
Abstract
Introduction:
The adolescent diet is high in sugars compared with other age groups. Effective approaches to support sugar reduction by adolescents are needed as part of caries prevention.
Objective:
To systematically review peer-reviewed evidence (1990 to 2023) to identify effective behavior change techniques (BCTs) for sugars reduction in adolescents aged 10 to 16 y.
Methods:
Nine databases (CINAHL, Cochrane, Dental and Oral Sciences Source, EMBASE, MEDLINE, PubMed, PsycINFO, Scopus, and Web of Science) were searched. Identified articles were screened independently in duplicate for eligibility. Interventions were eligible if they aimed to change adolescent dietary behavior(s) and reported pre- and postsugar-relevant outcome measures. Interventions from included studies were coded using a 93-item BCT Taxonomy (Michie Taxonomy v1). Risk of bias was assessed using the Effective Public Health Practice Project Quality Assessment Tool for Quantitative Studies. Evidence synthesis by vote counting (number of studies showing positive versus null or negative effects) was applied to BCTs that were present in more than 5 interventions.
Results:
Of 16,271 articles identified, 764 were screened in full, yielding 35 studies (in 43 papers), of which 3 were uncodeable. BCTs coded in interventions covered 11 of 16 BCT clusters and 25 of 93 individual BCTs in the BCT taxonomy. The median number of BCTs applied per study was 3 (interquartile range 2–6). Evidence synthesis indicated that the BCTs most positively associated with a positive reduction in sugars were (with the percentage of strong-/moderate-quality studies applying these techniques that successfully reduced sugars intake in brackets) feedback on behavior (100%), information on social and environmental consequences (100%), problem solving (75%), and social comparison (75%).
Conclusion:
Notwithstanding limitations in available data, the current evidence most strongly supports the use of BCTs relating to feedback on behavior, providing information on the social and environmental consequences, include problem solving and making social comparisons, to lower sugars intake in adolescents.
Knowledge Transfer Statement:
The results of this study will enable clinicians to provide more effective dietary advice when supporting dietary behavior change to reduce sugars intake in adolescents. The results may also be used by researchers to guide future directions for research into effective sugars reduction in adolescents.
Introduction
The early to mid-adolescent life stage (between 10 and 16 y) is a rapid phase of development, during which adolescents gain increasing psychosocial autonomy and independence including in their dietary choices (McKeown and Nelson 2018). Early adolescence is also the life stage during which the permanent dentition, including the second molars, has erupted (Fekonja 2022). Evidence synthesis shows moderate evidence for the effectiveness of multicomponent interventions in promoting oral health–related behavior in adolescents (Xiang et al. 2020), yet the impact of dietary behavior has not been investigated in isolation from other elements of oral health promotion.
The diet of adolescents compared with other age groups is poor (Lipsky et al. 2017; Patte et al. 2024). Dietary behavior changes observed during adolescence include an increased frequency of consuming energy-dense nutrient-poor foods (e.g., foods high in sugars, fats, and sodium and sugar-sweetened beverages). National surveys from several countries show that intakes of free sugars peak during adolescence (Turck et al. 2022). For example, most recent Australian data show 87% of those aged 9 to 13 y and 85% of those aged 14 to 16 y exceeded the World Health Organization (WHO) recommendation to limit free sugars intake to less than 10% of total energy (Louie et al. 2016). The UK National Diet and Nutrition Survey showed 11- to 18-y-olds on average consume 12.3% of energy as free sugars, which is substantially greater than the dietary reference value of less than 5% of total energy as a population goal. Dietary sugars are the most important direct cause of dental caries, and a wealth of evidence supports sugars reduction as a key part of preventive dental health (Moores et al. 2022). Moreover, limiting dietary sugars plays a key role in the prevention of undesirable weight gain (Public Health England 2015).
It is recognized that both upstream and downstream public health measures are required to reduce sugars consumption (Public Health England 2015). Interventions targeting sugars reduction can achieve relevant health outcomes (e.g., reduced dental caries; Rodrigues et al. 1999). Prerequisites for the development of interventions aimed at supporting individuals to lower sugars levels should include identification of the intervention modalities that are expected to be effective. However, many behavioral interventions have lacked adequate theoretical foundation for their content. Behavior change techniques (BCTs) are the “active ingredients” of an intervention, as described in a BCT taxonomy (Michie et al. 2013), which is an hierarchical model comprising 93 distinct BCTs organized into 16 parent clusters of related BCTs (Table 1). A recent analysis of data pertaining to the effectiveness of interventions and BCTs for improving dietary intake in young adults (17 to 35 y old) indicated that habit formation, salience of consequences, and adding objects to the environment were the most effective BCTs (Ashton et al. 2019). However, to date, there has been no systematic identification and synthesis of BCTs underpinning effective dietary behavior change interventions aimed at lowering sugars intake by adolescents.
The BCT Taxonomy: Parent Clusters and Example BCTs within Each Cluster (Michie et al. 2013).
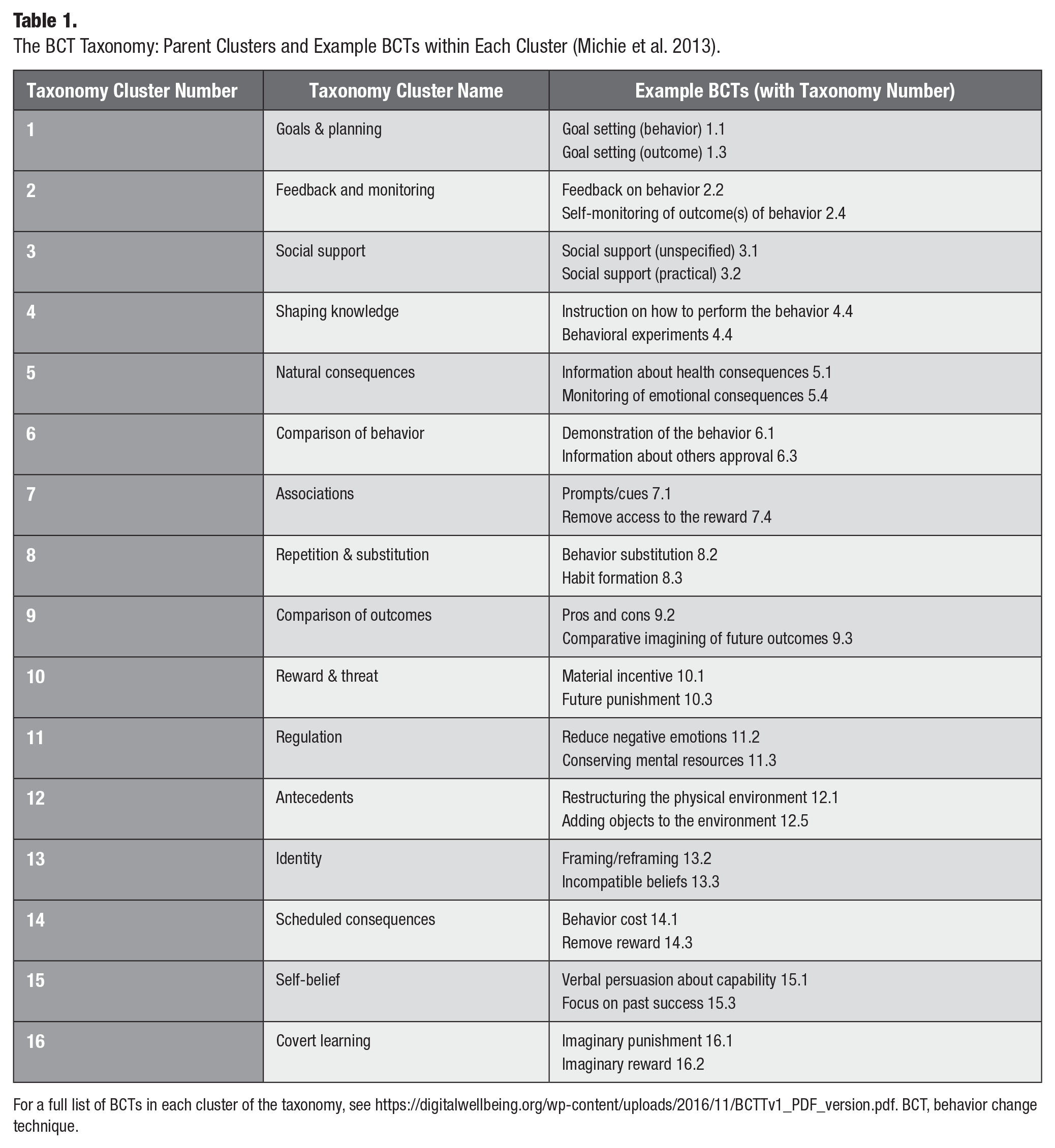
For a full list of BCTs in each cluster of the taxonomy, see https://digitalwellbeing.org/wp-content/uploads/2016/11/BCTTv1_PDF_version.pdf. BCT, behavior change technique.
If “best practice” with respect to effective dietary BCTs to apply with the adolescent age group can be identified, this would assist dental professions, other practitioners, policymakers, researchers, and funding bodies to make informed decisions around strategies for sugars reduction. In view of this, the aims of this research were to identify, from published data pertaining to interventions targeting mid to early adolescent diet behavior change, which BCTs (1) are effective, (2) are not effective, and (3) have not yet been studied, in relation to sugars reduction by adolescents aged 10 to 16 y. The objectives were (1) to systematically review peer-reviewed publications pertaining to dietary intervention studies aimed at adolescents aged 10 to 16 y that included a measure of dietary sugars as an outcome, (2) using the taxonomy of BCTs of Michie et al. (2013) to identify the BCTs that have been applied in the interventions, (3) to identify which specific BCTs were/were not effective with respect to sugars reduction, and (4) to identify any BCTs that have not been applied in interventions aiming to reduce sugars intake in adolescents and thus identify future research need.
Methods
This systematic review was prospectively submitted on PROSPERO (https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42020164544) on January 8, 2020, and was subsequently registered on April 28, 2020. The overarching research question was, “What are the effective components and behavior change techniques for interventions to change diet in adolescents (aged 10 to 16 y)?” This systematic review is reported according to the PRISMA 2020 statement. The completed PRISMA checklist can be found in Appendix Table 1.
Eligibility Criteria
Studies were eligible for inclusion if the design was an intervention study (including randomized controlled and quasi-experimental design study) or was a systematic review of intervention studies. Pre–post studies with no comparator group were also included. Cross-sectional design studies, review articles (e.g., narrative reviews), protocol papers, preprints, conference abstracts, theses, and retracted articles were excluded. Studies were included if they were published in the English language between 1990 and July 31, 2023.
Population
Studies were eligible if participants were adolescents aged 10 to 16 y or where data were reported separately for adolescents to other included population subgroups (e.g., children, adults). Studies were eligible where participant age range, median age, or mean age fell within 10 to 16 y of age. Studies were ineligible if participants were restricted to those with a specific disease or condition.
Intervention
Interventions were eligible for inclusion if they aimed to change adolescent dietary behaviors and reported independent effects for pre- and postintervention measures for at least 1 outcome of interest.
Comparator
Studies were eligible where the comparator group was either a different intervention (including varied intensity), usual care, or nonexposure to the intervention (nonexposed control group). Single-group pre–post studies were also eligible.
Outcomes
The main outcomes of interest were sugars-relevant dietary intake measures including total, free, or added sugars intake or intake of high-sugars foods and drinks, measured as g/day, percentage contribution to energy (%E), or the frequency of consumption. High-sugars foods included sugar-sweetened beverages (SSBs), confectionery, chocolate, desserts, cakes, biscuits/cookies, and ice cream. Other relevant outcomes (e.g., the intake of water and milk) were included where SSB intake was reported. Outcomes reported at all time points were included.
Information Sources
Searches were executed in CINAHL, Cochrane, Dental and Oral Sciences Source, EMBASE, MEDLINE, PubMed, PsycINFO, Scopus, and Web of Science on January 13, 2020, and again on July 31, 2023 (Appendix Table 2).
Search Strategy
Search terms were built around 4 broad concepts: intervention studies, the adolescent population, behavior change, and diet and nutrition outcomes. Searches were developed in collaboration with a research librarian and were piloted to optimize search terms for each database. Database-specific terms (e.g., MeSH terms) were used where relevant.
Prior to exporting of records, searches were limited to studies published in English and from 1990 to the search date (to capture data published since the first numerical threshold was placed on sugars intake by the WHO). Search records from each of the databases were exported and compiled in EndNote (X9). Records were imported to Covidence (Veritas Health Innovation 2019) from Endnote for removal of duplicates and screening.
Selection Process
A preliminary screening of titles and abstracts for eligibility was performed by 1 researcher (C.J.M., with K.G. conducting the updated search), with a second researcher (P.J.M.) independently screening a random sample of 5%. Interrater reliability was assessed, and the process was repeated with refinement of detailed inclusion criteria until full agreement was met. Full-text screening was performed independently in duplicate (original search by C.J.M. and S.C. and updated search by M.M. and P.J.M.) to assess final eligibility. Any differences between the reviewers’ decisions were resolved through discussion. If consensus was not reached, a third-party reviewer (P.J.M. or A.M.T.) was consulted. Reasons for exclusion at the full-text stage were noted and are reported as per the PRISMA statement.
Data Extraction
Data were extracted by one reviewer and checked by a second reviewer. Data pertaining to the study population and demographics, intervention characteristics (adapted from the TIDieR checklist (tidierguide.org), comparison group, dietary outcomes, differences between intervention and control groups (effectiveness), and BCTs were extracted. An example data extraction form is presented in Appendix Table 3.
Coding of BCTs
BCTs reported in the intervention descriptions were coded independently in duplicate against the 93-item Behaviour Change Technique Taxonomy v1 (BCTTv1; Michie et al. 2013) by 2 researchers (C.J.M., A.M.T. or S.C.) who had completed training in the use of the BCT Taxonomy (http://www.bct-taxonomy.com). Using a standardized coding form (Appendix Table 4), interventions from included studies were coded from the descriptions in published papers, protocols, or online supplementary materials. Discrepancies were resolved by discussion, and a BCT coding log was kept to record decisions.
The standard principles of the BCT Taxonomy v1 Online Training for coding BCTs were followed. Only BCTs that are directly applied to the target behavior(s) and population(s) were coded, the presence of a BCT was not inferred, and BCTs that differed in terms of their behavior change type (i.e., behavior versus outcome) were differentiated. Technical terms and packages of BCTs that correspond to BCTs in the taxonomy were coded as described in Appendix Table 5. BCTs in the intervention and control groups were identified, and only the BCTs exclusively applied in the intervention group were extracted. Where multiple papers or studies used the same intervention, all BCTs reported were coded in the group of papers. For the purposes of analysis, the lattermost study was selected for complete data extraction.
Study Risk-of-Bias Assessment
Two authors (C.J.M. and S.C. for original searches and P.J.M. and M.M. for updated searches) independently assessed study quality using the Effective Public Health Practice Project Quality Assessment Tool for Quantitative Studies (Armijo-Olivo et al. 2012). Studies were assigned a ranking of strong, moderate, or weak for 6 study components: (1) selection bias, (2) study design, (3) confounders, (4) blinding, (5) data collection methods, and (6) withdrawals and dropouts. A global ranking was assigned from the component rankings as either strong (no weak ratings), moderate (1 weak rating), or weak (2 or more weak ratings).
Evidence Synthesis
Evidence synthesis was conducted using a vote-counting method that is suited to data from a heterogeneous group of studies (McKenzie and Brennan 2019) and that weighs the evidence showing a positive relationship between application of the BCT in an intervention and outcome (sugars) with that showing a null or negative association. The BCTs that were used in 5 or more of the included studies were identified. For each intervention that applied these BCTs, it was noted if there was a positive, null, or negative effect of the intervention on reducing sugars outcomes based on direction of effect. Data were formulated into Harvest plots, to depict the weight of the evidence in relation to the BCTs considering study quality. For studies reporting more than 1 sugars-related outcome with differing effects, outcomes were depicted by separate bars in the Harvest plot. Vote counting was supplemented with a narrative synthesis of findings.
Results
Study Selection
Following the removal of duplicates, 16,271 unique records were retrieved. Following title and abstract screening, 764 records remained for full-text screening, which resulted in inclusion of 35 interventions, reported in 43 papers. Papers excluded at full-text screening are presented in Appendix Table 6. The PRISMA flow chart is presented in Figure 1.
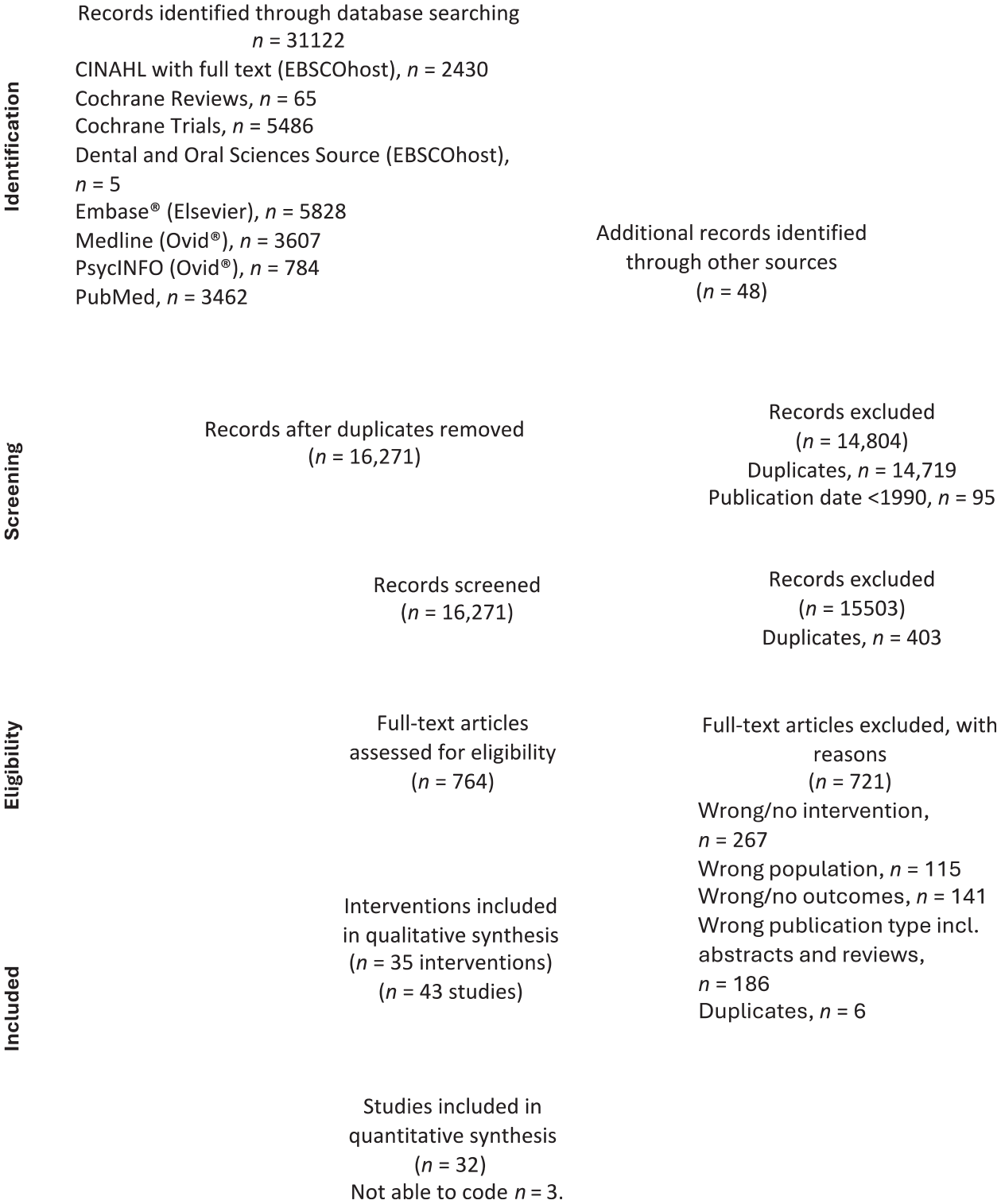
PRISMA flow chart.
Study Characteristics
The characteristics of the 35 included interventions are described in Table 2. Data extraction forms for included studies are presented in Appendix Table 7, where further details of the individual intervention duration and follow-up can be found. Most interventions (n = 27) were delivered in schools, and other settings included after-school clubs (n = 2), dental clinics in the school or community (n = 2), social media (n = 1), libraries (n = 1), and the home (n = 1). The global rating of study quality was weak for 20 studies, moderate for 12 studies, and strong for 3 studies (Table 2 and Appendix Table 8). Studies were of populations from 21 different countries in Europe (n = 11), North America (n = 10), Asia (n = 7), South America (n = 4), Africa (n = 2), and Australasia (n = 1).
Study Details and Global Study Quality.

BCT, behavior change technique; CI, confidence interval; C-group, control group; I-group, intervention group; SES, socioeconomic status; SSB, sugar-sweetened beverage.
Global quality ratings were assigned as per the Effective Public Health Practice Project Quality Assessment Tool for Quantitative Studies (Armijo-Olivo et al. 2012; Thomas et al. 2004), where global rating corresponds to number of weak ratings: strong (no weak ratings), moderate (1 weak rating), or weak (2 or more weak ratings).
Only the most recent reference associated with the study is cited. For references with an asterisk, see Appendix Table 10 for earlier papers associated with the study.
BCTs Applied
Across the 35 interventions, there was a median number of 3 (interquartile range 2–6) individual BCTs, ranging from 0 (no BCTs able to be coded as present) to 11 BCTs. Considering the moderate- and higher-quality studies only, the median number of individual BCTs used was 4, ranging from 1 to 9 in effective interventions and 1 to 11 in noneffective interventions. Most commonly, interventions applied 3 BCTs (n = 7 interventions). A total of 25 individual BCTs were coded across interventions; the number of interventions in which each BCT was applied is depicted in Figure 2. Interventions applied BCTs from a median of 3 (IQR 2–5; range 0–7) parent clusters from the BCT Taxonomy. The most frequent BCT clusters represented in the interventions were “Natural consequences” (cluster 5), present in 26 of 35 interventions; “Social support” (cluster 3), present in 13 of 53 interventions; “Repetition and substitution” (cluster 8), present in 13 of 35 interventions; and “Goals and planning” (cluster 1), present in 12 of 35 interventions.
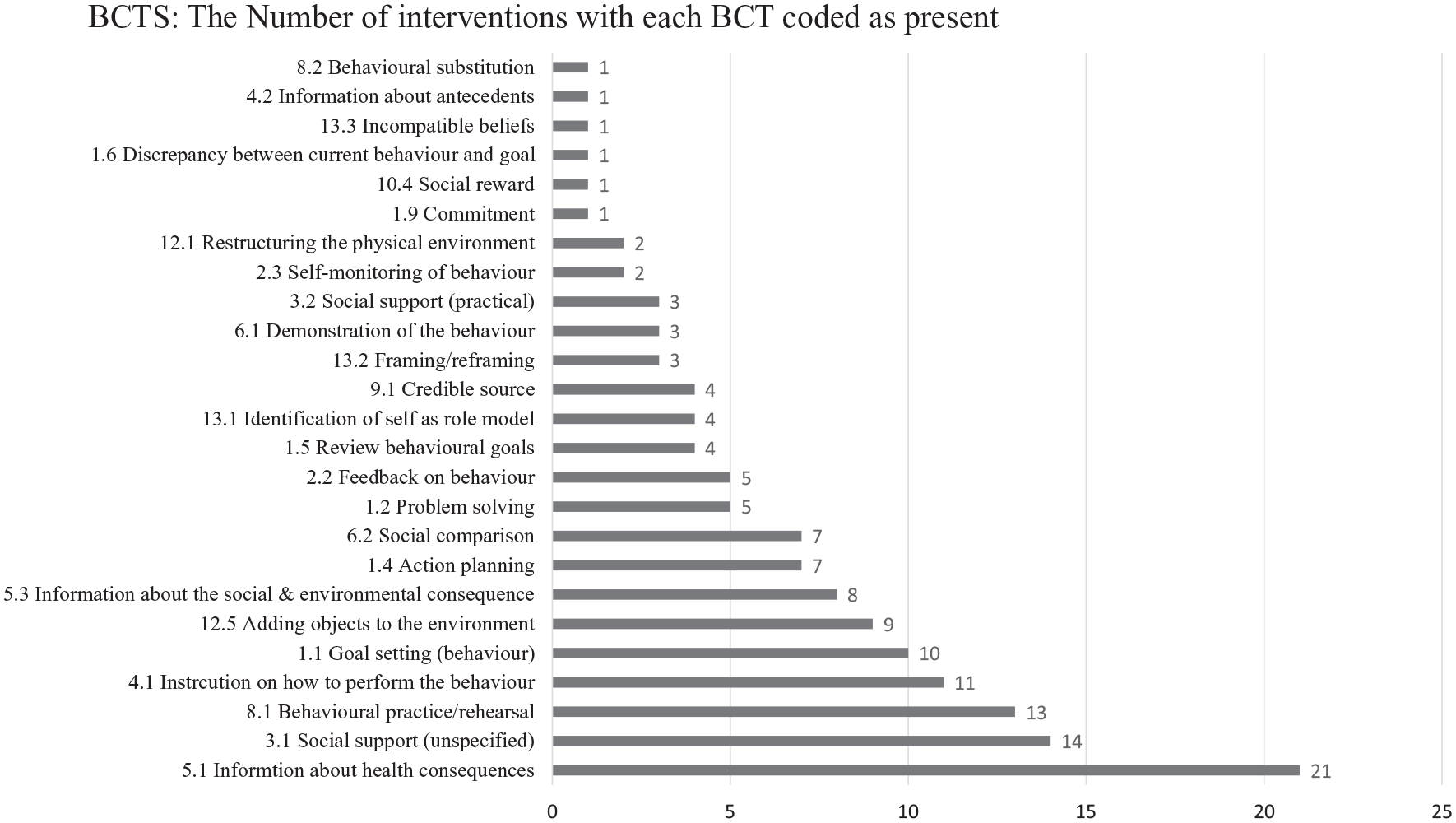
Frequency of Behavioural Change Technique Taxonomy V1, behavior change techniques used in the included intervention studies (descending order).
There were 5 BCT clusters, comprising 29 individual BCTs in the taxonomy, which were not applied in any intervention. These included “Associations” (cluster 7), “Regulation” (cluster 11). “Scheduled consequences” (cluster 14). “Self-belief” (cluster 15), and “Covert learning” (cluster 16). In addition to the individual BCTs within these 5 clusters, an additional 39 individual BCTs from within the 11 included clusters were not identified as being used in any intervention (Appendix Table 9). Collectively, 73% (68 of 93) of the individual BCTs in the taxonomy were not applied in the identified interventions.
Results of Evidence Synthesis by Vote Counting
Figure 3 presents the results of the evidence synthesis by vote counting. For each BCT applied in 5 or more studies, the graph indicates the balance and quality of those studies showing a positive versus null or negative impact on reduction of sugars outcomes. Based on a vote-counting assessment of studies rated strong or moderate only, the BCTs that were most strongly associated with a positive reduction in sugars intake were 2.2 Feedback on behavior, 5.3 Information on social and environmental consequences (100% of strong- and moderate-quality studies applying these techniques successfully reduced sugars intake), 1.2 Problem solving, and 6.2 Social comparison (75% of strong- and moderate-quality studies applying these techniques successfully reduced sugars intake).
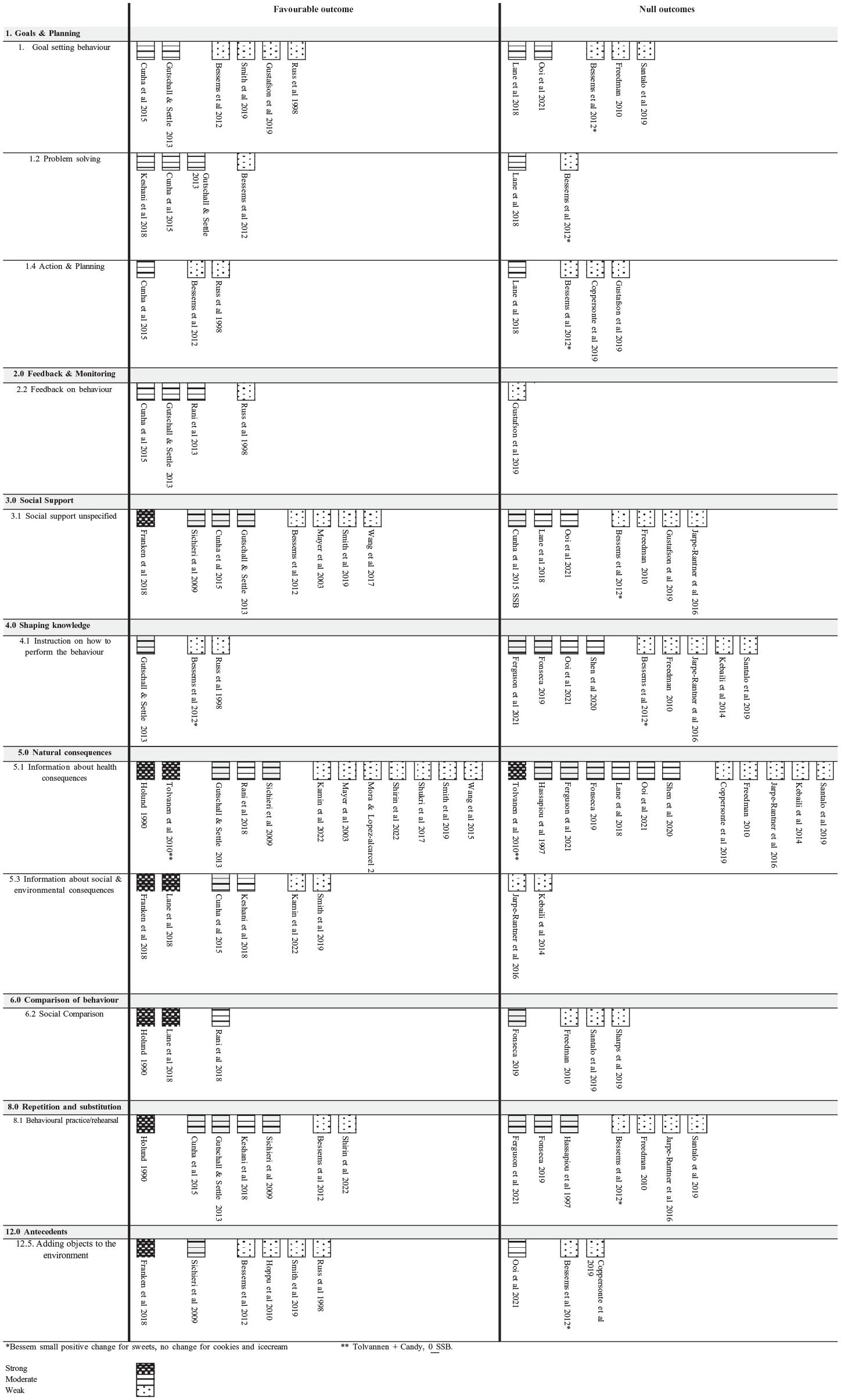
Harvest plots: the balance of interventions that had positive, null, or negative effects on lowering sugar-related outcomes for each BCT (for BCTs applied in 5 or more identified interventions).
Discussion
This review has shown that evidence from moderate- and high-quality studies most strongly support interventions that provide feedback on behavior (e.g., informing the adolescent how many teaspoons of sugar they consumed in a day), provide information on the social and environmental consequences (which included consequences other than those that were directly related to health or were unspecified), include problem solving (e.g., prompt the adolescent to identify the barriers preventing them from eating less sugary foods and drinks and discuss ways to overcome the barriers), and include social comparison (e.g., show the adolescent their average intake of SSB compared with that of their peers) for reducing intake of sugar/sugars-containing foods and/or drinks in adolescents. The findings showed that the effectiveness of the majority (73%) of the BCTs in the Behavioural Change Taxonomy (Michie et al. 2013) on sugars reduction in adolescents had not been tested.
Previous research investigating the efficacy of BCTs from the Behavioural Change Taxonomy (Michie et al. 2013), when applied to different dietary scenarios and age groups from that of the current study, have shown different results, which suggests the effectiveness of BCT varies by target age group. For example, in a review of the most effective BCT for changing diet in young adults aged 17 to 35 y, Habit formation (BCT 8.3), Salience of consequences (BCT 5.2), and Adding objects to the environment (BCT 12.5) were the most effective BCTs (Ashton et al. 2019). With the current younger age group, the evidence in support of Information on social and environmental consequences, and Social comparison suggests that young adolescents are influenced by their peers and social pressure. Indeed, previous research shows that adolescent dietary behavior is influenced by descriptive norms (the perception of what most adolescents do) (Verstraeten et al. 2014). Another systematic review of BCTs to promote physical activity in children aged 9 to 12 y from lower socioeconomic backgrounds found that 40 of the 93 individual BCTs (43%) had been applied to physical activity promotion, which is a higher proportion compared with the current study (27%). The most commonly applied BCTs for physical activity promotion were Behavioral practice rehearsal (BCT 8.1) and Instruction on how to perform the behavior (BCT. 4.1). However, these BCTs were shown to be applied in both effective and ineffective studies, and major differences in BCTs in effective versus noneffective interventions were not found. In the current analysis and in previous assessments of the effectiveness of different BCTs, the BCT Information on health consequences was broadly applied across effective and noneffective intervention studies, suggesting that providing information on specific health consequences as an individual BCT may not be effective in this age group. One intervention study (rated strong quality) applied the BCT on Information on health consequences in isolation but showed mixed results (reduced candy consumption but not SSB). However, providing education should be viewed as a part of a series of measures required to bring about sustained change and has an important role to play in driving change in opinion (Moynihan and Miller 2020). It is possible that providing information on health consequences is more effective when applied in conjunction with other BCTs, but this hypothesis remains to be tested.
The suggestion that interventions are likely to be more effective when BCTs are employed compared with education only is also relevant to wider oral health intervention. Tsai et al. (2020) in a systematic review evaluating the effectiveness of oral health promotion interventions in adolescents also found that interventions targeting adolescents that used behavioral change theory were more effective than those that were solely educational based. However, few oral health interventions comprehensively address sugars consumption: in a systematic review of oral health interventions, only 7 of 17 trials included a dietary element, which was in general knowledge based (Xiang et al. 2020). Future oral health interventions targeting adolescents should include evidence-based techniques to support lowering sugars intake.
In the current study, there did not appear to be any difference in study effectiveness according to the number of individual BCTs applied, which varied considerably but with a median of 4 BCTs for both effective and noneffective interventions. This median is lower than the median of 7 (range 1–13) BCTs applied to interventions targeting energy balance–related behaviors in children from lower socioeconomic status of 7 (range 1–13) (Anselma et al. 2020) and the median of 5 (range 1–25) BCTs applied to a wide range of dietary behaviors in young adults (Ashton et al. 2019).
Limitations
In the current analysis, the coding of BCTs was done retrospectively from published articles, and none of the included studies described the interventions against a BCT taxonomy. It is therefore possible that BCTs may have been missed due underreporting of intervention details in the study methods. It is also possible that studies in which interventions were poorly described or lacked details resulted in BCTs that may have been present in the intervention being not being coded. It is also possible that variation in terminology used to describe the interventions led to miscoding, although coding was done independently in duplicate to minimize this occurrence. Direct coding of the intervention materials may have been a more reliable approach to take but was not feasible because intervention materials and/or the source of such materials referred to were not always presented. Future studies when reporting intervention details should map approaches against a recognized BCT taxonomy such as the one used in the current evidence synthesis and report of the specific BCTs applied.
The current evidence synthesis by vote count dichotomized effect as effective versus noneffective and did not consider the size of the change in intake of sugars/sugars-containing items. Moreover, due to the diversity of the combinations of different BCTs applied in the included studies, it was not possible to compare the effectiveness of different combinations of BCT as no 2 studies were the same. This analysis also assessed only the presence or absence of a BCT. However, it is also likely that there were differences in how BCTs were applied, for example, the intensity and frequency the BCT was applied, consequent attendance/participation in an intervention, fidelity (whether the intervention was delivered as intended; BCTs could have been added/omitted unknowingly), and who delivered the intervention and how, and between-individual receptiveness to a particular BCT may also have had an impact on behavior change. Therefore, the effectiveness of a BCT depends on several factors around how it is applied that were not captured in the present assessment. A strength of the study was that it identified studies from a wide geographical spread of countries. However, it is also possible that the effectiveness of different BCTs varies by cultural factors, which further complicates the picture.
Future Research
Future research is needed to evaluate the effectiveness of BCTs in the taxonomy clusters for which no data on effectiveness were identified (Appendix Table 9). Many of the individual BCTs in these clusters would potentially lend to sugars reduction. For example, for the cluster “Associations,” the use of prompts and cues (BCT 7.1), which has been shown to be moderately effective in dietary interventions of young adults (Ashton et al. 2019), remains to be tested in adolescents. Likewise, the effectiveness of BCTs in the “Regulation” cluster such as “Conserving mental resources” (BCT 11.3; e.g., advising adolescents to carry a list of the sugar content of foods) could be tested. The UK Change4Life Sugar Smart Smartphone Application (App), which enabled users to scan and check the sugar contents of foods with bar codes, is an example of how this BCT can be applied. The Sugar Smart App was shown to be effective in younger children (5 to 11 y) (Bradley et al. 2020), but it was not tested in adolescents. For the cluster “Scheduled consequences,” BCTs such as “Schedule specific reward” (BCT 14.6; e.g., provide a reward for eating sugar at mealtimes only and not between meals) could be evaluated. In the present study, social comparison was identified as beneficial for sugars reduction; therefore, further assessment of thus far untested BCTs that involve some degree of adaptive peer influence is warranted (e.g., 3.3 Social support [emotional], 6.3 Information about others’ approval). The BCTs within “Self-belief” (cluster 15) and “Covert learning” (cluster 16) also warrant further research. Further exploration of the degree of effectiveness of different BCTs could include trials with multiple arms using BCTs alone or in combination to enable the simple and combined effects of BCTs to be determined. Such trials would, however, likely be complex and require large numbers of participants.
Conclusion
This evidence synthesis of the effectiveness of BCTs applied to sugars reduction in early to mid-adolescents suggests that the most effective BCTs for sugars reduction are providing feedback on behavior, including information about the social and environmental consequences, problem solving, and social comparison. Future studies should prospectively test the efficacy of BCTs and include details of applied BCTs in written reports.
Author Contributions
C.J. Moores, contributed to the concept and design, data acquisition, analysis and interpretation of the data, drafted and critically revised the manuscript; A.M. Taylor, contributed to data analysis and interpretation, critically revised the manuscript; S. Cowap, contributed to data acquisition and analysis, critically reviewed the manuscript; R. Roberts, contributed to the concept and design, data interpretation, critically reviewed the manuscript; K.A.M.M. Gunasinghe, contributed to data acquisition and analysis, critically reviewed the manuscript; P.J. Moynihan, contributed to the conception and design, data acquisition, analysis and interpretation of the data, drafted the manuscript. All authors gave their final approval and agree to be accountable for all aspects of the work.
Supplemental Material
sj-docx-1-jct-10.1177_23800844241280717 – Supplemental material for Behavior Change Techniques to Reduce Sugars Intake by Adolescents: A Systematic Review
Supplemental material, sj-docx-1-jct-10.1177_23800844241280717 for Behavior Change Techniques to Reduce Sugars Intake by Adolescents: A Systematic Review by C.J. Moores, A.M. Taylor, S. Cowap, R. Roberts, K.A.M.M. Gunasinghe and P.J. Moynihan in JDR Clinical & Translational Research
Footnotes
Acknowledgements
The authors wish to gratefully acknowledge Vikki Langton, liaison librarian for the Faculty of Health and Medical Sciences at the University of Adelaide, for her assistance and support in generating search terms and translating the database search strategies.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Paula Moynihan was a member of the European Food Safety Authority Working Group on Added Sugars and is a member of the UK Governments Scientific Advisory Committee on Nutrition Subgroup on Maternal and Child Nutrition. Paula Moynihan is a member of the Oral Health Advisory Council of Haleon. The other authors have no interests to declare.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
A supplemental appendix to this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.