
Abstract
Introduction:
Public service provision is one of the keys to reducing inequalities in the utilization of dental services. Given the increase in the aging population, there should be a focus on older adults’ oral health. However, this is often overlooked.
Objectives:
This study investigates the effectiveness of public services in reducing income-related inequalities in dental service utilization among older South Australians.
Methods:
A multiple counterfactual mediation analysis using the ratio of mediator probability weighting approach was used to explore the proposed mediation mechanism using a South Australian population of older adults (≥65 y). The exposure variable in the analysis was income, and the mediators were concession cards and the last dental sector (public or private). The outcome variable was the time of last dental visit.
Results:
Half of the older adults with high income (≥$40,000) owned a concession card, and 10% of those who attended public dental services belonged to this group. Interestingly, only 16.3% of the study participants had visited the public dental sector at their last dental appointment. Results showed a negligible indirect effect (odds ratio [OR], 0.99; 95% confidence interval [CI], 0.85–1.05) and a significant direct effect (OR, 3.09; 95% CI, 2.24–4.87). By changing the potential outcome distributions to the counterfactual exposure distributions and taking the mediators’ distribution as a counterfactual exposure distribution, the odds of dental visits occurring before the past 12 mo approximately tripled for low-income compared to high-income individuals.
Conclusion:
Income inequalities were associated with relatively delayed dental visits in older South Australians, and provision of public services could not improve this pattern. This might happen due to inequitable access to concession cards and public services. A review of policies is required, including addressing income inequalities and implementing short-term approaches to improve service utilization patterns in older South Australians.
Knowledge Transfer Statement:
The findings of this study can enable policymakers for informed decision-making about the provision of public dental services for older Australians. This study emphasizes the importance of reviewing the current public dental services and subsidies and implementing short-term approaches to reduce income inequalities for older Australians.
Keywords
Introduction
The global population of older adults is expected to exceed 2 billion by 2050, which is more than double the number of individuals aged 60 y or older in 2017. In 1950, there were approximately 668,000 (8%) Australians aged 65 y or over, which increased to 3.6 million (15%) by 2015. This trend is consistent with global patterns, and modeling suggests that by 2050, the number of older Australian adults will reach 7.5 million, accounting for 23% of the population (Australian Bureau of Statistics 2016; United Nations 2017).
Considering this demographic shift, reducing the burden of diseases in the elderly becomes crucial in tackling social inequalities. Among the most prevalent chronic diseases in older adults are oral and dental diseases, which should be considered a priority need (Petersen and Ogawa 2018). However, dental benefit packages often focus on preventive and restorative services for children, minority groups, and pregnant women, with no specific policy targeting older adults in Australia’s 2015–2024 Oral Health Plan (Council of Australian Governments 2014).
The triangle of inequalities in dental services concept model (Ghanbarzadegan et al. 2022) provides insights into the factors influencing access and utilization of dental services. This model proposes a hierarchical relationship between health policies and service provision. At the top of the hierarchy, health policies define the context of service provision through the availability of services and subsidies, which then leads to access and utilization of services. The model acknowledges that various barriers can hinder access and utilization of dental services. These barriers may include cultural factors, geographical constraints, financial limitations, long waiting lists, and other individual or contextual elements. Overcoming these barriers becomes crucial in improving access to dental services and promoting better service utilization.
When these barriers are effectively addressed and minimized, the provision of dental services with the availability of resources such as public services and subsidies can lead to increased access to care and subsequently better utilization of dental services by the population in need. However, this is not the case in Australia, where the government subsidies for oral health are minimal, and public dental services are limited, with only 20% of eligible adults receiving them due to various access barriers (Australian Institute of Health and Welfare 2020). For instance, in South Australia, only individuals with health care or pensioner cards issued by the Australian government’s Department of Veterans’ Affairs or Centrelink are eligible to receive public dental services. Concession cards are markers of low income and associated inequalities (South Australia Health 2021). Recent evidence suggests that the level of support provided through concession cards as eligibility criteria to receive public dental services was not effective in reducing the financial burden associated with the utilization of oral dental services (Ghanbarzadegan et al. 2023).
The issue of income inequality is of great concern for the over 6.7 million individuals residing in rural and remote areas of Australia. Access to health care services, housing, and education in these regions are also pressing concerns that further exacerbate the risk of chronic diseases among these populations. Although the elderly population in these areas is already grappling with poor health conditions, they are more likely to skip medical and dental visits, treatments, tests, and medication due to unaffordable costs (National Rural Health Alliance 2014).
In light of these pressing concerns, the present study aimed to examine the factors that mediate income-related factors and lead to service utilization inequalities for older Australians. Specifically, the study explored whether income inequality affects access to public or private dental service sectors and whether this has an impact on service utilization patterns. In other words, the research question was whether income-related factors play a role in creating inequalities in access to dental services and utilization patterns among older Australians.
Method
Deidentified data from the Dental Care and Oral Health Study (DCOHS) were used (Song 2020). DCOHS was a state survey conducted in South Australia from June to November 2015. Postal and email questionnaires were sent to 12,245 South Australians; subsequently, 4,494 responses were collected, resulting in a 44.6% response rate after excluding out-of-scope participants and those not residing at listed addresses. The University of Adelaide’s Human Research Ethics Committee approved the study (H-288-2011). In this cross-sectional study, DCOHS participants who were ≥65 y were selected and included in the analysis (n = 1,312). As this study aimed to explore inequality in a specific age range, an unweighted sample was used for analysis. This study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for Reporting Observational Studies (Elm et al. 2019). The STROBE checklist is available as Appendix Table 1.
Variables of Interest
Household income (exposure)
Participants were asked to report their household’s overall annual untaxed income using 10 categories ranging from $20,000 to more than $180,000. For statistical analysis, income was dichotomized into 2 groups: ≥$40,000 (coded as 1) and <$40,000 (coded as 2). The cutoff point of $40,000 was determined based on the distribution of household income in the sample. In this study, the group with income ≥$40,000 is referred to as the higher-income group, although it should be noted that this category may also include individuals with middle-income levels relative to the general population.
Concession card ownership (mediator 1)
Participants were asked to report if they held concession cards. Concession card ownership status for people who declared having a pensioner or health care card was considered as positive (yes = 2) and otherwise as negative (no = 1).
Dental service sector (mediator 2)
Participants were asked to report the place of their last dental visit, which was coded as (2) if it was a public facility, including dental hospitals and clinics, and as (1) if it was a private practice. In Australia, public dental facilities, especially in South Australia, are predominantly located in major cities, with dental services in South Australia mainly provided at the Royal Adelaide Dental Hospital in Adelaide. For statistical purposes, mediators were coded as 1 and 2 to account for their role in the analysis.
Last dental visit (outcome)
The time of participants’ last dental visit was captured and coded as follows: (0) if it occurred within the last year and (1) if it happened more than a year ago. It is important to acknowledge that visiting norms may differ in various contexts. In this study, a dental visit that took place before the last 12 mo is relatively considered a delayed dental visit, consistent with the Australian Report on Aging and Dental Health (Chalmers et al. 1999) and guidelines from the US Centers for Disease Control and Prevention (CDC 2023). It should be noted that this definition is irrespective of the perceived dental needs of the participants.
Confounders
Age
Participants’ age in 2015 was calculated based on their responses to their year of birth.
Gender
Gender was recorded as male (= 0) or female (= 1).
Country of birth
Participants recorded their country of birth, with Australia coded as (= 0) and overseas as (= 1).
Education
Information about the highest level of education was collected, ranging from no schooling to having a university degree. Participants with a university degree or more than 12 y of schooling were coded as (= 0), while those with less than 12 y of schooling were coded as (= 1).
Residential location
Participants’ residential location was determined as residing in greater Adelaide (capital area = 0) or the rest of South Australia (noncapital areas = 1) based on their postcodes.
General health status
Participants were asked to rate their general health status (very poor, poor, good, very good, excellent). Poor and very poor responses were dichotomized as poor (= 1) and otherwise as good (= 0).
Statistical Analysis
The research question investigated the mediation mechanism by which income-related disparities may directly or indirectly affect the pattern of the last dental visit through access to public services. The Figure, the Directed Acyclic Graph (DAG), illustrates the order of variables as a simplified overview of the cross-sectional analysis, depicting the direct and indirect pathways of mediation and confounding mechanisms. As stated in the Introduction, having a concession card (mediator 1) determines eligibility for receiving public dental services (mediator 2) in most Australian states, including South Australia. Thus, the proposed mediation consisted of 2 interacting mediators; as shown in the Figure, the application of the Ratio of Mediator Probability Weighting (RMPW)approach in counterfactual mediation analysis allows for mediation analysis in the presence of multiple mediators (Lange et al. 2014).
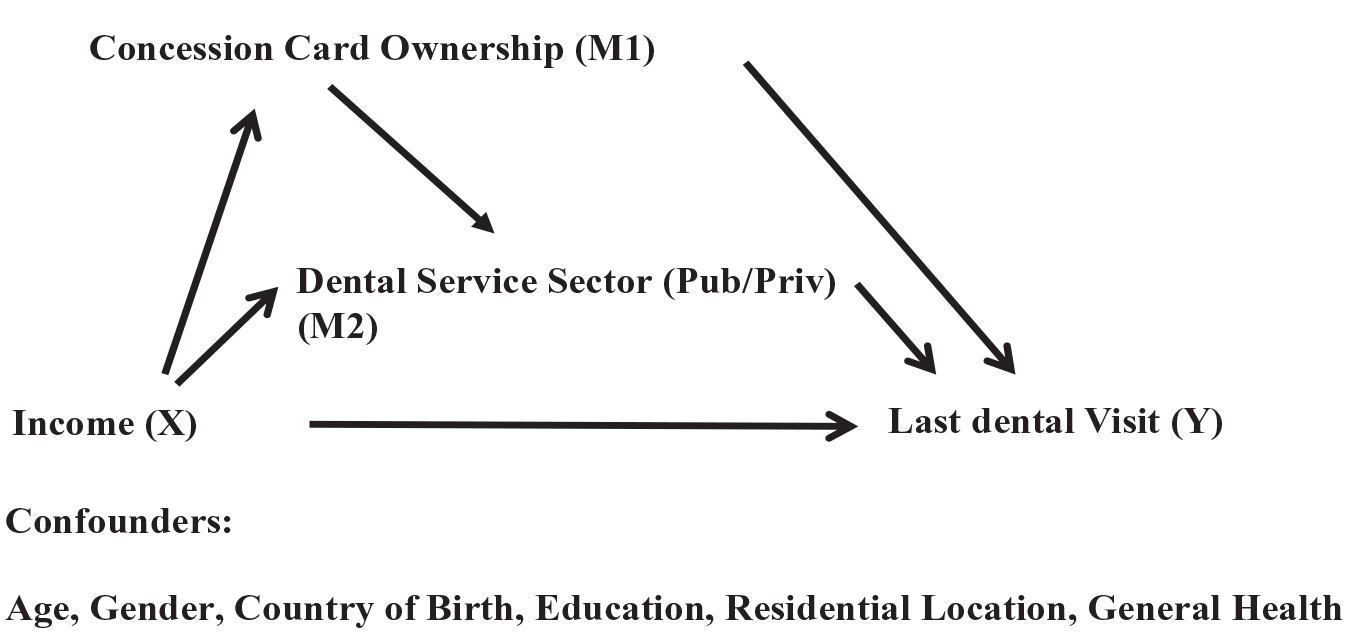
Directed Acyclic Graph (DAG) of the mediation analysis.
Counterfactual mediation allows for decomposition of the total mediation effect into direct and indirect effects. The direct effect quantifies the hypothetical change in the pattern of dental visits (i.e., outcome) if income status (i.e., exposure) were changed from high to low, while keeping the mediator’s status consistent with higher-income individuals. The indirect effect quantifies the additional change in outcome when the distribution of mediators changes to that of lower-income individuals.
To ensure robustness of the mediation analysis, confounders were included in the mediation model. However, counterfactual mediation analysis should be conducted under unmeasured confounding assumptions. These assumptions stipulate that there should be no unmeasured confounding between the exposure and the outcome, the exposure and the mediator(s), and the mediator(s) and the outcome. In addition, there should be no exposure-induced mediator outcome confounder. Therefore, conducting sensitivity analysis is crucial, as inference from mediation analysis may be sensitive in the presence of unmeasured confounders.
To estimate the mediation effects in the presence of multiple mediators, this study followed the approach by Lange et al. (2014) using marginal structural models (MSMs). In addition, for sensitivity analysis, this study adapted the method proposed by Ghanbarzadegan et al. (2023), which was originally built upon the approach introduced by Hong et al. (2018). However, Hong’s R package lacked the capability to handle sensitivity analysis for situations involving multiple mediators. To overcome this limitation, Ghanbarzadegan et al. (2023) made specific modifications to their approach, allowing it to effectively handle scenarios with multiple mediators.
For sensitivity analysis, new direct and indirect effects were calculated by step-by-step elimination of measured confounders (in this study: age, gender, location, country of birth, and general health) to account for potential sensitivity bias due to unmeasured confounders. Propensity weight discrepancy was assessed by comparing the new RMPW with the initially estimated RMPW. This comparison allowed the determination of several sensitivity parameters (i.e., ơ and ρ), which, in turn, facilitated the measurement of sensitivity bias for unmeasured confounders. For a comprehensive overview of the methodology employed in this study, please refer to Chapter 6 of Ghanbarzadegan’s (2022) dissertation.
Multiple imputations were conducted using the Mice package in R to impute missing data. Bootstrap assessment with 1,000 repetitions was conducted to assess estimation uncertainty. All statistical analyses were conducted with 95% confidence intervals using R.
Results
The imputed data for participants aged 65 y and older were entered for analysis (n = 1,312). Participants’ mean age was 72.1 ± 5.5 y, with 50.9% being female (n = 673). Before imputation, there was missingness of 13.2% for income and 4.6% and 0.5% for concession card ownership and time of last dental visit, respectively. The majority of respondents (64.9%) had their last dental visit within the past 12 mo, while a smaller proportion (35.1%) had their last dental visit more than 12 mo ago. The overall distribution of variables is available in Appendix Table 2.
Table 1 shows the cross-tabulation between exposure, mediators, and confounder variables and the time of last dental visit, whether it was over the previous 12 mo (outcome). Of those reporting a last dental visit more than 12 mo ago, 76.9% were in the lower-income group. There was no association between concession card ownership or private-sector attendance and time since last dental visit. This led to the next step of cross-tabulation between exposure and mediators (Appendix Table 3).
Distribution of Individuals Who Reported the Time of Their Last Dental Visit across the Exposure, Mediators, and Confounders Variables.
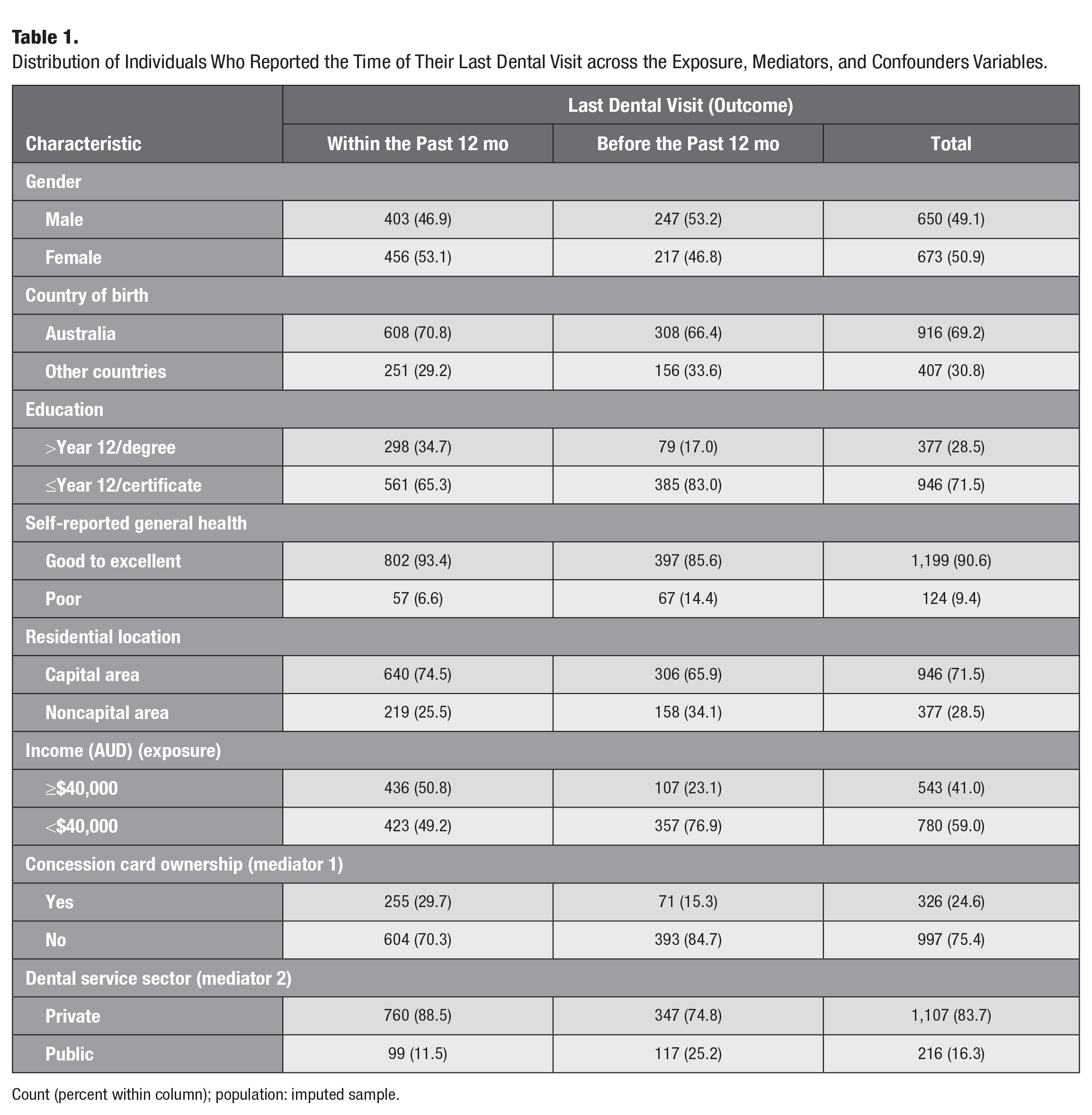
Count (percent within column); population: imputed sample.
Among concession card holders, 72.1% were lower-income participants, while 27.9% were from the higher-income group (278 participants). This implies that 51.2% of the higher-income individuals (278 of 543) had an eligible concession card. A discrepancy in dental public service utilization was observed, as only 10.2% of higher-income participants had their last dental visit in the public sector. Notably, overall utilization of public services was low, with only 16.3% of all participants using these services.
Table 2 presents the findings of the counterfactual mediation analysis. The total indirect effect was found to be minimal, with an odds ratio (OR) of 0.99 (95% confidence interval [CI], 0.85–1.05), indicating that the mediators considered in the analysis had a limited impact on the relationship between income and delayed dental visits. However, the majority of the total mediating effect (OR, 3.05; 95% CI, 1.90–5.14) was attributed to the direct effect of income. The odds ratio of the direct effect was 3.09 (95% CI, 2.24–4.87), indicating that income had a significant direct effect on delayed dental visits. The total mediation effect suggests that if the potential outcome distributions were changed to the counterfactual exposure distributions (high/low income) and the distribution of the mediators were taken from the counterfactual exposure distribution, then the odds of delayed dental visits (before the past 12 mo) would be approximately tripled in the lower-income group compared to the higher-income group. Further decomposition of the total direct and indirect effects supports this conclusion, indicating a negligible indirect effect and a significant direct effect.
Direct Effect of Income and the Total Mediating Effect of Income on the Time of the Last Dental Visit.
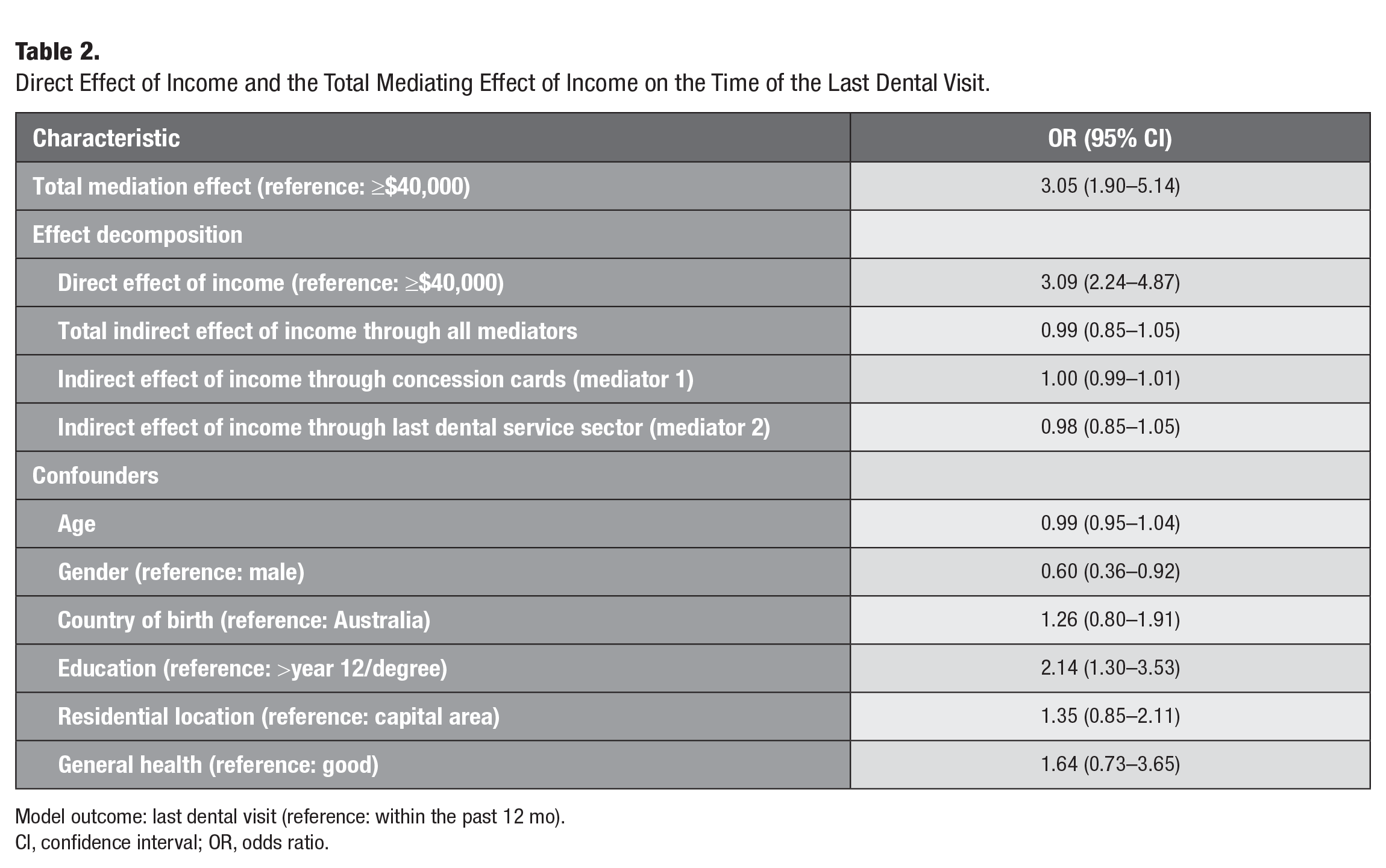
Model outcome: last dental visit (reference: within the past 12 mo).
CI, confidence interval; OR, odds ratio.
According to the sensitivity analysis results (Appendix Table 4), it was determined that the statistical inferences of the mediation analysis were not significantly affected by single unmeasured confounders. This conclusion was drawn by systematically eliminating measured pretreatment confounders one by one and examining the potential deviations from the original mediation results. However, it is important to note that this analysis does not take into account the possible cumulative biases from unmeasured confounders.
Discussion
This analysis sought to quantify direct and indirect effects of income on dental visiting behaviors among older South Australians using multiple mediation analysis. The findings demonstrated that when changing the potential outcome distributions to counterfactual exposure distributions, as well as taking the distribution of the mediators from the counterfactual exposure distribution, the odds of delayed dental visiting (before the past 12 mo) were approximately tripled individuals with low income compared to those with higher income. The results revealed a negligible indirect effect and a significant direct effect, indicating that income inequalities were associated with delayed dental visits in older South Australians, and the provision of public services did not ameliorate this pattern.
Oral health is an intrinsic constituent of general health and well-being; however, oral health is largely overlooked on the global health agenda (Petersen and Ogawa 2018). Despite being largely preventable, oral conditions are neglected in routine care for older individuals, leading to suboptimal oral health outcomes (Beard et al. 2016).
The neglect of oral health constitutes a failure of global health policy and a failure to deliver the basic human rights of older people. Income inequality and limited access to public dental services are significant contributors to this issue in the Australian population of older adults (Patel et al. 2021). In line with the study by Ghanbarzadegan et al. (2023) on a general population from the same survey, which reported that enablers such as concession card ownership, insurance status, or access to public dental services did not significantly reduce the financial burden on dental services utilization, this study found income inequality directly associated with the time of the last dental visit reported by participants, with minimal mediating effects through concession cards and the public dental sector. The findings indicate that approximately half of the higher-income individuals possessed an eligible concession card, which is primarily intended for distribution among low-income individuals. This points to a relatively inequitable distribution, as it does not align with the eligibility criteria for attending a public-sector service. It is essential to redistribute these concession cards to the low-income individuals to address this imbalance. The findings suggest that the limited mediating effect through public sector and concession card ownership could be attributed to this relative inequitable distribution of concession cards, as high-income individuals were also found to have access to these means-tested cards and public dental services. These findings suggest that policies and eligibility criteria for the dental public sector should be reviewed to address the inequitable distribution of concession cards and ensure that they effectively target those in need. Moreover, the overall utilization of public services was relatively low, with only 16.3% of all participants making use of these services. This suggests inadequate utilization of public services within this age group, possibly due to long wait lists.
The framing of oral health policies should prioritize the availability of public dental services for disadvantaged older adults, as this can ultimately improve access to such services (Ghanbarzadegan et al. 2022). However, it is important to note that access and service utilization patterns are influenced by various barriers, including chronic medical conditions, cognitive impairment, and rural and remote geographical barriers, all of which contribute to income disparities and delayed dental visits among older adults. Numerous studies worldwide identify that socioeconomically disadvantaged older adults, particularly those in residential aged care, have difficulty accessing urgent dental care services and receive poor standards of support with their mouth care (Welch et al. 2019). Policymakers should take short-term approaches to improve service utilization patterns in this priority population by considering all barriers and facilitators to accessing public dental services. This could include reviewing concession card eligibility criteria and inclusion of those who need it more (i.e., low-income individuals), including oral health assessments within general health care protocols to ensure holistic care, implementing outreach programs among older adults about the importance of oral health and available public dental services, provision of services to people with low access (financial, geographical or cultural) by using existing infrastructure (e.g., by using vans designed for school mobile dental programs to minimize costs and efficiently use existing capacity), providing transportation assistance to overcome transportation barriers, enhancing cultural competency of dental care providers, implementing telehealth options for remote access to dental care services, and advocating for policy changes such as designing a dedicated scheme for older adults’ dental services or incorporating dental care into existing Medicare programs. By implementing these short-term approaches and considering all barriers and facilitators to accessing dental services, policymakers can work toward improving service utilization patterns for socioeconomically disadvantaged older adults and addressing the challenges they face in accessing timely and appropriate dental care (Kiyak and Reichmuth 2005; Smith and Thomson 2017; Ben-Omran et al. 2021).
One of the strengths of this study is its design and methodology. Very few studies have examined patterns of service utilization in older Australians. Also, very few studies have investigated inequality mechanisms using counterfactual multiple mediation analysis in the dental literature. In addition, this study follows a novel modified RMPW approach for sensitivity analysis in the presence of multiple mediators.
Despite using a robust method, this study had some limitations. Most variables were dichotomized. Dichotomizing may result in information loss. However, in the presence of potential outcomes, dichotomization can provide a more direct interpretation than a continuous variable as it resonates better with randomized trial concepts (i.e., exposed/unexposed versus distribution). This also provides more stable counterfactual values using mediator propensity weights. However, findings may be sensitive to the threshold used in dichotomization and should be interpreted carefully. It is important to note that although counterfactual mediation is considered a causal method in the literature, the cross-sectional nature of this study and the absence of multiple studies limit the ability to imply causality. Therefore, caution should be exercised in interpreting the findings as causal relationships. In addition to the above limitation, this article studied unweighted state survey data. Further studies at a national population level are recommended.
Conclusion
Income inequality was associated with delayed dental visits in older South Australians, and provision of public services did not improve this pattern. This might happen due to inequitable access to public services and concession cards. It should be noted that card ownership is an indicator of eligibility to attend public dental services and reflects a greater level of disadvantage even within those on low income. Socioeconomically disadvantaged older Australians are more likely to be affected by the inability to access public services. This is especially salient for those with chronic diseases and cognitive impairment and those living in residential aged care facilities. Access relies on oral health problems being identified and then accessing the appropriate service. Failure to have that problem identified creates inequities that are then exacerbated by income inequity and access to public services. According to the significant effect of income, income disparities should also be addressed in the aging population. In addition to the above, policymakers should take short-term approaches to improve service utilization patterns in low-income older people.
Author Contributions
A. Ghanbarzadegan, L.M. Jamieson, contributed to conception, design, data analysis and interpretation, drafted and critically revised the manuscript; W. Sohn, contributed to conception, design, data interpretation, drafted and critically revised the manuscript; J. Wallace, contributed to data interpretation, drafted and critically revised the manuscript; D.S. Brennan, contributed to conception, design, data acquisition, analysis, and interpretation, drafted and critically revised the manuscript. All authors gave final approval and agree to be accountable for all aspects of the work.
Supplemental Material
sj-docx-1-jct-10.1177_23800844231199658 – Supplemental material for Examining the Effect of Income-Based Inequalities and Dental Service Provision on Dental Service Utilization among Older Australians: A Multiple Mediation Analysis
Supplemental material, sj-docx-1-jct-10.1177_23800844231199658 for Examining the Effect of Income-Based Inequalities and Dental Service Provision on Dental Service Utilization among Older Australians: A Multiple Mediation Analysis by A. Ghanbarzadegan, W. Sohn, J. Wallace, D.S. Brennan and L.M. Jamieson in JDR Clinical & Translational Research
Footnotes
Acknowledgements
We acknowledge all participants of the Dental Care and Oral Health Study. Language editing was partially done using ChatpGPT.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Data gathered from the Dental Care and Oral Health Study (DCOHS) were analyzed in this study. DCOHS was supported by National Health and Medical Research Council (NHMRC) CRE grant (1031310). The contents are solely the responsibility of the administering institution and authors and do not reflect the views of NHMRC.
Ethical Approval
Ethical approval was provided for the original survey from the University of Adelaide HREC (H-288-2011).
A supplemental appendix to this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.