
Abstract
Introduction:
The effectiveness of nonsurgical periodontal treatment is related to patient- and tooth-related factors. To overcome the limitations of the conventional approach, probiotics are one of the adjunct therapies that have been studied.
Objectives:
This umbrella review answered the focused question: in adult patients with periodontal diseases or peri-implant diseases, does the use of probiotic therapy as an adjuvant to nonsurgical periodontal treatment when compared with nonsurgical periodontal treatment alone affect treatment effectiveness and clinical disease parameters?
Methods:
A systematic electronic search to identify systematic reviews according to PICOS criteria, defined a priori, was used, and 5 electronic databases were searched (Medline, LILACS, Cochrane Central Registry of Controlled Trials, Google Scholar, and DANS EASY). Included systematic reviews were rated using quality assessment tools by 2 independent reviewers.
Results:
Thirty systematic reviews were identified evaluating the effectiveness of probiotics in periodontal and peri-implant disease treatment. A quantitative analysis of the results was not possible due to the high heterogeneity of clinical data. Seventeen of 31 reviews reported clinically relevant benefits of probiotic therapy as an adjuvant to scaling and root planning. Twenty-two reviews had a low risk of bias, 7 had a moderate risk, and 2 had a high risk.
Conclusion:
The evidence from the available studies is conflicting, which means that no definitive conclusions can be made about the effectiveness of probiotic therapy as an adjuvant to nonsurgical periodontal treatment. High-quality primary research studies are needed that control for known confounding variables.
Knowledge Transfer Statement:
This umbrella review provides some evidence regarding the efficacy of probiotics as an adjunct to nonsurgical periodontal therapy, despite some equivocal findings. However, short-term probiotic use alongside therapy appears to be advantageous; there is currently no evidence supporting their long-term benefits. We have also identified that probiotic research is primarily constrained by its origins in gastrointestinal applications, resulting in a lack of approved probiotics for dental use. This review highlights the need for extensive clinical research to ascertain their effectiveness in the oral environment. Nevertheless, the utilization of probiotics alongside periodontal treatment seems safe, with no reported adverse effects in patients. Thus, further clinical validations in oral health care settings are crucial.
Introduction
According to the World Health Organization, periodontal diseases are a major public oral health problem that affects systemic health (Salas and Palacios 2010; Seminario-Amez et al. 2017; Al-Nasser and Lamster 2020). The global prevalence of this disease is around 90% (Barboza et al. 2020), with its peak incidence in the fourth decade of life (Al-Nasser and Lamster 2020). Although periodontal diseases are not life-threatening, they can have a considerable effect on morbidity (Al-Nasser and Lamster 2020).
Previous studies have demonstrated that periodontal diseases have a polymicrobial etiology, but this by itself is not sufficient for disease development (Salas and Palacios 2010; Mdala et al. 2013). Periodontal diseases are caused by the interaction of the triad of the host, microorganisms, and environmental factors, which culminates in dysbiosis of the oral cavity (Salas and Palacios 2010; Donos et al. 2020).
The main objective of periodontal disease treatment is to reduce the burden of pathogenic microorganisms, thus restoring the symbiotic flora around tooth or implant surfaces (Suvan 2005; Tomasi et al. 2007; Martin-Cabezas et al. 2016; Matsubara et al. 2016; Donos et al. 2020). Scaling and root planing (SRP) are regarded as the primary therapeutic approach to achieve this in dental substrates (Martin-Cabezas et al. 2016). Local debridement, implant-surface decontamination, and anti-infective therapies are the conventional procedures for implant substrates (Arbildo-Vega et al. 2021). Despite the effectiveness of nonsurgical periodontal treatment (NSPT), its response varies between and within patients (Hung and Douglass 2002; Tomasi et al. 2007), depending on patient and tooth factors, such as deep probing depths, inaccessible root furcation, and interproximal areas of malposed teeth (Tomasi et al. 2007; Martin-Cabezas et al. 2016). For peri-implantitis, NSPT alone seems insufficient to restore peri-implant tissues, which in most cases needs surgical regenerative approaches (Chala et al. 2020).
Several adjuvant therapies have been developed to overcome the limitations complementing the conventional approach (Donos et al. 2020), including probiotics. Probiotics are defined by the World Health Organization and by the Food and Agriculture Organization of the United States as “live microorganisms which, when administered in adequate amounts confer a health benefit on the host”. (http://www.who.int/foodsafety/fs_management/en/probiotic_guidelines.pdf) (Teughels et al. 2008; Salas and Palacios 2010; Twetman and Keller 2012; Zarco et al. 2012; Laleman and Teughels 2015; Seminario-Amez et al. 2017). Probiotics purpose aims to restore the balance of the oral microbial ecological environment by increasing the proportion of beneficial bacteria through competitive inhibition of periodontal pathogens, thus modulating the subsequent host response (Caglar et al. 2005; Marcotte et al. 2006; Stamatova and Meurman 2009; Salas and Palacios 2010; Yanine et al. 2013).
The efficacy of probiotic therapy remains inconclusive due to the multitude of species and subspecies, as well as varying administration protocols. Systematic reviews (SRs) investigating probiotics as adjuncts to nonsurgical periodontal treatment yield inconsistent results: some support their use, while others deem it clinically irrelevant. Given the complexity of clinical decisions, grounded in high-quality evidence, understanding the relative risks and benefits of probiotic therapy is crucial. Clinical decisions should rely on secondary or tertiary evidence. An umbrella review systematically compiles evidence, consolidating it into an accessible document. It assesses topics with competing interventions, focusing on existing systematic reviews to provide practical recommendations, identify gaps, and guide future research, aiming to analyze existing knowledge and improve clinical practice.
For that purpose, this umbrella review aimed to answer the following focused question: in adult patients with periodontal diseases or peri-implant diseases, does the use of probiotic therapy as an adjuvant to nonsurgical periodontal treatment when compared with nonsurgical periodontal treatment alone affect the treatment effectiveness and clinical disease parameters?
Methods
Protocol Registration and Reporting Format
This umbrella review was reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Liberati et al. 2009) and previously registered in the International Prospective Register of Ongoing Systematic Reviews (PROSPERO; trial CRD42021254469).
Eligibility Criteria
Table 1 shows the main inclusion criteria for the PICOS question, including primary and secondary outcomes. We define probiotic therapy as the administration of a probiotic species either alone or in combination. There were no publication time or country restrictions; only systematic reviews published in English, Portuguese, Spanish, or French were included The exclusion criteria were as follows: 1) methodology not compatible with the systematic review according to the Cochrane Handbook for Systematic Reviews of Interventions definition (Higgins and Green 2011), 2) evaluating illnesses other than periodontal diseases, 3) including healthy periodontal patients, and 4) evaluating therapies different from probiotics.
Components of PICOS Question.

BOP, bleeding on probing; CAL, clinical attachment level; PPD, periodontal probing depth.
Information Sources and Searches
Five electronic databases were searched up to December 2022: Medline (via PubMed), LILACS, Cochrane Central Registry of Controlled Trials (CENTRAL), Google Scholar (first 300 references), and a database listing of unpublished studies (DANS EASY Archive available at https://doi.org/10.17026/dans-xtf-47w5). Detailed search strategies were adopted, combined with screening manual reference lists and contacting corresponding authors via email to ask about additional research work on the subject or knowledge of any accessible ongoing projects. The search strategy is presented in Appendix 2.
Study Selection and Data Extraction
Two reviewers independently screened titles and abstracts (when available) for eligibility based on the eligibility criteria and recorded detailed reasons for excluding studies. Full-text reports were obtained and reviewed for the included SRs and those with insufficient information in the title and abstract to make a clear decision. Two reviewers independently extracted data from the included SRs according to a predetermined datasheet form for systematic reviews from the Joanna Briggs Institute (JBI). The corresponding authors of potentially relevant articles or articles with data that needed further clarification were contacted via email and asked about missing data, additional research work on the subject, or if they were aware of any accessible ongoing projects.
Disagreements between the reviewers about the study selection and data collection were resolved through discussion until reaching a consensus. If necessary, a third reviewer was involved.
Risk of Bias in Individual Studies
The JBI Critical Appraisal tools for use in the JBI Systematic Reviews—Checklist for Systematic Reviews were applied to assess the methodologic quality of the included SRs. Two reviewers independently assessed the included SRs and scored each question (yes, unclear, no, not applicable). Any discrepancies were discussed until reaching a consensus. Cohen’s κ coefficients and asymptotic standard errors were used to evaluate the interrater agreement for individual questions and the overall score, considering the following κ interpretation: poor agreement, <0; slight agreement, 0.0 to 0.20; fair agreement, 0.21 to 0.40; moderate agreement, 0.41 to 0.60; substantial agreement, 0.61 to 0.80; and almost perfect agreement, 0.81 to 1.00 (Landis and Koch 1977). The final score of each SR was calculated based on the percentage of positive answers (yes) only. Each study’s risk of bias was subsequently categorized according to the final score as high (≤49%), moderate (50–69%), or low (≥70%) (Saletta et al. 2019).
Data Analysis and Synthesis of the Results
The included SRs were qualitatively synthesized, and summary tables were created with the measured effect for every SR or individual results from each SR successively. The results were categorized according to the specific outcome (primary and secondary) as clinically relevant (favors probiotic therapy) versus not clinically relevant (does not favor probiotic therapy) and separated by substrate (tooth or implant).
Results
Study Selection
Appendix 3 shows a flow diagram of the article screening process for inclusion in the review. The combined electronic search identified 2,660 articles, with 53 articles included for full-text review. In turn 2, 23 studies were excluded for not meeting the inclusion criteria (Appendix 4). Two additional records were identified through a manual search of the relevant studies’ references, resulting in 30 SRs accepted for qualitative evaluation, 1 unpublished work, and 1 protocol.
Study Characteristics
Table 2 summarizes the characteristics of the included SRs (Teughels et al. 2011; Yanine et al. 2013; Gruner et al. 2016; Jayaram et al. 2016; Martin-Cabezas et al. 2016; Matsubara et al. 2016; Priyanka et al. 2016; Seminario-Amez et al. 2017; Ikram et al. 2018; Akram et al. 2020; Barboza et al. 2020; Barootchi et al. 2020; Donos et al. 2020; Gao et al. 2020; Ho et al. 2020; Silva et al. 2020; Song and Liu 2020; Vives-Soler and Chimenos-Kustner 2020; Abdulkareem et al. 2021; Arbildo-Vega et al. 2021; Canut-Delgado et al. 2021; Corbella et al. 2021; Hu et al. 2021; Mishra et al. 2021; Saïz et al. 2021; Gheisary et al. 2022; Hardan et al. 2022; Liu et al. 2022; Ng et al. 2022; Sayardoust et al. 2022). Twenty-two SRs assessed adjuvant probiotic therapy in periodontitis treatment (Teughels et al. 2011; Yanine et al. 2013; Gruner et al. 2016; Jayaram et al. 2016; Martin-Cabezas et al. 2016; Matsubara et al. 2016; Priyanka et al. 2016; Seminario-Amez et al. 2017; Ikram et al. 2018; Donos et al. 2020; Ho et al. 2020; Song and Liu 2020; Vives-Soler and Chimenos-Kustner 2020; Abdulkareem et al. 2021; Canut-Delgado et al. 2021; Corbella et al. 2021; Hu et al. 2021; Mishra et al. 2021; Gheisary et al. 2022; Hardan et al. 2022; Ng et al. 2022), with 6 SRs in gingivitis treatment (Yanine et al. 2013; Jayaram et al. 2016; Priyanka et al. 2016; Akram et al. 2020; Barboza et al. 2020; Liu et al. 2022). Five SRs evaluated peri-implantitis treatment (Barootchi et al. 2020; Gao et al. 2020; Silva et al. 2020; Arbildo-Vega et al. 2021; Sayardoust et al. 2022) and 1 SR in oral health treatment in general (related to periodontal disease) (Saïz et al. 2021).
Main Characteristics of Included Systematic Reviews.

Aa, Aggregatibacter actinomycetemcomitans; BI, bleeding index; BOP, bleeding on probing; CAL, clinical attachment level; CFU, colony-forming units; CP, chronic periodontitis; Fn, Fusobacterium nucleatum; GBI, gingival bleeding index; GCF, gingival crevicular fluid; GI, gingival index; HM, host modulator; IL, interleukin; LB, Lactobacillus; LR, Lactobacillus reuteri; MA, meta-analysis; mGI, modified gingival index; NSAID, nonsteroidal anti-inflammatory drug; NSPT, nonsurgical periodontal treatment; Pg, Porphyromonas gingivalis; Pi, Prevotella intermedia; PI, plaque index; PD, peri-implant diseases; PPD, periodontal probing depth/probing pocket depth; RCT, randomized controlled trial; REC, gingival recession; SD, subgingival debridement; SM, Streptococcus mutans; SR, systematic review; SRP, scaling and root planning; Tf, Tannerella forsythia. y, year.
Five SRs evaluated Lactobacillus reuteri individually (Martin-Cabezas et al. 2016; Silva et al. 2020; Song and Liu 2020; Arbildo-Vega et al. 2021; Sayardoust et al. 2022), and 4 SRs assessed a combination of Lactobacillus reuteri and other 2 subspecies of Lactobacillus (brevis, planatarum, salivarus, or casei) (Yanine et al. 2013; Ikram et al. 2018; Barootchi et al. 2020; Gao et al. 2020). Twenty SRs analyzed the effectiveness of a combination of different species and subspecies of probiotics, such as Lactobacillus, Bifidobacterium, Streptococcus, Bacillus, Clostridium, Saccharomyces, and Pediococcus (Teughels et al. 2011; Gruner et al. 2016; Jayaram et al. 2016; Matsubara et al. 2016; Priyanka et al. 2016; Seminario-Amez et al. 2017; Akram et al. 2020; Barboza et al. 2020; Donos et al. 2020; Ho et al. 2020; Vives-Soler and Chimenos-Kustner 2020; Abdulkareem et al. 2021; Corbella et al. 2021; Hu et al. 2021; Mishra et al. 2021; Saïz et al. 2021; Gheisary et al. 2022; Hardan et al. 2022; Liu et al. 2022; Ng et al. 2022). One SR did not report the probiotic species (Canut-Delgado et al. 2021).
Risk of Bias within Included Studies
The Cohen’s κ interrater reliability for the 31 SRs subjected to the JBI Critical Appraisal tool was 0.95 (P = 0.018), considered an almost perfect agreement. After the overall appraisal, no SR was excluded. However, 6.4% of the studies (2) scored 49% or less, with eligibility criteria definition and search strategy as the most concerning items. See the detailed appraisal rating for randomized controlled trials (RCTs) included in the considered SRs in Appendix 5.
Results of Individual Studies
Table 3 summarizes the results of individual SRs. The studies ranged in the period of administration of the probiotic therapy from a single dose (Teughels et al. 2011) to 6 months (Silva et al. 2020). The follow-up period ranged from 1 day (Teughels et al. 2011) to 9 years (Gruner et al. 2016). The included SRs reported no clinical data about bone loss around teeth or implants, implant survival rate, and tooth loss outcomes. Sixteen SRs advocated the clinically relevant effect of probiotic therapy as an adjuvant to SRP for treating periodontal disease (Martin-Cabezas et al. 2016; Matsubara et al. 2016; Priyanka et al. 2016; Seminario-Amez et al. 2017; Ikram et al. 2018; Barboza et al. 2020; Song and Liu 2020; Vives-Soler and Chimenos-Kustner 2020; Arbildo-Vega et al. 2021; Canut-Delgado et al. 2021; Hu et al. 2021; Mishra et al. 2021; Saïz et al. 2021; Gheisary et al. 2022; Hardan et al. 2022; Ng et al. 2022). Twelve SRs did have low risk of bias (Martin-Cabezas et al. 2016; Matsubara et al. 2016; Ikram et al. 2018; Barboza et al. 2020; Song and Liu 2020; Arbildo-Vega et al. 2021; Hu et al. 2021; Mishra et al. 2021; Gheisary et al. 2022; Hardan et al. 2022; Ng et al. 2022), 4 did have moderate risk of bias (Priyanka et al. 2016; Vives-Soler and Chimenos-Kustner 2020; Canut-Delgado et al. 2021; Saïz et al. 2021), and 1 had a high risk of bias (Seminario-Amez et al. 2017). The probiotic therapy administration period in the included studies ranged from a single dose (Hu et al. 2021) to 7 months (Seminario-Amez et al. 2017). The follow-up period ranged from 4 days (Barboza et al. 2020) to 4 years (Seminario-Amez et al. 2017).
Results of Individual Studies.

Aa, Aggregatibacter actinomycetemcomitans; BI, bleeding index; BOP, bleeding on probing; CAL, clinical attachment level; CFU, colony-forming units; CI, confidence interval; Fn, Fusobacterium nucleatum; GCF, gingival crevicular fluid; GI, gingival index; IL, interleukin; LB, Lactobacillus; LR, Lactobacillus reuteri; MD, mean difference; MMP, metalloproteinase; NR, not reported; NSPT, nonsurgical periodontal treatment; OR, odds ratio; Pg, Porphyromonas gingivalis; Pi, Prevotella intermedia; PI, plaque index; PD, periodontal diseases; PPD, periodontal probing depth/probing pocket depth; RCT, randomized controlled trial; SMD, standardized mean difference; SRP, scaling and root planning; Tf, Tannerella forsythia; WMD, weighted mean difference; d, day; mo, month; wk, week; y, year.
Fourteen SRs detected no clinically relevant effects of probiotic therapy as an adjuvant to SRP (Teughels et al. 2011; Yanine et al. 2013; Gruner et al. 2016; Jayaram et al. 2016; Akram et al. 2020; Barootchi et al. 2020; Donos et al. 2020; Gao et al. 2020; Ho et al. 2020; Silva et al. 2020; Abdulkareem et al. 2021; Corbella et al. 2021; Liu et al. 2022; Sayardoust et al. 2022). With regards to the quality assessment, 10 SRs had a low risk of bias (Yanine et al. 2013; Gruner et al. 2016; Akram et al. 2020; Barootchi et al. 2020; Donos et al. 2020; Gao et al. 2020; Ho et al. 2020; Silva et al. 2020; Corbella et al. 2021; Liu et al. 2022). Three had a moderate risk of bias (Teughels et al. 2011; Jayaram et al. 2016; Sayardoust et al. 2022) and 1 SR had high risk of bias (Abdulkareem et al. 2021).
Primary outcomes
Studies showing a positive effect of probiotic therapy as an adjuvant on periodontal probing depth
Fourteen SRs published data on the short-term effects of the probiotics on periodontal probing depth (PPD) reduction in both tooth (Martin-Cabezas et al. 2016; Matsubara et al. 2016; Priyanka et al. 2016; Ikram et al. 2018; Song and Liu 2020; Vives-Soler and Chimenos-Kustner 2020; Canut-Delgado et al. 2021; Hu et al. 2021; Mishra et al. 2021; Gheisary et al. 2022; Hardan et al. 2022; Ng et al. 2022) and implant substrates (Vives-Soler and Chimenos-Kustner 2020; Arbildo-Vega et al. 2021). Lactobacillus reuteri was the subspecies that showed the best effects on this clinical parameter (Priyanka et al. 2016; Arbildo-Vega et al. 2021). One SR showed a reduction in PPD with Lactobacillus treatment and no differences between coadjuvant treatment with Streptococcus probiotics and conventional mechanical treatment alone (Matsubara et al. 2016).
The outcomes on tooth substrate, from a 1 month follow-up, did not detect any clinical benefits (Ikram et al. 2018). Nine studies revealed a significant favorable response to SRP + probiotics in PPD reduction at the 3 months follow-up (Martin-Cabezas et al. 2016; Matsubara et al. 2016; Priyanka et al. 2016; Song and Liu 2020; Hu et al. 2021; Mishra et al. 2021; Gheisary et al. 2022; Hardan et al. 2022; Ng et al. 2022); this was more significant when pockets were divided according to depth (moderate and severe) (Martin-Cabezas et al. 2016; Vives-Soler and Chimenos-Kustner 2020; Canut-Delgado et al. 2021; Hu et al. 2021). However, SRs also suggested that mid-term results were not as favorable, with a less significant PPD reduction in the probiotic groups than in the control/placebo groups at the 6 months follow-up (Song and Liu 2020; Hu et al. 2021; Ng et al. 2022).
The outcomes on implant substrates showed PPD improvement in the probiotic groups, although not always achieving statistical significance (Arbildo-Vega et al. 2021). Moreover, PPD showed significant statistical heterogeneity among primary studies in the 3- and 6 months analyses.
Heterogeneity (I2) ranged from 63% (Gheisary et al. 2022) to 99% (Song and Liu 2020; Mishra et al. 2021) in the different studies. The lowest percentage was associated with a shorter follow-up period.
Studies showing no effect of probiotic therapy as an adjuvant on PPD
Eleven SRs reported no statistically significant short-term effects of using probiotics as an adjuvant on PPD reduction in both tooth(Teughels et al. 2011; Gruner et al. 2016;Jayaram et al. 2016; Donos et al. 2020; Ho et al. 2020; Abdulkareem et al. 2021; Corbella et al. 2021) and implant (Barootchi et al. 2020; Gao et al. 2020; Silva et al. 2020; Sayardoust et al. 2022) substrates. The overall effect of the coadjuvant therapy did not show a clinically relevant improvement on tooth substrates’ clinical parameters (Donos et al. 2020; Ho et al. 2020; Corbella et al. 2021). One SR that included both smokers and animal studies found a significant PPD improvement in smokers and no significant benefit in animals due to the lack of oral hygiene habits, respectively (Teughels et al. 2011). In mucositis and peri-implantitis, 4 SRs showed a PPD reduction of approximately 0.4 mm after treatment completion but did not indicate significant clinical effects of probiotic therapy (Barootchi et al. 2020; Gao et al. 2020; Silva et al. 2020; Sayardoust et al. 2022).
Studies showing a positive effect of probiotic therapy as an adjuvant on clinical attachment level
Ten SRs published findings on the short-term effect of adjuvant probiotics on clinical attachment level (CAL) gain in tooth substrates (Martin-Cabezas et al. 2016; Matsubara et al. 2016; Ikram et al. 2018; Song and Liu 2020; Canut-Delgado et al. 2021; Hu et al. 2021; Mishra et al. 2021; Gheisary et al. 2022; Hardan et al. 2022). Patients with chronic periodontitis under probiotic therapy adjuvant to SRP attained CAL gain in the 1- and 3 months follow-up (Ikram et al. 2018; Song and Liu 2020; Hu et al. 2021; Mishra et al. 2021; Gheisary et al. 2022; Hardan et al. 2022). This was more significant when pockets were divided according to depth (moderate [Martin-Cabezas et al. 2016; Matsubara et al. 2016] and severe [Martin-Cabezas et al. 2016; Matsubara et al. 2016]). There was no evidence of significant CAL gain after 6 months (Hu et al. 2021).
Heterogeneity ranged from 62% to 97% in the included studies at the 3- and 6-mo follow-ups, respectively.
Studies showing no effect of probiotic therapy as an adjuvant on CAL
Nine SRs reported found no effect on using probiotics as an adjuvant on the short-term effect on CAL gain in tooth substrates (Teughels et al. 2011; Yanine et al. 2013; Gruner et al. 2016; Jayaram et al. 2016; Priyanka et al. 2016; Donos et al. 2020; Ho et al. 2020; Abdulkareem et al. 2021; Corbella et al. 2021). Seven SRs found no significant differences in CAL in the groups with probiotic adjuvant therapy (Teughels et al. 2011; Yanine et al. 2013; Gruner et al. 2016; Priyanka et al. 2016; Donos et al. 2020; Ho et al. 2020; Corbella et al. 2021). One SR reported no significant differences in CAL gain due to including smokers and animals in the studies and not adjusting for smoking habits and oral hygiene (Teughels et al. 2011).
The results for CAL outcomes were coherent with PPD data, with a significant benefit observed at 3 months but not at 6 months (Ho et al. 2020; Corbella et al. 2021). SRs found a positive effect of probiotics at 12 months (Ho et al. 2020; Corbella et al. 2021). However, the heterogeneity for this outcome, although smaller than for the PPD outcome, was still considerable, ranging from 0% (Gruner et al. 2016) to 96% (Ho et al. 2020). Like PPD outcome, the subspecies Lactobacillus reuteri was the most effective in improving this clinical parameter than other probiotics (Corbella et al. 2021).
Studies showing a positive effect of probiotic therapy as an adjuvant on bleeding on probing
Twelve SRs reported on the short-term effects of probiotics as an adjuvant on bleeding on probing (BOP) reduction in both tooth (Gruner et al. 2016; Martin-Cabezas et al. 2016; Matsubara et al. 2016; Priyanka et al. 2016; Vives-Soler and Chimenos-Kustner 2020; Canut-Delgado et al. 2021; Hu et al. 2021; Gheisary et al. 2022; Hardan et al. 2022) and implant (Silva et al. 2020; Vives-Soler and Chimenos-Kustner 2020; Arbildo-Vega et al. 2021) substrates.
For the tooth substrate, BOP reduction was higher in groups under NSPT + probiotic therapy (Gruner et al. 2016; Martin-Cabezas et al. 2016; Matsubara et al. 2016; Priyanka et al. 2016; Vives-Soler and Chimenos-Kustner 2020; Canut-Delgado et al. 2021; Hu et al. 2021; Gheisary et al. 2022; Hardan et al. 2022), remaining stable in the first year of follow-up (Matsubara et al. 2016). Similar to PPD and CAL outcomes, significant BOP reduction was also demonstrated at 3 months, but the studies reporting outcomes at 6 months were conflicting (Hu et al. 2021). The BOP outcome for Lactobacillus was positive but not for Streptococcus (Matsubara et al. 2016). Moreover, BOP outcomes were better with the bleeding index of Saxton (Vives-Soler and Chimenos-Kustner 2020).
For the implant substrate, the differences were not significant between groups for all studies (Silva et al. 2020; Vives-Soler and Chimenos-Kustner 2020; Arbildo-Vega et al. 2021).
Studies showing no effect of probiotic therapy as an adjuvant on BOP
Ten SRs published outcomes showing no positive effect on the short-term effect on BOP reduction in both tooth (Teughels et al. 2011; Yanine et al. 2013; Jayaram et al. 2016; Akram et al. 2020; Barboza et al. 2020; Abdulkareem et al. 2021; Liu et al. 2022) and implant substrates (Barootchi et al. 2020; Gao et al. 2020; Sayardoust et al. 2022).
For the tooth substrate, the overall effect of the coadjuvant therapy did not show clinically significant differences in BOP (Teughels et al. 2011; Jayaram et al. 2016; Barboza et al. 2020; Liu et al. 2022). Yanine et al. (2013) found that this was related to different BOP measurements. The included SRs lacked clinical data on this outcome (Akram et al. 2020). There was also considerable heterogeneity, with 1 study reporting significant heterogeneity that compromised the performance of a meta-analysis (Akram et al. 2020) and another not reporting the existence of heterogeneity (Liu et al. 2022).
In the implant substrate, adjuvant probiotics did not significantly reduce BOP around the implant (Barootchi et al. 2020; Gao et al. 2020), even with the Lactobacillus probiotic species (Gao et al. 2020). One SR found a significant beneficial effect of probiotic therapy on BOP reduction (Sayardoust et al. 2022).
Secondary outcomes
Studies showing a positive effect of probiotic therapy as an adjuvant on microbiological analysis
Six SRs reported studies showing the positive effect of using probiotics as an adjuvant on reducing periodontal pathogen on at tooth substrates (Song and Liu 2020; Vives-Soler and Chimenos-Kustner 2020; Canut-Delgado et al. 2021; Mishra et al. 2021; Saïz et al. 2021; Gheisary et al. 2022) and implant (Saïz et al. 2021). The periodontal pathogen reduction was significantly higher in the groups under SRP + probiotic therapy (Song and Liu 2020; Vives-Soler and Chimenos-Kustner 2020; Canut-Delgado et al. 2021; Mishra et al. 2021; Saïz et al. 2021). The pathogens evaluated were Aggregatibacter actinomycetemcomitans in 4 SRs (Song and Liu 2020; Vives-Soler and Chimenos-Kustner 2020; Canut-Delgado et al. 2021; Mishra et al. 2021), Porphyromonas gingivalis in 5 SRs (Song and Liu 2020; Vives-Soler and Chimenos-Kustner 2020; Canut-Delgado et al. 2021; Mishra et al. 2021; Gheisary et al. 2022), Prevotella intermedia in 3 SRs (Song and Liu 2020; Vives-Soler and Chimenos-Kustner 2020; Canut-Delgado et al. 2021), Treponema denticola in 1 SR (Canut-Delgado et al. 2021), Fusobacterium nucleatum in 2 SRs (Canut-Delgado et al. 2021; Gheisary et al. 2022), and Tannerella forsythia in 1 SR (Gheisary et al. 2022). P. gingivalis reduction was observed at 12 weeks, while A. actinomycetemcomitans reduction occurred at 3 weeks of follow-up (Mishra et al. 2021). The heterogeneity for A. actinomycetemcomitans was moderate (0%–74%) and for P. gingivalis was substantial (96%–97%) (Mishra et al. 2021).
Studies showing no effect of probiotic therapy as an adjuvant on microbiological analysis
Eight SRs reported no short-term effects of adjuvant probiotics on periodontal pathogen reduction in both tooth substrates (Teughels et al. 2011; Gruner et al. 2016; Seminario-Amez et al. 2017; Ho et al. 2020; Liu et al. 2022; Ng et al. 2022) and implant substrates (Silva et al. 2020; Sayardoust et al. 2022). Most SRs did not identify significant differences when NSPT was combined with probiotics (Teughels et al. 2011; Gruner et al. 2016; Seminario-Amez et al. 2017; Ho et al. 2020; Liu et al. 2022; Ng et al. 2022). The pathogens evaluated were A. actinomycetemcomitans in 2 SRs (Gruner et al. 2016; Liu et al. 2022), P. gingivalis in 2 SRs (Gruner et al. 2016; Liu et al. 2022), P. intermedia in 2 SRs (Gruner et al. 2016; Liu et al. 2022), and F. nucleatum in 1 SR (Liu et al. 2022). No significant heterogeneity was found (Liu et al. 2022). The findings in mucositis and peri-implantitis showed a very limited effect of probiotics on the peri-implant microbiota (Silva et al. 2020; Sayardoust et al. 2022).
Influence of systemic diseases
Twenty-three SRs (Teughels et al. 2011; Gruner et al. 2016; Jayaram et al. 2016; Matsubara et al. 2016; Priyanka et al. 2016; Seminario-Amez et al. 2017; Ikram et al. 2018; Akram et al. 2020; Barboza et al. 2020; Barootchi et al. 2020; Donos et al. 2020; Gao et al. 2020; Ho et al. 2020; Vives-Soler and Chimenos-Kustner 2020; Abdulkareem et al. 2021; Arbildo-Vega et al. 2021; Corbella et al. 2021; Hu et al. 2021; Mishra et al. 2021; Saïz et al. 2021; Gheisary et al. 2022; Hardan et al. 2022; Sayardoust et al. 2022) did not consider the influence of systemic disease as an eligibility criterion while 7 SRs (Yanine et al. 2013; Martin-Cabezas et al. 2016; Silva et al. 2020; Song and Liu 2020; Canut-Delgado et al. 2021; Liu et al. 2022; Ng et al. 2022) considered it as an exclusion criterion on the recruitment phase. The only SR (Corbella et al. 2021) that divided the results by healthy and systemically compromised patients reported no relevant randomized controlled trial where NSPT was combined with adjuvant probiotic therapy in systemically compromised subjects.
Table 4 summarizes the findings of the included SRs.
Summary of Findings.
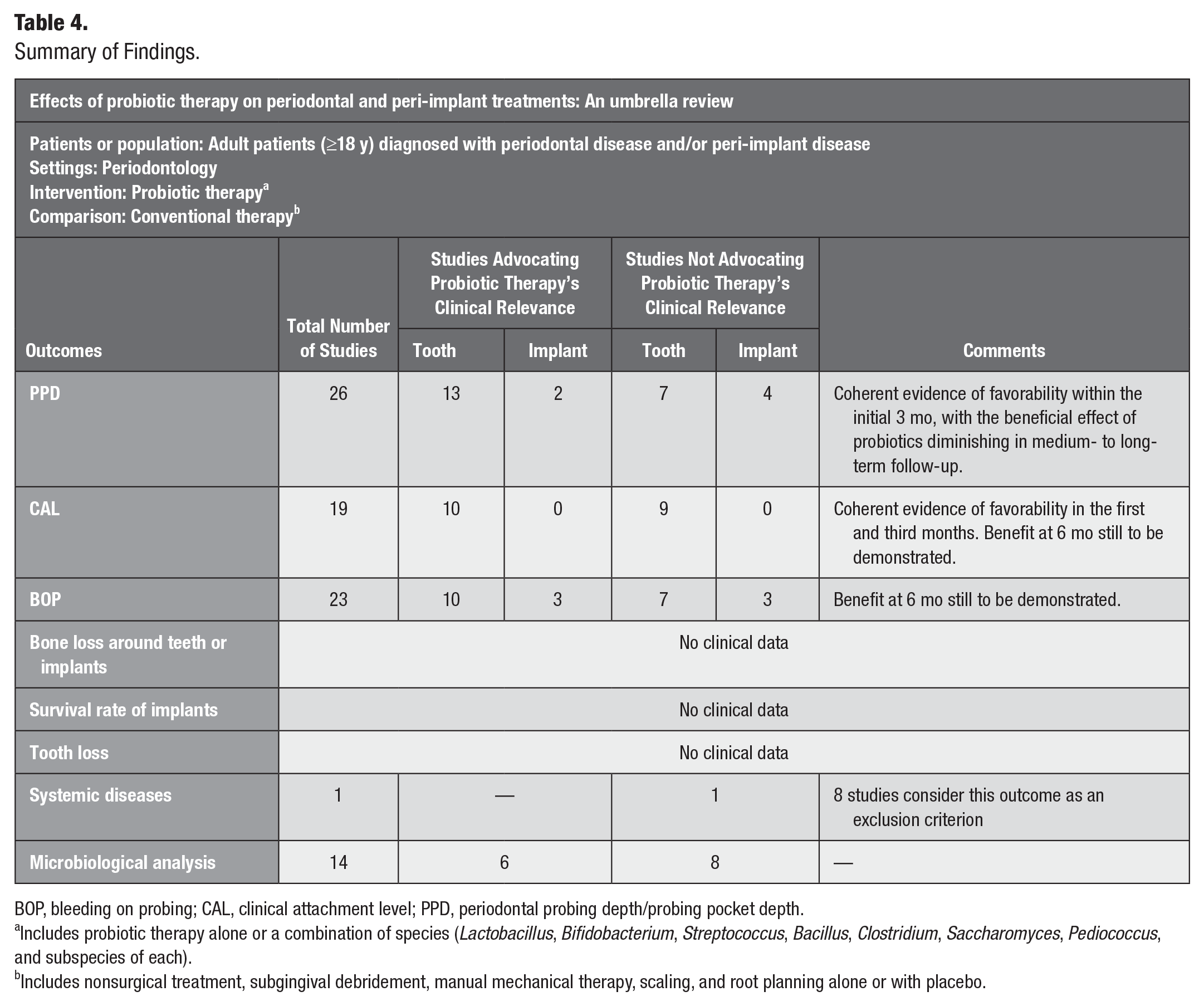
BOP, bleeding on probing; CAL, clinical attachment level; PPD, periodontal probing depth/probing pocket depth.
Includes probiotic therapy alone or a combination of species (Lactobacillus, Bifidobacterium, Streptococcus, Bacillus, Clostridium, Saccharomyces, Pediococcus, and subspecies of each).
Includes nonsurgical treatment, subgingival debridement, manual mechanical therapy, scaling, and root planning alone or with placebo.
Discussion
Summary of the Main Findings
This umbrella review included 30 SRs (Teughels et al. 2011; Yanine et al. 2013; Gruner et al. 2016; Jayaram et al. 2016; Martin-Cabezas et al. 2016; Matsubara et al. 2016; Priyanka et al. 2016; Seminario-Amez et al. 2017; Ikram et al. 2018; Akram et al. 2020; Barboza et al. 2020; Barootchi et al. 2020; Donos et al. 2020; Gao et al. 2020; Ho et al. 2020; Silva et al. 2020; Song and Liu 2020; Vives-Soler and Chimenos-Kustner 2020; Abdulkareem et al. 2021; Arbildo-Vega et al. 2021; Canut-Delgado et al. 2021; Corbella et al. 2021; Hu et al. 2021; Mishra et al. 2021; Saïz et al. 2021; Gheisary et al. 2022; Hardan et al. 2022; Liu et al. 2022; Ng et al. 2022; Sayardoust et al. 2022). A quantitative analysis of the results was not possible due to the high heterogeneity of clinical data.
Despite there being 30 previously published SRs, the evidence on the effectiveness of using probiotics as an adjuvant to conventional NSPT is still uncertain. In the included SRs, the short- and mid-term success of probiotics was determined, but their effect in the long term is still unclear. The SRs showed that long-term benefits were not evident at the 6 months evaluation (Song and Liu 2020; Hu et al. 2021; Ng et al. 2022). There is considerable heterogeneity in the variety of probiotic subspecies, probiotic regimens, and treatment protocols. However, a longer probiotic administration period seemed to be associated with prolonged maintenance of the probiotics’ effects on clinical parameters. The Lactobacillus species with reuteri subspecies produced the best improvement in the clinical parameters (Priyanka et al. 2016; Arbildo-Vega et al. 2021; Corbella et al. 2021).
Limitations of the Review and Importance on Clinical Practice and Research
Since this umbrella review included SRs, its limitations are directly related to those of the included SRs and, subsequently, the corresponding primary studies. Eighty-one percent of SRs had been reported as per the recommended PRISMA guidelines, and 29% had a risk of bias between moderate and high. This can be attributed to certain common methodological limitations such as the lack of a definition of a standardized treatment protocol, the lack of knowledge of the most effective probiotic combinations, the most appropriate probiotic vehicle, and the frequency of administration, and thus the probiotics’ clinical benefits on clinical parameters must be interpreted with caution. The main reason for conflicting evidence among the included studies was the variety in probiotic subspecies, probiotic regimens, chronic periodontitis definitions in primary studies, treatment protocols, follow-up periods, inclusion criteria (like smoking habits), and sample sizes. These aspects compromise the heterogeneity among the included primary studies of the SRs, often preventing a meta-analysis of the results.
These limitations hinder probiotic use in clinical practice, despite potential benefits on periodontal health.
Future Directions and/or Recommendations
The findings of this umbrella review highlight the need for future research in this field, focusing on RCTs with extended follow-up periods, 1 year at minimum, to better understand the sustained effects of probiotics. RCTs should strive for uniformity in the route of probiotic administration to ensure a consistent and commensurate basis for assessment; should engage in a comparative analysis to discern the advantages between protocols employing single probiotic species and those using a combination of probiotics, thereby ascertaining the most efficacious approach; and ought to standardize the methodologies for collecting clinical data related to periodontal outcomes, thereby enhancing the comparability and reliability of the obtained results.
Conclusion
Based on the available evidence, the results are conflicting, and there can be no definitive conclusion for or against probiotics. Future studies controlling for all the confounding variables mentioned are needed.
Author Contributions
C. Mendonça, contributed to conception, design, data acquisition, analysis, and interpretation, drafted the manuscript; D. Marques, contributed to conception, design, data interpretation, critically revised the manuscript; J. Silveira, J. Marques, contributed to conception, design, critically revised the manuscript; R.F. de Souza, contributed to data analysis, and interpretation, critically revised the manuscript; A. Mata, contributed to conception, design, data analysis, critically revised the manuscript. All authors have their final approval and agree to be accountable for all aspects of work.
Supplemental Material
sj-pdf-1-jct-10.1177_23800844241240474 – Supplemental material for Effects of Probiotic Therapy on Periodontal and Peri-implant Treatments: An Umbrella Review
Supplemental material, sj-pdf-1-jct-10.1177_23800844241240474 for Effects of Probiotic Therapy on Periodontal and Peri-implant Treatments: An Umbrella Review by C. Mendonça, D. Marques, J. Silveira, J. Marques, R.F. de Souza and A. Mata in JDR Clinical & Translational Research
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was self-funded by Center for Evidence-Based Dental Medicine, Faculty of Dental Medicine of the University of Lisbon.
A supplemental appendix to this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.