The pressures of operating within biomedical systems prevented delivery of culturally secure care.
It is almost a disincentive to get interpreters because that process slows you down. You have to wait for an interpreter, and then you have to take time to speak to an interpreter, etc.; it’s all time that we just don’t have in the hospital system. And, as a consequence, we just go on and do the, you know, do all of the tests and give the care as quickly as possible, and often without being able to do those really important things in language, and I think the time is a major barrier. . . . That’s one of our great barriers for being culturally secure we just don’t have the time. (Renal stakeholder)
The expectations on patients to be somewhere at a certain time, as a result of the health care system, can be difficult: Not many of my clients wear watches. I guess your phone has got the time on, but if your phone hasn’t been nicked by one of your grandchildren, actually knowing what the time is. So, if we said, “We can only see you at 10 o’clock,” the idea of you getting there at 10 o’clock may be quite difficult. (Renal stakeholder)
Fundamentally, cultural security was considered the first step for improving the provision and experience of care for Aboriginal and Torres Strait Islander peoples. Cultural security weaves together different ways of understanding well-being, as described by an AHW/P: It’s about bridging those differences and looking for different ways of working so that Aboriginal people feel respected, their cultural values are incorporated into their care. (ACCHS stakeholder)
In action, culturally secure models of care looked like the addition of dialysis chairs at an Aboriginal and Torres Strait Islander medical hostel: It’s at home, you live at home, the language that’s there, you know, being able to walk in and there’s a fire pit and all those kinds of environments, you don’t experience in a clinical setting. So that’s the cultural safe space that we can provide for fellahs that are coming off Country, that don’t have accommodation, and really stabilize their treatment on a dialysis machine so that they can return home. (CKD lived experience stakeholder)
Relationality, knowledge sharing, and listening are crucial for cultural security by addressing some of the power imbalances between health care providers and patients, a deep sense of listening to what people want and need . . . being culturally secure actually takes time. It takes time to sit down and talk to patients, to listen, to allow them to express themselves in their own time in their own way and in their own language. (Renal stakeholder)
Culturally secure care sees each person within the context of their holistic and cultural world: It’s about respecting my values, and cultural attitudes, or cultural understandings. It’s about respecting my family and community. So, it’s being inclusive of family and community not seeing me as an individual on my own, but about how I’m connected. (ACCHS stakeholder)
On an individual level, this translated into how care pathways are provided to patients in a way that best meets their needs and keeps them as healthy and safe as possible, considering the context of their lives, as one AHW/P describes: [Then the] patient’s thinking, “Well, I feel fine. I’m not hooked up [to a dialysis machine]. I’m going” . . . you know, because they’ve got to be home for family or whatever, you know? And I think that lack of understanding because it’s, you know, whereas for us, we . . . our health is not our number one priority, because it’s our family and our community and helping each other. (ACCHS stakeholder)
Importantly, the context of patient’s worlds varies considerably and needs to be respected as such: Instead of having the one blanket goes over all Aboriginal communities, it’s about finding out the specific needs of that community. Because there’s so many cultural protocols and different ways of interacting, and it’s different for each community, and how people interact with each other. (CKD lived experience stakeholder)
Cultural security requires an ongoing journey of unlearning and unsettling for non-Indigenous people, coupled with structural changes in health systems that facilitate Aboriginal and Torres Strait Islander sovereignty. Non-Indigenous care providers need to make a concerted personal effort to challenge their own beliefs and take away your prejudgment of your idea of how things should work and accept that, you know, that’s not going to be in line with how community or how their patients work, and you have to be accepting of that and understand. (ACCHS stakeholder)
Reflecting on one’s behaviors and addressing power differentials is a necessary part of the cultural security journey: No one person can ever be culturally secure. It is not a destination, it’s a journey . . . and I don’t think that you can go on a cultural security journey without going on a decolonization journey at the same time. . . . Some days I have really good days, and other days I have really bad days where . . . White privilege just clouds my judgment . . . because that’s the environment in which I grew up in, and it’s my modus operandum of functioning. And it’s a cognitive thought process to be able to correct that, and to be able to challenge that, and to be able to go forward in a decolonizing way . . . I think that making sure that you are looking inwards and addressing your own biases and your own privilege and your own, you know, racism within yourself that exists is . . . is the most important thing that you can do. (Renal stakeholder)
A number of challenges and limitations within the current system were identified by stakeholders. The experience of CKD requires high-intensity engagement with a medical model that is not fit for purpose for Aboriginal and Torres Strait Islander peoples: If you’ve got chronic kidney disease, is challenging to navigate if you are in town and highly literate and highly health literate, and if you are none of the above it’s, you know, no surprise that people have difficulty navigating that pathway, and we don’t really make any particular effort to help people. (Renal stakeholder)
For most patients, CKD demands a minimum of three 4-h hospital-based dialysis sessions each week, in addition to any other specialist appointments required. Such frequent contact with a colonial and biomedical system that does not align with Aboriginal and Torres Strait Islander values has ramifications for patient well-being: The ongoing effects of colonization and the disruption of [Aboriginal and Torres Strait Islander] ways of working and ways of developing communities and societies [results in] the dislocation of patients from their homelands and their communities, and then the downstream social and economic effects of that. . . . None of our health systems are really fit for purpose and patient centered. So, I think if we can get the Aboriginal space right and then extend that out to all patients, I think that we’re going to end up with a much more patient-centered system. But this is the group that’s, you know, at the tip of the iceberg in terms of the level and degree of disadvantage that our system brings. (Renal stakeholder)
While renal stakeholders discussed the importance of oral health throughout the CKD journey, the priority of oral health is currently too late in the kidney care pathway: It’s only when it comes up for people looking to access the transplant list or getting all their tests done that that’s when it’s “oh, you need a dental checkup and you need some teeth extracted,” or . . . which is really quite sad, when it’s something we could actually organize. . . . But, unfortunately, it’s not one of those things we focus in on. (Renal stakeholder)
Maintaining oral health and hygiene can also “slow down the progression of your chronic kidney disease. So, that’s the number one issue right from an early stage” (renal stakeholder). Oral health remains important posttransplant, but little support for patients postoperatively is provided: I think also, the priority of posttransplant patient, it takes a mammoth journey to get on that waitlist. But when you get on it, and we get a transplant, we still need the oral health side of it because of what’s happening with our bones. And yet, that’s not a priority with dental because you’ve already had transplant. We still have to eat. (CKD lived experience stakeholder)
In rural areas, demand for dialysis exceeds capacity, which means that many patients with CKD have to move away from home, family, community, and country to access care. This lack of resources within the dialysis care provision affects the ability to maintain one’s well-being: There’s the consideration of cultural issues and, how people’s responsibilities in their community, responsibilities to their family, how that impacts the choices people have to make in their care with, you know, whether they are able to meet cultural obligations, obligations to family or come and get treatment that they need. (ACCHS stakeholder)
Removal from country due to CKD affects not only an individual but their entire community: I heard one of the patients say that the chair takes their family. . . . Dialysis takes their family. So, that’s a whole cultural leader totally removed from his community. So, he can’t interact with his grandchildren, you know, the younger generation, the older generation sharing his knowledge, yeah. It’s quite heartbreaking. . . . And I don’t think people fully get it, at all. (Renal stakeholder)
Renal transplantation ultimately allows people to return home to country, community, and family, which ultimately improves well-being as opposed to urban dialysis. Clinics do their best to provide opportunities for community members to return to country, but capacity of staffing and resources limits implementation and sustainability of changes to care: It depends on staff availability, a whole range of different issues. So, there are also clients that come back for things like funerals or other cultural activities, so we try and accommodate them where we can but there are times when that’s not possible. (Renal stakeholder)
Capacity of staffing and resources also related to the accessibility of dental treatments and preventative services outside of metropolitan areas: “The only way we can [provide dental care] is if people are working in this space . . . and bring the treatment to them, but I don’t know. It’s the attraction and retention, isn’t it, of staff” (dental stakeholder).
Stakeholders external to the oral health system had little to no involvement in oral health pathways. In rural settings where dental services were available, some renal staff would assist with booking appointments for patients on dialysis; however, in urban areas, this was far less common: If we had a pathway, like we do for other allied health, for the patient to actually see somebody about their oral health, then we could then ensure that that connection happens and we can then sign off on that element of their care . . . because there’s no oral health team member . . . we can’t actually do that. It’s up to the patient to do that at the minute. (Renal stakeholder)
The lack of communication between dental and renal teams contributed to difficulties in navigating the oral health system: I think often there’s services available, but the two don’t get to meet . . . or they get to meet when it’s a little bit too late. . . . Enabling and supporting existing kidney team members to know how to advocate for [dental] services, I think that’s probably the most sustainable. (Dental stakeholder)
Stakeholders recognized the collective responsibility to ensure strong oral health for Aboriginal and Torres Strait Islander people with CKD: Part of the problem is [that oral health is] everybody’s and nobody’s responsibilities, but as the nephrologist, you know, I guess we have a role in coordinating care of dialysis patients and identifying and making sure that needs are met even if they’re not directly nephrological. So, I think we do have a responsibility, there’s no . . . but there’s no single responsibility. (Renal stakeholder)
Oral health was described as a luxury inaccessible to many patients with CKD due to a lack of cultural security, shared information, and the effects of social determinants of health. The dental gap for those who do not qualify for a health care card was highlighted by many stakeholders, including one AHW/P: You know, how can this help reiterate to the government that you’ve got the health care card and that, but basically we have to pay the full brunt for dental care, and hence why we won’t worry about getting an appointment because we can’t afford to . . . we live from pay to pay, we don’t have that luxury of saving for rainy days. (ACCHS stakeholder)
For some patients, they were able to pay for the initial consultation, only to find out that they required thousands of dollars of dental work, which was challenging. The sporadic nature of dental visits in a rural setting also created confusion and barriers to accessing care: [The health organization] sometimes has a dentist and you can get dental appointments, but again it’s very haphazard, and I have no knowledge of nor control over how the services are provided other than sometimes they’re there and sometimes they’re not. (Renal stakeholder)
The separation of oral health from Medicare limited functionality of the integration of care but also patient understanding of the centrality of oral health for their kidney health: Dental should be part of the health care system . . . and that’s legislation that needs to changed, I think there needs to be those conversations at the top. Dental should be, it’s a part of your whole body that you know, it should be it should be a part of the health care system, we have access to dental care, just like you have access anywhere else. (CKD lived experience stakeholder)
Importantly, many opportunities to strengthen care were suggested by stakeholders. Developing strategies that assist with navigating the oral health system has the potential to help not only patients but also members of their health team: We talk about, you know, collaboration and building partnerships and the importance of building relationships. But then it’s difficult. Because people don’t understand what roles and responsibilities belong to who in the dental field. . . . Who do you send someone to? . . . I can just imagine what it’s like for people on the ground who have no idea. (CKD lived experience stakeholder)
Having someone to help navigate the experience of CKD through a case manager, or a lived experience buddy system, was highlighted as an option that would benefit patients: So, there’s somebody who’s gone through the system, somebody who’s had experience of the disease, to be your buddy to get you through the system. And I think that would be really important for CKD . . . having somebody, not a doctor, not a nurse, but an educated patient, do you know what I mean? An expert patient who can actually be there to talk to and guide you through the process and tell you how to do things and what things mean. I think that would be the single biggest thing to help people get through all of this, because it’s complex, it’s really complex what you’ve got to do. (CKD lived experience stakeholder)
Clear referral pathways with consistent follow-up and integrated knowledge would enable more holistic provision of care: Dental stakeholder has such a high waitlist so, if they send out a letter or two and they don’t hear, they’ll try a phone call. If there’s no answer, then they’ll just go on the automatic recall, try again in a few months’ time . . . they don’t have the time or the support networks to continuously try and ring. . . . But maybe, yeah, there should be sort of a star person or a spreadsheet to be sent to everyone that just keeps getting updated. For everyone to flag, “Look, this patient hasn’t been in for their regular dental checkup, what’s going on? Can you please help follow-up?”
Aboriginal and Torres Strait Islander leadership in positions of power is needed for meaningful change, as exemplified by advancements within the renal sector in South Australia: We are getting Aboriginal people on the working group. We’re putting in workforce strategies, we’re putting in cultural protocols. We’re doing things, but we’re still at the point of recognizing that we have a problem, and I’m not even sure we’ve got to the point of recognizing the extent of the problem. And I think that will only come when we have more Aboriginal leadership in really high places . . . [and] positions of power that will actually be able to then take it down from a top-down approach. (Renal stakeholder)
Increased Aboriginal and Torres Strait Islander leadership requires fostering interest, skill, and employment opportunities. Within the dental context, many communities do not have stable or regular access to dental care: My dream for dental would be to have community members work in these [remote] areas . . . that’s why we started working within schools . . . sort of planting the seed and getting students interested in working in dental and just having dentists and dental therapists out there and not fly-in, fly-out. . . . I don’t think that really works, unfortunately. (Dental stakeholder)
Mob providing care for mob is required to ensure both culturally secure and cohesive care because Aboriginal people know what works for Aboriginal people, and they’ve been telling us for a long time, but it’s been falling on deaf ears. And we essentially, as mainstream health workers, ignore them, and we tell them that they’re wrong and they should do it our way, and then we are surprised when our way doesn’t work. (Renal stakeholder)
The need for Aboriginal and Torres Strait Islander employment in the dental workforce was also discussed as “really important [due to] a lot of fear and anxiety, so to be able to identify with someone that you can sit down and have a chat with, that’s really important, too” (dental stakeholder).
Early education and intervention programs were discussed as necessary to move from diagnosis to prevention in communities: Ultimately, we should be thinking about health prevention and promotion, and we should be stopping people from getting kidney failure to begin with, which means addressing all the things . . . from the prenatal environment right through the life course that puts people at an increased risk of developing kidney failure to begin with . . . people shouldn’t be ending up on dialysis at increased rates. (Renal stakeholder)
As well as prevention, education would strengthen self-determination of community: I think, first and foremost, a better understanding within community. So better education. For a lot of people with diabetes or early-onset kidney disease. It’s about educating them on the pathways around their own health . . . we need to get better at educating the whole community about what contributes to kidney disease . . . so that people are able to better manage their own their own health. (ACCHS stakeholder)
Similar to the holistic health approach championed by ACCHO, integrated and holistic care that meets community-identified needs was identified as beneficial for those living with CKD. Particularly, the integration of oral health services was key: Do we talk about teeth when they’re talking about kidney disease? No. Do they talk about it with cardiovascular health? No. So, the cardiologists, the nephrologists, we should all be talking together and there should be a big impact statement made and something put out there, you know how they advertise about different things. Dental needs to be incorporated absolutely within that. (Dental stakeholder)
Renal teams identified ways to begin the integration of oral health into the care pathway for community members living with CKD: Oral health services, can get forgotten because they’re not front and center in the hospital. . . . We’ve got an opportunity to just embed that into all of our care pathways. I’m just now thinking as I’m talking to you that maybe we should just . . . you know, we do a tick-box of “Have they seen a pharmacist? Have they done this? Have they done that?” and maybe we should be putting in there “Have they got a dental referral?” (Renal stakeholder)
Cross-discipline training and knowledge sharing were discussed as opportunities to strengthen provision of care across ACCHOs, renal teams, and dental teams. At an ACCHO level, oral health training was identified as important for self-determination: Our staff here definitely could do some more training around oral health and hygiene and how they spread that message across different areas . . . if there’s an opportunity for them to upskill in that area, definitely, we’d take that opportunity on board. Because it’s also giving them the skills and knowledge to transfer . . . it gives you, the individual worker, more tools and strategies. (ACCHS stakeholder)
Renal nurses reflected on the potential benefits of receiving information about a patient’s oral health: It would be very interesting to get feedback on what people’s teeth are like, not just send a person out for an appointment and then the patient’s understanding is “Yeah, I’ve been to the dentist” . . . rather than, like, you might flag and say “Well, actually, there’s X, Y, and Z wrong with their teeth,” you know, or “Their gums are really quite poor.” (Renal stakeholder)
Dental teams identified the need to support renal teams in navigating the dental health system: “Enabling and supporting existing kidney team members to know how to advocate for services, I think that’s probably the most sustainable [approach]” (dental stakeholder).
Fundamentally, recognition and appreciation for the collective responsibility to ensure oral health for Aboriginal and Torres Strait Islander people living with CKD are required across all health care providers. At an ACCHO level, AHW/P and managers recognized their role in oral health education: We all have a responsibility as an individual, parent, uncle, auntie, grandparent, but also from our perspective as [a health service], we have a really important role to play on educating mob in community around good oral health. (ACCHS stakeholder)
At a societal level, stakeholders discussed the effects of privatized dentistry and related societal responsibilities to ensure collective health: I think it’s everyone’s responsibility . . . I think it’s the patient’s responsibility, I think it’s the health care provider’s responsibility, I think it’s society’s responsibility to look after vulnerable people in our society, and therefore I think it’s the government’s responsibility as our elected officials to look after people within our society who are vulnerable, who may have ill health and be unable to look after themselves. The responsibility flows on to everybody; that’s what being a society is all about. (Renal stakeholder)
Discussion
While the relationship between CKD and oral health is well evidenced (He et al. 2023), little progress has been made regarding the integration of dental care into the kidney care journey within the Australian health care system. This project is distinct in that we brought together stakeholders with different expertise, while foregrounding Aboriginal and Torres Strait Islander leadership, to ascertain the current state of health equity at the nexus of CKD and oral health. The findings emphasize the unique multifaceted circumstances in which Aboriginal and Torres Strait Islander people living with CKD are expected to navigate complex racist government health systems to achieve oral health support. Critically, operating within the rigid bounds of a colonial biomedical system has ramifications for the spiritual, social, and emotional well-being of individuals. Prioritizing culturally secure care as well as encouraging cross-discipline communication and advocacy are required to improve the provision for oral health support within the spectrum of kidney care.
Many findings from this project echo previously identified barriers to oral care for Aboriginal and Torres Strait Islander communities in Australia and Indigenous peoples globally (Poirier, Soares, et al. 2023). However, the complex interplay of CKD and associated medical needs with oral health demonstrate the need for unique consideration and efforts that ensure oral health is no longer a barrier to kidney transplantation (Hughes et al. 2023). Data sharing between ACCHS, dental clinics, and government health services is currently not mandatory in South Australia; however, this is an essential step toward wraparound care that identifies dental needs earlier in the CKD journey and indeed for other chronic diseases as well. Previous works have successfully used peer navigators for individuals living with CKD (Taha et al. 2022) and used AHW/P for oral health promotion (Poirier, Sethi, et al. 2023). The need for assistance navigating the complexities of Australia’s oral health system was strongly articulated throughout the findings of this project. There is scope to include oral health in a peer navigator role (Kelly et al. 2022; Taha et al. 2022) or through the establishment of an oral health coordinator within the kidney care team that assists with dental appointments, oral health promotion, and integration of oral hygiene into daily routines. Further, providing oral health promotion training for AHW/P in ACCHS would have an upstream and preventative impact on Aboriginal and Torres Strait Islander community understandings of oral diseases while simultaneously supporting community self-determination of oral health.
The publication of the First Nations CARI (Caring for Australians and New Zealanders with Kidney Impairment) guidelines in November 2022 called for culturally safe screening and early detection programs, models of care throughout the kidney health journey, and public awareness of CKD prior to diagnosis (Tunnicliffe et al. 2023). As demonstrated here and elsewhere (Sethi et al. 2022; He et al. 2023), oral health remains a missing piece of overall well-being essential for healthy kidney function. Fundamentally, the inclusion of oral health within Australia’s Medicare would address the persistent neglect of oral disease while facilitating connectedness across care teams and easing cross-discipline communication (Nguyen et al. 2023). However, development at this nexus cannot wait for these policy changes to be achieved. We contend that further work and advocacy in alignment with the CARI guidelines is required to ensure the integration of dental care for Aboriginal and Torres Strait Islander people living with CKD, ensuring holistic models of care focused on early intervention (Tunnicliffe et al. 2023).
This work has identified actionable steps that will support the oral health of Aboriginal and Torres Strait Islander people living with CKD, including (1) cross-disciplinary training for renal teams regarding the importance of oral health and vice versa for dental teams and ACCHS teams; (2) the inclusion of dental appointments on prescreening checklists both at the general practitioner level and during workup for starting dialysis, and then consistently considered throughout one’s dialysis journey; (3) advocating for permanently funded peer navigators; and (4) the development of a clear referral pathway with integrated follow-up across the care team. While this project was undertaken in a context specific to South Australia, the colonial restraints of biomedical systems on Indigenous health, the fractured nature between medical and dental systems, and the centrality of dental health in chronic disease management is not unique to this context. The findings of this project can provide guidance for work intersecting at any 2 of these 3 aspects; the primary learnings being the importance of speaking to all actors in the space, especially those on the ground and with lived experiences, to identify challenges and opportunities to strengthen provision of care for patients.
Conclusion
To mitigate the impacts of systemic racism, colonialism, and disadvantage perpetuated by Australia’s social and political discourse and biomedical care models, cohesive and united action across dental, renal, and ACCHS networks is required. Ultimately, the inclusion of oral health within Medicare and ACCHS would strengthen early intervention for oral health and therefore reduce the barrier of oral health clearance necessary for transplantation eligibility. However, action is needed to mitigate these impacts in the meantime; this action requires dedication from all sectors involved in the management of CKD for Aboriginal and Torres Strait Islander peoples and must be grounded in cultural security and self-determination of patients. Recognizing the collective responsibility to support patient oral health compels all actors working at the nexus of oral health and CKD for Aboriginal and Torres Strait Islander peoples to create opportunities for cross-disciplinary communication, training, and referral pathways, as led by Aboriginal and Torres Strait Islander peoples.
Author Contributions
B. Poirier, contributed to conception, design, data analysis, drafted the manuscript; S. Sethi, contributed to conception, design, drafted the manuscript; L. Jamieson, contributed to conception, design, critically revised the manuscript; J. Hedges, contributed to conception, design, data analysis, critically revised the manuscript. All authors gave their final approval and agree to be accountable for all aspects of work.
Supplemental Material
sj-docx-2-jct-10.1177_23800844241286729 – Supplemental material for “It’s Everybody’s and It’s Nobody’s Responsibility”: Stakeholder Perspectives on Aboriginal and Torres Strait Islander Health Equity at the Nexus of Chronic Kidney Disease and Oral Health
Supplemental material, sj-docx-2-jct-10.1177_23800844241286729 for “It’s Everybody’s and It’s Nobody’s Responsibility”: Stakeholder Perspectives on Aboriginal and Torres Strait Islander Health Equity at the Nexus of Chronic Kidney Disease and Oral Health by B. Poirier, S. Sethi, L. Jamieson and J. Hedges in JDR Clinical & Translational Research
Supplemental Material
sj-pdf-1-jct-10.1177_23800844241286729 – Supplemental material for “It’s Everybody’s and It’s Nobody’s Responsibility”: Stakeholder Perspectives on Aboriginal and Torres Strait Islander Health Equity at the Nexus of Chronic Kidney Disease and Oral Health
Supplemental material, sj-pdf-1-jct-10.1177_23800844241286729 for “It’s Everybody’s and It’s Nobody’s Responsibility”: Stakeholder Perspectives on Aboriginal and Torres Strait Islander Health Equity at the Nexus of Chronic Kidney Disease and Oral Health by B. Poirier, S. Sethi, L. Jamieson and J. Hedges in JDR Clinical & Translational Research
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Australian Department of Health grant (4-G19UGVN)
A supplemental appendix to this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.