
Abstract
Introduction:
Early childhood caries (ECC) is the strongest predictor of dental caries in adulthood. Indigenous children have higher levels of ECC compared with non-Indigenous children. The study aimed to estimate the efficacy of an ECC intervention among Aboriginal Australian children.
Methods:
Baby Teeth Talk was an outcome assessor-blinded, closed-cohort cross-in randomized controlled trial conducted in South Australia, Australia. We randomly allocated 448 women pregnant with an Aboriginal child to either an immediate (II) or delayed (DI) intervention group between January 2011 and May 2012. The immediate intervention comprised (1) provision of dental care to mothers during pregnancy; (2) application of fluoride varnish to teeth of children at ages 6, 12; and 18 mo; (3) motivational interviewing delivered in conjunction; and (4) anticipatory guidance. Mothers/children in the DI group received the same intervention commencing when the child was 24 mo of age. The outcomes were assessed by the number of decayed, missing, and filled teeth (dmft) in children aged 24, 36, and 60 mo. Regression-based approaches with generalized linear mixed effect (log-Poisson) model characterized the mean dmft to estimate risk ratios (RRs) and 95% confidence intervals (95% CIs).
Results:
A total of 223 participants were randomly allocated to the II group and 225 to the DI group. Three hundred sixty-five children (178 II, 187 DI) received at least 1 dental clinical examination at 24, 36, and 60 mo of follow-up. The mean dmft was lower in the II group (0.48, 1.32, and 2.06) than in the DI group (0.82, 1.90, and 3.29) at each time point, respectively. The direct ECC intervention effect was to prevent/decrease dental decay experience (dmft) occurrence by 84% (RR = 1.84, 95% CI: 1.20–2.48) after adjusting for all covariates.
Conclusions:
Our analysis indicated that the time-varied ECC intervention had immediate and longer-term effects on the prevention of ECC among Indigenous Australian children.
Knowledge Transfer Statement:
The study aimed to estimate the efficacy of an early childhood caries (ECC) intervention among Aboriginal Australian children. The findings indicated that the culturally appropriate ECC intervention is effective for the preventive of ECC and can be used by clinicians, educators, and policy makers when planning an ECC intervention, so as to prevent and reduce ECC and meet identified oral health needs across the Australian population, which is important for preventive dental care.
Introduction
Indigenous Australians are those who identify as being of Aboriginal and/or Torres Strait Islander descent. Indigenous Australians represent 3% of the total Australian population; Indigenous children aged 0 to 4 y represent 11% of the total Indigenous population (Australian Bureau of Statistics 2016). Indigenous Australian children score worse on almost every indicator of general and oral health relative to their non-Indigenous counterparts. This includes oral health, with Indigenous children having (more than 2 times) higher levels of early childhood caries (ECC), compared with non-Indigenous children (Ha et al. 2016; Ju et al. 2019).
ECC, defined as the presence of 1 or more deciduous dental surfaces with caries, is the most prevalent chronic disease in children (Drury et al. 1999). ECC rates are increasing rapidly in low- and middle-income countries and are socially patterned (Kirthiga et al. 2019; Moynihan et al. 2019). ECC is the strongest predictor of dental caries in adulthood (Isaksson et al. 2013). Multiple factors, including sociodemographic, dietary, and oral hygiene factors, are associated with ECC (Kirthiga et al. 2019). Social economic status, such as low maternal education and low family income (Warren et al. 2016), and consumption of free sugar or sugar-rich foods and beverages (Ndekero et al. 2016) have been positively associated with ECC. Maternal smoking during pregnancy, low birth weight (dos Santos Juniorv et al.2014), and preterm birth (Boustedt et al. 2020) have additionally been linked with ECC prevalence (Claudia et al. 2016; Akinkugbe et al. 2020; Akinkugbe et al. 2021). Positive oral health behaviors, including parents assisting children to brush their teeth twice daily with fluoridated toothpaste, fluoride varnish application (Gao et al. 2020), and regular dental visits have been associated with low rates of ECC (Pereira et al. 2020).
ECC is preventable, with the short-term effects of some ECC interventions reported (Basir et al. 2017; Jamieson et al. 2018; Jamieson et al. 2019a; Turton et al. 2021). There is limited information on the overall effect of such interventions due to the lack of a “lag-period” intervention effect estimation, because of the study designs, some groups received a delayed ECC intervention when a group was allocated to start the intervention. The current study aimed to estimate the overall efficacy of an ECC intervention delivered among Australian Indigenous children in partnership with Indigenous South Australian key stakeholders. The hypothesis was that a culturally acceptable time-varied ECC intervention would be effective for preventing ECC among Indigenous Australian children.
Methods
Study Design and Sample Size
Data were from the Baby Teeth Talk (BTT) trial, an outcome assessor-blinded, closed-cohort cross-in randomized controlled trial (registration ID: ACTRN12611000111976) conducted in South Australia, Australia (Merrick et al. 2012; Jamieson et al. 2018; Jamieson et al. 2019 a and b). Based on previous studies (Harrison et al. 2007; Slade et al. 2011) involving motivational interviewing (MI) to prevent ECC among Indigenous children, to detect a 25% difference in ECC prevalence between the 2 groups, at the significance criterion of 0.05 and a power of 0.80 at baseline, and allowing for an attrition rate of 35% after 36 mo, 385 participants would be necessary at baseline (193 test-immediate intervention [II] group, 193 control-delayed intervention [DI] group). Determination of whether a pregnant woman with an Aboriginal baby or babies would be assigned/treated by II or DI groups was made by reference to a statistical series based on random sampling numbers drawn up for age, socioeconomic position, and tobacco smoking status at each hospital by a biostatistician at the Australian Research Centre for Population Oral Health (ARCPOH). Details of the series were unknown to any of the investigators or project manager and were contained in a set of sealed opaque envelopes, each bearing on the outside only the name of the hospital and a number. After acceptance of participant by the panel, and before admission to ARCPOH, the appropriate numbered envelope was opened at the central office; the card inside indicated whether the pregnant woman was to be in the II or DI group, and this information was then given to the project team. Because of the nature of the intervention, neither participants nor research officers who implemented the intervention were blind to the treatment allocation. To achieve single blinding, a separate set of research staff collected 2-y outcome data. The closed-cohort cross-in randomized trial study design means that participants start in the control arm and end up in the intervention arm (all participants eventually receive the intervention before the end of the trial), and no individuals are able to join the trial once the recruitment period has ceased (Li et al. 2021). Eligible women who were pregnant with an Aboriginal child (n = 448) were randomly allocated to either an II or DI group between January 2011 and May 2012, with follow-up at 2, 3, and 5 y (Jamieson et al. 2018; Jamieson et al. 2019a; Jamieson et al. 2019b; see Figure 1).
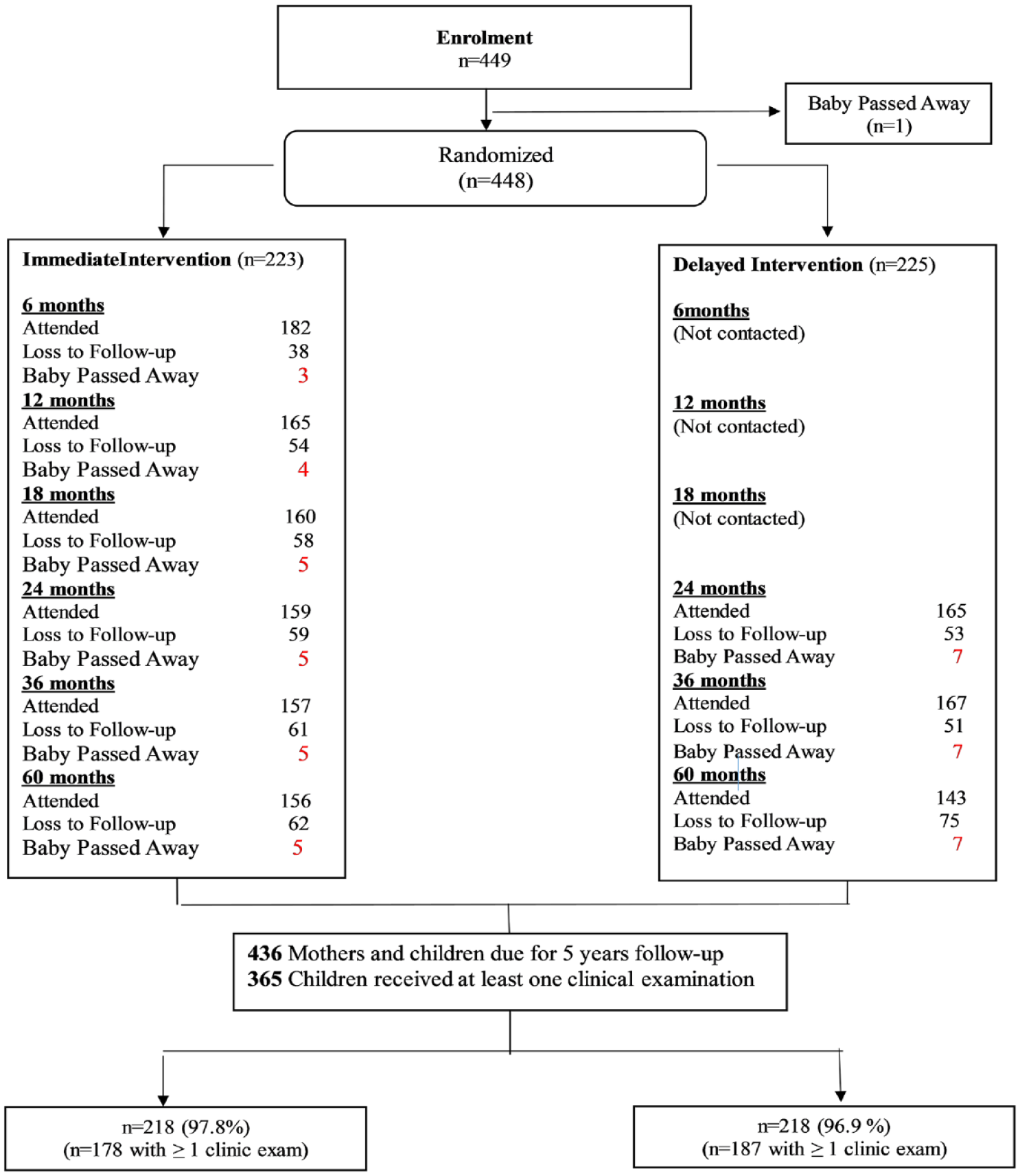
Flow diagram of participants through key stages of the closed-cohort cross-in randomized controlled trial. Immediate intervention including (1) dental care during pregnancy (mothers), (2) anticipatory guidance (mothers), (3) motivational interviewing (mothers), and (4) fluoride varnish application (children). Delayed intervention received when children aged 2 y including (1) dental care to mothers, (2) anticipatory guidance (mothers), (3) motivational interviewing (mothers), and (4) fluoride varnish application (children).
Ethics Approval
Ethics approval was obtained from the University of Adelaide Human Research Ethics Committee (H-057-2010), the Aboriginal Health Council of South Australia (04-09-362), the Government of South Australia, and the Human Research Ethics Committees of the 3 participating South Australian birthing hospitals. The study additionally used the Ethical Conduct in Aboriginal and Torres Strait Islander Health Research guidelines to obtain consent (National Health and Medical Research Council 2018). Parents of participants provided signed informed consent when participants younger than 16 y were recruited.
Data Collection
Eligibility included residing in South Australia and pregnant with an Indigenous child during the recruitment period. Face-to-face interviews were conducted by experienced researchers, and oral examinations for children at 2, 3, and 5 y of age were conducted by 3 calibrated dental professionals. Intraclass correlations for the mean untreated decay (dt) between each examiner and the gold standard examiner ranged from 0.80 to 0.88 (Jamieson et al. 2018).
ECC Intervention
A culturally appropriate ECC intervention that comprised 4 components were delivered to the II group at pregnancy and at 6, 12, and 18 mo (Jamieson et al. 2018). The intervention comprised provision of comprehensive dental care with no cost either for public or private services, implementation of MI in combination with anticipatory guidance, and application of fluoride varnish to children’s teeth at ages 6, 12, and 18 mo. Mothers in the DI group received dental care when their children were aged 24 mo and MI in combination with anticipatory guidance when their children were aged 24, 30, and 36 mo. Children in the DI group had fluoride varnish applied to their teeth at ages 24, 30, and 36 mo.
Variables
The exposure (X) variable was intervention status, which was identified as II or DI group. The outcome variable (Y) was an accumulated dental caries experience as assessed by number of decayed, missing, and filled teeth (dmft) in children aged 24 (Y2), 36 (Y3), and 60 (Y5) mo.
The covariates included the following:
1. Mothers’ baseline characteristics included maternal age, education level, household income, residential location, smoking and drinking status. Maternal age was classified as “14–24” or “25 or over” y. Education level was dichotomized into “≤12 years” or “>12 years.” Household income was dichotomized into “job” or “Centrelink (welfare).” Centrelink is the Australian agency that provides welfare payments to those who are unemployed. Residential location was dichotomized into “metropolitan” (Adelaide and outer suburbs) and “nonmetropolitan” (regional areas). Smoking status was categorized as “current,” “former,” or “never.”
2. Children’s characteristics included sex, gestational age, and birth weight. Sex was categorized as “boy” or “girl.” Gestation age was classified as “premature (<37 weeks)” or “normal.” Baby birth weight was dichotomized into “low (≤2500g)” or “normal.”
3. Children’s dental health–related behaviors included breast-feeding, free sugar consumption, frequency of toothbrushing, and dental visits at 2-y and 3-y follow-up. Breast-feeding was classified as “breastfeeding (exclusive breast-feeding 6–12 months),” “mixed feeding,” or “never breastfed.” Free sugar consumption was categorized as “<5%,” “5%-10%,” “11%-15%,” or “>15%” of total energy intake at 2-y follow-up. Frequency of toothbrushing was dichotomized into “< 2 times/day” or “≥2 times/day,” and had dental visit was grouped as “yes” or “no.”
Statistical Analysis
Completed data were analyzed based on intention-to-treat principles, which excluded children who died, for whom data were not imputed. Data analyses included descriptive and cross-in randomized trial analysis, which involved the characterization of a group-level, time-specific outcome trajectory (see the Supplemental Appendix) by using a statistical software program (SAS, version 9.4; SAS Institute Inc).
Descriptive Analysis
Baseline maternal sociodemographic characteristics, children’s characteristics and dental health–related behaviors, and dental caries experience (dmft) at 2, 3, and 5 y were described. Number and percentage or mean were reported with standard deviation (SD) for total and II and DI groups.
ECC Intervention Effect Estimates
For this closed-cohort design, under the assumption of no unmeasured covariates or other sources of bias, the conditional model was used to estimate the intervention effect on individuals (Li et al. 2021).
The time-varying ECC intervention effect on children’s dental caries experience is depicted in Figure 2.
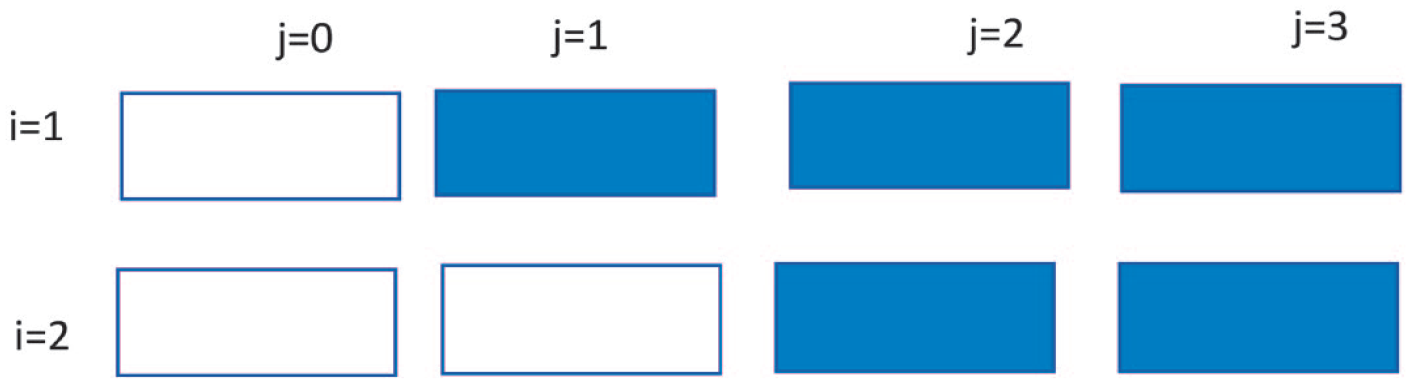
A closed-cohort cross-in randomized controlled trial with i = 2 and j = 3 periods. Each white cell indicates a group period under the control condition, and each blue cell indicates a group period under the intervention condition.
We define kij to be the number of individuals included during period j in intervention group i. Each group begins in the control condition, before being randomized to an intervention, and both groups are exposed to the intervention condition before the end of the trial (Li et al. 2021). The basic model is written:
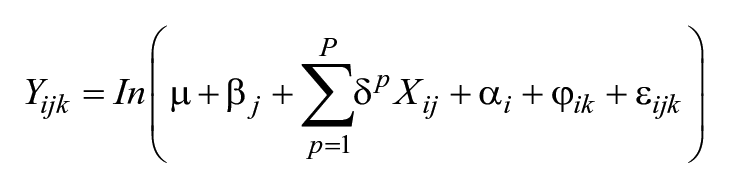
where
1. Yijk is the response (dmft) corresponding to individual k at time period j (j = 0, 1, 2, 3) from intervention group i (i = 1, 2);
2. µ is the grand mean of the outcome in the absence of covariates and period effects;
3. βj is the jth period effect;
4. Xij is a time-varying intervention indicator for intervention i during period j, and δ is the intervention effect (fixed effect) weighted for covariates p (p = 1, 2, . . ., P);
5. αi ~N(0, τ2) is the random effect for intervention group i;
6.
7. ε ijk ’s are independent and identical errors distributed as N (0, σ2).
Adjustment of regression-based approaches with generalized linear mixed-effect (log-Poisson) models were used to characterize the mean dental caries experience (dmft) to estimate risk ratios (RRs) and 95% confidence intervals (CIs). The multivariable models included 5 steps: (1) the intervention condition was entered in model 1; (2) time was added in model 2; (3) mothers’ characteristics were added in model 3; (4) model 2 plus adjusting for children’s characteristics were in model 4; (5) with the final full model (model 5) comprising all covariates.
Time-Dependent Correlation Estimates
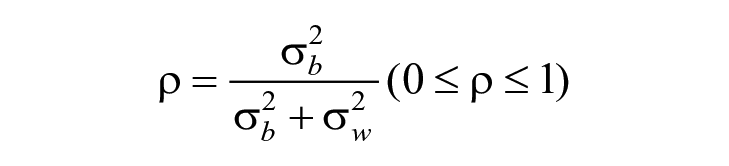
Two types of intraclass correlation coefficients (ICCs) were used: the within-period ICC (ρw) and the between-period ICC (ρb). ρw describes the correlation between 2 within-cluster observations (dmft) collected during the same period, and ρb describes the correlation between 2 within-cluster observations collected in different periods. Since the variance components are positive, the between-period ICC is constrained to be no larger than the within-period ICC.
The outcome variable (dmft) was counts with variance
The smaller the value, the more precise the overall reliability of the sample estimate.
Results
A total of 223 participants were randomly allocated to the II group and 225 to the DI group. The 12 babies who passed away before 24 mo of follow-up (5 in the II group and 7 in the DI group) were excluded from the data analyses. Three hundred sixty-five children (178 in the II group and 187 in the DI group) received at least 1 clinical examination at 24-, 36-, and 60-mo follow-up.
Mothers’ sociodemographic characteristics are presented in Table 1. Among pregnant mothers, a higher percentage was of younger age (14–24 y), had attained low levels of education (≤12 y), had low household income (Centrelink), resided in nonmetropolitan locations, and were current tobacco smokers. There was a similar pattern in both the II and DI groups.
Baseline maternal sociodemographic characteristics by intervention group among pregnant women in South Australia.
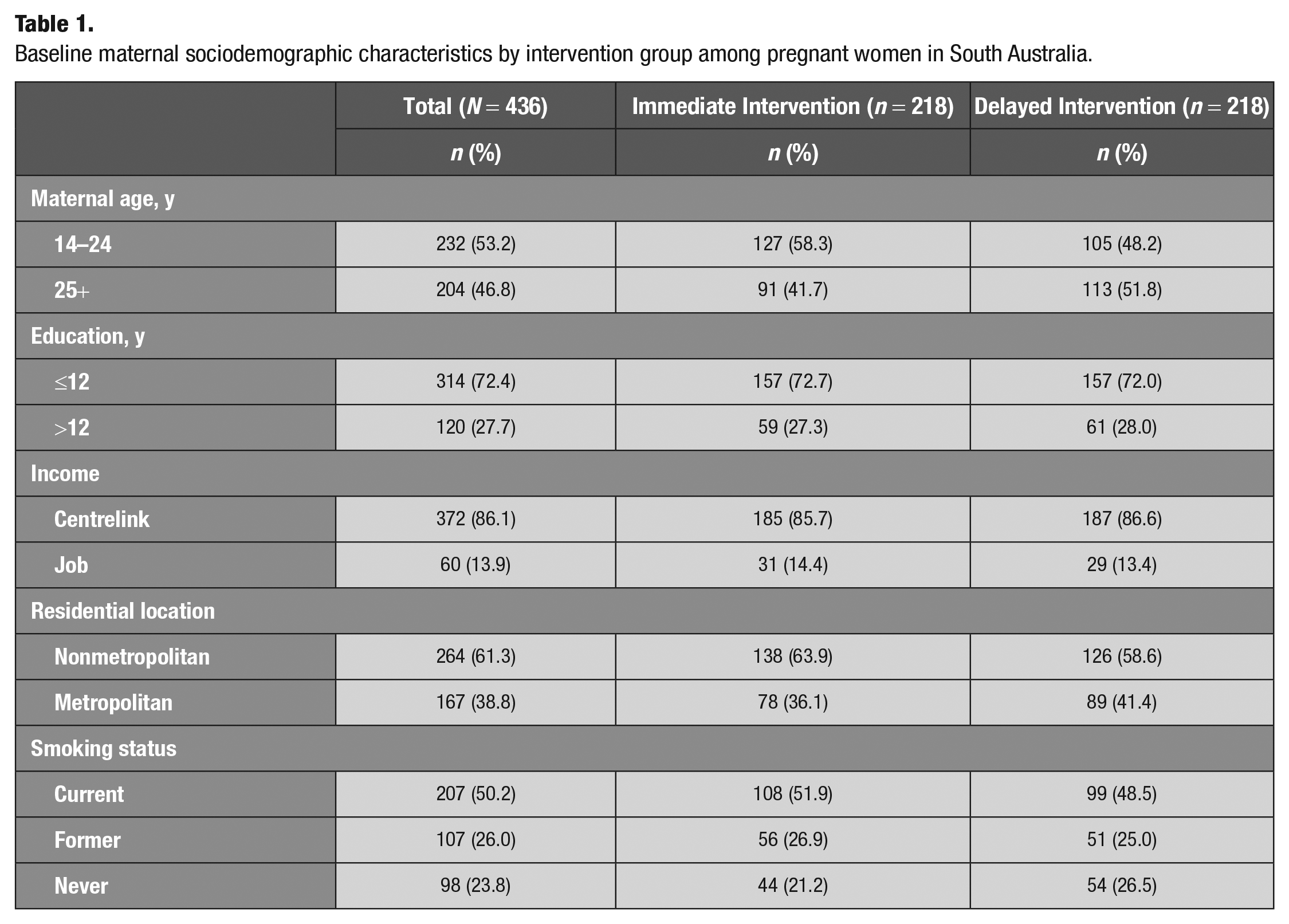
Table 2 shows the children’s perinatal, dietary, and dental behavior characteristics and dental caries experience. A higher percentage were of term gestational age and birth weight, had mixed feeding, had a free sugar consumption of 5% to 10% of total energy intake, had their teeth brushed less than twice per day, and had not visited a dentist in the past 12 mo. The percentage of preterm gestation, low birth weight, mixed feeding, free sugar consumption less than 5% of total energy intake, frequency of toothbrushing ≥2 times/d at 2-y follow-up and regular dental visiting at 2- and 3-y follow-up was higher in the II group than in the DI group. The mean dmft was lower in the II group than in the DI group, with estimates being 0.48 versus 0.82, 1.32 versus 1.90, and 2.06 versus 3.29 at 2, 3, and 5 y, respectively.
Children’s perinatal, dietary and dental behavior characteristics and dental caries experience by intervention group among Indigenous children in South Australia.
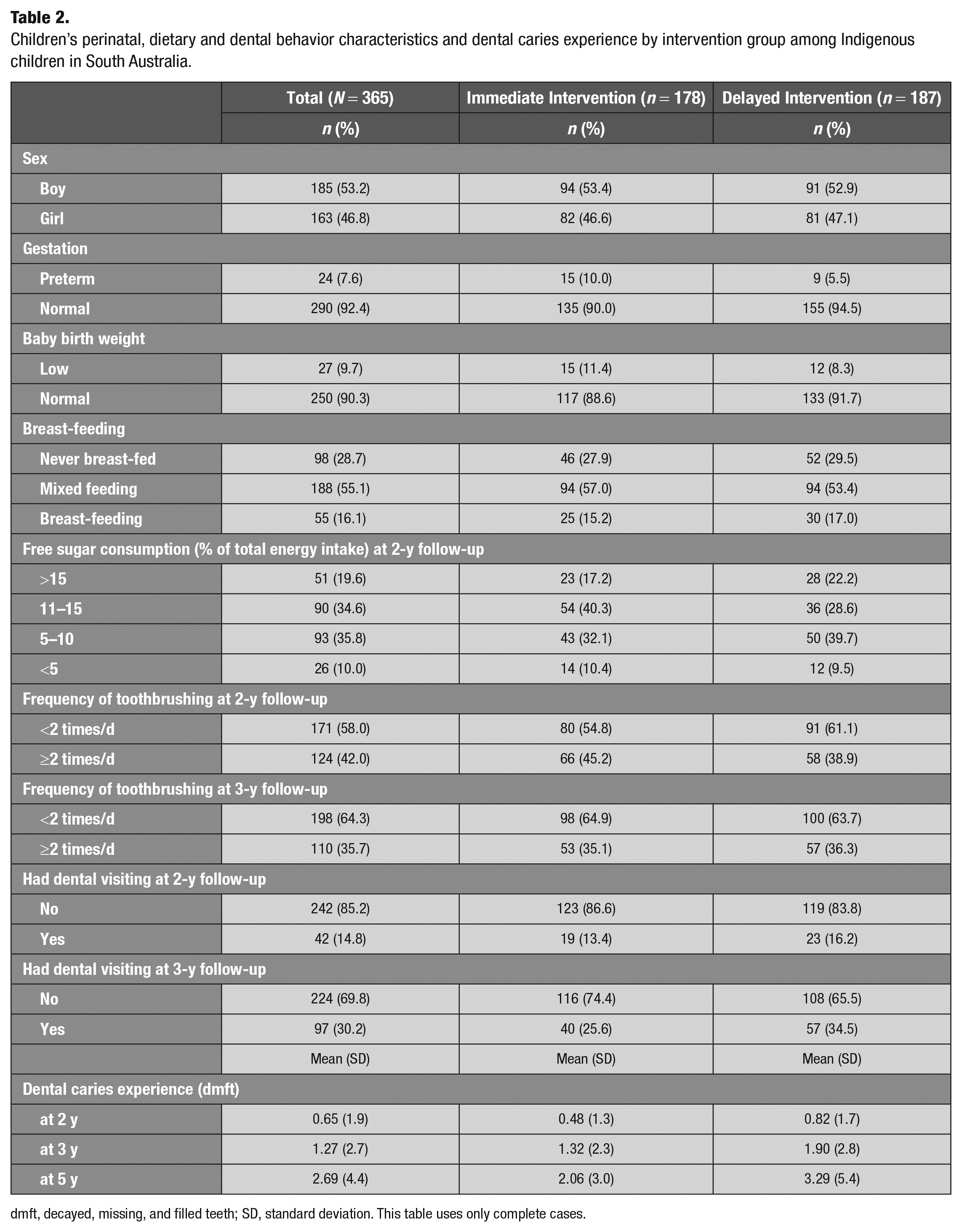
dmft, decayed, missing, and filled teeth; SD, standard deviation. This table uses only complete cases.
Table 3 shows findings from the ECC intervention effect analyses and ICC. The direct ECC intervention effect was to prevent/decrease dental decay experience (dmft) occurrence by 150% for the unadjusted model and by 84% after adjusting for all covariates. No statistically significant differences were observed in mothers’ and children’s characteristics. The ICC value was 0.067, which indicated that dental caries experience (dmft) in the intervention group was approximately 7% more likely to have the same value than if the 2 dmft were chosen randomly.
ECC Intervention Effects among Indigenous Children in South Australia.
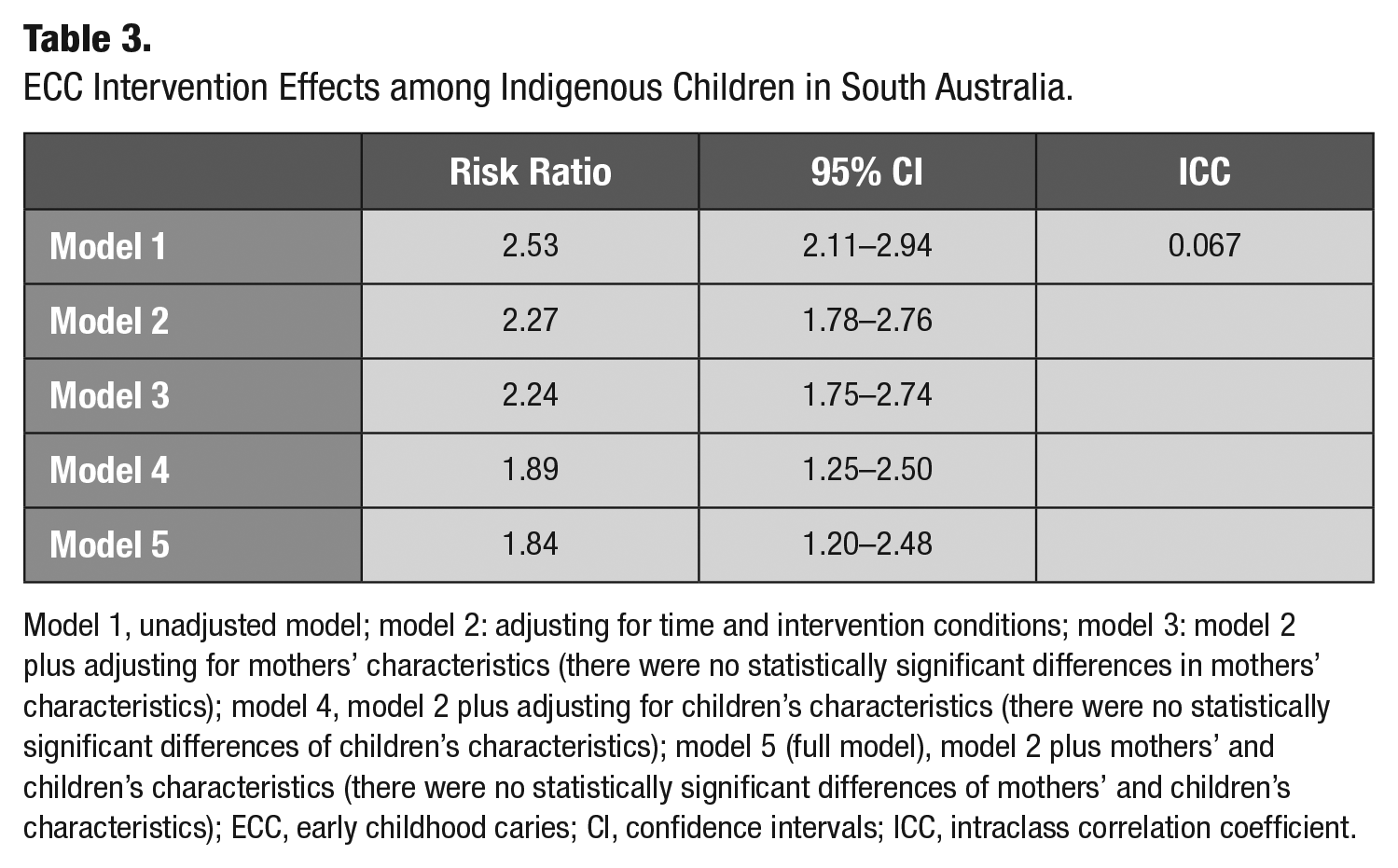
Model 1, unadjusted model; model 2: adjusting for time and intervention conditions; model 3: model 2 plus adjusting for mothers’ characteristics (there were no statistically significant differences in mothers’ characteristics); model 4, model 2 plus adjusting for children’s characteristics (there were no statistically significant differences of children’s characteristics); model 5 (full model), model 2 plus mothers’ and children’s characteristics (there were no statistically significant differences of mothers’ and children’s characteristics); ECC, early childhood caries; CI, confidence intervals; ICC, intraclass correlation coefficient.
Discussion
Our findings support our hypothesis that the time-varied ECC intervention had an effect on the prevention of ECC among Indigenous Australian children. Our findings indicate that a culturally sensitive the time-varied ECC intervention not only has a short effect but also has a carryover effect: lower dental caries experiences were observed among the II group at 2-, 3-, and 5-y follow-up compared with the DI group. Our findings additionally indicated that deferred acceptance of a culturally appropriate ECC intervention would have an impact on the improvement of parents’ knowledge and ability to look after their children from diet to oral hygiene, which manifested as higher percentages of “free sugar consumption (>15% of total energy intake)” and “tooth brushing less than 2 times/day” in the DI group at 2 y of age.
Our findings indicated that the culturally appropriate 4-pronged ECC intervention (Jamieson et al. 2019a) is effective for the preventive of ECC:
MI combined with anticipatory guidance interventions is an important part of our ECC intervention. MI is a promising intervention to activate a pregnant mother’s desire to enact positive behavior change, such as healthier diets and good daily oral hygiene routine/habits, to achieve the prevention of ECC for their children (Jamieson et al. 2016; Leske et al. 2021). Our cross-culturally adapted anticipatory guidance is a proactive and developmentally appropriate oral health education intervention (Jamieson et al. 2018). A combination of both was not only provision of theory foundation in the improvement and promotion of parents’ oral health literary but also change in oral health–related behaviors on the prevention of ECC. On the contrary, there was higher percentage of “free sugar intake (>15% of total energy intake)” and “tooth brushing less than 2 times/day” in the DI group due to not having had an earlier intervention.
The provision of comprehensive dental care at no cost for pregnant mothers (including dental checkups, X-rays, dental scaling and cleanings, restorations, and extractions) aimed to reduce bacterium, such as Streptococcus mutans (ten Cate 1999; Chaffee et al. 2014), in oral biofilm, so as to prevent maternal-child transmission of oral bacteria and, moreover, to reduce oral infection in dental caries development (Riggs et al. 2019).
As is well known, the caries-preventive effect of fluoride is a physical-chemical process, and as such precipitates fluorapatite, reducing demineralization and increasing remineralization and mineralization of hypomineralized areas; interferes with the bacterial enzymatic process; modifies tooth morphology; and so on (Riggs et al. 2019). Meanwhile, varnish prolongs the contact between fluoride and the enamel to maintain a cariostatic fluoride level in the saliva and the dental biofilm via a slow-releasing reservoir of fluoride (Turska-Szybka et al. 2021). The application of fluoride varnish in early age is an effective strategy for preventing and reducing ECC.
The strengths of the study were (1) the longitudinal closed-cohort with baseline randomized controlled trial design to allow for an estimated time-varied intervention effect and (2) the unbiased estimate by using a cross-in randomized trial analysis to ensure more precise inferences. The limitation of the study was that we did not assess the protective effect of other fluoride-related products, such as fluoride toothpaste, community water fluoridation, dental sealants, or silver nitrate/silver diamine fluoride. In addition, we had data on free sugar consumption only at 2 y age, which might affect the estimation of the intervention effect. Another potential limitation is that the Poisson models include only 1 parameter. However, negative binomial, zero-inflated Poisson, and zero-inflated negative binomial models did not provide a better fit.
Conclusion
Our analysis indicated that the time-varied ECC intervention has immediate and longer-term effects on the prevention of ECC among Indigenous Australian children.
Author Contributions
X. Ju, contributed to conception and design, data acquisition, analysis, and interpretation, drafted and critically revised the manuscript; M.N. Mittinty, contributed to conception and design, data analysis and interpretation, drafted and critically revised the manuscript; L. Smithers, L. Jamieson, contributed to conception and design, data acquisition and interpretation, drafted and critically revised the manuscript. All authors gave their final approval and agree to be accountable for all aspects of the work.
Supplemental Material
sj-docx-1-jct-10.1177_23800844231191714 – Supplemental material for Early Childhood Caries Intervention in Aboriginal Australian Children: A Cross-in Randomized Trial
Supplemental material, sj-docx-1-jct-10.1177_23800844231191714 for Early Childhood Caries Intervention in Aboriginal Australian Children: A Cross-in Randomized Trial by X. Ju, M.N Mittinty, L. Smithers and L. Jamieson in JDR Clinical & Translational Research
Footnotes
Acknowledgements
The authors gratefully acknowledge the support of the Baby Teeth Talk (Australia) study participants, study staff, and partners: South Australian Dental Service, Colgate Palmolive, Women’s and Children’s Hospital, Lyell McEwen Hospital, Flinders’ Medical Centre, Aboriginal Family Support Services, Aboriginal Primary Health Unit, Metro Aboriginal Family Birthing Program, Kura Yerlo Centre, Aboriginal Legal Rights Movement, Wodlitinattoai Program, Ninko Kutangga Patpangga, Kanggawodli Step Down Service, Kaurna Plains, Fleurieu Families, Gilles Plains Community Health, MADEC Community Support Services, Naporendi Aboriginal Forum, Nunga MiMinar, Aboriginal Strategy Unit of Families South Australia, Inbarendi College, Para West Adult Campus, Pangula Mannanurna Aboriginal Health Corporation and the Muno Parra Medical Centre, Second Story, Inner Southern Health Service, The Corner House, Louise Place, PARKS, Talking Realities Program, Child Youth Women’s Health Services, Southern Junction Community Services, TAFE campuses, GP Plus centers, employment programs, childcare centers, women’s centers, domestic violence shelters, and primary and high schools. This study was funded by the National Health and Medical Research Council of Australia (NHMRC, project grant 627350). L. Jamieson is supported by a NHMRC Senior Research Fellowship.
Availability of Data and Materials
The data sets generated and/or analyzed during the current study are not publicly available due to privacy issues of the participants. Data are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
A supplemental appendix to this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.