
Abstract
This visualization extends previous research reporting a positive effect of prenatal exposure of Democratic presidencies on the health outcomes of Black and White infants in the United States between 1971 and 2018. Using detailed information on race and ethnicity and new data for 2019 to 2024, the authors disaggregate birth outcome rates for Black, White, Hispanic, and Asian babies during a 36-year period between 1989 and 2024. They address three questions: (1) Do the earlier findings extend to this historical period? (2) Is there heterogeneity in effects across racial/ethnic minority groups? and (3) Do the findings for Whites and Blacks mask heterogenous effects by race and Hispanic ethnicity? The results indicate that presidential party effects persist in the recent period and extend to all four major racial and ethnic groups in the United States. All groups experienced better infant health outcomes under Democratic administrations, with the largest effects among non-Hispanic Black infants.
Health at birth is a key indicator of population well-being, providing a marker of life chances at the beginning of life. A large literature has examined the role of prenatal environmental exposures—including pollutants, violence, income transfers, and access to health care services, among many others—in shaping infant health outcomes. However, proximate environmental factors often flow from upstream causal factors, such as national-level political ideologies that guide policy priorities and resource distribution. Previous research shows that the political context is an important distal cause affecting infant health in the United States: between 1971 and 2018, infant health in the United States improved during Democratic administrations relative to Republican ones (Torche and Rauf 2021) Specifically, rates of preterm birth and small-for-gestational-age (SGA) birth, two central markers of poor health at birth (Behrman and Stith-Butler 2007; Conley, Strully, and Bennett 2003), declined under Democratic presidents. These improvements were evident for both Black and White infants, though effects were stronger for Black infants. In contrast, the party of the state governor was found to have no significant effect on infant health.
This visualization provides a theoretical replication and extension of Torche and Rauf (2021). Our key independent variables are the presidential and gubernatorial party in power in the calendar year prior to birth, approximating prenatal exposure. The president’s party can influence infant health in the United States through multiple institutional and ideological channels. Presidents exercise broad formal and informal powers that shape laws, budgets, and norms. They control the federal budget ex ante and the distributive arms of government ex post (Berry, Burden, and Howell 2010), issue unilateral executive orders (Howell 2003), and use veto and bargaining powers to extract concessions from Congress (Cameron 2000; Kiewiet and McCubbins 1988). These tools give presidents substantial capacity to direct the allocation of resources and to influence public policy, including health and welfare spending (Faricy 2015). Presidents also shape public opinion and national identity through appointments, judicial nominations, and rhetoric (Beasley 2006; Kennedy 2003; Kernell 2005).
Since the 1960s, party platforms have diverged sharply. Republicans have emphasized tax cuts, deregulation, and reduced social programs, whereas Democrats have advanced redistributive policies and social protection (Faricy 2011; McAdam and Kloos 2014; Prasad 2018). These partisan differences can translate into measurable effects on population well-being. Mechanisms linking presidential party to infant health include economic redistribution, health care expansion, and the reduction of racial and social exclusion, factors known to improve birth outcomes through enhanced access to resources, lower maternal stress, and healthier prenatal environments especially among minority populations (Dunkel Schetter 2011; Hoynes et al. 2015).
Governors hold significant executive authority within states and can influence infant health through policies such as the minimum wage, access to health insurance, income transfers, and abortion access. However, evidence on the impact of gubernatorial party control is mixed. Early research found little partisan effect on state policy or economic outcomes (Erikson, Wright, and McIver 1993; Hofferbert 1966), and more recent work suggests that party differences remain modest, often limited to specific contexts or policy domains (Alt and Lowry 1994; Caughey, Warshaw, and Xu 2017; Leigh 2008). Still, as federal authority has devolved and polarization has increased, the governor’s party may matter more for health and welfare policies (Grumbach 2018; Montez 2017). Democratic governors may allocate more resources to health and education (Beland and Oloomi 2017), though this is not universal (Joshi 2015).
Our analysis examines a partially overlapping sample including the period from 1989 to 2024. Our panel begins in the year that the National Vital Statistics System began consistently providing ethnicity information for birthing mothers. This extension addresses three issues: First, does the substantial impact of Democratic presidents and the nonsignificant impact of Democratic governors extend to the most recent time period, and do we see different patterns amid disruptions brought about by the coronavirus disease 2019 (COVID-19) pandemic? Second, prior findings for Whites and Blacks included Hispanics (approximately 30 percent of White mothers and 8 percent of Black mothers are Hispanic). Failure to consider Hispanics separately may mask distinct trends for non-Hispanic Black and White infants. Disaggregating effects for Hispanic births is also essential from a demographic perspective, as this group constitutes more than one quarter of total U.S. births and may exhibit different responses. Third, Asian infants were excluded from the prior analyses because of incomplete coverage across states; examining the period from 1989 to 2024 period allows us to provide the first assessment of the impact of political context on this group.
Our outcome variables are preterm birth and SGA birth. A preterm birth is defined as delivery before 37 weeks of gestation. An SGA birth is defined as birth weight below the 10th percentile by gestational age and sex, according to distributions for the entire period from 1989 to 2024 period. These outcomes are orthogonal by construction. Preterm birth and intrauterine growth restriction leading to SGA share some causes but have distinct main predictors. Preterm birth is driven largely by maternal stress, anxiety, infection, and inflammation (Dunkel Schetter 2011; Goldenberg et al. 2008), while SGA birth is linked to maternal smoking, low pre-pregnancy weight, and chronic conditions such as hypertension and diabetes (Goldenberg and Culhane 2007; Wollmann 1998). Consequently, preterm birth is expected to respond more to stress-induced pathways, whereas SGA birth reflects sustained maternal health and behavioral influences. Full details about variables, models, and regression results are provided in the online supplement.
Figures 1A and 1B present national trends in preterm and SGA birth, respectively. Figure 1A shows relative stability for Black infants and a slight increase in preterm birth for all other groups. This trend, also seen in other high-income countries, is partly attributable to increasing maternal age and use of assisted reproductive technology (Aradhya et al. 2023; Chang et al. 2013). Centrally to address our research questions, all racial groups display similar temporal fluctuation, with declines in preterm birth below the predicted trend during Democratic administrations in the 1990s and early 2010s and increases above prediction during Republican administrations in the 2000s and late 2010s. These departures provide initial evidence suggesting a beneficial effect of Democratic presidencies. Figure 1B shows a similar pattern for SGA births.
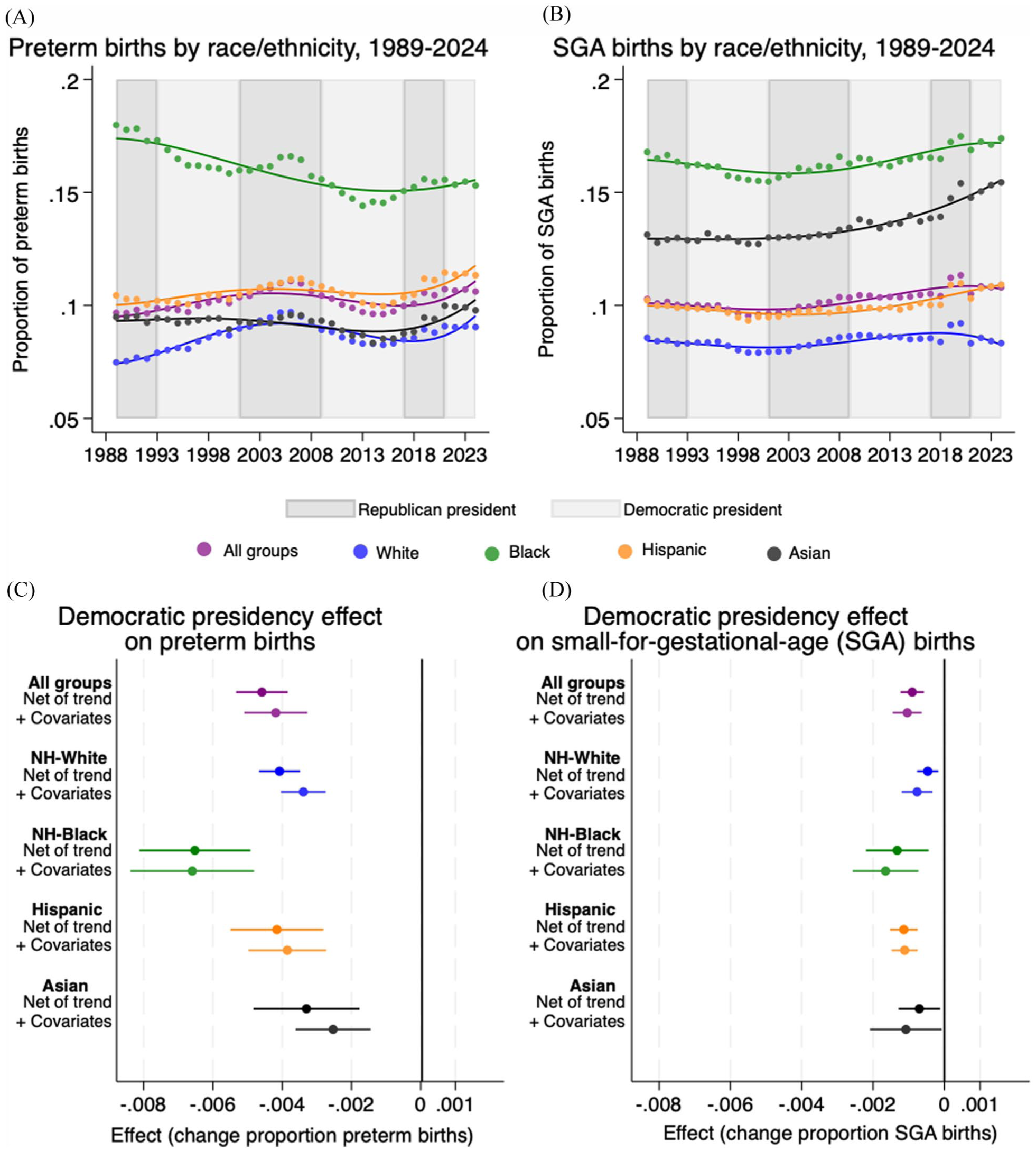
Trends in preterm and SGA births and effect estimates of the impact of Democratic presidencies on infant health in the United States, 1989 to 2023.
To assess whether these aggregate patterns reflect causal effects of the presidents’ party, we show estimates from state fixed-effects models in Figures 1C and 1D. The first set of models in each panel (“Net of trend”) show effect estimates and confidence intervals quantifying the association between Democratic administrations and the two infant health outcomes, net of a fourth-order time trend.
A limitation of the first set of models is that our study period includes several major historical events that affected Americans’ lives and could have influenced birth outcomes. These include the Great Recession, Hurricane Katrina, and, most recently, the COVID-19 pandemic. In our second set of models (“+Covariates”), we adjust for factors that control of such historical changes in context and could have confounded the effect of the presidential party. Specifically, we control for state-level macroeconomic conditions (real per capita income and employment rate) and states’ composition of mothers (rates of high school graduation, rates of marriage, mean maternal age, and proportion of foreign-born mothers).
The estimated effect of a Democratic president for all racial and ethnic groups is a 0.42 percentage point reduction in preterm births and a 0.11 percentage point reduction in SGA births. In contrast, the party of the governor has no significant effects for all births on for all the groups distinguished. We therefore do not show these effects in the visualization (full results are available in the online supplement). The effects of the president’s party are substantial at the population level. For example, in 2024, this translates to approximately 14,811 fewer preterm births (3,5,26,370 births × 0.0042). For preterm births, the effects are comparable for White and Hispanic infants (0.339 and 0.3685 percentage points, respectively), smaller for Asians (0.253 percentage points), and larger for Black infants (0.660 percentage points). Applying these estimates to the number of births in 2024 implies 2,991 fewer preterm births among non-Hispanic Black infants, 5,854 fewer among non-Hispanic White infants, 3,727 fewer among Hispanic infants, and 561 fewer among Asians under a Democratic president. 1 The effects on SGA births are similarly beneficial but smaller in magnitude. Again, they are largest for Black infants and similar for White and Hispanic infants.
Our findings show that between 1989 and 2024, infant health outcomes were better under Democratic than Republican presidencies. These effects are statistically significant, robust to covariate adjustment, and sizable at the population level. This pattern has persisted beyond 2018. All racial/ethnic groups benefit from Democratic administrations, with effects similar for White and Hispanic infants, smaller for Asian infants, and largest for Black infants. Because preterm birth rates remain much higher among Black infants than among other groups (Braveman et al. 2021), Democratic administrations have contributed not only to improved infant health overall but also to a narrowing racial disparities in early-life health.
Supplemental Material
sj-docx-1-srd-10.1177_23780231251400112 – Supplemental material for Effects of the President’s Party on Infant Health Across Racial & Ethnic Groups in the United States
Supplemental material, sj-docx-1-srd-10.1177_23780231251400112 for Effects of the President’s Party on Infant Health Across Racial & Ethnic Groups in the United States by Florencia Torche and Tamkinat Rauf in Socius
Footnotes
Data Availability
Restricted-access natality data were obtained from the National Center of Health Statistics (NCHS) of the Centers for Disease Control and Prevention (CDC). The authors are grateful to the NCHS and CDC for providing access to the data. Researchers interested in these restricted data should contact the NCHS directly.
Supplemental Material
Supplemental material for this article is available online.
1
The sum of these reductions for Blacks, Whites, and Hispanics is not the same as the decline in preterm birth among all infants, as 9.6 percent of infants of other racial/ethnic groups are not included in the race/ethnicity-specific analysis.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.