
Abstract
Despite initial declines in fertility since the onset of the pandemic, less is known about how fertility intentions are related to pandemic-based stressors in the United States. The authors examine the following two questions. First, how are pandemic stressors associated with short-term fertility intentions? Second, among those delaying fertility, what are the rationales for doing so, and how are pandemic stressors related to these rationales? The authors draw on the National Couples’ Health and Time Study, a nationally representative sample of 20- to 50-year-olds in the United States who were married or cohabiting and interviewed between September 2020 and April 2021. Among those desiring or remaining open to having (more) children, experiencing pandemic-related stressors was associated with delays in fertility plans; those whose lives were most disrupted and those who experienced relationship stress were less likely to intend to have children in the next year. The most common rationale for not intending to have children in the next year was economic worries, followed by health worries and concerns about an uncertain future. Economic and health stress were linked to these rationales, net of objective indicators. A comprehensive assessment of fertility intentions and underlying rationale for intentions on the basis of subjective factors is critical for understanding fertility patterns.
The initial fertility downturn during the Great Recession was consistent with demographic theories (Sobotka, Skirbekk, and Philipov 2011), but the ongoing decline in the years since the recession ended has stymied explanation (Kearney, Levine, and Pardue 2022), at least when considering the typical economic indicators from such theories. The coronavirus disease 2019 (COVID-19) pandemic introduced another shock that affected fertility rates, with a sizable dip in 2020 and 2021 before rates recovered slightly to resume the prepandemic trajectory (Cohen 2021; Osterman et al. 2024). This is consistent with other work documenting a link between public health crises and fertility. For instance, during the 1918–1919 influenza pandemic, fertility levels fell in the United States (Chandra et al. 2018). Similarly, in recent history, there have been several health crises linked to lower fertility levels, including the Ebola virus (associated with lower birth rates in Liberia), the severe acute respiratory syndrome epidemic (lower fertility in Hong Kong), and the Zika virus outbreak (lower fertility in Brazil) (Marteleto et al. 2020; Richmond and Roehner 2018; World Health Organization Ebola Response Team 2014). The impacts of public health crises on fertility extend well beyond the direct health effects (Boberg-Fazlic et al. 2021; Chandra et al. 2018), and the COVID-19 pandemic was no exception.
Not surprisingly, it appears that Americans’ fertility goals shifted substantially during the pandemic. In a cross-sectional Guttmacher survey conducted in late spring of 2020, 40 percent of women of reproductive age reported that they had either delayed having, or decided not to have, any (more) children as a result of the pandemic (Lindberg et al. 2020). Similarly, a longitudinal sample of adults in their 30s interviewed immediately prior to the pandemic and during late summer and fall of 2020 documented declines in the share who expected to have children (Manning et al. 2022).
As the pandemic-related shifts in fertility seem to have merged with the preexisting downward trends in fertility in the United States and elsewhere, researchers interested in understanding the mechanisms underlying contemporary fertility patterns have increasingly incorporated two dimensions: (1) a focus on individual fertility decision making and (2) an emphasis on subjective evaluations of well-being. The former stems from that the fact that a focus on actual births tells us little about how individuals process exogeneous shocks given the lags between events, conceptions, and births, and the latter acknowledges that factors less easily measured by sociodemographic characteristics—such as stress, worry, and uncertainty—also contribute to fertility decision making (Brauner-Otto and Geist 2018; Comolli 2017; Comolli et al. 2021). The pandemic exacerbated stressors across multiple domains, such as health, relationships, and economics, and there is evidence that fertility goals shifted substantially during the pandemic (Lindberg et al. 2020; Manning et al. 2022). Yet little is known about the specific rationales that drove these shifts in the United States.
Exploiting the pandemic as an event that intensified uncertainty, we contribute to the burgeoning literature on subjective evaluations of well-being as key determinants of fertility decision making and, furthermore, explore how individuals rationalized their decisions to avoid childbearing in the short term. To do so, we rely on a unique U.S. population-based sample of married and cohabiting couples ages 20 to 50 years (the National Couples’ Health and Time Study [NCHAT]) interviewed between September 2020 and April 2021 that collected data about pandemic-specific stressors and fertility goals. Focusing on a sample of adults who desire to have children or who remain open to doing so, we first assess how pandemic stressors in terms of general disruptions and stress specifically related to economic, health, and relationship factors influenced short-term fertility intentions (within the next year, after the next year, or being uncertain about the timing of intentions). Second, focusing on those who want children but reported not intending to have children in the next year, we examine potential rationales (general sense of unpredictable future, economic worries, health concerns, and relationship uncertainty) for doing so. Although our analyses focus on the pandemic period in particular, our results can speak more broadly to the contemporary context in which men and women are making fertility decisions by considering a multidimensional set of subjective and objective domains.
Background
In 2020, the total fertility rate (the average expected number of children born per woman given current age-specific fertility rates) reached 1.64, a record low (Osterman et al. 2024). Prior to the onset of the pandemic and ensuing economic crisis, there were already calls for new research on U.S. fertility patterns (Guzzo and Hayford 2020). Fertility began falling during the Great Recession (2007–2008) (Percheski and Kimbro 2017; Schneider 2017; Su 2019) but did not respond to subsequent improvements in the economy (Allred and Guzzo 2018; Hamilton, Martin, and Osterman 2021). These declines did not seem to be driven by dramatic shifts in overall lifetime fertility goals, but by shifts in fertility timing and the ability to realize goals (Guzzo and Hayford 2023). Thus, turning to short-term fertility plans may provide a useful lens to understand how fertility decision making occurs during periods of uncertainty.
The pandemic forced most people to navigate new terrain given both the novelty of COVID-19 itself and the widespread impacts of mitigation efforts. In addition to escalating hospitalizations and rising mortality levels, the spillover health effects included restricted access to health care services for non-COVID-19 needs, mental health challenges, and new health-based behaviors (i.e., social distancing, masking, telehealth, and frequent vaccination). Along with these health-based responses were economic impacts, including changes in employment and working conditions, potentially increased income volatility, shifts in where and how people worked, school closings and reopenings, and difficulty finding and managing childcare. Social ties were strained as families had to work through evolving circumstances and figure out how to best manage these pandemic-era issues. Taken together, the coronavirus pandemic brought in a new wave of uncertainty, reflecting a lack of clarity about future events (Beckert 2016). Not surprisingly, there were reports of rapid increases in stress (Taylor et al. 2020). Broadly speaking, stress can be conceptualized as an overload of demands that exceed individuals’ abilities to cope, or as interruptions to individuals’ daily lives or ways of thinking (Burke 1991). Most Americans of childbearing age have not faced such high levels of stress and uncertainty across multiple domains in their lifetimes. Thus, it seems likely that the pandemic-related changes to life may have generated shifts in how they plan for the future, including the timing of their fertility plans (and certainty around those plans).
There is extensive empirical evidence showing that fertility responded to changes in the economy on the basis of work during the Great Recession. Macro-level measures of a fragile economy (unemployment rates, consumer confidence, mortgage foreclosures) were associated with fertility declines (Comolli 2017; Goldstein et al. 2013; Morgan, Cumberworth, and Wimer 2011; Schneider 2015). Similarly, at the individual level, objective economic indicators (e.g., income, unemployment, job type) have been linked with fertility decision making, with more precarious employment and earnings tied to lower fertility (Alderotti et al. 2021; Hofmann, Kreyenfeld, and Uhlendorff 2017; Kreyenfeld 2015; Mills and Blossfeld 2013; Raymo and Shibata 2017; Testa and Basten 2014; Vignoli, Mencarini, and Alderotti 2020b). A meta-analysis of research in Europe indicates that at the micro-level, employment instability is associated with lower fertility levels, especially in more recent periods (Alderotti et al. 2021). These indicators seem to demonstrate that individuals’ experiences influence how confident they feel about the future and their inclination to take on a long-term and expensive commitment such as childbearing and rearing. A shortcoming of this body of work, however, is this evidence is indirect and reliant solely on objective economic measures. Yet there is evidence that fertility decision making is strongly influenced by noneconomic factors, especially those related to relationships (Rackin and Bachrach 2016 ).
Recent work has integrated the importance of the perception of economic prospects by including indicators specifically measuring subjective concerns about employment, framing this as economic uncertainty. Evidence in Germany, Italy, Norway, and the United States demonstrates that not only are objective indicators of economic prospects important, but that subjective viewpoints on economic conditions are also key factors in fertility behaviors and decision making (Brauner-Otto and Geist 2018; Gatta et al. 2022; Guetto, Bazzani, and Vignoli 2021; Hanappi et al. 2017; Kreyenfeld 2015; Lappegård et al. 2022). For example, Kreyenfeld (2015) found that in Germany, women’s worries about their economic circumstances were associated with lower fertility levels, most notably for women who had their first child after age 26. Experimental vignette-based research in Norway and Italy, offering respondents potential positive and negative economic futures, found that negative economic prospects were linked to reduced fertility intentions (Lappegård et al. 2022; Vignoli et al. 2022). Similarly, Brauner-Otto and Geist (2018) relied on young American adults in the Panel Survey of Income Dynamics and reported that elevated worries about job security were associated with more uncertain fertility intentions and expected delays in fertility. Furthermore, heightened insecurity due to work during the pandemic was associated with lower fertility intentions in Italy (Guetto et al. 2021). It appears subjective indicators of their future prospects may play a role in the formation of fertility intentions, independent of objective statuses and characteristics. These factors might be especially relevant for short-term fertility intentions, whereas fertility intentions that do not reference a particular time frame (i.e., intending to have children at any time in the future) likely capture generalized social norms. Social demographers have amply demonstrated that fertility delayed—deciding not to have a child now—is strongly related to fertility foregone (Berrington 2004; Quesnel-Vallée and Morgan 2003). Thus, studying individuals’ perceptions of economic stressors and uncertainty will likely provide valuable insights into how macro- and micro-level economic conditions influence the contemporary fertility behaviors that underlie longer term trends.
In addition, understanding how individuals feel about other domains of their lives is key, as fertility decision making encompasses a wide range of factors. Romantic partnerships, for instance, are strongly linked to fertility behaviors (Brauner-Otto and Geist 2018). Work following young women over a two-year period documented that women’s fertility plans are highly contingent on their relationship, finding that as relationships become more serious and committed, pregnancy desires increased (Barber et al. 2019). As such, we might expect that uncertainty in relationships, then, would depress fertility plans. Moreover, how individuals perceived their own health has been shown to be associated with fertility intentions and realized fertility. Indeed, among foreign-born individuals in Sweden, Alderotti and Trappolini (2021) found that reporting poor health was negatively linked to fertility intentions. And certainly, during a pandemic, health concerns may play a further role; for many, the immediate concerns over contracting COVID-19 (either themselves or among their loved ones) could make it seem risky to have a child in the short term. In Italy, insecurity about one’s health was associated with lower fertility intentions (Guetto et al. 2021). More generally, though, the early stages of the pandemic were filled with uncertainty about when life would return to normal. Parents, in particular, may have found disruptions to routines and sources of support—both informal, such as friends and family, and formal, such as childcare centers and schools—to be overwhelming (Calarco et al. 2020).
In sum, the pandemic introduced considerable flux into the lives of Americans. Almost certainly, many people experienced the pandemic—especially the first few months, when much less was known about the disease, and pathways back to normal seemed unclear—in a negative way, contributing to stress and uncertainty (e.g., Andrews et al. 2023; Killgore et al. 2021; Zhou, MacGeorge, and Myrick 2020). These changes, in turn, likely had an effect on short-term fertility intentions, yet traditional theories of fertility intentions, such as the theory of planned behavior (Ajzen 1985), are not equipped to integrate the levels of uncertainty and stress that have unfolded during the pandemic.
We draw on approaches better suited to an era of uncertainty. Recently, scholars have introduced the idea of “shadows of the future” as a way to demonstrate how future orientations may shape behavioral repertories, and this idea has been applied in research on how precarity influences life decision making across the life course (Bernardi, Huinink, and Settersten 2019; Huinink and Kohli 2014; Settersten 2020). Prior to the formulation of this idea, empirical work demonstrated that individual’s views of their future in adolescence were related to their adult well-being and economic circumstances, showing how agency and aspirations determine behavior (Hitlin and Johnson 2015). This is part of a related and long tradition in cultural sociology and social psychology that considers how future cognitions, future selves, and imagined futures guide behavior (Mische 2009) and makes arguments for attention to dimensions of these future projections, such as “contingency” or conditions of uncertainty. In their work on social class and young adulthood, for instance, Silva and Snellman (2018) explored how young adults create narratives of their future selves that influence their perceptions of the value of college.
Vignoli et al. (2020) formalized this life-course perspective in their approach, called “narratives of the future,” in work investigating fertility intentions and behavior during the pandemic. They argue that reliance on objective determinants provides an incomplete, and potentially inaccurate, lens on fertility and advocate for incorporating subjective evaluations about one’s life circumstances as a key determinant of fertility decision making. Fertility is an inherently future-oriented behavior (given that the parental role is irreversible), and so how individuals feel about their past, current, and future lives will almost certainly affect their plans around childbearing, especially in the short term. And, indeed, their empirical work finds that anticipated economic uncertainty (measured with survey responses and experimental modeling) is associated with fertility plans net of objective measures (Lappegård et al. 2022; Vignoli et al. 2020). Moreover, this perspective allows room for not only uncertainty in domains that influence fertility but in fertility plans themselves. We integrate these perspectives and apply this approach to the current U.S. setting with the inclusion of indicators capturing uncertainty not only in the economic realm, but also generalized views of pandemic disruptions, economic stress, perceived health threats, and uncertainty in the proximal relational realm.
Given that fertility rates fell during the pandemic, the arguments above focus on the likely dampening effect of the pandemic on fertility intentions. However, we acknowledge the possibility that some individuals’ experiences may be associated with fertility intentions in a positive manner. For instance, Friedman, Hechter, and Kanazawa’s (1994) uncertainty reduction theory posits that children may be a source of meaning in an era with ambiguous and disrupted futures. Given the particular uncertainty that existed during the early phases of the pandemic, short-term fertility might be especially important to consider. There is also both anecdotal and survey evidence that suggests a subset of individuals found pandemic-related shifts in work to ease work-family conflict given limited parental leave options in the United States and that the pandemic elevated the centrality of family life (Eales et al. 2021; Lindberg et al. 2021; Lossio-Ventura et al. 2021). For these individuals, positive fertility intentions were bolstered during the pandemic, but the larger pattern seems to be that more individuals downgraded than increased fertility plans (Lindberg et al. 2021).
The Present Study
Drawing on work on economic uncertainty and narratives of the future, we consider how the pandemic influenced short-term fertility intentions among a sample of individuals who either want to have a child or remain open to doing so. First, we hypothesize that subjective evaluations of pandemic-related stress in multiple domains is associated with fertility postponement (wanting to have a child but not intending to do so at the moment) as well as uncertainty (wanting a child but unsure of intentions), net of objective characteristics. More specifically, the subjective evaluations of pandemic-related stress include COVID-19 disruption, economic stress, health stress, and relationship stress. Second, among those who do not intend to have a child in the short term, we consider individuals’ rationales for postponement or uncertainty. Namely, we examine how those same pandemic-related stresses (i.e., COVID-19 life disruption, economic stress, health stress, and relationship stress) are related to citing economic worries, health concerns, uncertainty about one’s future because of the pandemic, or relationship uncertainty as an explanation to not intend to have children in the next year. Here, each rationale is treated as an outcome, testing these reasons independently of each other. Our hypothesis is that subjective appraisals will have stronger associations with rationales to avoid having a child in the short term compared with objective economic measures, such as income and economic hardship. In other words, individuals’ perceptions of their situations in different life domains will be linked to their explanations in delaying having children. For example, once economic stress is considered, income and hardship will have a weak connection with identifying economic worries as a rationale to not a have a child in the next year.
This study provides critical new information regarding how short-term childbearing intentions in the United States are shaped. Building on past work that has considered how objective factors, especially economic characteristics, influence fertility decision making, we incorporate both objective and subjective measures, finding that both objective and subjective dimensions of economic context are important. These subjective concepts are rarely measured in demographic surveys and are critical additions to understanding motives that underlie fertility behavior. Rising uncertainty about the future necessitates an analytical framework that explicitly acknowledges its forward-looking nature. Furthermore, we extend prior work on uncertainty, which has largely focused on employment instability, to include dimensions relevant during the pandemic including health worries, relationship stress, and anticipated future well-being. Although perceptions of future economic prospects are important, they provide a rather narrow lens on the concerns people have about their lives in the future and how these concerns influence fertility decision making.
Data and Methods
This study draws on a recently collected population-based data source, NCHAT. The interviews were conducted between September 1, 2020, and April 30, 2021. The study is based on couples who were married or cohabiting and between 20 and 60 years of age, with oversamples of racial and ethnic individuals as well as sexual and gender minorities. Respondents were members of the Gallup Panel or Gallup population-representative samples. The surveys were web based and conducted in English and Spanish and lasted, on average, 40 minutes. Public access to the NCHAT dataset is provided through the Inter-University Consortium for Political and Social Research website at https://www.icpsr.umich.edu/web/DSDR/studies/38417. The bivariate and multivariate results are weighted based on Gallup-produced poststratification methods. To focus on those of childbearing age, we limited our analysis to the 2,361 respondents who were between the ages of 20 and 50 years with valid weights and intentions data. The analytic sample for this study excluded respondents who were pregnant, adopting or involved in surrogacy at the time of interview (n = 80), respondents who did not want any (more) children (i.e., those who have reached their desired parity; n = 1,461), and respondents missing on a covariate (n = 2). 1 The final analytic sample consists of 819 respondents. Analysis of rationales for avoiding births are limited to those who did not intend to have children within the next year or were not sure if they intended in the next year (n = 711). We discuss the specific measures of fertility desires and intentions in the next section.
Measures
Dependent Variables
Our focus is the timing of fertility intentions among those who still want to have a child. Supplemental analysis of the total sample indicates that only 1.3 percent of respondents retrospectively reported the pandemic changed their desire for children. This suggests that among couples the pandemic did not change individuals’ fertility desires but, rather, seemed to largely affect the time horizon for having desired children. Thus, to answer our first research question, we created a dependent variable using the question, “Do you intend to have a child in the next year?” with response categories of “yes”, “no,” and “not sure.” By restricting the analyses to those who have not reached their desired parity and using the timing of fertility intentions measure, we have three mutually exclusive categories: does not intend to do so in the next year (n = 534), unsure of fertility timing (n = 183), and intends to have a child within the next year (n = 102).
For the second research question related to why people who want or remain open to having children have decided to postpone childbearing, there are actually several dependent variables, all tapping into different rationales for avoiding childbearing. Respondents who did not report intending to have children in the next year (n = 711) were asked a series of questions about the importance of specific reasons for avoiding having a child in the next year. 2 The questions included “economic worries,” “health concerns,” “pandemic makes my future unpredictable,” and “unsure about relationship,” with responses including “not at all important” (1), “not too important” (2), “somewhat important” (3), “pretty important” (4), and “very important” (5). Thus, there is a score of 1 to 5 for each of these domains, and each is used as a dependent variable.
Independent Variables
The independent variables include subjective stressors related to the pandemic, objective economic indicators, and sociodemographic measures. We have several subjective measures. These include a general indicator about how COVID-19 respondents’ lives, on the basis of the measure “To what extent has your life been affected or disrupted by the coronavirus situation?” with responses ranging on a four-point scale from “not at all” to “a great deal.” Three subjective indicators of stressors also specific to the pandemic were included: health, economic, and relational. Health stress references the average score of how stressed the respondent was about “getting coronavirus,” “my spouse or partner getting coronavirus,” or “my parents, siblings or other family members getting coronavirus.” The responses were based on a five-point scale ranging from “not at all stressed” to “very stressed.” Cronbach’s α was .88. 3 Economic stress measures the average of responses to stress about “money and finances,” “my job,” and “getting food and supplies” during the pandemic. Cronbach’s α was .71. Relationship stress is based on three questions about strength of the couples’ relationship after the pandemic, questioning their relationship since the pandemic, and the probability of breaking up after the pandemic with response items ranging from 1 (“strongly disagree”) to 5 (“strongly agree”) and were reverse coded to generate the scale. Cronbach’s α was .72.
We include three objective economic indicators. Couple’s education was divided into three categories: neither has a college degree, one member has a college degree, and both have a college degree. Household income was top coded at the 95 percent level and was logged because of the skewed nature of the variable. Economic hardship was a dichotomous variable indicating whether in the past month the respondent indicated at least one of six items such as “we were unable to pay our gas, electric, other utility bill or rent/mortgage,” “we were unable to make minimum payment on credit cards,” and “we received an eviction or foreclosure notice.”
Finally, the data include a rich set of sociodemographic indicators. Parity was based both on the respondents’ household roster and a separate item about the number of children who did not live with the respondent, combined measure the total number of biological children (zero, one, two, or three or more). Age was included as age and age squared due to the nonlinear relationship between age and childbearing. Respondents reported their gender identity from five options, including woman, man, trans woman, trans man, and some other gender identity. For these analyses, women and trans women, and men and trans men, were grouped together. Gender was coded into a three-category variable indicating woman, man, or “other.” Respondents reported their race/ethnicity, and we coded as non-Latinx White, non-Latinx Black, non-Latinx Asian, non-Latinx other race, non-Latinx multirace, or Latinx. A dichotomous indicator for foreign born was constructed if the main respondent was born outside of the United States. Respondents answered the following question about their sexual identity: “What do you consider yourself to be? Select all that apply,” with 11 responses comprising heterosexual or straight, gay or lesbian, bisexual, same-gender-loving, queer, pansexual, omnisexual, asexual, don’t know, questioning, and “something else,” with an option to specify. We coded respondents into four mutually exclusive categories heterosexual exclusively; gay or lesbian exclusively; bisexual exclusively or with pansexual, omnisexual, and queer; and other or multiple sexual identities. Union status was based on whether the respondent reported they were legally married. Self-rated health was a dichotomous indicator where “excellent” “very good,” and “good” were merged as “good health” and “fair” and “poor” were combined as “poor health.” Month of survey spanned from September 2020 through April 2021 and was included as a series of dummy variables.
Analytic Plan
Multinomial logistic regression models were estimated for short-term fertility intentions given the categorical nature of the dependent variable (intends to have a child in the next year, unsure about fertility timing, or does not intend in the next year); recall that these are restricted to individuals who have not yet reached their desired parity. We estimated five sets of models that include sociodemographic measures and (1) COVID-19 life disruption, (2) economic stress, (3) health worries, and (4) relationship stress. The final model includes all the subjective measures and the sociodemographic indicators. The second set of analyses focused on the subset of respondents who do not immediately intend to have a child (unsure or not in the next year; again, these are individuals who desire or remain open to having children) by assessing the role of four rationales (i.e., economic worries, health concerns, future as unpredictable, and relationship uncertainty) separately. We used ordinal logistic regressions because of the ordinal nature of our outcomes, each ranging from 1 (“not at all important”) to 5 (“very important”). We tested for the parallel lines assumption using the Brant command and were supported for the future and health rationales. On the basis of Wald tests in the generalized ordered logistic regression model the parallel lines assumption was not violated for the economic rationale model, but was for the relationship rationale model. However, the key significant subjective factor, relationship stress, did not violate the assumption and results were similar when we used an ordinary least squares or ordered logit model for the relationship rationale. These multivariable models used each of the rationales for not having a child as the dependent variable. In other words, each rationale is tested independently of each other as separated outcomes. We show two models for each rationale: (1) a model focusing on objective economic factors (as these are most often hypothesized to be the key influence) and (2) a model including the pandemic-related stressors as well as the objective economic factors. Both of these models include the full set of sociodemographic controls. All analyses are weighted.
Results
The distribution of the dependent and independent variables are presented in Table 1. Among the analytical sample of partnered adults aged 20 to 50 years who have not yet reached their desired parity, about one in seven couples intended to have a child in the next year (15.26 percent). An important category often omitted from prior work is those who were unsure, with about one quarter (26.15 percent) of respondents reporting that they were unsure about their plans. About three of five (58.60 percent) respondents did not intend to have children in the next year. More than one quarter (28 percent) of respondents indicated that COVID-19 disrupted their life a great deal, and the mean was 3.01 on the 4-point scale. The mean level of economic stress was 2.61, representing a score below the midpoint for this 5-point scale (i.e., 3 = “somewhat important”). The average health stress was 2.80, approaching the midpoint, and the mean level of relationship stress was lower at 1.7. The distributions of the remaining sociodemographic indicators are listed in Table 1.
Distribution of Dependent and Independent Indicators among Respondents Who Desire Children.

Source: National Couples’ Health and Time Use Study.
Note: n = 819; weighted analysis. COVID-19 = coronavirus disease 2019; HH = household.
Timing of Fertility Intentions During the Pandemic
The multivariable multinomial logistic regression results are presented in Table 2, showing the relative risk ratios of intending a birth in the next year versus intending a birth later as well as intentions in the next year versus not sure about timing; recall that this is among those who want or remain open to having children. In model 1, respondents who reported higher levels of COVID-19 life disruptions had lower risks of intending to have children in the next year versus later or being unsure (p < .001). Model 2 replaces COVID-19 disruption with economic stress. Although higher levels of economic stress were not associated with fertility plans when the reference category was later timing, it was associated with a 37 percent lower risk for intending to have children when the reference group was respondents unsure about their plans (p < .05). That is, greater economic stress, net of objective economic characteristics, was linked to greater uncertainty about the timing of having a child. Model 3 replaces economic stress with relationship stress, which was associated with a 54 percent lower risk for fertility plans in the short term versus the longer term (p < .05). Compared with those who were unsure about their plans, individuals who intend to have a child were not significantly different in terms of relationship stress. Model 4 substituted health stress, and this indicator was not associated with of intending to have children in the next year versus both contrast categories.
Multinomial Regression Models Estimating Relative Risk Ratios of Fertility Intentions in the Next Year among Respondents Who Desire Children.

Source: National Couples’ Health and Time Use Study (n = 819).
Note: Reference group in parentheses. Month of survey included. Analyses are weighted. “Intend” means intending in the next year, “later” means intending after the next year, “don’t know” means intending but not sure about timing. COVID-19 = coronavirus disease 2019; HH = household.
p < .10. *p < .05. **p < .01. ***p < .001.
The final model (i.e., model 5) includes all the subjective indicators. COVID-19 life disruptions were associated with a 52 percent and 60 percent lower risks, respectively, of intending to have children in the next year when contrasted to those who intended to delay as well as those who were unsure about their plans (p < .01). The magnitude of the association between COVID-19 life disruption and fertility intentions was only slightly attenuated by including stressors. Respondents with greater relationship stress reported a 48 percent lower risk of intending to have children in the next year compared with those who intended to delay fertility (p < .10). Respondents with higher household incomes had a marginally lower risk of intending to have children in the short term rather than intending to have children later (p < .10). Thus, the subjective indicators, particularly those linked to relationships and to general life disruptions, appear to be independently associated with fertility plans net of objective characteristics.
Across models, economic hardship were not strongly associated with fertility intentions across models. Respondents with higher household incomes reported lower risks of intending to have children in the next year rather than delaying, but there were no significant household income associations for individuals intending to have children in the next year compared with those who were unsure about their fertility intentions. Couples who were highly educated reported overall marginally higher risks of expecting a child in the next year versus being unsure about intentions. Older respondents were more likely to expect a child in the next year. Respondents with greater numbers of children were less likely to expect a child in the next year versus intending to have children later. Respondents with Asian and Latinx racial and ethnic identities were more likely to expect a child in the next year. Individuals with a lesbian or gay identity had lower risks of intending to have children in the next year in most models, and those with a bisexual identity had lower risks of expecting a child in the next year than those with a heterosexual identity. Compared with cohabiting respondents, married respondents had higher risks of expecting a child in the next year versus waiting until later. Self-rated health was not associated with short-term fertility intentions.
Reasons to Avoid Having Children during the Pandemic
Respondents who wanted children or remained open to having children but were not intending to have children within the next year were asked why they wanted to avoid having children in the short term. The means and confidence intervals are reported in Table 3 and ranged from 1 (“not at all important”( to 5 (“very important”). The top-ranking rationale was economic reasons (3.20), followed by health concerns (2.62) and an unpredictable future (2.56). Concerns about the future of their relationship was the response ranked as least important by respondents. The share who endorsed “pretty important” or “very important” responses was about half (45.1 percent) for economic worries, approaching 1 in 3 (31.0 percent) for health reasons, about 1 in 4 (27.0 percent) for unpredictable future, and roughly 1 in 10 (11.1 percent) for relationship worries (results not shown). Although these indicators appear to be somewhat related to one another, they do not scale well together as indicated by a Cronbach’s α of .67. This low α suggests that these rationales to avoid having a child are rather distinct and independent constructs, meaning that reasons to delay childrearing are different across individuals.
Rationales for Avoiding Having Children in the Next Year among Respondents Who Desire Children.

Source: National Couples’ Health and Time Use Study (n = 711)
Note: Weighted analyses.
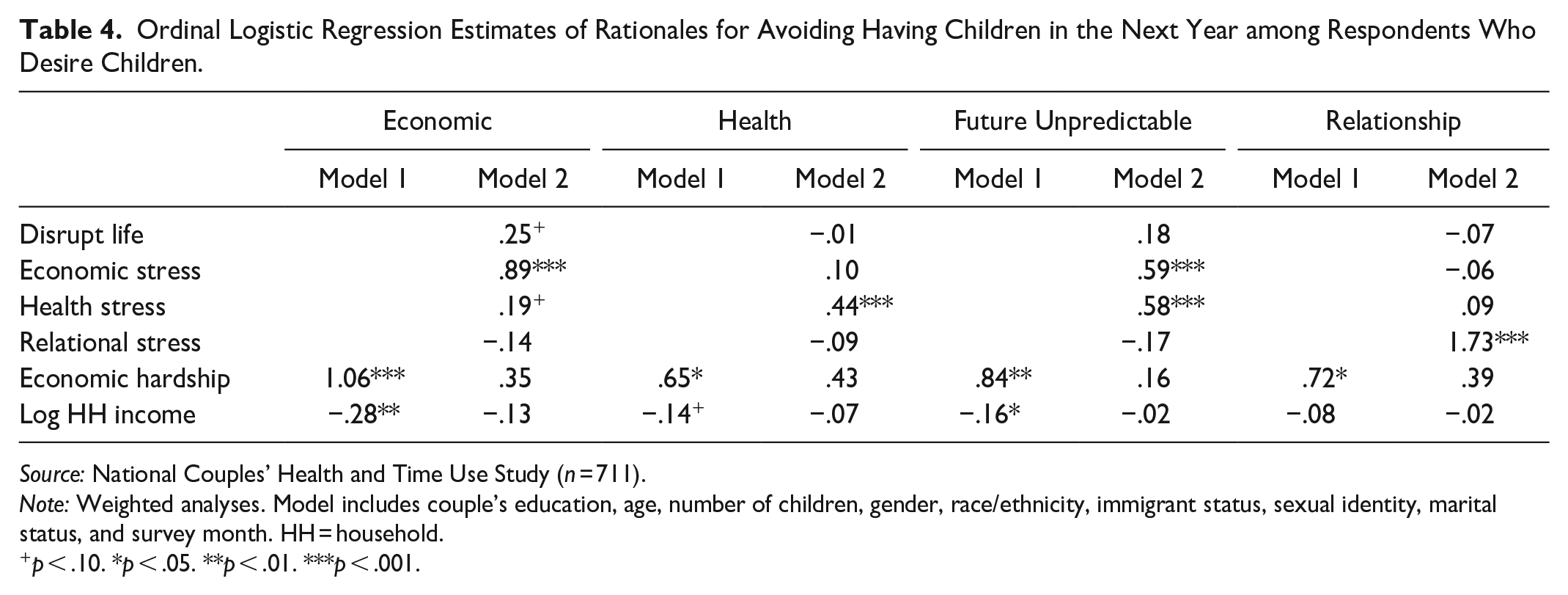
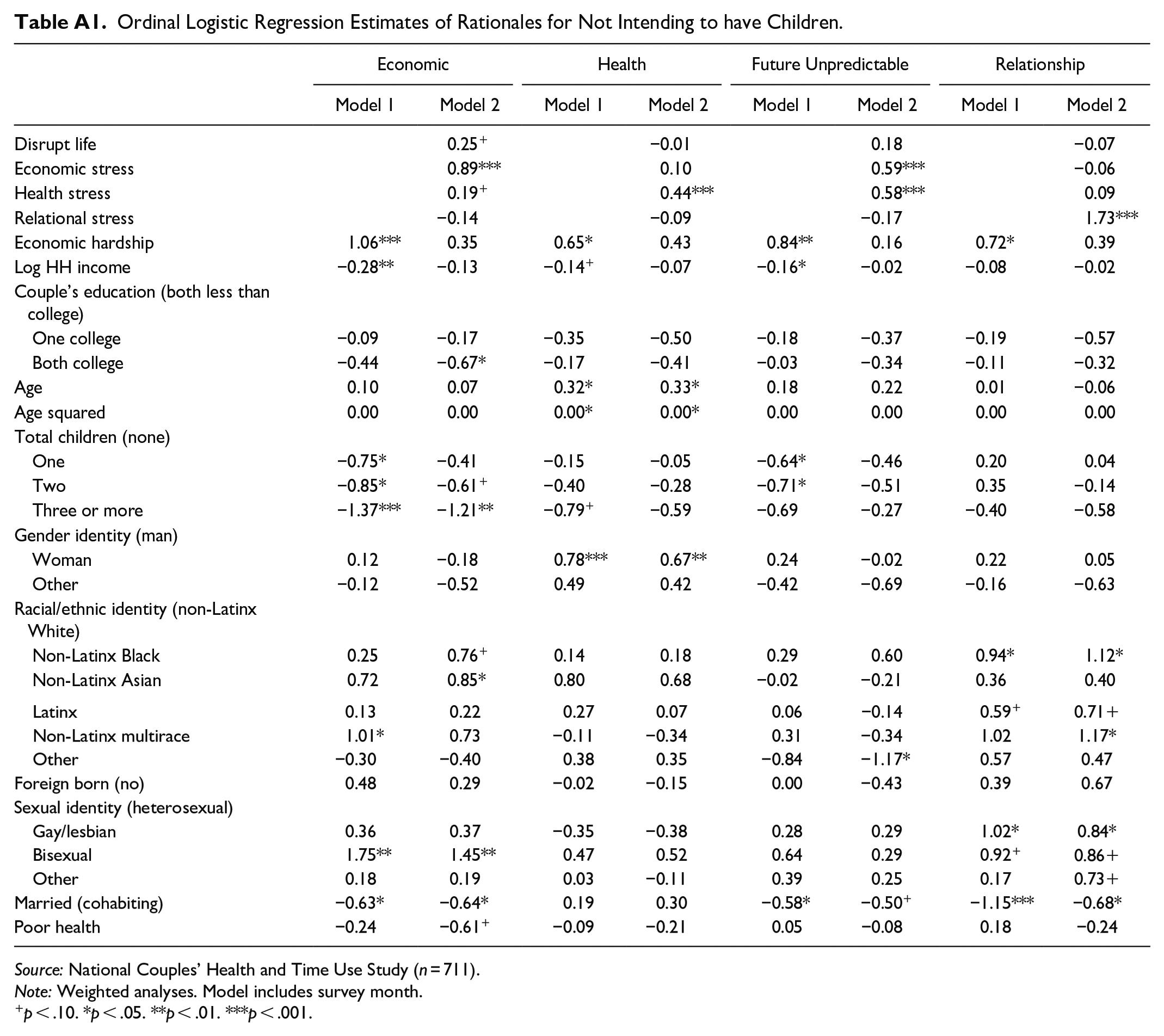
Table 4 presents the correlates of stress and sociodemographic indicators predicting each rationale for avoiding having children in the next year among those who want children (the complete models with all covariates are presented in Table A1 in the Appendix). For each rationale, we first present a model that controls for all sociodemographic variables but highlights the role of objective economic characteristics in predicting the rationale, and the second model adds the pandemic-related stressors as predictors. In the interest of brevity, we do not show the coefficients for the sociodemographic variables (see Table A1). The first set of models tackled the economic issues rationale. Economic hardship was positively associated and household income was negatively associated with endorsing economic issues as a reason for delaying childbearing. The second model adds in the pandemic-based subjective indicators. For a 1-unit increase in economic stress, there was a 0.89-unit increase in the ordered log odds of considering the economic rationale for avoiding having children in the next year as “very important” (p < .001). The objective indicators of economic circumstances were no longer associated with the economic rationale for delaying fertility. Moving next to health issues as a rationale for delaying childbearing, reporting poor health had no association with naming health concerns as a rationale to avoid having a child in the next year, but objective economic indicators were. However, this no longer holds true when the pandemic-based subjective indicator of health stress was included in the second model. Next, for the unpredictable future rationale, objective economic factors were associated with endorsing this rationale, but it was no longer statistically significant with the inclusion of the pandemic-based subjective measures. Stress about economic issues and health worries were both positively associated with endorsement of the unpredictable future rationale (p < .001). Finally, respondents who experienced economic hardship more often (log odds = 0.72, p < .05) endorsed relationship factors as reason to avoid having children, but objective economic indicators were no longer predictive of this rationale when considering subjective relationship stress in the second model. In particular, a 1-unit increase in relationship stress was associated with a 1.73-unit increase in the ordered log odds of reporting relationship factors as a rationale for avoiding having children in the next year as “very important” (p < .001). Taken together, once the subjective indicators were considered, objective economic measures were no longer directly related to specific rationales for delaying fertility.
Ordinal Logistic Regression Estimates of Rationales for Avoiding Having Children in the Next Year among Respondents Who Desire Children.
Source: National Couples’ Health and Time Use Study (n = 711).
Note: Weighted analyses. Model includes couple’s education, age, number of children, gender, race/ethnicity, immigrant status, sexual identity, marital status, and survey month. HH = household.
p < .10. *p < .05. **p < .01. ***p < .001.
Discussion
Declining fertility rates over the past decade, which were exacerbated in the short term during the pandemic, have been the subject of considerable scholarly and mainstream discourse. Some research suggests that overall fertility ideals and goals remain fairly stable (Brenan 2023; Guzzo and Hayford 2023), which then begs the question as to why fertility rates continue to decline. To answer this question, then, requires a focus on short-term fertility decision making, as many individuals in their childbearing years may have altered their childbearing plans but not abandoned them. In this article, we consider this group specifically by focusing on a U.S. sample of partnered men and women in their childbearing years who remain want or remain open to having children and explicitly examine their plans to have a child in the next year. Among this group, those who experienced greater levels of pandemic-associated stress were less likely to intend to have a child in the next year, providing support for arguments about the importance of subjective perceptions in decision making during an era of uncertainty (and as independent of standard socioeconomic characteristics). In fact, at least during the pandemic, objective economic indicators were not strongly related to the timing of fertility plans in the short term, perhaps because the pandemic hit all segments of society, and traditional economic protections, such as high education or high income, were not safeguards against the disruption of the pandemic. Thus, to the extent that pandemic stress and disruption capture aspects of uncertainty about the future, we find that these subjective evaluations of one’s current and anticipated well-being are related to delaying fertility or being uncertain about the timing of a(nother) birth. This finding is consistent with recent approaches focusing on “shadow of the future” from a life-course and social psychology perspective (Bernardi et al. 2019; Guetto et al. 2021; Mische 2009; Vignoli et al. 2020a) arguing that an unpredictable future is an important reason individuals decide to postpone or limit fertility.
Although work drawing from the “shadow of the future” approach, most of which focuses on European contexts, has demonstrated the importance of subjective perceptions of current and future well-being, this body of work has not been able to assess which reasons individuals themselves seem to consider especially important for delaying having a child among those who have not yet reached their desired parity. An asset of the NCHAT are the questions about reasons for limiting fertility during the pandemic. Among those who did not intend to have children within the next year, the results investigating rationales for having no short-term fertility plans indicated that the overarching measure of concerns about an unpredictable future was not endorsed as highly as economic worries. This seems to suggest that economic concerns weigh heavily on adults even when they are not worried about specific financial issues and are not experiencing specific economic hardships or disadvantages. Given declining economic mobility and the high demands that stem from the intensive parenting norms of contemporary parenthood (Chetty et al. 2017; Ishizuka 2019), parents (or would-be parents) seem to be concerned about whether their children will fare well in the future or whether they could adequately provide for their children the type of upbringing necessary to maintain their relative economic position. Our work aligns with prior studies in that financial concerns rank at the top of the list and health worries also ranked high (Lindberg et al. 2021). Certainly, these issues that have arisen because of the pandemic appear to be salient. About two out of five respondents endorsed economic factors as a reason for limiting fertility, and worries about health threats and an unpredictable future was endorsed by 30 percent of respondents. More generally, the pandemic-related stressors of economic, health, and relational concerns during the pandemic are all associated with the rationales for limiting fertility. The economic and health stressors of the pandemic were positively associated with endorsing the future uncertainty of the pandemic as a reason for limiting fertility. Our analyses indicated that each specific stressor was associated with the parallel rationale for limiting fertility. Higher scores on the subjective appraisals of stressors, rather than the traditional approach of simply being exposed to stressors, are related to identifying these indicators as reasons for limiting fertility.
Limitations
Although these data provide rich measurement and new opportunities to assess fertility intentions, there are a few shortcomings. First, the sample is limited to couples (married and cohabiting) and ignores the perspectives of single adults in their childbearing years, so this work cannot speak to experiences of single men and women who may also have modified their fertility plans in different ways during the pandemic. There is, of course, also selection of more advantaged individuals into coresidential partnership that cannot be accounted for in these analyses.
Second, the data are cross-sectional, preventing rigorous causal analyses of factors predicting fertility intentions nor how fertility intentions may or may not be realized. Longitudinal data from before and after the pandemic would allow us to capture changes in fertility intentions and actual fertility.
Third, these analyses are based on short-term fertility plans during the pandemic and may not apply to periods prior to the pandemic. Our analysis examines the timing of intentions among those who still want to have or remain open to having children and may represent a lower bounds estimate because those whose fertility desires changed during the pandemic are excluded from analysis. However, we expect that this bias is likely minimal as a very small share of partnered respondents reported the pandemic changed their desires for children.
Finally, the data do not include contraceptive use histories or sexual frequency indicators that are often used in analysis of fertility intentions among different-gender couples.
Conclusion
Understanding contemporary fertility patterns in the United States requires data on how individuals make childbearing decisions, yet few sources of data in the United States contain nuanced measures that incorporate the myriad factors individuals may consider or measure the complexity of individuals’ fertility goals (i.e., including fertility timing or uncertainty about goals). NCHAT provides new opportunities to consider how individuals experienced the pandemic as well as aspects of fertility intentions that are not available with other nationally representative data collections. We are not the first to focus on subjective factors, as prepandemic research has highlighted the importance of subjective factors (Brauner-Otto and Geist 2018; Comolli 2017; Hanappi et al. 2017; Kreyenfeld 2015). This work complements other researchers’ focus on pandemic fertility intentions in Europe, whose work has demonstrated how the inclusion of subjective indicators that capture uncertainty of economic circumstances is key for understanding fertility behaviors (Gatta et al. 2022; Guetto et al. 2021; Lappegård et al. 2022; Vignoli et al. 2022). More generally, it is increasingly clear that economic concerns are often a reason for avoiding having children—and that this is true even when considering standard objective measures of socioeconomic status, such as income and education. Yet we also demonstrate that noneconomic domains are also relevant. Individuals who report greater pandemic-related stressors in the economic and health realms more often endorse the pandemic as a reason for delaying fertility, and stressors in adults’ romantic relationship were important reasons for delaying fertility. As such, stress appraisals across multiple domains are critical for understanding fertility and consistent with research in other countries (Guetto et al. 2021). New research focusing on declines in fertility should incorporate theoretical and measurement advances that include subjective appraisals.
Footnotes
Appendix
Ordinal Logistic Regression Estimates of Rationales for Not Intending to have Children.
| Economic | Health | Future Unpredictable | Relationship | |||||
|---|---|---|---|---|---|---|---|---|
| Model 1 | Model 2 | Model 1 | Model 2 | Model 1 | Model 2 | Model 1 | Model 2 | |
| Disrupt life | 0.25 + | −0.01 | 0.18 | −0.07 | ||||
| Economic stress | 0.89*** | 0.10 | 0.59*** | −0.06 | ||||
| Health stress | 0.19 + | 0.44*** | 0.58*** | 0.09 | ||||
| Relational stress | −0.14 | −0.09 | −0.17 | 1.73*** | ||||
| Economic hardship | 1.06*** | 0.35 | 0.65* | 0.43 | 0.84** | 0.16 | 0.72* | 0.39 |
| Log HH income | −0.28** | −0.13 | −0.14 + | −0.07 | −0.16* | −0.02 | −0.08 | −0.02 |
| Couple’s education (both less than college) | ||||||||
| One college | −0.09 | −0.17 | −0.35 | −0.50 | −0.18 | −0.37 | −0.19 | −0.57 |
| Both college | −0.44 | −0.67* | −0.17 | −0.41 | −0.03 | −0.34 | −0.11 | −0.32 |
| Age | 0.10 | 0.07 | 0.32* | 0.33* | 0.18 | 0.22 | 0.01 | −0.06 |
| Age squared | 0.00 | 0.00 | 0.00* | 0.00* | 0.00 | 0.00 | 0.00 | 0.00 |
| Total children (none) | ||||||||
| One | −0.75* | −0.41 | −0.15 | −0.05 | −0.64* | −0.46 | 0.20 | 0.04 |
| Two | −0.85* | −0.61 + | −0.40 | −0.28 | −0.71* | −0.51 | 0.35 | −0.14 |
| Three or more | −1.37*** | −1.21** | −0.79 + | −0.59 | −0.69 | −0.27 | −0.40 | −0.58 |
| Gender identity (man) | ||||||||
| Woman | 0.12 | −0.18 | 0.78*** | 0.67** | 0.24 | −0.02 | 0.22 | 0.05 |
| Other | −0.12 | −0.52 | 0.49 | 0.42 | −0.42 | −0.69 | −0.16 | −0.63 |
| Racial/ethnic identity (non-Latinx White) | ||||||||
| Non-Latinx Black | 0.25 | 0.76 + | 0.14 | 0.18 | 0.29 | 0.60 | 0.94* | 1.12* |
| Non-Latinx Asian | 0.72 | 0.85* | 0.80 | 0.68 | −0.02 | −0.21 | 0.36 | 0.40 |
| Latinx | 0.13 | 0.22 | 0.27 | 0.07 | 0.06 | −0.14 | 0.59 + | 0.71 + |
| Non-Latinx multirace | 1.01* | 0.73 | −0.11 | −0.34 | 0.31 | −0.34 | 1.02 | 1.17* |
| Other | −0.30 | −0.40 | 0.38 | 0.35 | −0.84 | −1.17* | 0.57 | 0.47 |
| Foreign born (no) | 0.48 | 0.29 | −0.02 | −0.15 | 0.00 | −0.43 | 0.39 | 0.67 |
| Sexual identity (heterosexual) | ||||||||
| Gay/lesbian | 0.36 | 0.37 | −0.35 | −0.38 | 0.28 | 0.29 | 1.02* | 0.84* |
| Bisexual | 1.75** | 1.45** | 0.47 | 0.52 | 0.64 | 0.29 | 0.92 + | 0.86 + |
| Other | 0.18 | 0.19 | 0.03 | −0.11 | 0.39 | 0.25 | 0.17 | 0.73 + |
| Married (cohabiting) | −0.63* | −0.64* | 0.19 | 0.30 | −0.58* | −0.50 + | −1.15*** | −0.68* |
| Poor health | −0.24 | −0.61 + | −0.09 | −0.21 | 0.05 | −0.08 | 0.18 | −0.24 |
Source: National Couples’ Health and Time Use Study (n = 711).
Note: Weighted analyses. Model includes survey month.
p < .10. *p < .05. **p < .01. ***p < .001.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by grants from the Eunice Kennedy Shriver National Institute of Child Health and Human Development (R03HD105848, R01HD094081, and U01HD108779) and also benefited from support provided by the Center for Family and Demographic Research (P2CHD050959) at Bowling Green State University and the Minnesota Population Center (P2CHD041023) at the University of Minnesota.
1
The survey asks individuals, “Would you, yourself, want to have a/another child?” Responses included “Definitely yes,” “Probably yes,” “Probably no,” “Definitely no,” and “Not sure.” Respondents who reported “probably no” or “definitely no” were excluded, and the remaining were coded as desiring, or at least being open to having, a child in the future (“definitely yes,” “probably yes,” or “not sure”).
2
The analytical sample for this is based on the same question as analyzed previously regarding whether individuals intended to have a child in the next year; individuals who said they did not intend to have a child in the next year or were uncertain were asked the reasons why they were not intending to have children in the next year.
3
Cronbach’s α is a measure computing the internal reliability of summing the items.