
Abstract
Introduction:
Developmental disabilities (DDs), obesity, and dental caries are highly prevalent health conditions among adolescents. Evidence indicates that a significant proportion of adolescents with DDs are obese, and those with obesity and dental caries share common risk factors.
Objective:
In this first-ever US-based cross-sectional national study, we assessed the likelihood of adolescents with DDs and obesity experiencing chronic difficulty with decayed teeth, toothaches, bleeding gums, and eating and swallowing due to a health condition among adolescents with DDs and obesity compared to adolescents with no DDs or obesity.
Methods:
For this secondary data analysis study, we used data of 68,942 adolescents aged 10 to 17 y from the 2016 through 2019 National Survey of Children’s Health. Weighted descriptive and bivariate analyses were conducted. Four multiple logistic regression models predicting chronic difficulty in the past 12 mo with decayed teeth, toothaches, bleeding gums, and eating and swallowing due to a health condition were conducted, controlling for other variables.
Results:
The adjusted odds ratio (aOR) of experiencing chronic difficulty in the past 12 mo for adolescents with no DDs or obesity was significantly lower for decayed teeth (aOR, 0.64; 95% confidence interval [CI], 0.51–0.80;
Conclusions:
Results from this study indicate that DD adolescents with obesity have more/greater impending oral health needs than adolescents with no DDs or obesity.
Knowledge Transfer Statement:
Results of this study highlight the high oral health needs and the chronic difficulty adolescents with developmental disabilities and obesity experience compared to adolescents without developmental disabilities and obesity. Targeted oral health policies and interventions that will promote oral health among this high-risk group are recommended.
Keywords
Introduction
The period of adolescence represents a time of significant growth, maturation, and change. Three of the most prevalent such conditions in adolescents are developmental disabilities (DDs), obesity, and dental caries (Centers for Disease Control and Prevention [CDC] 2021; Sanyaolu et al. 2019; Zablotsky et al. 2019).
Children and adolescents with DDs experience delayed developmental milestones and may have disturbances in cognition, motor performance, vision, hearing, speech, or behavior (Institute of Medicine 2001). Due to these conditions’ complex and chronic nature, these children tend to experience a high need for health care services (Boulet et al. 2009). Nationally, the prevalence of DDs among US children and adolescents significantly increased from 16.2% in 2009–2011 to 17.8% in 2015–2017 (Zablotsky et al. 2019). Among the group, adolescents aged 12 to 17 showed the highest prevalence of DDs at 21.1% (2015–2017) and the most significant increase (10.2%) of prevalence in DDs between 2009–2011 and 2015–2017 (Zablotsky et al. 2019).
The prevalence of obesity has also increased significantly among US children and adolescents over the past 2 decades (Sanyaolu et al. 2019). The prevalence of obesity was also the highest among adolescents 12 to 19 y of age at 21.2% (2017–2018) compared to 6- to 11-y-olds (20.3%) and 2- to 5-y-olds (13.4%) (Fryar et al. 2021). Obesity and overweight conditions affect adolescents’ psychological health. Such adolescents experience higher body dissatisfaction, mood disorders, anxiety, and negative self-esteem than normal-weight adolescents. Also, because of obesity’s association with many other health conditions like sleep apnea, hypertension, diabetes, and cardiovascular diseases, obesity is a growing public health concern (Sanyaolu et al. 2019).
The 2011–2016 National Health and Nutrition Examination Survey (NHANES) data showed that adolescents aged 12 to 19 y had the highest dental caries prevalence (56.8%) compared to children aged 6 to 11 y (17.4%) or 2 to 5 y (23.3%) (CDC 2021). Untreated dental caries prevalence was also highest among adolescents 12 to 19 y of age (16.6%) compared to children aged 6 to 11 y (5.2%) and 2 to 5 y (10.4%) (CDC 2021). Untreated dental caries in children and adolescents results in pain, loss of school days, poor nutrition, low self-esteem, and low oral health–related quality of life (US Department of Health and Human Services 2000). Thus, good oral health is a vital and an inherent component of the overall physical and mental health of children and adolescents (US Department of Health and Human Services 2000).
National-level data from 3 major US surveys (NHANES, National Health Interview Survey, and National Survey of Children Health) conducted between 2005 and 2013 show that obesity prevalence among children and adolescents with DDs varied from 19% to 23%. They were at a 27% to 59% higher risk of being obese compared to their normally developed peers (Bandini et al. 2015). In a recent systematic review and meta-analysis of the association between obesity and dental caries in children 6 y of age and younger, the authors found that children with overweight and obesity had a significantly higher dental caries experience than children with normal weight (Manohar et al. 2020). A scoping review of common risk factors identified developmental disabilities as one of the most common, individual-level risk factors for obesity and dental caries (Chi et al. 2017). These studies suggest that there could be an association between DDs, obesity, and experiencing dental caries and other oral health complications.
Understanding the oral health issues that DD adolescents with obesity face, including experiencing chronic difficulty with toothaches, decayed teeth or cavities, bleeding gums, and eating or swallowing due to a health condition, is critical to developing national programs, interventions, and oral health promotion policies. Therefore, we hypothesized that adolescents with no DDs or obesity would be less likely than adolescents with DDs and obesity to experience chronic difficulty with toothaches, decayed teeth or cavities, bleeding gums, and eating or swallowing due to a health condition in the past 12 mo.
Methods
The UCLA Office of the Human Research Protection Program determined that this secondary data analysis study did not meet the definition of human subjects research (IRB#21-00167). This article conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) checklist of items for observational studies.
Data Source
For this cross-sectional study, we used the data from the 2016, 2017, 2018, and 2019 waves of the National Survey of Children’s Health (NSCH), sponsored by the Maternal and Child Health Bureau of the Health Resources and Services Administration (HRSA), to determine the prevalence of experiencing frequent or chronic difficulty in the past 12 mo with toothaches, decayed teeth or cavities, bleeding gums, and eating or swallowing due to a health condition. The data were collected by the US Census Bureau using a 2-stage paper survey instrument and a single-stage web-based survey instrument. During data collection, a screener questionnaire was used to identify households with children ages 0 to 17 y and included a battery of questions to identify children with special health care needs. One child was randomly selected from each eligible household, and that child was the subject of a more detailed topical questionnaire. The parent or the caregiver completed the questionnaire. Survey coverage includes the 50 states and the District of Columbia.
Variables
Main independent variable
Developmental disability (DD) and obesity status, the main independent variable, was developed using multiple variables. Based on parent-reported body mass index (BMI), a child could be categorized into 4 possible categories: underweight (less than 5th percentile), normal weight (5th to 84th percentile), overweight (85th to 94th percentile), and obese (95th percentile or above). We developed the “obesity status” variable by combining the obese and overweight categories into 1 category (obese) and healthy weight and underweight categories into another category (nonobese). We combined normal weight and underweight categories to create a category that is not “overweight/obese” because we primarily were interested in DDs in adolescents “with obesity,” as well as those without DDs and “without obesity.” We used the same methodology used by scientists from the CDC and the HRSA to create a “disability” variable that described whether the sample had 1 or more DDs versus none (Zablotsky et al. 2019). Any child whose parent reported that the child currently has any of the following DDs was considered to have a DD: autism spectrum disorders (ASDs), attention-deficit/hyperactivity disorder (ADHD), blindness, cerebral palsy, hearing loss/deafness, learning disability, intellectual disability, seizures in the past 12 mo, stuttering or stammering in the past 12 mo, or any other developmental delay (Zablotsky et al. 2019). Using the obesity status and disability variables, we categorized adolescents aged 10 to 17 y into 4 different groups: adolescents with 1) DDs and obesity, 2) DDs but no obesity, 3) obesity but no DDs, and 4) no DDs or obesity.
Outcome variables
Four oral health complication–related variables were used as primary outcome variables. Parents were asked, “During the past 12 months, has this child had frequent or chronic difficulty with any of the following?” The following 4 oral health complications were listed among other health conditions: 1) toothaches, 2) decayed teeth, 3) bleeding gums, and 4) eating or swallowing because of a health condition. For each of these conditions, parents had the option of choosing either a “yes” or a “no” response.
Other independent variables
The following sociodemographic variables were included in the study: gender (male/female), race/ethnicity (Hispanic/non-Hispanic, White/non-Hispanic, Black/other), language spoken in the house (Spanish/English/other), the highest level of education in the household (less than high school/high school or GED/some college or technical school/college degree and above), insurance status (public only/private only/private and public/insurance not specified/not insured), and federal poverty level (FPL) (0% to 99% FPL/100% to 199% FPL/200% to 400% FPL/more than 400% FPL), and presence of a medical home (yes/no). We included “having access to a medical home” as a variable because not having a medical home is negatively associated with receiving dental care services and unmet dental care needs among children with special health care needs (Akobirshoev 2019; Lebrun-Harris et al. 2021). The NSCH uses the following 5 components to measure the presence of a medical home: personal doctor or nurse, usual source for sick care, family-centered care, problems getting needed referrals, and effective care coordination when required. Adolescent’s dental visit in the past 12 mo was defined as having had a dental visit if the respondents responded positively to any 1 of the 2 options of “dentist” and “other oral health care provider” to the question, “During the past 12 months, did this child see a dentist or other oral health care provider for any kind of dental or oral health care?”
Statistical analyses
Analyses incorporated the survey elements (i.e., sampling weight, primary sampling variable, and stratification variable) provided by the NSCH. The analyses focused only on the subpopulation of interest (adolescents aged 10 to 17 y). Weighted percentages of the analytical sample were estimated to describe the demographic characteristics and to understand the prevalence of experiencing chronic difficulty with each of the 4 oral health complications in the past 12 mo. Main independent and other variables were compared to experiencing chronic difficulty with toothaches, decayed teeth, bleeding gums, and eating or swallowing. Four different multiple logistic regression models were run to understand factors that predicted the outcomes. The following variables were included as predictors in all 4 models: disability and obesity status, gender, race/ethnicity, language spoken in the household, type of insurance coverage the child had, the highest level of education achieved in the household, FPL, presence of a medical home, and dental visit in the past 12 mo. We used Stata version 17 (StataCorp LLC) to conduct these analyses. Missing data were handled via listwise deletion for all variables except FPL. The NCHS data were released with 6 imputed replicates for the FPL variable. These replicates were used in all analyses that involved the FPL variable. We looked at interactions but did not find any meaningful associations.
Results
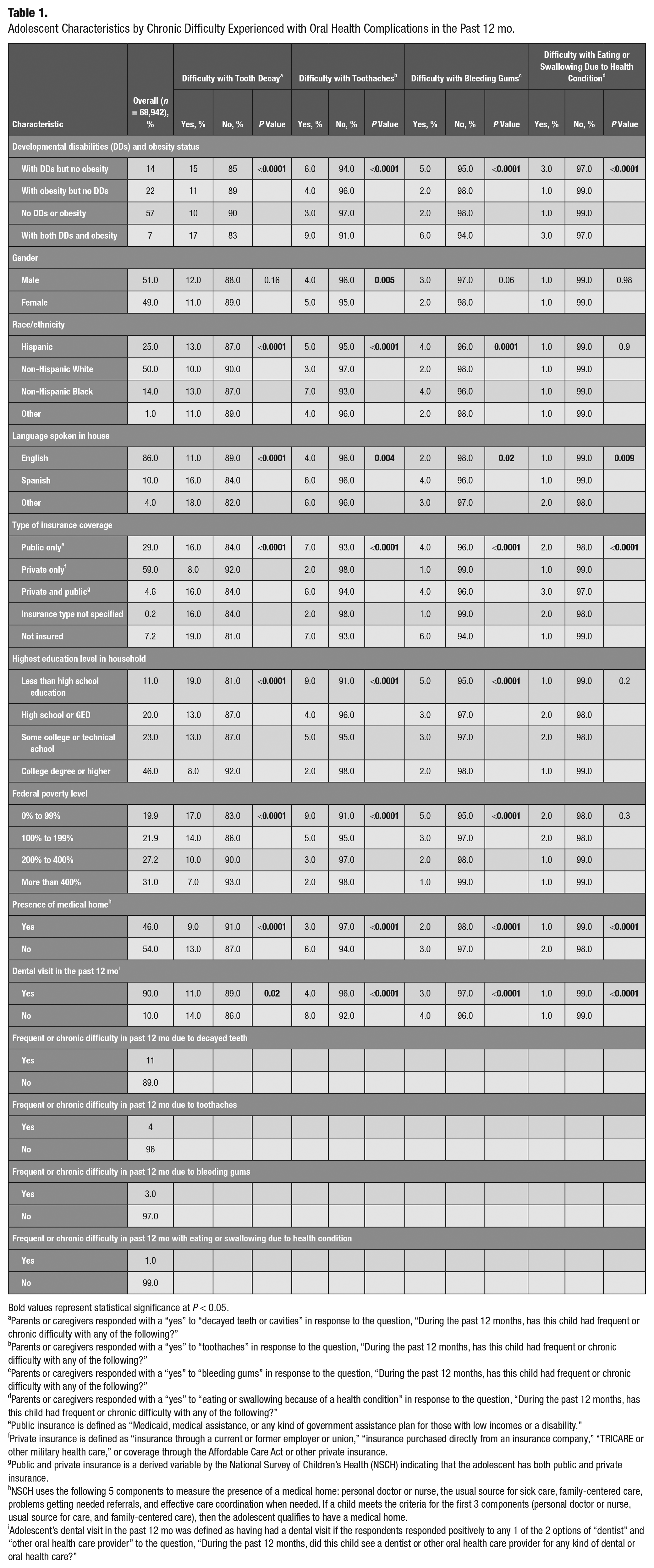
We present the overall analytical sample (n = 68,942) of adolescents aged 10 to 17 y (Table 1). The sample consisted of adolescents with DDs and obesity (7%), DDs but no obesity (14%), obesity but no DDs (22%), and neither DDs nor obesity (57%). Most of the adolescents were male (51%), non-Hispanic White (50%), and from an English-speaking household (86%). Almost 59% of the adolescents had private health insurance, 29% had public health insurance, 7% had no insurance, and the rest had other insurance arrangements. The majority of the adolescents’ parents (70%) had some college education and above, with approximately 58% reporting to live at or above 200% FPL. Parents reported that 46% and 90% of adolescents had a medical home and had a dental visit in the past 12 mo. Parents reported that adolescents experienced chronic or frequent difficulty in the past 12 mo with decayed teeth (11%), toothaches (4%), bleeding gums (3%), and eating or swallowing because of a health condition (1%), respectively.
Adolescent Characteristics by Chronic Difficulty Experienced with Oral Health Complications in the Past 12 mo.
Bold values represent statistical significance at P < 0.05.
Parents or caregivers responded with a “yes” to “decayed teeth or cavities” in response to the question, “During the past 12 months, has this child had frequent or chronic difficulty with any of the following?”
Parents or caregivers responded with a “yes” to “toothaches” in response to the question, “During the past 12 months, has this child had frequent or chronic difficulty with any of the following?”
Parents or caregivers responded with a “yes” to “bleeding gums” in response to the question, “During the past 12 months, has this child had frequent or chronic difficulty with any of the following?”
Parents or caregivers responded with a “yes” to “eating or swallowing because of a health condition” in response to the question, “During the past 12 months, has this child had frequent or chronic difficulty with any of the following?”
Public insurance is defined as “Medicaid, medical assistance, or any kind of government assistance plan for those with low incomes or a disability.”
Private insurance is defined as “insurance through a current or former employer or union,” “insurance purchased directly from an insurance company,” “TRICARE or other military health care,” or coverage through the Affordable Care Act or other private insurance.
Public and private insurance is a derived variable by the National Survey of Children’s Health (NSCH) indicating that the adolescent has both public and private insurance.
NSCH uses the following 5 components to measure the presence of a medical home: personal doctor or nurse, the usual source for sick care, family-centered care, problems getting needed referrals, and effective care coordination when needed. If a child meets the criteria for the first 3 components (personal doctor or nurse, usual source for care, and family-centered care), then the adolescent qualifies to have a medical home.
Adolescent’s dental visit in the past 12 mo was defined as having had a dental visit if the respondents responded positively to any 1 of the 2 options of “dentist” and “other oral health care provider” to the question, “During the past 12 months, did this child see a dentist or other oral health care provider for any kind of dental or oral health care?”
Frequent or chronic difficulty in the past 12 mo with decayed teeth (17%), toothaches (9%), and bleeding gums (6%) was much more common in adolescents with both DDs and obesity than any other group (Table 1). Adolescents with neither DDs nor obesity were the least affected with decayed teeth (10%) and toothaches (3%). Non-Hispanic White adolescents were the least affected with decayed teeth (10%) and toothaches (3%) compared to adolescents from other racial/ethnic groups. Adolescents living in English-speaking households were the least affected with decayed teeth (11%), toothaches (4%), bleeding gums (2%), and difficulty eating or swallowing due to a health condition (1%) compared to adolescents from other language speaking households. Adolescents with no insurance had greater difficulty with decayed teeth (19%), toothaches (7%), and bleeding gums (6%) compared to those with private insurance. Adolescents from a household that had a less than high school education compared to those from the highest education level were the most affected with decayed teeth (19%), toothaches (9%), and bleeding gums (5%). Those living below 100% FPL were the most affected with decayed teeth (17%), toothaches (9%), and bleeding gums (5%). In comparison, those living above 400% FPL had the least difficulty with decayed teeth (7%), toothaches (2%), and bleeding gums (1%). Adolescents who had access to a medical home had less chronic difficulty with decayed teeth (9% versus 13%), toothaches (3% versus 6%), bleeding gums (2% versus 3%), and eating or swallowing due to a health condition (1% versus 2%). Adolescents who visited a dental office in the past 12 mo had less chronic difficulty with decayed teeth (11% versus 14%), toothaches (4% versus 8%), and bleeding gums (3% versus 4%) compared to those who did not (Table 1).
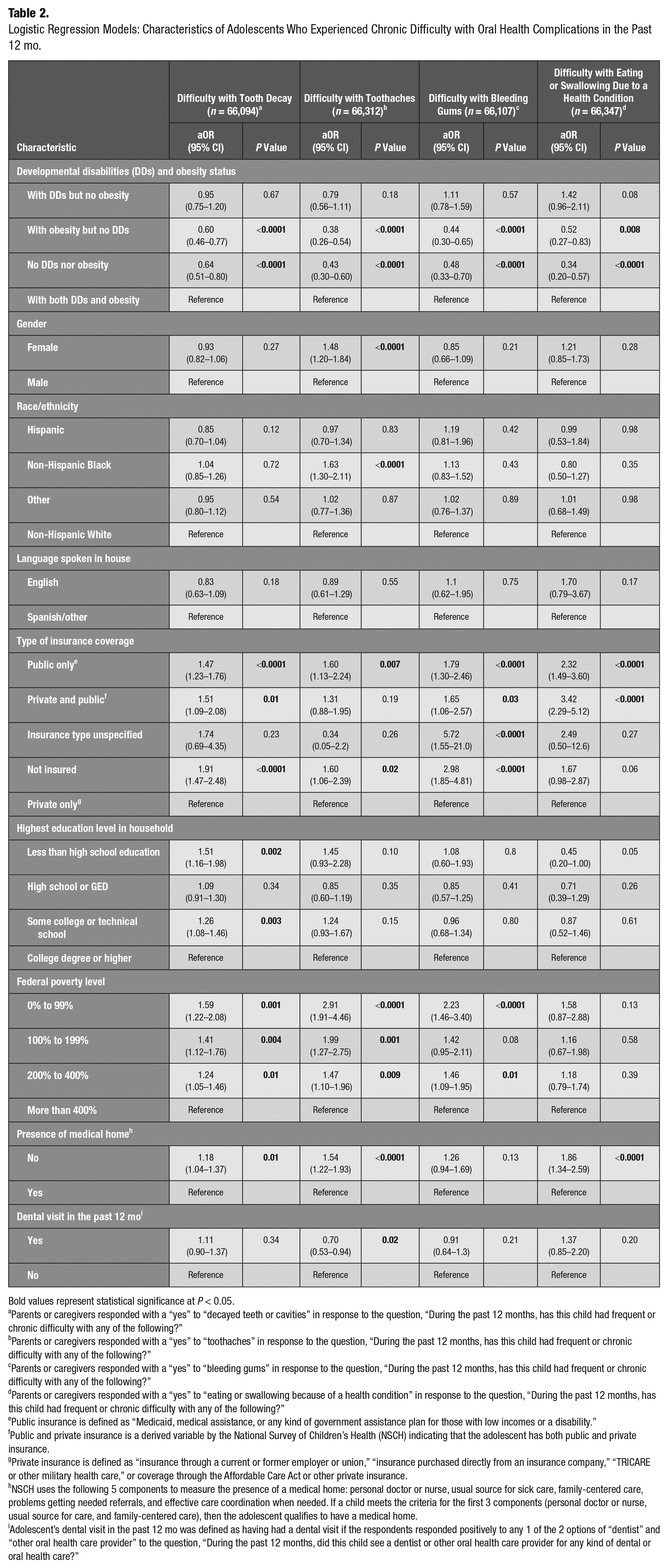
Four multiple logistic regression models were run (Table 2). The 4 binary outcomes were chronic difficulty in the past 12 mo with 1) tooth decay, 2) toothaches, 3) bleeding gums, and 4) eating or swallowing due to a health condition. In all 4 logistic regression models, the overall test of the “disability and obesity status” variable was statistically significant, and the pattern of results was consistent across the models. Specifically, 3 results were observed for all models. First, there was no statistically significant difference between the group with DDs and obesity and the group with DDs but no obesity. Second, there was a statistically significant difference between the group with DDs and obesity and those with obesity but no DDs. Third, there was also a statistically significant difference between the group with DDs and obesity and the group with neither DDs nor obesity. The adjusted odds ratios (aORs) ranged from 0.34 to 0.64 (see Table 2 for all adjusted odds ratios, 95% confidence intervals [CIs], and P values). The odds of experiencing chronic difficulty in the past 12 mo with decayed teeth (aOR, 0.60; 95% CI, 0.46–0.77; P < 0.0001), toothaches (aOR, 0.38; 95% CI, 0.26–0.54; P < 0.0001), bleeding gums (aOR, 0.44; 95% CI, 0.30–0.65; P < 0.0001), and eating or swallowing due to a health condition (aOR, 0.52; 95% CI, 0.27–0.83; P = 0.008) significantly decreased by 40%, 62%, 56%, and 48%, respectively, among adolescents with obesity but no DDs, compared to adolescents with both DDs and obesity, holding all other variables in the model constant. Adolescents with DDs but no obesity were as likely as those with DDs and obesity to experience difficulty with all 4 oral health complications.
Logistic Regression Models: Characteristics of Adolescents Who Experienced Chronic Difficulty with Oral Health Complications in the Past 12 mo.
Bold values represent statistical significance at P < 0.05.
Parents or caregivers responded with a “yes” to “decayed teeth or cavities” in response to the question, “During the past 12 months, has this child had frequent or chronic difficulty with any of the following?”
Parents or caregivers responded with a “yes” to “toothaches” in response to the question, “During the past 12 months, has this child had frequent or chronic difficulty with any of the following?”
Parents or caregivers responded with a “yes” to “bleeding gums” in response to the question, “During the past 12 months, has this child had frequent or chronic difficulty with any of the following?”
Parents or caregivers responded with a “yes” to “eating or swallowing because of a health condition” in response to the question, “During the past 12 months, has this child had frequent or chronic difficulty with any of the following?”
Public insurance is defined as “Medicaid, medical assistance, or any kind of government assistance plan for those with low incomes or a disability.”
Public and private insurance is a derived variable by the National Survey of Children’s Health (NSCH) indicating that the adolescent has both public and private insurance.
Private insurance is defined as “insurance through a current or former employer or union,” “insurance purchased directly from an insurance company,” “TRICARE or other military health care,” or coverage through the Affordable Care Act or other private insurance.
NSCH uses the following 5 components to measure the presence of a medical home: personal doctor or nurse, usual source for sick care, family-centered care, problems getting needed referrals, and effective care coordination when needed. If a child meets the criteria for the first 3 components (personal doctor or nurse, usual source for care, and family-centered care), then the adolescent qualifies to have a medical home.
Adolescent’s dental visit in the past 12 mo was defined as having had a dental visit if the respondents responded positively to any 1 of the 2 options of “dentist” and “other oral health care provider” to the question, “During the past 12 months, did this child see a dentist or other oral health care provider for any kind of dental or oral health care?”
The logistic regression analyses showed that gender and race/ethnicity did not have a significant influence in having chronic difficulty with oral health complications except that the odds of having chronic difficulty with toothaches increased by 48% among female adolescents (aOR, 1.48; 95% CI, 1.20–1.84; P < 0.0001) and 63% among non-Hispanic Black adolescents (aOR, 1.63; 95% CI, 1.30–2.11; P < 0.0001) compared to their counterparts. Adolescents with public insurance and no insurance were consistently and significantly at higher odds of having chronic difficulty due to decayed teeth, toothaches, and bleeding gums compared to adolescents with private insurance. Adolescents in households with lower than high school education compared to the highest education level (aOR, 1.51; 95% CI, 1.16–1.98; P = 0.002) and with some college or technical school education (aOR, 1.26; 95% CI, 1.08–1.46; P = 0.003) were at higher odds of experiencing chronic difficulty with decayed teeth compared to those adolescents in households with a college degree or higher as the highest education level. The educational status of the household was not a significant predictor of having chronic difficulty with the other 3 outcomes (toothaches, bleeding gums, eating, and swallowing due to a health condition). FPL was a significant predictor of having chronic difficulty with decayed teeth and toothaches, with adolescents living below 400% FPL consistently being affected more than those living above 400% FPL. The odds of chronic difficulty with decayed teeth (P = 0.01), toothaches (P < 0.0001), and eating or swallowing due to a health condition (P < 0.0001) significantly increased between 18% and 86% among adolescents with no medical home compared to those with a medical home but not for bleeding gums (P = 0.13). Dental visit in the past 12 mo for any kind of oral health care was not significantly associated with decayed teeth (P = 0.34), bleeding gums (P = 0.21), or eating or swallowing due to a health condition (P = 0.20). However, the odds of experiencing chronic difficulty with toothaches significantly decreased by 30% among those who had a dental visit in the past 12 mo compared to those who did not (P = 0.02).
Discussion
The period of adolescence is a unique stage of human development, during which adolescents experience rapid physical, cognitive, and psychosocial growth (MacKay and Duran 2007). Adolescence is also a period when many health problems may first emerge (MacKay and Duran 2007). The national data described above confirm that adolescents have the highest prevalence of DDs, obesity, and dental caries compared to younger children. For all these reasons, DD adolescents with obesity can be considered a high-risk group for health complications, including oral health complications. However, studies assessing oral health conditions and complications among this high-risk group of adolescents are rare. In a small study of 119 children in Poland, children with ADHD had a higher prevalence of abnormal body weight, hip circumference, and BMI and a higher frequency of dental caries than non-ADHD children (Paszynska et al. 2020). A study in Taif City, Saudi Arabia, found that special needs children with obesity were at 1.7 times greater risk for dental caries compared to special needs children without obesity (Mohamed et al. 2021). To understand the oral health needs of DD adolescents with obesity in the United States, we conducted a secondary data analysis study using the 2016–2019 NSCH. Our analytical sample represented approximately 33.27 million US adolescents 10 to 17 y of age. The adolescents with DDs and obesity made up 7% of the sample, representing approximately 2.31 million high-risk US adolescents.
The logistic regression analyses revealed some important findings for dental and public health professionals. Results showed that DD adolescents with obesity compared to healthy adolescents with no DDs or obesity were significantly at higher odds of experiencing all 4 oral health complications. DD adolescents with obesity were consistently the most affected by all 4 oral health complications compared to adolescents with obesity but no DDs and adolescents with no DDs or obesity. DD adolescents with obesity were as likely as those with DDs but no obesity to be affected by all 4 oral health complications. This is an important finding that suggests DD adolescents with obesity are a high-risk group.
The American Academy of Pediatrics (AAP) indicates that a medical home is an approach to providing comprehensive and high-quality health care services to children (AAP 2021). A child who has a medical home will have easier access to and receive family-centered, continuous, comprehensive, compassionate, coordinated, and culturally effective care (AAP 2021). An intriguing finding from our study, which supports the advantages of a medical home, was that the adolescents having access to a medical home were less likely to have chronic difficulty with toothaches, decayed teeth, bleeding gums, and eating or swallowing because of a health condition in the past 12 mo. While the percent difficulty was not large, the association was both significant and consistent. In a previous study, children with special health care needs (CSHCN) who did not have a medical home were 70% more likely to experience poor oral health compared to CSHCN with a medical home (Akobirshoev et al. 2019). In this study, even among non-CSHCN, those without a medical home were 50% more likely to experience poor oral health compared to non-CSHCN with a medical home. Having a medical home also significantly predicted unmet dental care needs in non-CSHCN (Akobirshoev et al. 2019). Therefore, it is not surprising that our study found very similar associations. However, this association needs to be further explored to understand how or why having access to a medical home improves oral health, since the data showed that dental visits in the past 12 mo did not predict experiencing chronic difficulty with oral health complications except for toothaches. Those who had a dental visit in the past 12 mo compared to those who did not were significantly less likely to experience chronic difficulty with toothaches. This finding shows that having a dental visit, and possibly identifying and treating the root causes, can prevent extreme complications like toothaches from occurring. However, it is intriguing that those who did and did not have a dental visit in the past 12 mo did not significantly differ with experiencing chronic difficulty with the other 3 oral health complications.
Many previous studies have shown the racial/ethnic disparities in oral health status among children and adolescents (Flores and Tomany-Korman 2009; Guarnizo-Herreño and Wehby 2012; Gupta et al. 2018). However, in our study, race/ethnicity was only a significant predictor of a higher rate of difficulty with toothaches for non-Hispanic Blacks.
Maintaining optimal oral health requires easy access to dental care; however, previous studies show that children and adolescents with DDs experience delays in dental visits (Chi et al. 2011) often associated with difficulty finding a dentist who is willing to provide care (Nelson et al. 2011). The finding that DD adolescents with obesity have greater risk suggests they should access dental offices and receive not only preventive dental care services but also other needed dental care services to maintain optimal oral health care services. This warrants a study to understand access to dental care and utilization of dental care services among DD adolescents with obesity.
This study is not without limitations. First, the data are based on reports from parents about their children. There is a possibility of both recall bias and social desirability bias. Furthermore, as in any survey, nonresponse bias analysis is possible. However, the Office of Management and Budget Standards regularly conducts a nonresponse bias analysis on the NSCH. No strong or consistent evidence of nonresponse bias has been identified in the 2016, 2017, 2018, and 2019 surveys. We used a standard case definition to identify adolescents with DDs that was developed by researchers from the CDC and HRSA and has been often used in the medical literature. We were unable to assess the association between each type of DD and oral health complications because the subsample size for each category was very low, which would have compromised the validity. The survey data are predominantly based on parents’ reports of their children’s behaviors, health conditions, and diseases. Therefore, it is justifiable to question the accuracy of parental assessments of child and adolescent health status because parent reports of health conditions were not clinically validated in the NSCH. However, studies have shown high concordance between parent reports and their children’s health behaviors, health conditions, and health outcomes (Daniel et al. 2012; Fisher et al. 2014; Chai et al. 2019). Although the associations were statistically significant for all 4 oral health complications in the regression models between DD adolescents and those with no DDs or obesity, we must consider the clinical significance of these associations, especially for bleeding gums and difficulty with eating or swallowing. This is because differences in these 2 outcomes between DD adolescents with obesity and those with no DDs or obesity vary only by 2% to 4%. Therefore, these associations should be interpreted with caution. Despite these limitations, this is the first-ever study using national-level data to establish the associations between disability and obesity status and oral health complications among a high-risk group, DD adolescents with obesity, making up at least 2.31 million adolescents in the United States.
Conclusions
DD adolescents with obesity experienced chronic difficulty with all 4 oral complications compared to adolescents without DDs or obesity, indicating that oral health needs are much higher in this high-risk group of adolescents than those without DDs or obesity. Further studies are needed to understand the barriers in oral health maintenance and the ability to access dental care among this understudied group.
Author Contributions
V. Bhoopathi, contributed to conception, design, data acquisition, analysis, or interpretation, drafted and critically revised the manuscript; C. Wells, contributed to data analysis and interpretation, critically revised the manuscript; F. Ramos-Gomez, contributed to data interpretation, critically revised the manuscript; K.A. Atchison, contributed to conception, data acquisition, analysis, or interpretation, drafted and critically revised the manuscript. All authors gave final approval and agree to be accountable for all aspects of the work.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project is supported by the Health Resources and Services Administration (HRSA) of the US Department of Health and Human Services (HHS) under [R41MC42491] the Autism Secondary Data Analysis Research (SDAR) Program. The information, content, and/or conclusions are those of the authors and should not be construed as the official position or policy of, nor should any endorsements be inferred by, HRSA, HHS, or the US government.