
Abstract
Objectives:
Lower socioeconomic status (SES) is associated with increased dental pain among children. Lower SES in childhood may also contribute to the experience of dental pain among older adults, regardless of the SES in later life. However, this association is still unclear.
Methods:
We used cross-sectional data from the 2019 Japan Gerontological Evaluation Study using self-administrated questionnaires to investigate the causal mediating pathways between childhood SES and dental pain in later life using several SES variables collected at older age as potential mediators. A total of 21,212 physically and cognitively independent participants aged 65 y or older were included in the analysis. The dependent variable was experiencing dental pain during the past 6 mo. The independent variable was the SES at the age of 15 y (low/middle/high). Ten covariates were selected covering demographics and other domains. Education, subjective current income, objective current income, objective current property ownership, and the number of remaining teeth were used as mediators. Prevalence ratios (PRs) and 95% confidence intervals (95% CIs) for dental pain by childhood SES were calculated using a modified Poisson regression model.
Results:
The mean age of the study participants was 74.5 ± 6.2 y, and 47.5% were men. Of these, 6,222 participants (29.3%) experienced dental pain during the past 6 mo, and 8,537 participants (40.2%) were of low childhood SES. Adjusted for covariates and mediators, the participants with middle and high childhood SES had a lower PR of dental pain (PR = 0.93 [95%, CI 0.89–0.98], PR = 0.79 [95% CI, 0.73–0.85], respectively). Almost 40% of the association between childhood SES and dental pain at older age was mediated via SES in later life and the number of teeth.
Conclusions:
This study reemphasizes the importance of support for early-life SES to maintain favorable oral health outcomes at an older age.
Knowledge Transfer Statement:
The results of this study can be used by policymakers to promote policies based on a life-course approach that supports children living in communities with low SES and helps them maintain favorable oral health outcomes into their older age.
Introduction
Dental pain is a significant public health issue as it causes distress and negatively impacts the quality of life (Santos et al. 2019). Additionally, dental pain can lead to absence from work (Zaitsu et al. 2020) or school (Seirawan et al. 2012) and can affect other physical and social activities (Santiago et al. 2013). Previous studies have shown that dental pain was associated with various factors, such as current socioeconomic status (SES) (Kuhnen et al. 2009), mental health status (Kakoei et al. 2013), smoking (Kuhnen et al. 2009), social networks (Santiago et al. 2013), and dental visits (Kuhnen et al. 2009; Kakoei et al. 2013).
Early-life SES has been shown to negatively impact oral health in later life stages, with childhood SES linked to various oral health conditions in older adults, such as caries (Teixeira et al. 2019), periodontal disease (Thomson et al. 2004), few remaining teeth (Listl et al. 2018; Yamamoto-Kuramoto et al. 2023), and tooth loss (Åstrøm et al. 2021; Celeste et al. 2022). Therefore, it is likely that SES in childhood may have an impact on dental pain in older adults, an outcome that represents a current and/or recent oral condition.
Based on previous observational studies, it may be hypothesized that childhood SES might influence dental pain in later life by affecting subsequent SES (Seirawan et al. 2012) or increasing untreated dental disease (Teixeira et al. 2019; Thomson et al. 2004). However, less is known of associations between early-life stage conditions and dental pain in later life, and the underlying mechanisms are unclear.
This study aimed to determine the association between childhood SES and dental pain in Japanese community-dwelling older adults. Exploring whether childhood SES predicts dental pain in older adults allows us to understand how early-life SES inequalities currently affect oral health among older adults. This attempt may provide a foundational insight for determining dental public health policies addressing inequalities and poverty.
Methods
Study Setting and Participants
We used data from the Japan Gerontological Evaluation Study (JAGES) survey conducted from December 2019 to January 2020, a nationwide survey focusing on aging and social determinants of health. The target population was 345,356 participants aged 65 y or older living in 64 municipalities across Japan who were physically and cognitively independent. This cross-sectional survey was conducted via a self-administered questionnaire sent by mail. The total number of respondents to this survey was 240,889 (response rate: 69.8%). The questionnaire used in the study consisted of a main questionnaire sent to all participants and 8 subsidiary questionnaires randomly assigned to some of the targeted participants. One-eighth (24,353 participants) of the targeted participants were sent the subsidiary questionnaire that contained questions related to oral health, including dental pain and dental visits. Overall, 21,212 participants were included in the analysis after the exclusion of those who did not answer the question about dental pain and those who were edentulous. This study followed the reporting requirements of the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement.
Dependent Variable
Dental pain was used as the dependent variable. Dental pain was measured using the following question: “Have you had any dental pain within the past 6 months?” Response options were: “1. Never, 2. Hardly ever, 3. Occasionally, 4. Fairy often, and 5. Very often.” Dental pain was dichotomized as “no (1 and 2)” and “yes (3 to 5).”
Independent Variable
Childhood SES was used as the independent variable. Information about childhood SES was gathered using the following question: “How would you rate your socioeconomic status when you were aged 15 years, compared with standards at that time?” Response options were: “1. Low, 2. Middle-low, 3. Middle, 4. Middle-high, and 5 High.” Childhood SES was categorized into 3 categories: “Low (1 and 2),” “Middle (3),” and “High (4 and 5).”
Covariates
A directed acyclic graph (DAG) is shown in Appendix Figure 1. Several variables were used as covariates: sex, age, smoking, marital status, frequency of meeting friends, psychological distress, self-rated health, denture use, dental visit for treatment, and dental visits for prevention. The categories of each variable were as follows: sex (men, women), age (65–69, 70–74, 75–79, 80–84, over 85), smoking (never, quit, and yes), marital status (married, except for married), frequency of meeting friends (twice a week, 1/wk or 1/mo, and never), psychological distress (none, moderate, and severe), self-rated health (good, bad), denture use (no, yes), dental visit for treatment (within 1 y, within 1 to 3 y, and never), and dental visit for prevention (within 1 y, within 1 to 3 y, and never).
Mediators
Five variables were used as mediators: education, subjective current income, objective current income, objective current property ownership, and the number of remaining teeth. The number of remaining teeth was used as a proxy for the cumulative oral diseases across the life course (Kotronia et al. 2021). Objective current income was collected as a continuous variable but was recategorized into tertiles.
The categories of each variable were as follows: education (under 9 y, 9–12 y, or over 12 y), subjective current income (low, middle, or high), objective current income (low, middle, or high), objective current property ownership (low, middle, middle-high, or high), and the number of remaining teeth (20 or more, 9–5, and 4–1). In mediation analysis, we used these mediators as binary variables (education [under 12/over 12 y], subjective current income [low and high (middle and high)], objective current income [low and high (middle and high)], objective current property ownership [low and high (middle, middle-high, and high)], and the number of remaining teeth (20 or more and <20 [19–10, 9–5, and 4–1]).
Statistical Analyses
First, a modified Poisson regression model was performed to investigate the association between childhood SES and dental pain. We calculated the prevalence ratio (PR) and 95% confidence intervals (CIs) for dental pain. Model 1 was adjusted for sex and age. Model 2 was adjusted for sex, age, and education. Model 3 was adjusted for sex, age, and 4 SES variables. In model 4, all 15 variables were included in the model. Additionally, we calculated the E-value to check the robustness of the main analysis considering the unmeasured confounding factors. Next, we conducted a mediation analysis to estimate the proportion of the direct effect of childhood SES on dental pain. To ensure comparability with the results of Poisson regression analysis, we selected the “paramed” Stata package that allows Poisson regression to be specified. Due to the programmed methods of this mediation analysis command, the binary mediators (education, subjective current income, objective current income, objective current property ownership, and the number of remaining teeth) were used. Each mediator was included in the model one at a time to avoid multicollinearity.
We conducted the 6 sensitivity analyses to check the consistency of the results. First, we conducted a Poisson regression analysis using the SES trajectory from childhood to older age as an explanatory variable. The SES trajectory was categorized into 6 groups based on the probable change from childhood SES to subjective SES in older age as follows: persistent low, upward mobility from low, downward mobility from middle/high, persistent middle, upward mobility from middle, and persistent high. Second, based on a previous study (Celeste and Fritzell 2018), we hypothesized that the impact of the SES trajectory on dental pain is higher at younger ages. We examined the impact of the interaction between current age categories and the SES trajectory categories on dental pain. Third, we conducted an ordered logistic regression, treating the options for dental pain as a 5-level variable. Fourth, we defined the presence of dental pain using a different cutoff value. Dental pain was dichotomized into 1 (never, hardly ever, and occasionally) and 2 (fairly often and very often). We conducted a logistic regression as the prevalence of dental pain was 5.6%. Fifth, since a relatively large number of respondents to childhood SES indicated “middle to low,” we reclassified childhood SES into 4 categories—“low (1), middle to low (2), middle (3), high (4)”—and conducted a Poisson regression analysis. Finally, among the covariates, several variables other than sex and age were considered potential effect modifiers: smoking, marital status, frequency of meeting friends, psychological distress, self-rated health, denture use, dental visits for treatment, and dental visits for prevention. Therefore, we conducted the mediation analysis with adjustments for only sex and age as covariates.
To address the potential bias due to missing data, we conducted multiple imputation to generate 20 imputed data sets, and the final estimates were pooled using Rubins rules (van Buuren 2018). All analyses were performed using Stata software (version 16.1; StataCorp LP). The threshold for significance was set at P < .05, 2-tailed.
Ethics Approval and Consent to Participate
Ethical approval for the JAGES was obtained from the Ethics Committee of the National Center for Geriatrics and Gerontology (approval number: 992–3) and Chiba University (approval number: 2493).
The following 3 points were stated in the survey questionnaire: 1) Participation in this study is voluntary. 2) Returning the answered questionnaire is regarded as consent to participate in the study. 3) Respondents can withdraw their consent even after returning the answered questionnaire without repercussions.
Results
Figure 1 shows the flowchart of the participants in this survey. Of the 24,353 participants who received the oral health subsidiary questionnaire, those who did not respond to the question about dental pain (n = 1,695) and those who were edentulous (n = 1,446) were excluded from the analysis. Overall, 21,212 participants were included for the analysis. The characteristics of the study participants are shown in Table 1. The mean ± standard deviation age was 74.5 ± 6.2 y, and 47.9% were men. Of these, 6,222 participants (29.3%) experienced dental pain during the past 6 mo. Among the participants, 8,537 (40.2%) were of low, 9,811 (46.3%) were of middle, and 2,864 (13.5%) were of high childhood SES.

The flowchart of this study.
Characteristics of Study Participants (n = 21,212).

The percentage in total (n, %) indicates the column ratio. The number and percentage of missing data for each variable among respondents who received the oral health questionnaire (total n = 24,353): childhood SES (n = 1,404; 5.8%), education (n = 918; 3.8%), subjective current income (n = 1,083; 4.4%), objective current income (n = 3,462; 14.2%), objective current property (n = 5,558; 22.8%), smoking (n = 641; 2.6%), marital status (n = 620; 2.5%), frequency of meeting friends (n = 758; 3.1%), psychological distress (n = 5,635; 23.1%), self-rated health (n = 719; 3.0%), number of remaining teeth (n = 1,147; 4.7%), denture use (n = 1,012; 4.2%), dental visit for treatment (n = 1,494; 6.1%), and dental visit for prevention (n = 2,017; 8.3%).
SES, socioeconomic status.
The results of the modified Poisson regression model are shown in Table 2. In model 1, the sex- and age-adjusted model, the participants with middle and high childhood SES had lower PR for dental pain than participants with low childhood SES as the reference group (middle PR = 0.87 [95% CI, 0.83–0.91], high PR = 0.72 [95% CI, 0.67–0.78]). A similar pattern was observed in model 2 adjusted for sex, age, and education (middle PR = 0.88 [95% CI, 0.84–0.92], high PR = 0.74 [95% CI, 0.68–0.80]). This pattern was also observed in model 3, adjusted for sex, age, and 4 SES variables (middle PR = 0.90 [95% CI, 0.86–0.95], high PR = 0.76 [95% CI, 0.70–0.83]), as well as in model 4, adjusted for all variables (middle PR = 0.93 [95% CI, 0.89–0.98], high PR = 0.79 [95% CI, 0.73–0.85]). Additionally, for model 4, the point estimates of E-value about childhood SES (middle and high) were 1.36 and 1.85, respectively. The magnitude and direction of the sensitivity analyses were similar to those of the main analyses (shown in Appendix Tables 1 and 4–7).
Association between Socioeconomic Status in Childhood and Dental Pain in Older Adults (n = 21,212).

Model 1: adjusted for sex and age; model 2: adjusted for sex, age, and education; model 3: adjusted for sex, age, education, subjective current income, objective current income, and objective current property; model 4: adjusted for all variables. PR was estimated by a modified Poisson regression model with all variables simultaneously entered into the model. Bold means P < 0.05.
CI, confidence interval; PR, prevalence ratio; SES, socioeconomic status.
The results of the mediation analysis are shown in Table 3. Of the 4 variables considered as mediators for the association between childhood SES and dental pain, all the natural direct effects were statistically significant: education (PR = 0.79; 95% CI, 0.73–0.85), subjective current income (PR = 0.78; 95% CI, 0.73–0.85), objective current income (PR = 0.79; 95% CI, 0.73–0.85), objective current property ownership (PR = 0.79; 95% CI, 0.73–0.85), and the number of remaining teeth (PR = 0.80; 95% CI, 0.74–0.86). The natural indirect effect of subjective current income and number of remaining teeth were statistically significant: natural indirect effect of education (PR = 0.97; 95% CI, 0.94–1.01), subjective current income (PR = 0.97; 95% CI, 0.95–0.99), objective current income (PR = 0.99; 95% CI, 0.97–1.001), objective current property ownership (PR = 0.99; 95% CI, 0.97–1.01), and the number of remaining teeth (PR = 0.80; 95% CI, 0.74–0.86). The proportion of mediation was calculated using the estimates of both natural direct effect and natural indirect effect. The total proportion mediated by education was 11.8%, subjective current income was 12.7%, objective current income was 6.1%, objective current property ownership was 5.1%, and the number of remaining teeth was 4.1%. Therefore, subsequent SES and the number of remaining teeth explained up to 39.8% of the impact of childhood SES on dental pain in older age (Fig. 2).
Types and Proportions of the Mediation Effects of Potential Mediators for the Association between Childhood SES and Dental Pain.
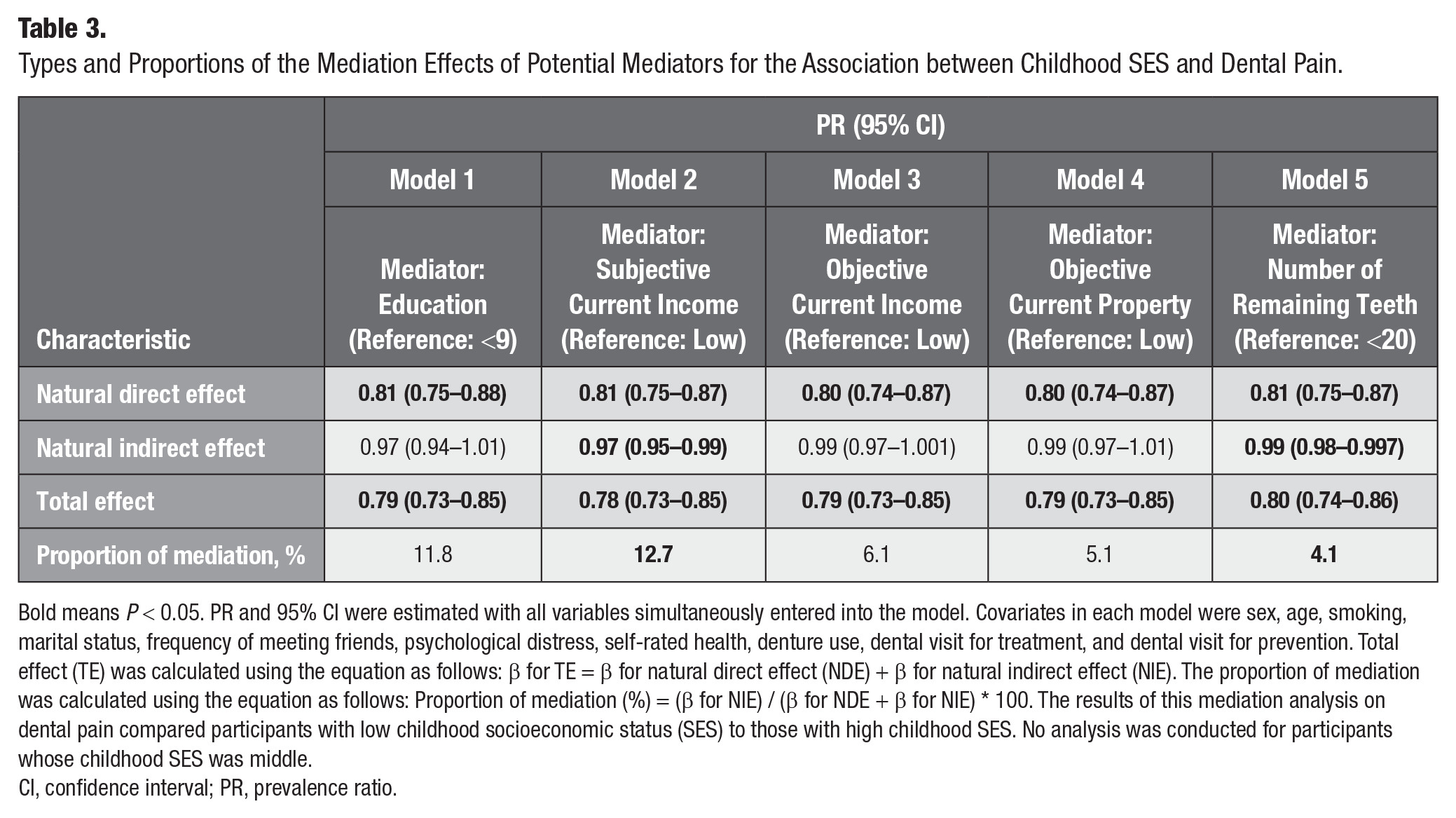
Bold means P < 0.05. PR and 95% CI were estimated with all variables simultaneously entered into the model. Covariates in each model were sex, age, smoking, marital status, frequency of meeting friends, psychological distress, self-rated health, denture use, dental visit for treatment, and dental visit for prevention. Total effect (TE) was calculated using the equation as follows: β for TE = β for natural direct effect (NDE) + β for natural indirect effect (NIE). The proportion of mediation was calculated using the equation as follows: Proportion of mediation (%) = (β for NIE) / (β for NDE + β for NIE) * 100. The results of this mediation analysis on dental pain compared participants with low childhood socioeconomic status (SES) to those with high childhood SES. No analysis was conducted for participants whose childhood SES was middle.
CI, confidence interval; PR, prevalence ratio.

The result of mediation analysis.
Discussion
To the best of our knowledge, this is the first study to show that childhood SES was associated with the prevalence of dental pain among older adults. Our findings are consistent with previous findings that investigated the association between childhood SES and resembling cumulative oral health indicators in older adults such as the number of remaining teeth (Listl et al. 2018) and tooth loss (Åstrøm et al. 2021). Moreover, our findings indirectly suggested the existence of other mechanisms than the current SES mechanism for the association between childhood SES and dental pain. First, the point estimates of childhood SES on dental pain are still robust after adjusting for the current SES in the model (Table 2, model 3), and the E-values were 1.36 (for middle SES) and 1.85 (for high SES). Our model may be robust even in the presence of an unmeasured confounder. Second, the proportion of the impact of childhood SES on dental pain that is mediated through either subsequent SES or the current number of remaining teeth was about 40% (Table 3, Fig. 2). A previous study suggested the impact of childhood SES on the number of remaining teeth in older adults, and education mediated nearly 80% of the relationship between the two (Yamamoto-Kuramoto et al. 2023). The magnitude of this mediating effect of SES in adulthood and older age differs from the results of our study focusing on dental pain. Third, our analysis showed that even after adjusting for the number of remaining teeth as a proxy for cumulative oral diseases across the life course, the point estimates for the impact of childhood SES on dental pain in older adults remained largely unchanged. Additionally, the pathway through which childhood SES affects dental pain in older adults via the number of remaining teeth accounted for 4.1% of the total effect. The series of results suggest the possibility of specific pathways between childhood SES and dental pain in older adults.
Based on previous observational studies, 1 mechanism that may explain the association between low childhood SES and dental pain in older age can be considered. Low SES at childhood was associated with children’s poor oral health status, including dental pain and caries (Nomura et al. 2004). Also, low childhood SES was associated with fewer dental visits (Da Silva et al. 2011). Refraining from dental visits accumulates untreated oral diseases and increases their severity, which prolongs the duration of dental visits for treatment and leads to more dental pain and loss of children’s educational opportunities by absence from school (Seirawan et al. 2012), which may negatively affect the SES in adulthood. In adulthood and later, those who belonged to low childhood SES groups had fewer dental visits than those who belonged to high childhood SES groups (Crocombe et al. 2011). Dental visits for treatment lead to absence from work, resulting in economic loss (Zaitsu et al. 2020). Additionally, worsening economic conditions limit dental visits, which is associated with the occurrence of dental pain. A previous study reported worsening economic conditions as a risk factor for dental pain during the COVID-19 pandemic (Matsuyama et al. 2021). Also, the economic condition among older adults influences their dental visits (Hoshi-Harada et al. 2022) and tooth loss (Cooray et al. 2021). This bidirectional association between low SES and dental pain may have contributed to poor oral health throughout the life course.
Considering the results of our study, while the possibility of pathways other than mechanisms involving subsequent SES was suggested, no previous study has provided a clear mechanism or sufficient evidence that low SES in childhood directly causes dental pain in older adults. Therefore, we extended the scope of previous studies focusing on general pain and explored mechanisms by which childhood SES affects dental pain in older age without involving subsequent SES. The biological programming model is a theory that suggests early socioeconomic and environmental exposures may have enduring effects on health outcomes (Barker and Osmond 1986). Several previous studies suggested that low SES in childhood increases vulnerability to pain. Low SES in childhood adversely affects later neurodevelopment (Hackman and Farah 2009) and increases the prevalence of musculoskeletal pain (Palermo 2020; Summers et al. 2021). The musculoskeletal pain itself also adversely affects neurodevelopment. A previous review article suggested that continuous nociceptive stimulation may alter pain-processing neural pathways, resulting in long-term anatomical and functional changes that increase vulnerability to pain (Bhatt et al. 2020; Palermo 2020). Adults with low SES also had lower pain thresholds than adults with high SES (Dorner et al. 2011). Just as childhood SES is associated with the susceptibility to pain, it may also influence the susceptibility to dental pain in older adults, independent of subsequent SES.
Another mechanism was also previously suggested to negatively influence neurodevelopment in childhood. Those under chronic stress caused by low childhood SES fall into a cumulative bodily strain known as allostatic load, which increases the stress-induced biological risk (Szanton et al. 2005; Seeman et al. 2010). Chronic stress worsens the oral environment through decreased saliva secretion (Tikhonova et al. 2018), increased bruxism (Chemelo et al. 2020), and so on. This may have increased vulnerability to dental pain throughout life. Additionally, the existence of stereotypes depicting low-SES individuals as “tough and resilient” suggests that low-SES people may not receive adequate pain management (Summers et al. 2021). In dental care, insufficient pain management practices, such as restrained use of analgesics, might have been employed, potentially subjecting individuals with low SES to continuous stress from inadequate treatment. Chronic stress states increase cortisol production, enhancing pain sensitivity (Knezevic et al. 2023), and may impair the body’s ability to regulate pain through the endogenous opioid system (Nakamoto and Tokuyama 2023), further contributing to increased pain sensitivity. The biological programming model and allostatic load may be related to dental pain inequalities throughout the life course.
The main implication of this study is that solely addressing later-life predictors of dental pain might not fully mitigate its impact stemming from childhood SES. At this stage, insufficient evidence proves a direct pathway by which childhood SES affects dental pain in older age. Therefore, future research, including biological or clinical studies, is required to elucidate the mechanisms by which childhood SES independently affects dental pain in older age.
A strength of this study was the use of a large Japanese gerontological survey data that included questions related to social determinants of health. We clarified the causal relationship between childhood SES and dental pain while considering the influence of socioeconomically related factors shown to confound resembling relationships in previous studies. However, this study has several limitations. First, the municipalities that participated in the JAGES survey were not randomly selected, limiting the generalizability of our findings. Also, the impact of childhood SES on dental pain in older age may be influenced by early-life conditions and health care access. When Japan introduced a national health insurance system in 1961 (Sakamoto et al. 2018), most participants in this study were around 15 y old. Therefore, many participants likely benefited from the protective effects on oral health provided by the national health insurance system in their adulthood. A previous study showed that oral health in Japan was better than in other countries due to this health insurance system (Aida et al. 2021). The prevalence of dental pain among older adults in Japan may also be lower than in other countries. Our findings may be influenced by the unique social and policy context of Japan. Caution should be exercised when applying these results to contexts outside of Japan. Second, because we used cross-sectional data, we cannot rule out the influence of recall bias on childhood SES responses. However, the validity of using childhood SES information gathered retrospectively has been confirmed in a life-course epidemiological study (Krieger et al. 1998). Third, we cannot rule out the possibility that the results are overestimated because we may not have adjusted for potential confounders like cumulative oral diseases. Our analysis showed that the combined indirect effect of all SES-related pathways and the number of remaining teeth on dental pain was only around 17% to 40%. This suggests that other factors may contribute to the association between childhood SES and dental pain in later life apart from current SES. Fourth, the findings may be influenced by age-related pain inequalities throughout the life course. Inequality of general pain across the life course has been suggested to peak in middle age and then decrease (Celeste and Fritzell 2018). Therefore, it was necessary to examine the possibility that age interacts with SES trajectory and dental pain in older age. In our study, the proportion of those in the persistent low-SES group was smaller in the older age groups (as shown in Appendix 2). Additionally, the point estimates of the interaction between age and the impact of SES trajectories on dental pain in older age did not show a significant association (as shown in Appendix 3). The previous study (Celeste and Fritzell 2018) suggests that, after middle age, age may act to reduce the pain inequalities associated with SES inequalities, which is consistent with our findings. However, we could not consider the survival bias due to the cross-sectional data. The interaction effect of age on the relationship between SES trajectories and dental pain in older age may be disrupted by survival bias, so the results should be interpreted cautiously. Further research is needed to determine whether inequality in dental pain, similar to general pain, also peaks in middle age. Finally, the dental pain used in this study was self-reported and its cause was unknown (caries, periodontal disease, hypersensitivity, etc.). However, other surveys have also used similar questions to identify dental pain (Santiago et al. 2013).
Conclusion
Childhood SES inequalities negatively affect dental pain long-term. Several studies, including biological and clinical research, will be necessary to elucidate the mechanisms explaining the relationship between childhood SES and dental pain in older adults.
Author Contributions
T. Yamamoto, J. Aida, contributed to conception and design, data analysis and interpretation, drafted the manuscript; U. Cooray, T. Kusama, S. Kiuchi, H. Abbas, contributed to data interpretation, critically revised the manuscript; K. Osaka, K. Kondo, contributed to data acquisition, critically revised the manuscript. All authors gave final approval and agreed to be accountable for all aspects of the work.
Supplemental Material
sj-docx-1-jct-10.1177_23800844241271740 – Supplemental material for Childhood Socioeconomic Status Affects Dental Pain in Later Life
Supplemental material, sj-docx-1-jct-10.1177_23800844241271740 for Childhood Socioeconomic Status Affects Dental Pain in Later Life by T. Yamamoto, U. Cooray, T. Kusama, S. Kiuchi, H. Abbas, K. Osaka, K. Kondo and J. Aida in JDR Clinical & Translational Research
Supplemental Material
sj-tif-2-jct-10.1177_23800844241271740 – Supplemental material for Childhood Socioeconomic Status Affects Dental Pain in Later Life
Supplemental material, sj-tif-2-jct-10.1177_23800844241271740 for Childhood Socioeconomic Status Affects Dental Pain in Later Life by T. Yamamoto, U. Cooray, T. Kusama, S. Kiuchi, H. Abbas, K. Osaka, K. Kondo and J. Aida in JDR Clinical & Translational Research
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by JSPS (Japan Society for the Promotion of Science) KAKENHI Grant Number (JP15H01972, JP23K16245), Health Labour Sciences Research Grant (H28-Choju-Ippan-002), Japan Agency for Medical Research and Development (AMED) (JP18dk0110027, JP18ls0110002, JP18le0110009, JP20dk0110034, JP21lk0310073, JP21dk0110037, JP22lk0310087, JP22rea522107), Open Innovation Platform with Enterprises, Research Institute and Academia (OPERA, JPMJOP1831) from the Japan Science and Technology (JST), a grant from Innovative Research Program on Suicide Countermeasures (1–4), a grant from Sasakawa Sports Foundation, a grant from Japan Health Promotion & Fitness Foundation, a grant from Chiba Foundation for Health Promotion & Disease Prevention, the 8020 Research Grant for fiscal 2019 from the 8020 Promotion Foundation (adopted number: 19–2- 06), and grants from Meiji Yasuda Life Foundation of Health and Welfare and the Research Funding for Longevity Sciences from National Center for Geriatrics and Gerontology (29–42, 30–22, 20–19, 21–20). The views and opinions expressed in this article are those of the authors and do not necessarily reflect the official policy or position of the respective funding organizations. The results of this study can be used by policymakers to promote policies based on a life-course approach that supports children living in communities with low SES and helps them maintain favorable oral health outcomes into their older age.
A supplemental appendix to this article is available online.
Data Availability Statement
The data that support the findings of this study were obtained from the JAGES data management committee and are not third-party data. Data are available upon reasonable request. Detailed information and all inquiries should be addressed to the JAGES data management committee via e-mail (
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.