
Abstract
This study draws on symbolic empowerment theory to examine the mental health significance of Donald Trump’s unexpected presidential election victory in fall 2016 for white male veterans. Some whites, including military veterans, gravitated toward Trump’s messaging of restoring traditional power structures and defending white masculine cultural and economic dominance. The authors hypothesized that white male veterans would experience improved mental health after Donald Trump’s installation as president and commander in chief. The authors also ™hypothesized that white male veteran mental health after the 2016 election could depend on state-level sociopolitical contexts. With nationally representative survey data from the Behavioral Risk Factor Surveillance System, the authors tested these hypotheses by predicting poor mental health days white male veterans experienced preelection and postelection in fall 2016. The authors found no time period main effects. However, veterans living in Trump-won states reported .38 fewer poor mental health days postelection, whereas those living in Clinton-won states reported .54 more poor mental health days postelection. Additionally, veterans in states where Trump’s popular vote advantage was high experienced fewer poor mental health days postelection. These findings suggest that symbolic empowerment theory may provide a unique framework for understanding health outcomes in the context of political geography and sociopolitical change.
Keywords
Donald Trump’s 2016 presidential run directed nationalist and exclusionary rhetoric toward certain U.S. citizens, immigrants, and Muslims. He alienated many voters but cultivated feelings of group threat, precarity, and relative deprivation among his supporters (Cherlin 2016; Francis 2018; Johnson 2017). Many white men felt aggrieved entitlement, that they were the rightful heirs to America’s bounty, and that government bureaucrats took their birthright and gave it to undeserving minorities, immigrants, and women (Kimmel 2017). Trump stoked those feelings by promising a return to a masculine America, free from political correctness and social justice (Esposito and Romano 2018). Many white men gravitated toward his messaging of American exceptionalism, hegemonic masculinity, and disdain for women and nonwhite groups (Carian and Sobotka 2018; Johnson 2017; Katz 2016; Ott and Dickinson 2019; Smith and Hanley 2018). Following eight years of the first Black U.S. president, juxtaposed with the prospect of the first female U.S. president, Trump exploited feelings of urgency, panic, and perceived aggrievement among his followers (Esposito and Romano 2018; Johnson 2017; Ott and Dickinson 2019). Trump lost the popular vote but clinched an Electoral College victory by winning traditional Republican states and flipping six states won previously by Barack Obama in 2012 (Farley 2019).
Factors such as the Electoral College, state-controlled election processes, and electoral changes routinely influence federal elections. These factors, especially electoral change, were important in 2016. An important aspect of the 2016 presidential election was electorate conversion (Farley 2019; Hill, Hopkins, and Huber 2021). For example, Iowa, Michigan, Ohio, Pennsylvania, and Wisconsin all shifted at least 10 points from Obama in 2008 to Trump in 2016, with white Obama voters driving the shift (Farley 2019). Thus, state-level sociopolitical contexts (e.g., political cultures, policy environments, and concentration among Trump voters) were important in 2016. Another important factor in Trump’s victory was the support of white veterans (Maniam 2017).
Trump’s campaign rhetoric offended many U.S. constituents, but the majority of white veterans supported him (Maniam 2017). White veterans supported Trump despite comments many thought would offend military-connected voters. For example, Trump verbally disrespected Senator John McCain (a veteran and former prisoner of war) and the family of a soldier killed in action and questioned U.S. generals’ efficacy (Gibbons-Neff and LaMothe 2016; LaMothe 2016). Furthermore, Trump avoided the Vietnam War with five draft deferments. Still, he received 60 percent of the veteran vote in the 2016 election (Maniam 2017). We suspect that white men populated most of the 60 percent because they are overrepresented in the military, and white veterans tend to be conservative (Maclean and Cassidy Forthcoming; Maniam 2017; U.S. Department of Veterans Affairs, National Center for Veterans Analysis and Statistics 2018). Alternatively, some white veterans rejected Trump. For example, of the 354 retired generals and admirals who composed Mitt Romney’s 2012 campaign military advisory council, only 36 appeared on Trump’s council (Timm 2016). Thus, Trump was still polarizing among white veterans. Although he addressed veteran concerns, his strategy focused primarily on emotional appeal rather than traditional Republican policy stances (Gibbons-Neff and LaMothe 2016; Ott and Dickinson 2019). Trump was victorious largely because of how he made many whites feel.
This study investigates the mental health significance of Trump’s 2016 presidential election for white male veterans. We invoke symbolic empowerment theory to frame our hypotheses (Brown, Solazzo, and Gorman 2021). Analyzing nationally representative data from the 2016 Behavioral Risk Factor Surveillance System (BRFSS; Centers for Disease Control and Prevention 2016), we hypothesize that white male veterans would experience improved mental health postelection, compared with preelection. Additionally, we investigate whether symbolic empowerment depended on state-level sociopolitical contexts. Hence, we hypothesized that white male veterans living in Trump-won states and those living in states where Trump won handily would experience improved mental health postelection compared with preelection. Findings suggest Trump’s presidential victory empowered white male veterans in Trump-won states but disempowered those in Clinton-won states.
Symbolic Empowerment Theory
Symbolic empowerment refers to social and psychological uplift experienced by an aggrieved group when one of its members attains an authoritative position (Brown et al. 2021, 2024). That individual’s authority and political ascendancy can empower aggrieved constituents excluded from such positions, signaling broader societal inclusion and influence (Goldman and Mutz 2014; Simien 2015). Moreover, symbolic empowerment relies on descriptive representation, where a leader shares physical, social, or experiential traits with aggrieved constituents (Brown et al. 2024; Simien 2015). Such representation signals a potential power shift toward aggrieved constituents, affirming their social status (Brown et al. 2024; Simien 2015). These conditions of shared identity and political ascendancy may generate a sense of collective effervescence among constituents, which can manifest as political mobilization and voter turnout, as in the historic boost in nonwhite participation in the 2008 and 2012 presidential elections (Krogstad and Lopez 2017; Lopez and Taylor 2009), and high levels of Black women’s support for Kamala Harris (Alford 2024). Consequently, research on descriptive representation has laid the foundation for understanding how symbolic empowerment shapes political attitudes, behaviors, and efficacy (Banducci, Donovan, and Karp 2004; Bobo and Gilliam 1990; Gay 2002; Gleason and Stout 2014; Parker 2016; Simien 2015; Stout and Tate 2013). For example, Black residents in districts with Black congressional representatives reported greater confidence in government responsiveness than those without such representation (Gay 2002; Gleason and Stout 2014; Merolla, Sellers, and Fowler 2013). Moreover, Broockman (2014) found that constituents were more likely to communicate with legislators of the same race, indicating descriptive representation encourages political participation.
Prior studies have demonstrated the health effects of symbolic empowerment (Brown et al. 2021, 2024; Gorman, Brown, and Culver 2023; Malat, Timberlake, and Williams 2011; Morey et al. 2021; Stolte et al. 204). For example, Malat et al. 2021; showed improvements in self-rated health for Black people and Hispanics immediately following Barack Obama’s 2008 Democratic Party nomination. Stolte et al. (2024) found postelection improvement in perinatal health within Black communities after Obama’s 2008 victory. Furthermore, prior studies showed that Obama’s 2008 presidential victory delivered a temporary mental health boost for Black men generally (Brown et al. 2021) and Black and Hispanic veterans specifically (Gorman et al. 2023). Regarding 2016, Morey et al. (2021) examined the impact of the presidential election on population health. They found that non-Latinx white populations in Clinton-won states and English-speaking Latinx people in Trump-won states reported worse mental health during a five-month period postelection, suggesting that they experienced disempowerment. Building on established connections between symbolic empowerment and health, we consider how this association may manifest among groups not historically considered marginalized.
Because symbolic empowerment relies on descriptive representation and feelings of group inclusion, status affirmation, and societal recognition, whites may also experience health benefits when political representation reinforces their identity and values. Donald Trump’s 2016 election victory followed Obama’s eight-year presidency and prevented continued Democratic leadership of the executive branch led by the first female president. The potential Democratic transition coincided with discussions of whites’ perceived vulnerability within a society undergoing demographic and cultural change (Craig and Richeson 2017; Jardina 2019; Norton and Sommers 2011; Rasmussen et al. 2022). Many whites, especially men, feel entitled to disproportionate wealth, power, and stability (Esposito and Romano 2018). Prior studies showed that white Americans reported perceptions of being on the losing team in the zero-sum game of race relations (Norton and Sommers 2011; Rasmussen et al. 2022). Trump’s campaign rhetoric manufactured precarity and perceived aggrievement among his base through four interlocking themes: felt powerlessness as a sign of agency, democracy as danger, raced and gendered hostility toward otherness, and charisma as compensatory for lack (Johnson 2017). Donald Trump leveraged white Americans’ feelings of vulnerability and relative deprivation by framing his political movement as a return to white American dominance, hence the “again” conclusion to his campaign slogan.
A racialized version of hegemonic masculinity (i.e., patterns of practice allowing white men’s dominance over women and nonwhite men to continue; Connell and Messerschmidt 2005) undergirded Trump’s appeal to white men (Dignam et al. 2021; Esposito and Romano 2018; Smirnova 2018). He connected with less educated and downwardly mobile white men who felt that the world and political establishment were no longer theirs, often through displays of humor or vitriol toward women and perceived weaker men (Katz 2016; Kimmel 2017; Smirnova 2018). In turn, his displays of racism, sexism, and nativism elevated him to champion status among aggrieved white men, many of whom shared his prejudices (Katz 2016; Smith and Hanley 2018).
Many white Americans perceived Trump’s 2016 election as restoring traditional power structures (Pettigrew 2017; Sides, Tesler, and Vavreck 2017, 2019). His campaign mobilized white identity politics and feelings of relative deprivation with overt racial and gender-based appeals (Jardina 2019; Johnson 2017), positioning his candidacy as a defense of white masculine cultural and economic dominance. Prior studies showed that symbolic racism and modern prejudice, right-wing authoritarianism, social dominance orientation, ethnic identification, xenophobia, racial resentment, and sexism all predicted support for Trump among whites in 2016 (Buyuker et al. 2021; Choma and Hanoch 2017; Farley 2019; Major, Blodorn, and Blascovich 2018; Pettigrew 2017). These social psychological constructs signal aggression and prejudice toward outgroups, deference to authority, and hierarchical views of society characterized by domination of lower status groups (Pettigrew 2017).
Historical whiteness, masculinity, and a rigid hierarchy mold military culture. White men represent the military’s modal demographic (U.S. Department of Defense, Military OneSource 2024). The military was the first U.S. institution to desegregate and requires racial cohesion, hence it is sometimes portrayed as racially progressive (Burk and Espinoza 2012; Butler and Holmes 1981). However, the military has treated racial diversity and multiculturalism as tools for mission readiness, not as steps toward genuine racial egalitarianism (Armstrong 2024). Following recent legislative changes, women began serving at higher rates and in combat roles, challenging the military’s masculine culture (Crowley and Sandhoff 2017; Moore 2017). Military leadership tends to dismiss advocacy for repairing historical wrongs toward Black people, women, and other racial, ethnic, and sexual minority groups as examples of critical race theory, diversity, equity, and inclusion initiatives, gender ideology, or wokeness (i.e., buzzwords used to defend white hegemonic masculinity within U.S. institutions; see Spoehr 2022 and U.S. Department of War 2025 as examples). Thus, veterans served within a patriarchal color-blind habitus that perpetuates white hegemonic masculinity.
Many veterans live by values, customs, and norms associated with military culture after separation or retirement (McCormick et al. 2019). Considering alignment between some of Trump’s campaign rhetoric (e.g., masculinity, military strength, nationalism, and white American identity) and values associated with military culture, Trump’s election victory possibly signaled a return to a version of America white male veterans felt was lost and made them feel included, affirmed, and recognized. Donald Trump’s 2016 presidential election provides a novel opportunity to test whether symbolic empowerment extends to white Americans, particularly white male veterans, and how that empowerment associates with well-being.
Hence, we hypothesize that veterans would experience improved mental health postelection compared with preelection (hypothesis 1). Furthermore, Trump’s polarizing 2016 campaign prompts us to investigate whether white male veterans’ mental health depends on state-level sociopolitical contexts (e.g., political cultures, policy environments, and concentration among Trump voters). State-level sociopolitical contexts facilitate the proposal, passage, and implementation of policies that influence social determinants of health (Morey et al. 2021). We assume that veterans living in traditional or recently flipped red (i.e., Republican) or blue (i.e., Democratic) states are exposed to and socialized within qualitatively different sociopolitical environments, which could help empower or disempower them. Prior studies have highlighted the significance of state-level sociopolitical contexts following the 2016 presidential election (Morey et al. 2021; Yan et al. 2021). Thus, we hypothesize that white male veterans living in Trump-won states (hypothesis 2) and those living in states where Trump won handily (hypothesis 3) would experience improved mental health postelection compared with preelection.
Study Contributions
This study makes at least three significant contributions to the literature. First, we examine the mental health of veterans, who suffer disproportionately from posttraumatic stress disorder and suicide (Koven 2017). However, rather than highlighting combat-produced disease and pathology, we examine whether Donald Trump’s installation as president and commander in chief associates with improved mental health. Second, we sharpen symbolic empowerment theory by focusing on white male veterans. White men represent the dominant social group in U.S. society, with 31 white male veterans serving as U.S. presidents (VA News 2019). However, Donald Trump’s presidential election represented a perceived return to white hegemonic masculinity. Its sociological significance may depend upon race and veteran status, among other factors. We examine whites with prior military service and may embrace a return to their perceived status quo. Third, we analyze nationally representative survey data from the 2016 BRFSS and investigate veterans’ mental health before and after November 8, 2016. Future studies can replicate our design to examine additional sociopolitical shifts relevant to veterans (e.g., the beginning or end of combat operations or legislation advancing veterans’ rights) because BRFSS collects data year round.
Methods
Data
We analyzed nationally representative survey data from the 2016 BRFSS (Centers for Disease Control and Prevention 2016). The BRFSS is the United States’ premier system of health-related telephone surveys. It collects state-specific data year round from noninstitutionalized adults regarding risk behaviors, chronic health conditions, and the use of preventive services. Established in 1984, the BRFSS collects more than 400,000 survey interviews annually, making it the world’s largest continuously conducted health surveillance system.
The BRFSS conducts interviews daily through landlines and cell phones during both daytime and evening hours, every month of the calendar year. In 2016, states used a disproportionate stratified sample design for landline samples. States divided landline numbers into two strata on the basis of city block density (i.e., high and medium density), then sampled the two strata to obtain a probability sample representing all households with landlines. BRFSS sampled cell phones randomly from commercially available sampling frames. In 2016, BRFSS response rates, representing median rates for all states and U.S. territories, were 47.7 percent for landlines and 46.4 percent for cell phones. For additional information about the 2016 BRFSS, visit https://www.cdc.gov/brfss/annual_data/annual_2016.html.
The available sample consisted of non-Hispanic white male veterans from the 2016 BRFSS (n = 51,645). We aimed to isolate the contemporaneous effect of Donald Trump’s November 8, 2016, presidential election. Therefore, replicating a method developed by Brown et al. (2021) and used in two other peer-reviewed studies (Brown et al. 2024; Gorman et al. 2023), we restricted the available sample to non-Hispanic white male veterans (n = 7,243) surveyed during one of two time periods: October 9, 2016, to November 7, 2016 (i.e., 30 days before the election), or December 8, 2016, to January 6, 2017 (i.e., a 30-day period starting 30 days after the election). The second period began 30 days postelection, accommodating an “incubation interval” to allow the election’s significance to materialize (see Brown et al. 2021:105). Additionally, the second period’s 30-day lag accounts for the dependent variable’s “during the past 30 days” framing, substantiating potential causal claims. Finally, we retained respondents with complete information on study variables, resulting in an estimation sample of 6,153 white male veterans (see Table 1).
Descriptive Statistics Stratified by Time Period for Poor Mental Health Days, State Won by Trump, Trump-Clinton Percentage Differential, and Control Variables among White Male Veterans in the 2016 Behavioral Risk Factor Surveillance System.
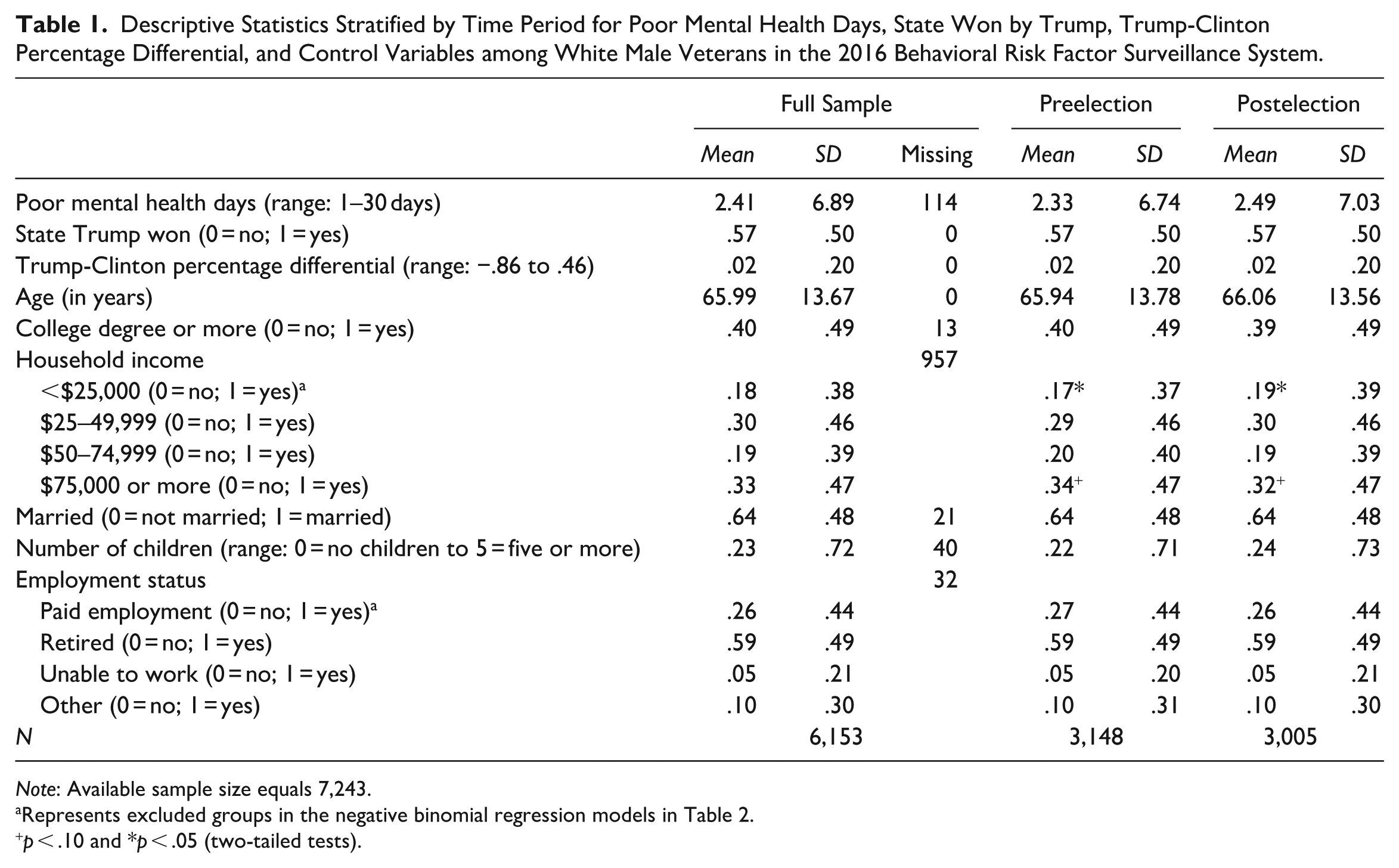
Note: Available sample size equals 7,243.
Represents excluded groups in the negative binomial regression models in Table 2.
p < .10 and *p < .05 (two-tailed tests).
Estimates from Negative Binomial Regression Models Predicting Poor Mental Health Days Using Time Period, State Won by Trump, Trump-Clinton Percentage Differential, and Control Variables among White Male Veterans in the 2016 Behavioral Risk Factor Surveillance System.

Note: Standard errors are shown in parentheses beside coefficients. Standard errors are corrected for within-state clustering. The estimation sample size equals 6,153. The available sample size for these analyses equals 7,243.
Represents excluded groups.
p < .10, *p < .05, **p < .01, and ***p < .001 (two-tailed tests).
Variables
This question captured self-identified veteran status:
Have you ever served on active duty in the United States Armed Forces, either in the regular military or in a National Guard or military reserve unit? Active duty does not include training for the Reserves or National Guard, but DOES include activation, for example, for the Persian Gulf War.
The outcome variable was the number of poor mental health days reported during the past 30 days (range = 0–30). The question read, “Now thinking about your mental health, which includes stress, depression, and problems with emotions, for how many days during the past 30 days was your mental health not good?” Time period was the primary predictor: (0 = preelection vs. 1 = postelection). Time period captured whether the survey interview occurred from October 9, 2016, to November 7, 2016 (i.e., a 30-day period before the election), or from December 8, 2016, to January 6, 2017 (i.e., a 30-day period starting 30 days after the election). We treat the two periods as a control condition and an experimental condition, respectively, with the treatment being Donald Trump’s election on November 8, 2016.
Established social determinants of health (see Braveman, Egerter, and Williams 2011), whether respondents lived in a state where Trump won the popular vote, and the Trump-Clinton percentage differential constituted the control variables. We controlled for age (range = 18 to ≥80 years), college degree or more (no, yes), household income (<$25,000, $25,000–$49,999, $50,000–$74,999, and ≥$75,000), marital status (married, not married), number of children in the household (range = 0 to 5 or more), and employment status (paid employment, retired, unable to work, other).
The BRFSS does not collect data on partisanship (i.e., party identification or political orientation), voting behavior, or attitudes serving as proxies for them (e.g., views on birth control, abortion, affirmative action). The BRFSS omits these data intentionally because it is sponsored by nonpartisan federal agencies. We constructed two variables to capture differences in state-level sociopolitical contexts (e.g., political party control shaping state-level political cultures, policy environments, and voter mobilization efforts) during the 2016 presidential election. The Massachusetts Institute of Technology Election Data and Science Lab (2017) provided information regarding which 2016 presidential candidate received the most votes by state. We recoded state election data to construct a variable indicating whether respondents lived in a state where Trump won the popular vote (i.e., no, yes). The state won by Trump variable accounts for interstate differences in sociopolitical contexts. Additionally, we constructed the Trump-Clinton percentage differential to capture more nuanced differences among states’ sociopolitical contexts during the 2016 presidential election. First, we calculated each candidate’s percentage of the total vote count for each state. Next, we subtracted Hillary Clinton’s vote percentage from Trump’s vote percentage. Thus, the variable represents the difference between Donald Trump’s state vote winning percentage and Hillary Clinton’s state vote winning percentage. It ranged from −.86 (i.e., Clinton outgained Trump by 86 percentage points) to .46 (i.e., Trump outgained Clinton by 46 percentage points).
Whereas the state won by Trump variable captures the difference in state-level sociopolitical contexts, the Trump-Clinton percentage differential accounts for heterogeneity within Trump-won and Clinton-won state categories. For example, Wyoming and Wisconsin are both Trump-won states and hold equal values on the state won by Trump variable. However, Trump won Wyoming handily (percentage differential = .46) and barely won Wisconsin (percentage differential = .01). Alternatively, Clinton won Washington, D.C., handily (percentage differential = −.86) and barely won New Hampshire (percentage differential = −.00). We assume that the sociopolitical contexts between these states and Washington, D.C., would be qualitatively different (i.e., higher percentage differential values indicate more conservative political cultures and environments and the inverse for lower values). Though not proxies for individual partisanship, in some ways, the state won by Trump and the Trump-Clinton percentage differential variables also capture the probability of party affiliation at the aggregate level.
Analytic Strategies
To meet BRFSS sample design standards, states must confirm that sample records represent a probability sample of all households in the state with telephones. A sample record represents a randomly selected telephone number from the list of numbers (i.e., landlines and cell phones) obtained through random-digit dialing techniques. BRFSS respondents are surveyed randomly and continuously across an entire calendar year. Hence, we assume respondents have the same probability of being contacted by telephone on any day of the calendar year. We treat this feature of the BRFSS design as a form of randomization. Presumably, unmeasured characteristics (e.g., poor mental health, enlisted or commissioned status, length of military service, political orientation, racial resentment, voting behavior, or white consciousness) are distributed randomly across the two periods. Data in the estimation sample come from all 50 states and the District of Columbia. We omitted respondents from Guam, Puerto Rico, and the U.S. Virgin Islands. Respondents from these U.S. territories cannot vote in presidential elections and would be missing on the state won by Trump and the Trump-Clinton percentage differential variables.
We present unweighted analyses asserting the time periods represent random assignment (see Brown et al. 2021, 2024; Gorman et al. 2023). Patterns in Table 1, whereby study variables tend not to differ systematically across time periods, support treating the two periods as control and experimental conditions, respectively. Item nonresponse was low (i.e., on average, 1.62 percent missing cases per variable). The household income variable had the most missing cases (n = 957). However, missing cases should not influence the results because they should be distributed randomly across periods (see the “Robustness Checks” section and Appendix 1 for additional analyses on the missingness of household income). We applied negative binomial regression with robust standard errors because the dependent variable originates from a count probability distribution with overdispersion and clustering by respondents’ state of residence. We conducted all analyses in Stata 19.
In Table 1, we present descriptive statistics for white male veterans in the full sample and stratified by time period. In Table 2, we present estimates from negative binomial regression models predicting veterans’ poor mental health days using time period, state won by Trump, Trump-Clinton percent differential, and control variables. To address our hypotheses, we examined time period main effects, and interaction effects between time period and state won by Trump and between time period and the Trump-Clinton percentage differential.
Results
Table 1 presents descriptive statistics for white male veterans in the full sample and stratified by time period. Respondents averaged more than two poor mental health days during the previous 30 days. More than half lived in a state Trump won, and the Trump-Clinton percentage differential equaled .02. Respondents were roughly 66 years old. Forty percent held at least a college degree. A third earned at least $75,000. More than 60 percent were married. Respondents had fewer than one child living in the household. About 60 percent were retired, and more than a quarter held paid employment.
Table 1 shows household income differed significantly across time periods. For example, fewer respondents reported earning $25,000 or less preelection (i.e., 17 percent) than postelection (i.e., 19 percent). Respondents earning $75,000 or more were overrepresented marginally preelection (i.e., 34 percent) compared with postelection (i.e., 32 percent). Finally, investigators interviewed more respondents during the preelection period (i.e., n = 3,148) than the postelection period (i.e., n = 3,005). We suspect that fewer interviews took place during the U.S. holiday season.
Table 2 presents estimates from negative binomial regression models with robust standard errors. A negative and statistically significant time period coefficient in row 1, column 1 would support hypothesis 1. Net of control variables, time period was not significant. White male veterans did not report significant change in poor mental health postelection compared with preelection, thus we did not find support for hypothesis 1. Age associated with better mental health. Respondents earning at least $75,000 in household income reported better mental health than those earning less than $25,000. Married respondents reported better mental health. Respondents who were retired, unable to work, and those holding other employment reported worse mental health than those with paid employment.
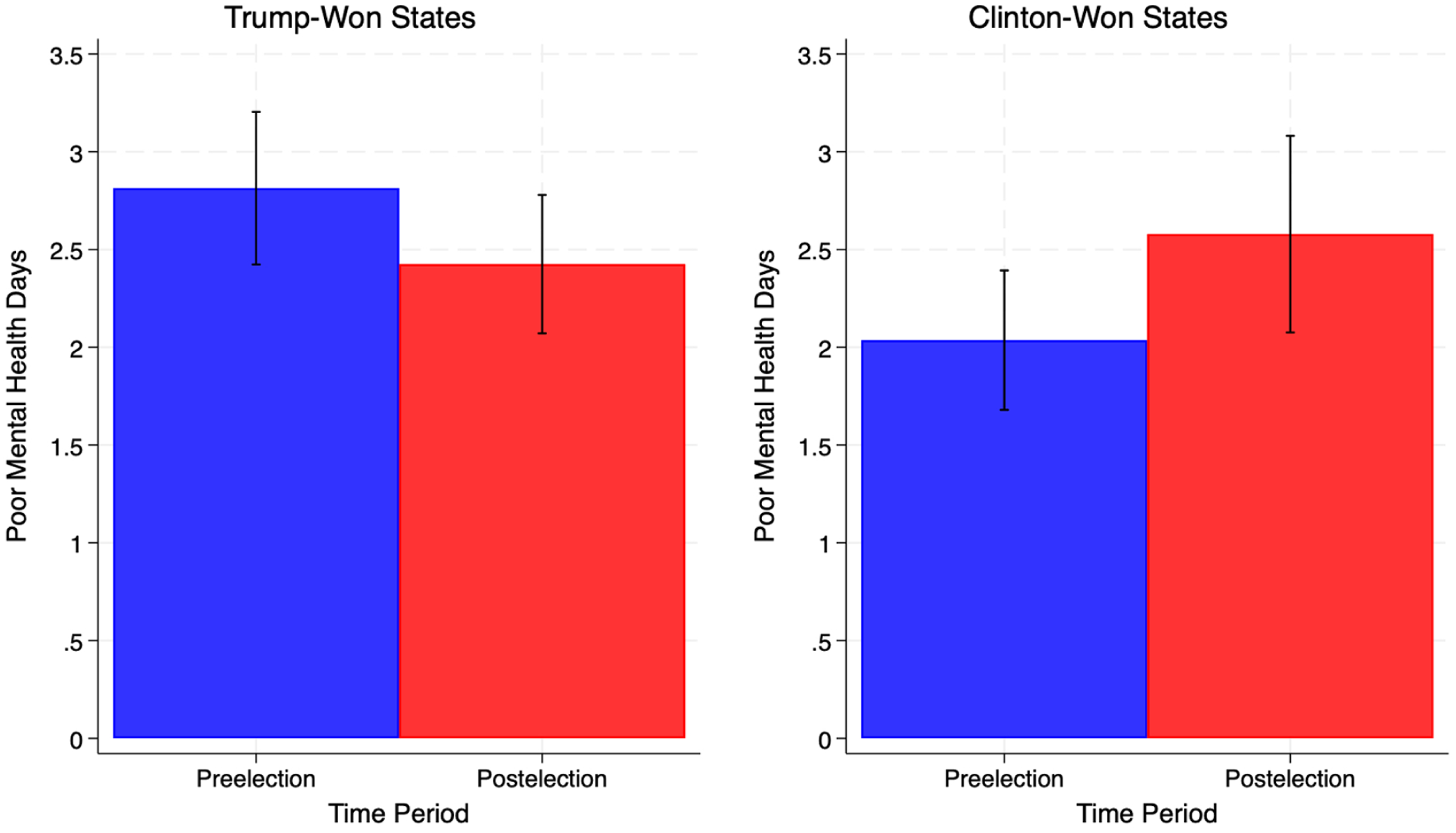
Model 2 included a statistical interaction between time period and state won by Trump. A negative and statistically significant interaction coefficient in row 3, column 2 would support hypothesis 2. In states where Trump won the popular vote, white male veterans’ expected log count of poor mental health days was .38 lower postelection, compared with preelection. That means these veterans reported 32 percent fewer poor mental health days (incidence risk ratio = .68, p < .01). Thus, we found support for hypothesis 2. Time period’s main effects mean that white male veterans in states Clinton won reported a marginal increase in poor mental health days. Figure 1 plots the predicted number of poor mental health days respondents reported preelection compared with postelection. In states Trump won (left panel), respondents reported a .38 decrease in poor mental health days, from 2.81 preelection to 2.43 postelection. In states Clinton won (right panel), respondents reported a .54 increase in poor mental health days, from 2.04 preelection to 2.58 postelection. These findings support symbolic empowerment theory. Once again, age associated with better mental health. Respondents earning at least $75,000 in household income reported better mental health than those earning less than $25,000. Married respondents reported better mental health. Respondents who were retired, unable to work, and those holding other employment reported worse mental health than those with paid employment.
Predicted poor mental health days among white male veterans living in Trump- and Clinton-won states before and after Donald Trump’s 2016 presidential election, Behavioral Risk Factor Surveillance System.
Model 3 included a statistical interaction between time period and the Trump-Clinton percentage differential. A negative and statistically significant interaction coefficient in row 5, column 3 would support hypothesis 3. Among white male veterans in the postelection period, living in states where Trump won handily (i.e., respondents lived among more Trump voters) associated with a significant decrease in poor mental health days (−.84, p < .05), relative to living in states where Clinton won handily. Thus, time period’s association with poor mental health days depended upon the Trump-Clinton percentage differential. Hence, we found support for hypothesis 3. Figure 2 plots the interaction. The red line indicates predicted probabilities of poor mental health days postelection. The blue line indicates predicted probabilities of poor mental health days preelection but was not statistically significant. Shaded areas represent 95 percent confidence intervals. At Clinton’s largest percentage advantage (x = −.86), respondents reported 4.80 poor mental health days postelection. As Trump’s percentage advantage increased, respondents reported fewer poor mental health days postelection. At Trump’s largest percentage advantage (x = .46), respondents reported 1.82 poor mental health days postelection, equaling nearly a three-day decrease (i.e., 4.80 − 1.82) across the Trump-Clinton percentage differential variable’s range. Yet again, age associated with better mental health. Respondents earning at least $75,000 in household income reported better mental health than those earning less than $25,000. Married respondents reported better mental health. Respondents who were retired, unable to work, and those holding other employment reported worse mental health than those with paid employment.

Predicted poor mental health days among white male veterans by time periods before and after Donald Trump’s 2016 presidential election and the Trump-Clinton percentage differential, Behavioral Risk Factor Surveillance System.
Robustness Checks
The Appendix presents robustness checks, showing estimates from nine separate negative binomial regression analyses predicting poor mental health days, net of control variables (see supplemental materials). All but one set of analyses replicate the models reported in Table 2. In the first three panels, we examined whether this study’s findings applied to other veterans. The “2016 White Female Veterans” and “2016 Black Male Veterans” panels show that those veteran groups reported no significant change in poor mental health days postelection. In the “Hispanic Male Veterans” panel, time period associated with a marginally significant decrease in poor mental health days postelection in model 1 (−.61, p < .10), despite a small sample size (n = 233). The “2016 White Male Veterans, Time Period × College Degree or More” panel (n = 6,153) investigated whether commissioned officers and college-educated enlisted veterans differed from veterans with less than a college degree. It contained a statistical interaction between time period and college degree or more. Once again, we found no statistical evidence supporting symbolic empowerment theory. The “2016 White Male Civilians” panel (n = 14,263) examined whether this study’s findings captured a unique phenomenon among veterans, rather than simply Trump supporters. White civilian men reported no significant change in poor mental health days postelection. In the “2024 White Male Veterans” panel, we examined whether findings from 2016 would replicate in 2024. We argue that the potential sociopolitical shift concomitant with the 2016 election drove the effects reported in Table 2, not just support for Trump or for respondents’ preferred presidential candidate. White male veterans reported no significant change after Trump’s presidential reelection in 2024. Finally, to investigate whether our findings were due to potential seasonal effects (e.g., salubrious or deleterious mental health effects of Veterans Day, Thanksgiving, and the U.S. holiday season), we replicated the analyses reported in Table 2 for identical time periods in 2015 and 2017. White male veterans reported no significant change in poor mental health days in these years. We found no statistical evidence of potential seasonal effects. Findings were specific to fall 2016.
Although we assume missing values should not bias results because of randomization across time periods (see the “Analytic Strategies” section), we investigated whether missing household income data (n = 957; see Table 1) biased results reported in Table 2. First, we examined the distribution of missing values across time periods. Household income’s missing values showed near even distribution, with preelection values equaling 480 and postelection values equaling 477. Next, a logistic regression model predicted missingness on household income, including all other variables in our models (analyses not shown). Key study variables (i.e., poor mental health days, time period, state won by Trump, and the Trump-Clinton percentage differential) did not predict missingness on household income. Among control variables, respondents with less than a college degree, those with fewer children in the household, retired respondents, and those with other employment tended to be missing on household income. These findings suggest household income’s missingness did not bias findings reported in Table 2.
Discussion
Using a quasi-experimental design with nationally representative survey data from the 2016 BRFSS, we investigated the mental health significance of Donald Trump’s 2016 presidential election for white male veterans. We invoke symbolic empowerment theory to frame our hypotheses (Brown et al. 2021). The 2016 presidential election provided a novel opportunity to examine associations between a presidential election and symbolic empowerment among whites. We hypothesized that white male veterans would experience improved mental health following Trump’s 2016 election (hypothesis 1) because it could signal a sociopolitical shift. This shift would align with veterans’ cultural values and affirm their service and dominant status in the U.S. racial hierarchy. We did not find evidence supporting hypothesis 1. To investigate whether symbolic empowerment depended on state-level sociopolitical contexts (e.g., political cultures, policy environments, and concentration among Trump voters), we hypothesized that white male veterans living in Trump-won states (hypothesis 2) and those living in states Trump won handily (hypothesis 3) would experience improved mental health postelection than preelection. We found support for hypotheses 2 and 3. White male veterans living in Trump-won states reported a .38 decrease in poor mental health days postelection. In Clinton-won states, respondents reported a marginally significant .54 increase in poor mental health days postelection. White male veterans in states where Trump’s popular vote advantage was high experienced improved mental health. Across the Trump-Clinton percentage differential variable’s range (i.e., −.86 to .46), respondents reported nearly a three-day decrease (i.e., 4.80 − 1.82) in poor mental health days postelection. Robustness checks corroborate our findings.
Null findings for all white male veterans were unexpected. One plausible explanation originates from the broader societal polarization characterizing reactions to Trump’s victory. Trump offended many Americans during his campaign. His comments about certain U.S. social groups and disparaging remarks toward military-connected individuals did not prevent his electoral victory but probably eroded some veteran support. Liberal and more traditional conservative white male veterans living in Clinton-won states were likely disempowered by Trump’s victory and viewed him as a threat to U.S. democracy. Findings validating hypotheses 2 and 3 corroborate this polarization explanation because the association between the 2016 presidential election and symbolic empowerment depended on state-level sociopolitical contexts, as demonstrated by previous studies (Morey et al. 2021; Yan et al. 2021).
Findings for white male veterans living in Trump-won states and states where Trump won handily suggest these particular veterans experienced a collective racial effervescence after the 2016 election. Gorman et al. (2023) found a similar effect among Black veterans after the 2008 election. However, the 2016 presidential election did not represent a historic first for a perpetually aggrieved group. It possibly symbolized a return of traditional power structures associated with white hegemonic masculinity. Its symbolic value was largely perception based because white men’s status at the apex of the U.S. racial hierarchy was safe during the Obama presidency and unthreatened by a potential Hillary Clinton presidency. White veterans are not monolithic regarding attitudes, ideology, and partisanship. However, at the aggregate level, white male veterans in Trump states may be among some of the more conservative members of U.S. society, more so than white civilian men. Factors such as far-right political cultures and environments, physical proximity to other Trump voters, pride, and a sense of belonging associated with living in a red state may have reinforced effervescent emotions and attitudes among these veterans. Many of them likely spend time discussing politics alongside similarly situated veterans at work or in social organizations. Trump’s rhetoric targeting outgroups perceived as threats to traditional white masculine American values possibly resonated with this group.
Like conservative white men in general, many white male veterans were among Trump’s staunchest supporters throughout his first term and during the Biden presidency. When the empowerment of Trump supporters extended beyond symbolism, some white male veterans took the lead. For example, in 2017, some conservative white male veterans participated in the Unite the Right “alt-right” event in Charlottesville, Virginia (Blout and Burkart 2021; LaMothe 2017). Years later, many participated in the January 6, 2021, insurrection at the U.S. Capitol to prevent a peaceful transfer of power to incoming president Joe Biden. Veterans represented 10 percent of individuals arrested (Hodges 2021). In both cases, some veterans who decided to participate served in leadership roles, and some committed violent acts. Evidence suggests notable connections between Donald Trump and segments of the white veteran population. His role as commander in chief seemingly extended beyond active service members to veterans. In the 2024 presidential election, Trump defeated Kamala Harris with a higher popular vote percentage than his 2016 victory. Once again, he enjoyed support from white military veterans (Copeland 2024). Such support reflects how symbolic empowerment reaffirms identity and culture, strengthening in-group boundaries in ways that shape well-being.
Robustness checks revealed findings reported in Table 2 did not extend to other veteran groups. Null findings for white female and Black male veterans suggest Trump’s campaign messaging did not resonate with those groups as it did with white male veterans. White women supported Trump overall, but veterans were not empowered by his election victory. However, Hispanic male veterans reported improved mental health postelection. In a prior study, Hispanic male veterans also reported improved mental health days after Barack Obama’s 2008 presidential election (Gorman et al. 2023). These combined findings suggest more intersectional research is needed on political and racial attitudes among Hispanic veterans.
This study’s findings hold important implications for understanding the role political polarization, representation, and identity play in health outcomes. The mental health divergence between veterans in Trump-won and Clinton-won states highlights how sociopolitical and geographic context can shape mental health. We suspect symbolic empowerment may reinforce in-group solidarity while intensifying out-group alienation. These findings underscore the role of political representation as a social determinant of health in specific contexts. Observed mental health effects among white male veterans suggest perceived affirmation or threat to group status, whether real or symbolic, can have tangible consequences for mental health. These insights call for a more nuanced understanding of how identity, place, and politics intersect to shape health outcomes.
Limitations and Future Directions
To our knowledge, this is the first study to examine the mental health significance of Donald Trump’s 2016 presidential election for white male veterans. Its limitations should inspire future research. First, BRFSS data do not include details regarding military service (e.g., branch of service, rank, time in service). Second, BRFSS does not ask whether respondents voted for Trump. We assume voting behavior and other omitted variables are distributed randomly across the time periods. Third, it would be ideal to investigate symbolic empowerment and mental health using panel data collected from the same veterans over time. To our knowledge, no such data exist; therefore, BRFSS data are the only option. Fourth, future studies should investigate political and racial attitudes among Hispanic male veterans. Findings from this study and Morey et al.’s (2021) study suggest their attitudes may deviate from Hispanic civilians. Finally, future studies should investigate associations between symbolic empowerment and other mental health indicators and psychological resources (e.g., self-esteem, personal mastery, and satisfaction with life). For example, when analyzed with panel data, these indicators may reveal durable effects of symbolic empowerment.
Supplemental Material
sj-docx-1-srd-10.1177_23780231261419871 – Supplemental material for Make America Great! How Political Geography Shaped White Male Veterans’ Mental Health after the 2016 Presidential Election
Supplemental material, sj-docx-1-srd-10.1177_23780231261419871 for Make America Great! How Political Geography Shaped White Male Veterans’ Mental Health after the 2016 Presidential Election by Quintin Gorman and Julian Culver in Socius
Footnotes
Supplemental Material
Supplemental material for this article is available online.
1
See supplemental materials for ![]() .
.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.