
Abstract
Objective:
Research into the influence and role of social networks on oral health outcomes has been limited. This study aims to demonstrate via explanatory modeling the influence of social networks on oral health outcomes among women in who live in public housing in Boston, Massachusetts.
Methods:
Individual- and network-level data were obtained from a cross-sectional survey of adult female residents of 2 public housing developments in Boston, Massachusetts. Participants responded to close-ended questions about sociodemographic characteristics, oral and general health status, and health-related behaviors for themselves as well as their named social contacts. Based on this information, network-level variables were calculated for each participant, including the proportion of the social network with certain characteristics or attributes. To assess the salience of network measures in explaining the variability in self-reported oral health status, overall health status, use of dental services within the last year, and current dental treatment needs, logistic regression models with individual-level covariates were compared with corresponding models that additionally included network-level variables with McFadden R2 for comparison purposes.
Results:
Model comparisons for each outcome of interest demonstrated that adding network-level covariates significantly improved model fit. Additionally, network-level covariates displayed strong independent associations with the outcomes of interest. The network proportion needing dental treatment was positively associated with participants’ odds of reporting current dental treatment needs (odds ratio, 4.71; 95% CI, 1.47 to 15.05). An individual’s odds of reporting no dental visit within the past year decreased with increasing exposure to social contacts with reported dental visits within the past year (odds ratio, 0.26; 95% CI, 0.07 to 0.89).
Conclusion:
The salience of specific network attributes depended on the outcome under study. Interventions aimed at reducing the poor oral health burden in this and similar population groups may benefit from integrating information on social networks, including tailoring intervention delivery and/or messaging to account for the potential influence of social networks.
Knowledge Transfer Statement:
This work may be beneficial to those developing policy solutions and interventions aimed at reducing the burden of poor oral health outcomes in socioeconomically disadvantaged populations, such as women who reside in public housing developments. The potential for leveraging social networks to seed messaging about oral health, for example, may enhance efforts to reduce oral health disparities.
Introduction
Social networks refer to the webs of social relationships formed by interconnected people. Research has shown that social networks influence health via social influence, social support, and the delivery of resources needed to maintain good health (Berkman and Glass 2000). Social network analysis is a theory-driven method within the domain of complex systems science that aims to measure the presence and influence of social structures (Heaton and Baker 2023). This method has increasingly been applied to public health research, with a growing number of studies evaluating the social aspects of health-related behaviors and outcomes, specifically with respect to oral health (Maupome and McCranie 2015; Broomhead and Baker 2019; El-Sayed et al. 2021).
A key motivation in the study of social networks in relation to health outcomes is the demonstrated potential for the social network to serve as an effective and efficient delivery system for health-related behavioral change interventions (Carson et al. 2013; Kim et al. 2015). Additionally, leveraging social networks to modify health behavior holds promise as an effective means to address health disparities. Individual behavior change is complex, particularly in populations where health-promoting behaviors are not normative, and it may demand a greater amount of social support for change to occur and persist over time (Gondal 2015). For this reason, individually focused behavioral interventions are likely to fail when they ignore the role of social influence, as delivered by the social network, in behavioral choices (Valente and Fosados 2006; Heaton and Gondal 2023).
Social network analysis can inform the potential power of network-level interventions for a particular behavior or set of behaviors (Perry et al. 2018). However, applications of social network analysis to oral health remain in their infancy and are limited in scope (Maupome and McCranie 2015; Pullen et al. 2018; Pullen et al. 2019; Vettore et al. 2022). Instead, the role of social support has been measured via other means, including single questionnaire items pertaining to the number of close friends or the need for more emotional support (Sabbah et al. 2011; Burr and Lee 2013; Watt et al. 2014; Jang et al. 2014; Sadeghipour et al. 2017). Without the elucidation of network characteristics via social network analysis, existing research into social support is limited in its ability to inform the potential utility of network-level interventions.
We conducted a social network analysis among women living in 2 government-funded housing developments (public housing) in Boston, Massachusetts. Public housing developments are a natural site for network-level health interventions because they represent discrete, geographically bounded communities with strong social connections. Additionally, the selective forces that drive people to public housing are more broadly reflective of vulnerable populations in the United States, including disproportionately higher rates of chronic disease, such as poor oral health (Digenis-Bury et al. 2008). Our objective was to determine the salience of social network characteristics in explaining variability in oral health–related outcomes and to identify which network characteristics were most impactful for each outcome evaluated under a statistical modeling paradigm. To this end, our research applied an egocentric (e.g., personal) network perspective, as opposed to a sociometric/centric (e.g., whole) network perspective.
Methods
This work leverages data collected from a cross-sectional survey study employing social network analysis to elicit network connections and to quantify the importance of an individual’s social ties in explaining the variability in self-reported oral health outcomes.
Social Network Terminology
Our analysis takes an egocentric perspective. Ego is the individual at the center of the network, who provided the information, and thus refers to all enrolled participants in this study. Alters are individuals named by an ego, or those who form the ego’s social network. The term alters is often considered interchangeable with network ties, although ties formally refers to the connection between egos and alters. An ego network, or egocentric, perspective refers to an analysis centered on the ego and those network ties emanating from the ego to alters (Appendix Figure).
Study Population
The Boston Housing Authority, the local government entity responsible for managing publicly funded housing in Boston, Massachusetts, provided a complete list of all households within 2 similarly sized (approximately 450 households) family-designated housing developments to serve as the sampling frame. With a random number generator, 190 households per development were selected for participant recruitment. Residents were eligible if they were women aged 18 to 55 y and spoke English or Spanish. Door-to-door knocking of selected households served as the primary means of recruitment, while outreach at community events, referral from enrolled participants, and flyers posted in communal spaces in the residences served as additional sources of participant recruitment. Following common network sampling techniques, we also attempted to recruit any named alters as egos who were themselves Boston public housing residents via snowball sampling. Recruited alters did not have to meet the age eligibility criterion for initially recruited egos to be included in this analysis.
Data Collection
In-person interviews were conducted by trained bilingual study staff in the participants’ preferred language (English or Spanish) between November 2014 and September 2015. Network data were collected from all respondents (egos) with 5 questions aimed at eliciting names of alters (ie, name generators) with whom they had talked about a variety of subjects (discussants), including personal matters or problems and health-related topics, encompassing general health and oral or dental health (Perry et al. 2018). After names were elicited, egos were asked to report information about each alter: demographics (e.g., gender, race), details of their relationship (e.g., frequency of communication, ego’s perceptions of alter’s health and health-related behaviors), and ego’s perception of relationships present among all possible pairs of alters named (Appendix Figure). Responses were collected on paper forms that were subsequently coded, double entered, and checked for errors.
Data collection procedures were reviewed and approved by the Boston University Medical Campus Institutional Review Board (H-32328), and informed consent was obtained from each participant prior to interview conduct. Reporting of this study conforms to the STROBE guidelines.
Measures
Outcomes
Four binary dependent variables representative of general and oral health status and dental service utilization were analyzed:
1) Self-reported general health status of fair or poor was compared with responses of good, very good, or excellent health.
2) Self-reported oral health status was similarly evaluated.
3) Women who reported that their last dental visit was over a year ago were compared with those who reported a visit in the last year.
4) Dental treatment needs were assessed by asking whether women reported a current need for dental treatment (yes/no).
Egocentric Network Measures
Social networks were constructed with the information obtained from egos. Network characteristics were operationalized by egos’ reports on their own behavior and characteristics, as well as those of their named alters. Network size (degree) was operationalized as the number of individuals in an ego’s network. The number of general health and oral health discussants in a network was dichotomized as ≥1 discussants versus no discussants. We also calculated measures characterizing the proportion of ties in each ego’s network with a given characteristic—specifically,
The proportion of ties perceived as having good, very good, or excellent general health
The proportion of ties perceived as having good, very good, or excellent oral health
The proportion of ties that an ego talks to daily
The proportion of ties living locally in Boston, Massachusetts
The proportion of ties perceived as currently in need of dental treatment
The proportion of ties believed to have visited a dentist within the past year
Network proportion measures were calculated by dividing the number of alters with a given attribute by the total number of alters named (excluding alters from the denominator that had missing or unknown values for that item), which ranged from 0 to 1 (0% to 100% of ties).
Covariates
All analyses controlled for ego age, ethnicity (Hispanic vs. non-Hispanic), and level of education (high school degree or equivalent vs. less than high school or equivalent). Education level was used as an indicator of socioeconomic status given that income levels <100% of the federal poverty line are nearly ubiquitous in this population. Age was categorized into 10-y increments.
Statistical Analysis
Descriptive statistics were calculated for demographic characteristics on the ego and network levels. Logistic regression models explored the relationship between individual- and network-level characteristics and ego self-reported general and oral health, dental treatment need, and dental health service utilization. To assess whether social networks may be related to these individual-level outcomes, we examined 2 regression models for each outcome of interest: 1) a model including only ego-level variables (restricted models) and 2) a model that included ego-level and network measures (full models). Restricted and full models were compared through Akaike information criterion and McFadden R2 values. We assessed collinearity of the variables in each model by calculating correlation coefficients for each model. Coefficients <|0.40| were considered uncorrelated. Overall, there were very few missing data for measures used in these analyses: outcome measures and participant control variables had no missing values, and the network measures (n = 8) each had missing data <5%. All analyses were conducted in Stata 13 (StataCorp).
Model Building
Covariates in the restricted and full models were based on previous research and differed by outcome (Armfield 2012; Peres et al. 2019). On the ego level, all models controlled for age, Hispanic ethnicity, and education. Because individuals with lower socioeconomic status (for which educational attainment is a proxy here) are more likely to experience significant barriers to accessing needed dental services (Peres et al. 2019), the model examining self-reported oral health status included dental service utilization in the past 12 mo as a covariate. Additionally, those with poor oral health may delay seeking care until acutely needed out of fear or embarrassment (Armfield 2012); thus, the models for current dental treatment need and dental health service utilization each included self-reported oral health status as a covariate.
Network variable selection was theoretically driven, with initial analyses investigating all plausibly relevant network measures available for each outcome. Given our objectives and the limits imposed by the sample size and correlations among covariates, network measures that were not significant or did not improve model fit were dropped. The resulting analyses therefore include network measures that produce parsimonious models.
To examine the potential influence of differential ego recruitment (i.e., random sampling vs. snowball sampling), we ran each model including a covariate indicating the method of ego recruitment and subjectively assessed whether the conclusions differed after the inclusion of this variable.
Results
Our sample included 176 women. A total of 621 alters were named by 175 women (1 woman named zero alters). Characteristics of the sample are provided in Table 1. The mean age was 38 y (SD =11.51), ranging from 18 to 75 y. Snowball sampling converted some alters to egos, and those egos did not need to meet the initial age eligibility criterion. Participants were primarily of Hispanic ethnicity (62%) but racially diverse, with 22% identifying as exclusively White, 36% as exclusively or partially African American or Black, and 41% as other races.
Individual (Ego) and Network Characteristics of the Study Population (N = 176).
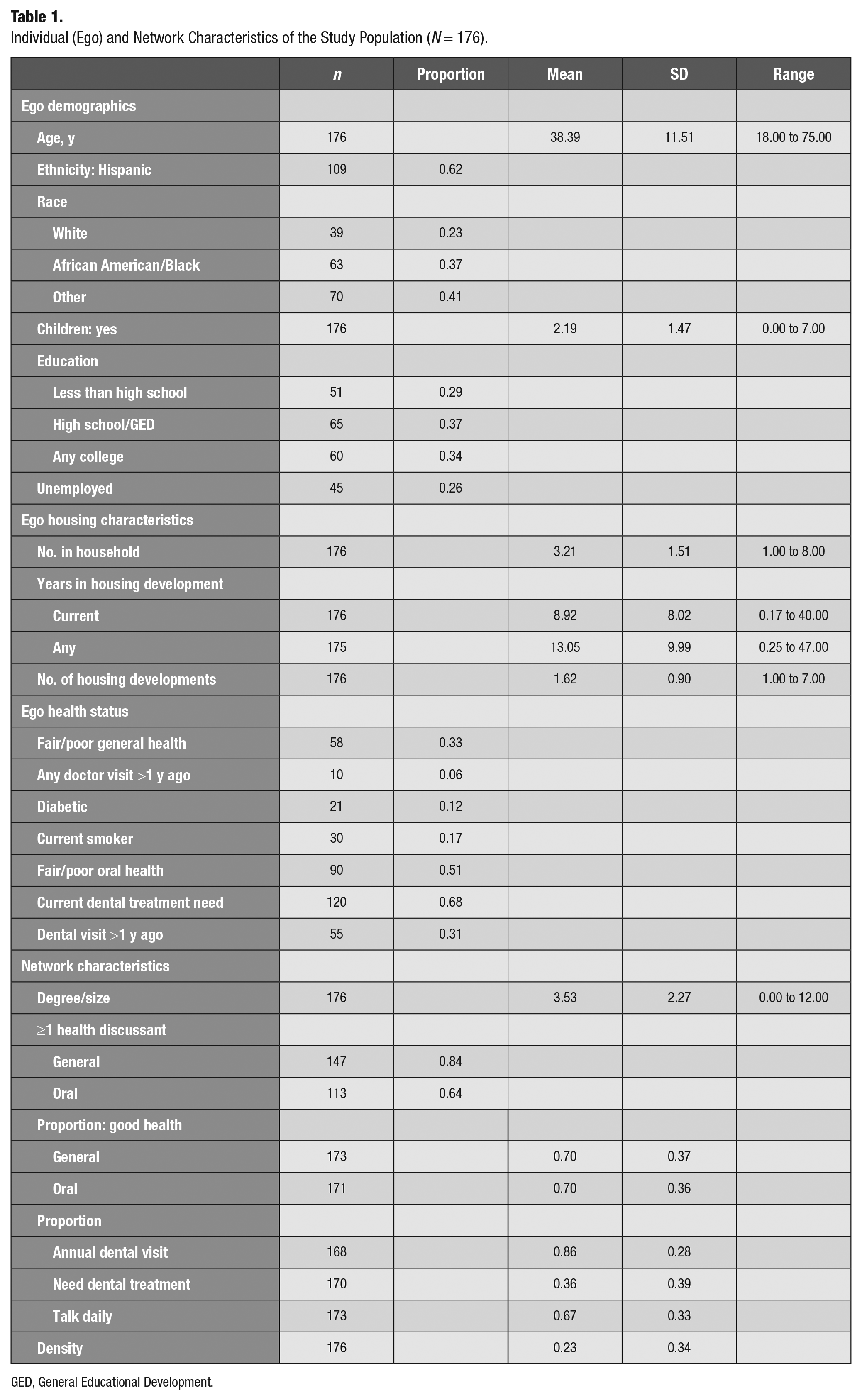
GED, General Educational Development.
Overall, 67% of the women sampled reported having good, very good, or excellent general health, with 33% reporting fair or poor health. Only 6% of participants indicated that they had not seen a doctor or visited a health clinic in the past year. Despite having favorable general health status overall, over half reported fair or poor oral health (51%). Though 69% of the women sampled had seen a dentist in the past year, 68% indicated that they had a current need for dental treatment.
Respondents named between 0 (n = 1) and 12 (n = 2) alters (mean, 3.53). Most women named at least 1 general and oral health discussant (84% and 64%, respectively) and, on average, reported that 70% of alters had good, very good, or excellent general and oral health (SD = 0.37 and 0.36, respectively). Participants indicated, on average, that about 86% of alters had seen a dentist in the past year and 36% currently need dental treatment. Overall, participants reported seeing or talking to 67% of their network ties daily.
For each of the 4 outcomes, the full model containing network characteristics had a superior fit when compared with the model that did not contain network characteristics, as indicated by a lower Akaike information criterion and higher R2 values (see Tables 2–4 for details by outcome).
Logistic Regression Models of Self-reported Fair or Poor General Health on Ego and Network Measures.
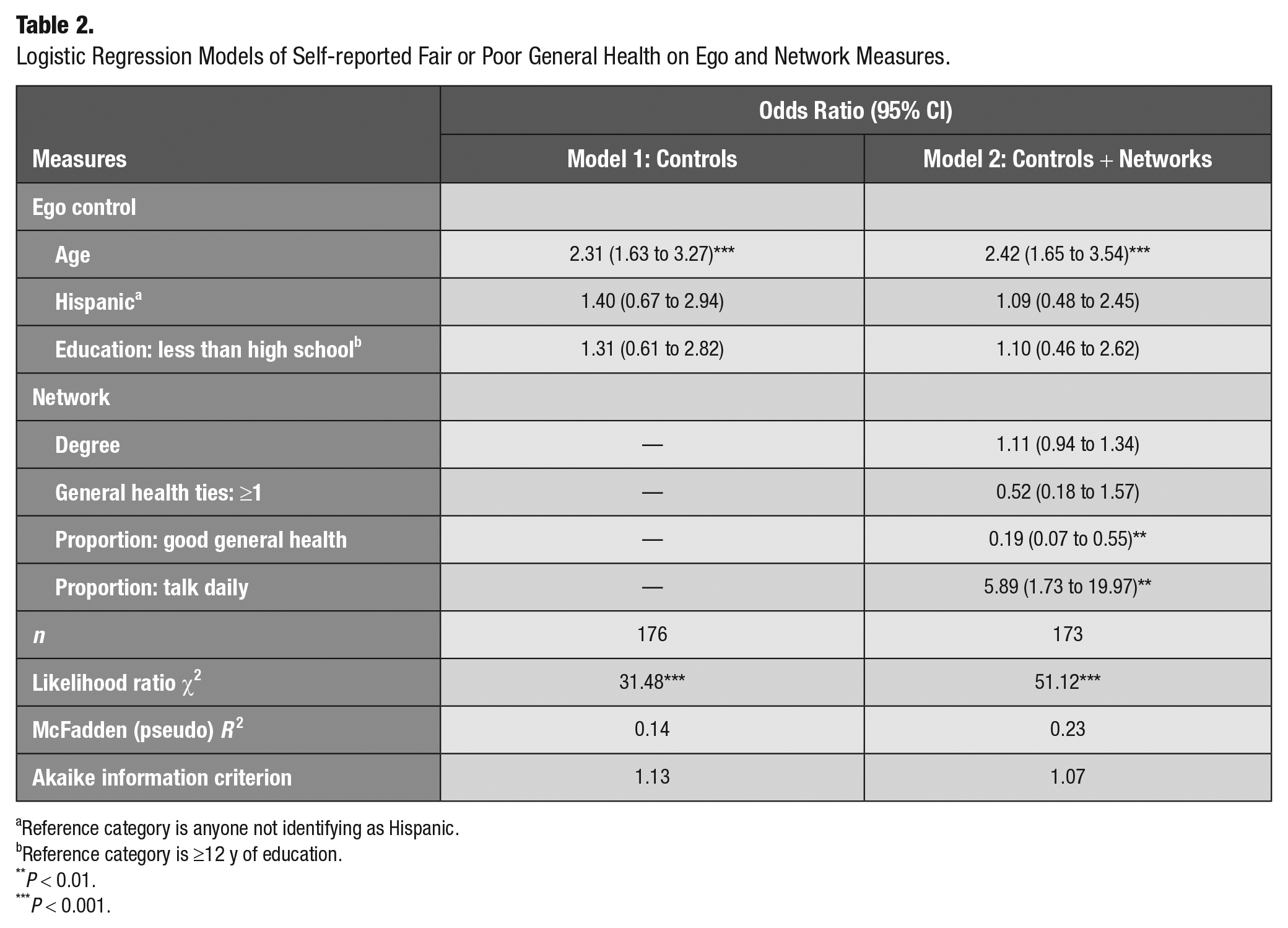
Reference category is anyone not identifying as Hispanic.
Reference category is ≥12 y of education.
P < 0.01.
P < 0.001.
Logistic Regression Models of Self-reported Fair or Poor Oral Health Status on Ego and Network Measures.
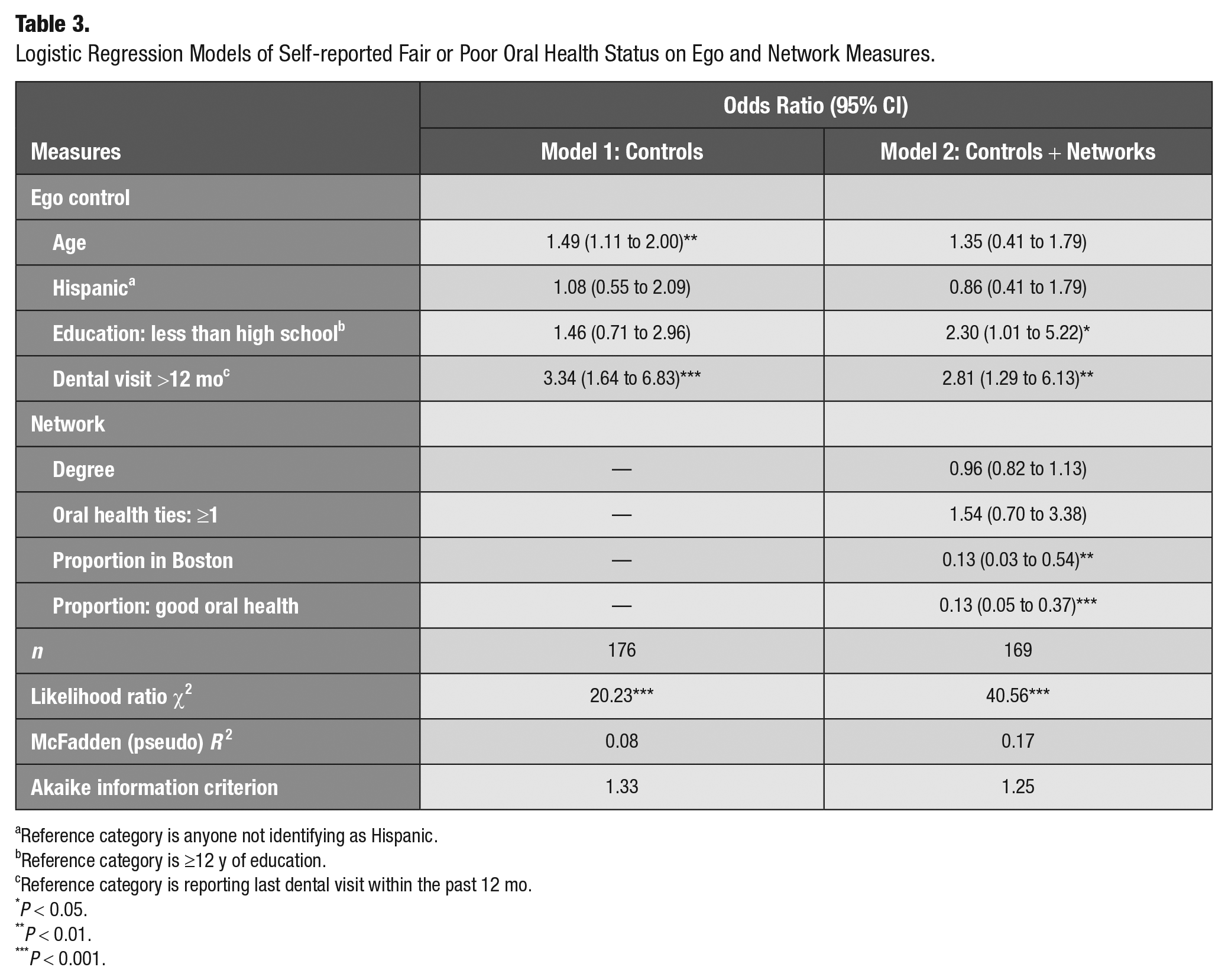
Reference category is anyone not identifying as Hispanic.
Reference category is ≥12 y of education.
Reference category is reporting last dental visit within the past 12 mo.
P < 0.05.
P < 0.01.
P < 0.001.
Logistic Regression Models of Dental Treatment Need on Ego and Network Measures.
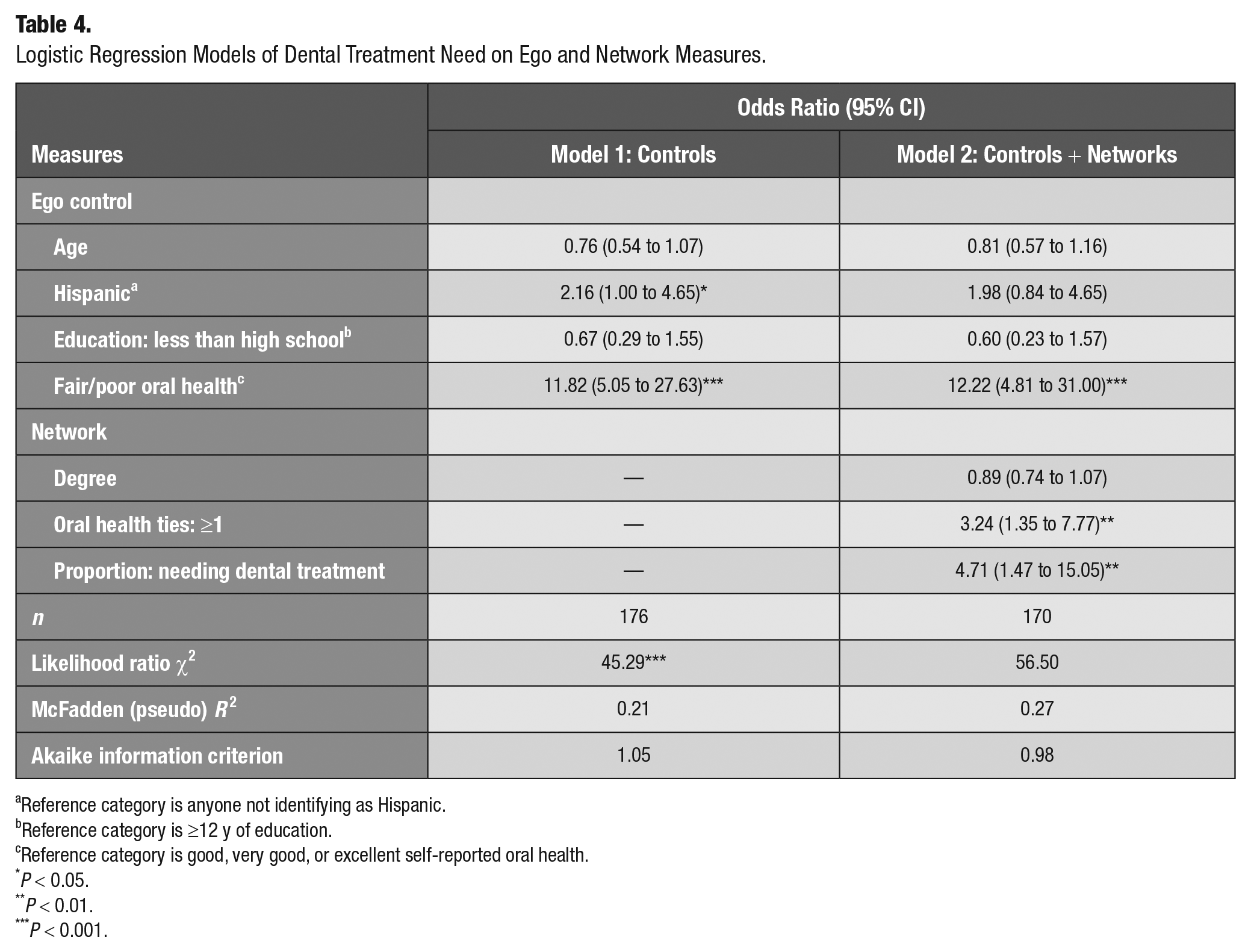
Reference category is anyone not identifying as Hispanic.
Reference category is ≥12 y of education.
Reference category is good, very good, or excellent self-reported oral health.
P < 0.05.
P < 0.01.
P < 0.001.
General Health Status
Table 2 presents the results for general health status. The preferred model containing network characteristics suggested that increasing age is significantly associated with the odds of fair or poor general health. The proportion of ties with good, very good, or excellent health was strongly inversely associated with the odds of having fair or poor general health (odds ratio [OR], 0.19; 95% CI, 0.07 to 0.55), and the proportion of ties that women talk to daily was positively associated with the odds of fair/poor general health (OR, 5.89; 95% CI, 1.73 to 19.97).
Oral Health Status
Table 3 presents the results for self-reported oral health status. The preferred model containing network characteristics suggested that women who reported having their last dental visit >1 y ago had significantly greater odds of fair or poor oral health status (OR, 2.81; 95% CI, 1.29 to 6.13) and that women with less than a high school education had greater odds of fair or poor oral health as compared with women with more educational attainment (OR, 2.30; 95% CI, 1.01 to 5.22). The proportion of ties living in Boston was inversely associated with the odds of reporting fair or poor oral health status (OR, 0.13; 95% CI, 0.03 to 0.54). Similarly, as the proportion of ties with good, very good, or excellent oral health status increased, the odds of egos reporting fair or poor oral health decreased (OR, 0.13; 95% CI, 0.05 to 0.37).
Dental Treatment Need
Table 4 presents the results for dental treatment need. In the preferred model with network characteristics, ego fair or poor oral health status positively corresponded to treatment need (OR, 12.22; 95% CI, 4.81 to 31.00). Women with ≥1 oral health discussants in their network had greater odds of needing dental treatment (OR, 3.24; 95% CI, 1.35 to 7.77). Additionally, the proportion of ties needing treatment was positively associated with the odds of egos reporting that they need dental treatment (OR, 4.71; 95% CI, 1.47 to 15.05).
Dental Service Utilization
Table 5 presents results for dental health service utilization in the past year. The preferred model containing network characteristics suggested that fair or poor oral health was associated with most recent dental visit being >1 y ago, as compared with good, very good, or excellent oral health (OR, 3.97; 95% CI, 1.82 to 8.67). The proportion of participants’ ties that had visited a dentist in the past year was inversely associated with the odds that the ego had their last visit >12 mo ago (OR, 0.26; 95% CI, 0.07 to 0.89).
Logistic Regression Models of No Annual Dental Visit on Ego and Network Measures.
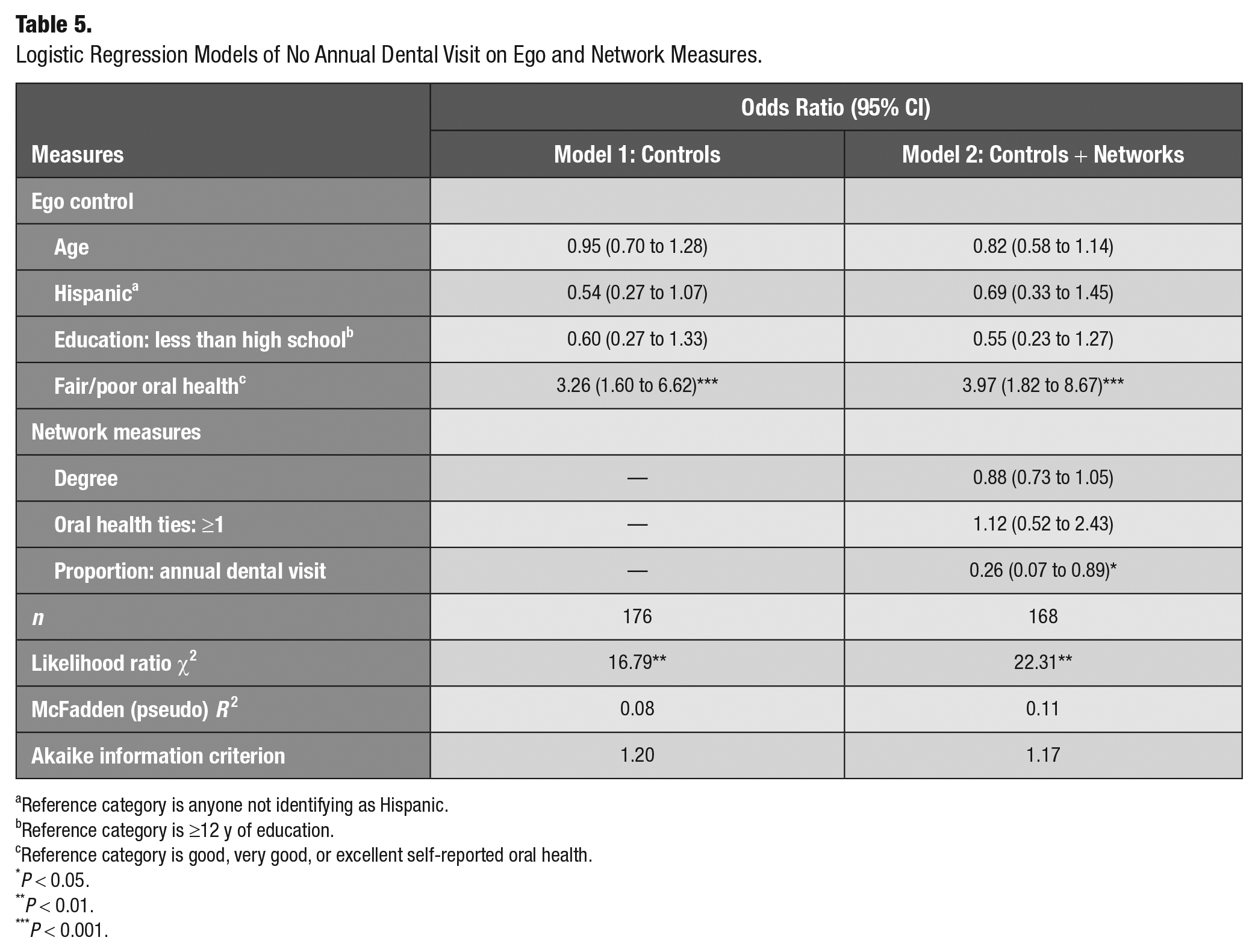
Reference category is anyone not identifying as Hispanic.
Reference category is ≥12 y of education.
Reference category is good, very good, or excellent self-reported oral health.
P < 0.05.
P < 0.01.
P < 0.001.
Discussion
We found that social networks were associated with oral health outcomes in a population of women living in public housing. Inclusion of network characteristics improved model fit for all outcomes assessed, and the estimated ORs for some network characteristics were quite large. Previous research has demonstrated the salience of social characteristics in oral health (Sabbah et al. 2011; Burr and Lee 2013; Jang et al. 2014; Watt et al. 2014; Sadeghipour et al. 2017; Pullen et al. 2018; Pullen et al. 2019; Vettore et al. 2022). Our study expands on these findings to suggest that social network characteristics are associated with oral health in a population of adult women living in public housing, a population that may be generally reflective of those populations in the United States associated with high social and medical need.
Our findings suggest that the composition of social networks is important for the oral health outcomes that we evaluated and that salient network characteristics may differ across outcomes, which is, as far as we know, a unique contribution to this nascent field. Having oral health discussants had a positive association with the odds of having a dental treatment need. Though we cannot comment on temporality, this would be consistent with existing theories that people with health needs “activate” social networks to obtain resources and support (Perry and Pescosolido 2015). In fact, a recent analysis of health-based homophily among residents of public housing indicated that oral health needs and related risk factors, such as sugary foods and beverage consumption, reflect socially clustered phenomena and may serve as organizing frameworks for networks (Heaton and Gondal 2023). We also found that the number of ties that an ego talks to daily was positively associated with fair or poor general health. This may be indicative of people leveraging social networks for support and information when facing health challenges.
We found that networks tended to be reflective of an individual’s self-reported general and oral health: those with a higher proportion of alters with fair or poor general or oral health were themselves less likely to have good, very good, or excellent general or oral health. Similarly, the proportion of alters who had visited a dentist in the previous year was inversely associated with the odds of the ego not having seen a dentist in the past year. This aligns with findings among Mexican American immigrants in the Midwest (Maupome, McConnell, and Perry 2016; Maupome, McConnell, Perry, et al. 2016). The relationship between network properties and any given outcome tends to be population dependent and may be of particular importance among racial or ethnic minority individuals or those of lower socioeconomic position. Though low socioeconomic position has been associated with higher levels of network instability and turnover (Cornwell 2015), social networks may have heightened relevance in disadvantaged or vulnerable populations, including residents of public housing, because they provide social belonging, information, and resources (Umberson and Karas Montez 2010). Therefore, understanding the nuanced role of social networks in health outcomes among disadvantaged populations may be a critical step toward addressing population health disparities.
Our study is primarily limited by the cross-sectional nature of the data. It is possible that network characteristics influence health status; it is also possible that health status plays a role in social network development. Longitudinal studies will be necessary to track the interplay of social networks and health outcomes over time. Furthermore, the 2-stage recruitment process employed may reduce the study’s generalizability from public housing residents more broadly. As a sensitivity analysis, we included a variable controlling for respondent type in all models. All substantive results held across models; thus, we concluded that type of recruitment did not significantly alter the findings. Finally, our sample size was relatively small, which likely contributed to the imprecision of some estimates. However, the small sample size is appropriate for a preliminary investigation into the overall salience of network analysis in the evaluation of oral health outcomes in this population.
Our results suggest that social networks are relevant to general and oral health in a population of women living in public housing. These findings are a call to consider the broader social context that influences oral health status and decision making, particularly among socially and economically disadvantaged groups. A holistic understanding of oral health disparities, which would underlie effective interventions to reduce them—for example, by leveraging social networks to seed messaging about oral health (Valente an Fosados 2006)—may depend on a careful incorporation of network measures to capture the social context in which individuals live.
Author Contributions
B. Heaton, contributed to conception and design, data acquisition, analysis, and interpretation, drafted and critically revised the manuscript; J.C. Bond, contributed to interpretation, drafted and critically revised the manuscript; J. Bae, contributed to data analysis and interpretation, critically revised the manuscript; E. Pullen, contributed to data analysis and interpretation, drafted and critically revised the manuscript. All authors gave final approval and agree to be accountable for all aspects of the work.
Supplemental Material
sj-docx-1-jct-10.1177_23800844231182571 – Supplemental material for Modeling Social Network Influences on Oral Health Outcomes among Women Living in Public Housing
Supplemental material, sj-docx-1-jct-10.1177_23800844231182571 for Modeling Social Network Influences on Oral Health Outcomes among Women Living in Public Housing by B. Heaton, J.C. Bond, J. Bae and E. Pullen in JDR Clinical & Translational Research
Supplemental Material
sj-pptx-2-jct-10.1177_23800844231182571 – Supplemental material for Modeling Social Network Influences on Oral Health Outcomes among Women Living in Public Housing
Supplemental material, sj-pptx-2-jct-10.1177_23800844231182571 for Modeling Social Network Influences on Oral Health Outcomes among Women Living in Public Housing by B. Heaton, J.C. Bond, J. Bae and E. Pullen in JDR Clinical & Translational Research
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute of Dental and Craniofacial Research (awards K99/R00 DE025917 and U54 DE019275).
Data Availability Statement
Requests for data may be made to the corresponding author by email.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.