
Abstract
Many studies suggest that people discriminate against individuals with a mental illness. Despite these generally robust patterns, however, variability in the results from laboratory experiments examining competence-based discrimination leaves questions about the specific diagnoses that elicit the discrimination and gender differences in the discriminatory behavior. Therefore, we revisit this question with a design aimed at clarifying some of the ambiguities. We examine the effects of two diagnoses (schizophrenia and depression) and a nonpsychiatric health problem (the need for leg surgery). As with other laboratory studies, we examine if and how a teammate’s psychiatric diagnosis affects participants’ willingness to accept the teammate’s problem-solving suggestions in a two-person task group. But we go beyond the previous studies by crossing the teammate gender with participant gender and by exploring the robustness in our results by examining the moderating role of numerous participant attributes (e.g., education, social desirability, parents’ education, age, political liberalism, three gender ideology scales, trust in others). We find that participants discriminate against teammates with both types of psychiatric diagnoses but not against teammates with the nonpsychiatric health problem and that this pattern is highly robust: The processes are almost entirely unrelated to teammate gender and participant attributes, including participant gender. Together, these results suggest that both schizophrenia and depression elicit competence-based discrimination, that these processes differ very little by participants’ demographic and attitudinal attributes, and that the status beliefs underlying this discrimination may be fairly uniform.
The stigma of mental illness is widespread. Decades of research suggest that people tend to fear, negatively evaluate, and seek social distance from individuals known to have a mental illness (e.g., Hipes and Gemoets 2019; Kroska et al. 2014; Lucas and Phelan 2012, 2019; Phelan et al. 2019; Thibodeau and Principino 2019). A 2018 survey showed, for example, that 52 percent of U.S. respondents were unwilling to socialize with individuals with schizophrenia, and 30 percent were unwilling to do so with individuals with depression (Pescosolido et al. 2021). This stigma also extends to perceptions of incompetence (e.g., Hipes and Gemoets 2019; Phelan et al. 2019; Sadler, Meagor, and Kaye 2012) and to behaviors that are likely rooted in perceptions of incompetence (e.g., Lucas and Phelan 2012, 2019; Manago and Mize 2022). A multistate field experiment showed, for example, that employers were less likely to call back applicants with a history of mental illness hospitalization than applicants with a history of physical injury hospitalization (Hipes et al. 2016).
Despite the generally robust patterns, however, the results from laboratory experiments examining discrimination arising from perceptions of incompetence show mixed findings regarding two factors: the specific diagnoses that elicit the discrimination and gender differences in the behavior (Kroska et al. 2015; Lucas and Phelan 2012, 2019; Manago and Mize 2022). Therefore, we revisit this question with a design aimed at clarifying some of these ambiguities. We examine the effects of two diagnoses (schizophrenia and depression) and a nonpsychiatric health problem (the need for leg surgery). As with the other four studies, we use a laboratory experiment to examine if and how a teammate’s psychiatric diagnosis affects individuals’ willingness to accept that teammate’s problem-solving suggestions in a two-person task group. But we go beyond the other studies in two ways: (1) We cross the gender of the teammate with the gender of the participant, allowing us to examine the independent and joint effects of teammate and participant gender, and (2) we explore the robustness in our results by examining the moderating role of numerous participant attributes (e.g., education, social desirability, parents’ education, age, political liberalism, three gender ideology scales, trust in others).
Mental Health as a Status Characteristic
We examine these questions within the scope conditions of status characteristics theory (SCT; Berger, Cohen, and Zelditch 1972; Berger et al. 1977; for an overview, see Berger and Webster 2018). According to SCT, when individuals work together on a valued task, the diffuse status characteristics that differentiate them shape their expectations about how they and others will perform on the task. Diffuse status characteristics are culturally defined characteristics (e.g., gender) whose states (e.g., man, woman) have different degrees of esteem in the widely shared status beliefs of the dominant culture. According to SCT, those widely shared status beliefs shape performance expectations in a consistent way, leading most group members to expect, perhaps subconsciously (for an examination of this using mental health, see Kroska et al. 2023), that those in the status-advantaged category will perform better than those in the status-disadvantaged category. Those expectations then create self-fulfilling prophecies: Individuals in the status-disadvantaged group, sensing that they have less to contribute than those in the status-advantaged group, defer to those in the status-advantaged group more frequently, whereas those in the status-advantaged group, sensing that they have more to offer, defer less frequently. Thus, SCT proposes a causal chain to explain influence processes in problem-solving groups: Widely shared status beliefs in the larger culture shape performance expectations in a fairly uniform way, and those expectations then affect deference behavior. Together, these propositions suggest that deference behavior in a given culture will be similar across individuals and, therefore, across studies.
Yet the results in the four studies that have investigated mental illness as a status characteristic do vary. All four examine individuals’ willingness to accept problem-solving suggestions from teammates with a mental illness, operationalized with hospitalization for “psychological problems” (Lucas and Phelan 2012) or a specific mental illness (Kroska et al. 2015; Lucas and Phelan 2019) or with a performance on a social competence test that is described as indicative of a (fictional) diagnosis (Manago and Mize 2022). But their results differ regarding the specific diagnoses that elicit the discrimination and the gender differences in the behavior, raising the possibility that the status beliefs about mental illness are not as widely shared as other status beliefs. We review these results next. Given the mixed results, we conclude each section with research questions rather than hypotheses.
Variation by Diagnosis
Three of the four studies have examined the effects of specific psychiatric diagnoses. Lucas and Phelan (2019) examined schizophrenia, depression, and panic disorder and found that only schizophrenia functioned as a status characteristic, with resistance to influence greater in the schizophrenia condition than both the control and the depression conditions. Kroska et al. (2015) examined schizophrenia and depression but combined the two conditions into a single condition because they did not differ significantly. The combined diagnoses functioned as a status characteristic only for men, and when the schizophrenia and depression conditions were analyzed separately among men, only the depression condition differed significantly from the control. Manago and Mize (2022) examined the effects of two fictional diagnoses combined into a single condition and found that the combined diagnoses functioned as a status characteristic only in the conditions that gave participants information about the disorder’s symptoms and how those symptoms hamper people’s lives; the combined diagnoses in the labels-only condition did not function as a status characteristic. Thus, the three studies show some conflicting patterns, with one suggesting that schizophrenia functions as a status characteristic but that depression may not, the other suggesting that depression functions as a status characteristic only among men but that schizophrenia may not, and the other suggesting that psychiatric diagnoses function as status characteristics but only when participants are knowledgeable about the symptoms and life problems connected to the diagnoses. Thus, we revisit these questions by examining the effects of two of these diagnoses (schizophrenia and depression).
We also include a nonpsychiatric health-problem condition (the need for leg surgery) to explore the extent to which these processes differ for nonpsychiatric health problems. Although researchers have hypothesized that physical ability functions as a status characteristic (Eiesland and Johnson 1996; Lucas and Phelan 2012), the sole test of that hypothesis in the scope conditions of SCT did not support it (Lucas and Phelan 2012). Thus, we revisit a version of that hypothesis using leg surgery hospitalization as an operationalization of a physical health problem. Thus, our first two research questions are:
Research Question 1: Does the effect of a psychiatric label on deference vary by diagnosis (depression vs. schizophrenia)?
Research Question 2: Do the deference patterns for psychiatric and nonpsychiatric health problems differ?
Variation by Gender
Studies conducted several decades ago showed that women were less likely than men to behave in discriminatory ways toward individuals with a mental illness and that women with a mental illness were less likely than men with a mental illness to experience discrimination (see review in Farina 1998). Consistent with those trends, the two SCT-style studies that examined the moderating role of participant gender found that men resisted problem-solving suggestions from teammates with a mental illness, whereas women did not (Kroska et al. 2015; Lucas and Phelan 2012), a gender difference that reached significance in one of the studies (Kroska et al. 2015).
Yet the source of those gender differences is unclear. Participants in one study were not told their teammate’s gender (Lucas and Phelan 2012), so it is not clear if or how the participants gendered their teammate. If participants assumed they were working with a same-sex teammate, the gender difference could reflect greater discrimination against men with a mental illness rather than greater discrimination among men participants. Participants in the other study (Kroska et al. 2015) were given their teammates’ gender, but the dyads were matched by gender, so the source of the gender difference was similarly unclear. We address this limitation by crossing the gender of the participant with the gender of the teammate, allowing us to explore the independent and joint effects of participant and teammate gender. Thus, our third research question is:
Research Question 3: Does the effect of a psychiatric label on deference vary by the gender of the participant and/or the gender of the individual with a mental illness?
Robustness to Participant Attributes
The variability in results across the four studies raises questions about the robustness of these patterns and about the uniformity of the status beliefs hypothesized to drive the deference behavior. Random assignment should create an equal distribution of status beliefs across conditions in a study. But if status beliefs vary significantly across the culture, random sampling is needed to produce a similar distribution of status beliefs and, hence, a similar pattern of deference across studies. Although we do not have a random sample of the U.S. population, we do have a large sample and numerous measures of participant attributes, allowing us to explore variation in effects by those attributes. If status beliefs about mental illness do vary in the United States and vary with the attributes we measured, the attributes should moderate the effect of condition on deference behavior. Therefore, we explore questions of robustness and status belief variability by examining the way that participant attributes moderate the effect of the hospitalization conditions, and we do so with nine attributes beyond participant gender (education, social desirability, age, parents’ education, political liberalism, ambivalent sexism toward women, benevolent attitudes toward men, hostile attitudes toward men, and trust in others). We also explore several other moderators (e.g., semester) in a series of additional robustness checks. Our use of a large sample also reduces the possibility that the study is underpowered, a growing concern in the social sciences (e.g., Arel-Bundock et al. 2022; Gelman and Carlin 2014). Thus, our final research question is:
Research Question 4: Does the effect of a psychiatric label on deference vary by participant attributes?
Here, we briefly explain why these nine attributes might affect status beliefs about mental illness and, in turn, deference to individuals with a mental illness. A college education increases liberal attitudes (Brooks and Weber 2022; Campbell and Horowitz 2016; but see Wodtke 2018), suggesting that education (i.e., year in college) may also foster more egalitarian status beliefs about mental illness. Individuals with a tendency toward socially desirability may not have more egalitarian status beliefs about mental illness, but they may feel more uncomfortable than others resisting suggestions from individuals with a mental illness. Age increases the range of a person’s life experiences, increasing the possibility of exposure to individuals with a mental illness, and exposure to individuals with a mental illness is associated with higher competence ratings of individuals with a mental illness (Hipes and Gemoets 2019). Parental education and occupational prestige reduce children’s traditional attitudes about housework (Platt and Polavieja 2016) and their gender-conventional occupational aspirations (Polavieja and Platt 2014), suggesting that parental education may also foster other egalitarian outcomes, including egalitarian status beliefs about mental illness. Political liberalism in the United States is associated with concern for disadvantaged individuals and support for equality (Graham et al. 2013; Haidt 2012) and communion (i.e., the maintenance of relationships and social functioning; Eriksson 2018), suggesting that political liberalism and liberal attitudes about gender (i.e., the inverse of ambivalent sexism toward women, benevolent attitudes toward men, and hostile attitudes toward men) will also be associated with egalitarian status beliefs about mental illness. Finally, trust in others is linked to greater tolerance of others who are different, which may include a greater respect for individuals with a mental illness.
Methods
Sample
We collected data from 559 students who were taking an undergraduate course at a public university in the South between 2013 and 2015. Students were given extra credit in their course for participating. Five of the participants were high school students who were taking a class for college credit. We have parental approval for their participation but dropped them for methodological reasons explained below. Three participants elected to have their data destroyed, a standard option in the debriefing form, which left us with 551 undergraduate students who were willing to be included. Motivation for success on the joint task is an important criterion for inclusion in SCT studies, so we excluded the cases in the bottom 3 percent (16 cases) on a two-item composite measure (“How important was it to you that your team obtained correct answers on the contrast sensitivity tasks?” and “How important was it to you to succeed on the contrast sensitivity tasks?”). These 16 cases had scores that ranged from 0 to 15.5 on a scale that ranged from 0 to 100 (M = 60.9, SD = 19.9). In the debriefing, 26 (16 men and 10 women) of the remaining 535 participants reported a clear and early suspicion that there was no teammate and/or that the task was not real, leaving 509 nonsuspicious participants who were willing to have their data retained and were motivated to succeed. Our exclusion rate, 42 of 551 (7.6 percent), is below the average rate (14.53 percent) among SCT studies that report doing exclusions, according to Dippong’s (2012) meta-analysis. The rates of exclusion by condition are 7.2 percent in the schizophrenia condition, 5.2 percent in the depression condition, 6.6 percent in the leg surgery condition, 11.2 percent in the nonpatient condition, 10.6 percent among men, and 6.2 percent among women. The difference in exclusion rates between the depression and nonpatient conditions (p = .079; two-tailed test) and by gender (p = .074; two-tailed test) are close to significance. Nonetheless, the results are similar when all 551 cases are retained and when using other cutoffs for the motivation-to-succeed composite. 1
Teammate Hospitalization History and Gender
We manipulated the teammate’s hospitalization history and gender through an information exchange. At the beginning of the computerized instructions, participants learned that they would be working with a teammate on 25 “contrast sensitivity tasks.” The instructions then asked them to fill out an electronic information sheet that would be exchanged with the teammate. The instructions explained that, “The educational, employment, and demographic information you exchange will be similar to the information you might obtain from coworkers at a job” and asked them to “Please answer the following questions about yourself carefully and accurately.” The form asked participants their gender, age, year in college, years of work experience, type of work experience, whether they had had to take a leave of absence from school or work, and if so, the reason. The teammate’s responses to the gender question and the last two questions were randomly assigned by the computer and served as the manipulation of teammate gender and teammate hospitalization history. In the nonpatient condition, the teammate response to the leave-of-absence question was “No.” In the other three conditions, the answer was “Yes,” and the answer to the follow-up question was “Last year I was hospitalized for [depression/schizophrenia/leg surgery], so I took a little time off.” Table 1 shows the descriptive statistics for these and the other variables in the analyses.
Descriptive Statistics for Variables in Analyses (N = 509).

The teammate’s responses were matched with the participant’s on the other information sheet questions so as not to introduce other status differences, and we used broad categories for all the response options except year in college so that the matching responses did not arouse suspicion. After participants were shown the teammate’s responses, the instructions asked them to write the teammate’s responses on a “Partner Information Sheet” beside the computer, a task designed to ensure that they saw the hospitalization and gender information.
High School Students
The responses to the demographic questions at the beginning of the study show that five participants were high school students. Unfortunately, however, the response options we provided for the year-in-college question in the information exchange did not include high school student, so those participants selected “freshman,” as did, of course, the computerized teammate; consequently, those participants thought they were working with someone with higher educational attainment. Therefore, we dropped those five cases to ensure that all participants perceived their teammate as equal in education.
Contrast Sensitivity Task
After exchanging information with the teammate, participants learned about the contrast sensitivity tasks. They learned that on each of the 25 tasks, the two teammates would be presented with images and that their task was to determine which of the two images included more white area. Through an example trial, they learned that they would provide an initial answer that was shared and that each teammate would then privately enter a final answer. In reality, all sets of images had an equal proportion of white, and the teammate was computerized and programmed to give an initial answer that differed from the participant’s on 20 of the trials (all but trials 1, 6, 13, 17, and 22). Participants were told that the two teammates’ final choices on each trial would be combined and that teams with scores in the top 25 percent would split a $20 bonus. (In reality, we randomly selected 25 percent of the participants to receive a $10 payment at the end of each semester.) This joint reward was designed to create a valued outcome and to motivate participants to work with the teammate to find the correct answer, contributing to the fulfillment of two SCT scope conditions. More generally, the contrast sensitivity task and the way we executed it (e.g., making 20 of the 25 trials disagreement trials) are consistent with the standardized experimental situation needed to test SCT hypotheses (Berger 2014).
Dependent Variable
Resistance to influence is the proportion of the 20 disagreement trials in which participants stay with their initial choice for their final choice in the contrast sensitivity tasks.
Other Independent Variables
Participant attributes
All but two of the participant attributes (year in college and social desirability) were measured in a separate survey that was conducted before the experiment started. We made clear in the invitation to participate, the instructions, and the informed consent sheet that the survey was unrelated to the “perceptual skills study.” For example, the invitation to participate in the study described it as a “two-part study” and explained,
The first study is a short, general survey that is being conducted by the Department of Sociology. The purpose of the survey is to gather demographic and attitudinal information from students. The survey will be immediately followed by the second study, which focuses on perceptual skills. The two studies together will take about one hour.
The consent form offered a similar explanation but explained that the purpose of the second study was to “evaluate visual skills when working with a teammate through the computer.” The instructions at the beginning of the study repeated these same points. And to deflect attention from the attitudinal measures in the survey, we included a set of filler questions at the end of the survey that focused on social networks.
Education is dummy coded and reflects the participant’s year in college (0 = first year). This variable was matched to the teammate’s during the information exchange, so education reflects both the participant’s and the teammate’s year in college. Female participant is dummy coded (0 = male). Age was measured in years and capped at 30 because the only participant older than 30 was 49, creating a highly skewed distribution and giving that one case undue influence on the model.
Parents’ education is the average of both parents’ education. We coded the educational categories in years, with values ranging from 10 for “some high school or less” to 19 for “graduate or professional degree (MA, PhD, MD, MBA, JD).” Nineteen participants reported “I don’t know” for one parent (17 cases) or both parents (2 cases). We dealt with those responses in one of three ways: (1) imputing based on occupational entries that specified educational credentials (RN and LPN; 2 cases), (2) replacing the missing value with the other parent’s education (15 cases), or (3) replacing the missing value with the gender-specific mean (computed without the cases imputed with the other-parent values) if the value was missing for both parents (2 cases). Given the limitations of mean imputation, we ran all the analyses without the two mean-imputation cases, and the results are highly similar and substantively the same. For example, the hospitalization coefficients in Models 1 and 2 and the parents’ education by hospitalization condition coefficients in Model 8 are highly similar and significant at the same levels as the models in Tables 2 and 3.
Coefficients from Ordinary Least Squares Regressions of Resistance to Teammate Influence on Conditions, Education, and Controls (N = 509).
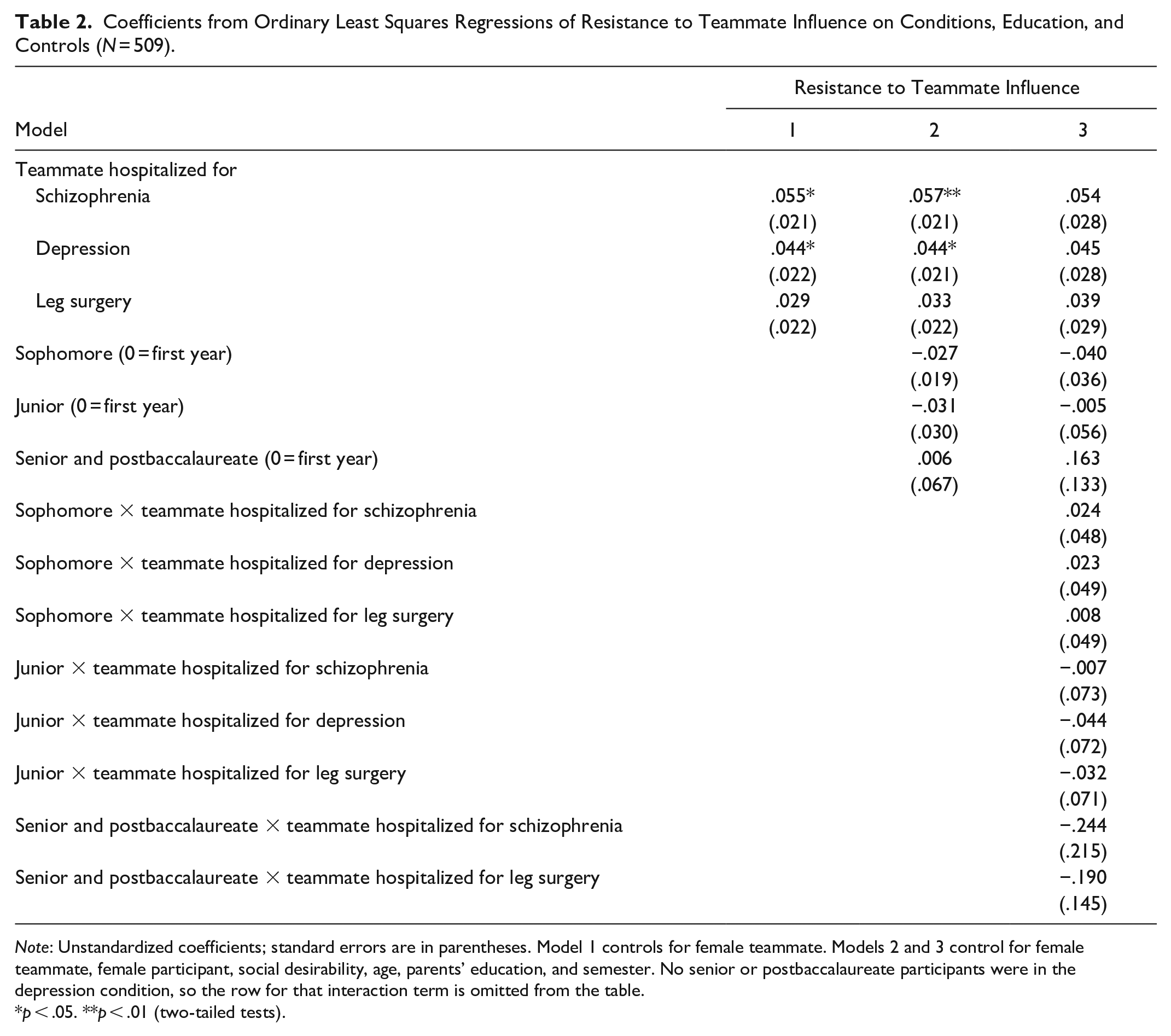
Note: Unstandardized coefficients; standard errors are in parentheses. Model 1 controls for female teammate. Models 2 and 3 control for female teammate, female participant, social desirability, age, parents’ education, and semester. No senior or postbaccalaureate participants were in the depression condition, so the row for that interaction term is omitted from the table.
p < .05. **p < .01 (two-tailed tests).
Coefficients from Ordinary Least Squares Regressions of Resistance to Teammate Influence on Conditions, Moderators, and Controls (N = 509).

Note: Unstandardized coefficients; standard errors are in parentheses. All models control for education, female teammate, female participant, social desirability, age, parents’ education, and semester.
p < .05. **p < .01 (two-tailed tests).
Coefficients from Ordinary Least Squares Regressions of Resistance to Teammate Influence on Conditions, Moderators, and Controls (N = 509).

Note: Unstandardized coefficients; standard errors are in parentheses. All models control for education, female teammate, female participant, social desirability, age, parents’ education, and semester.
p < .05. **p < .01 (two-tailed tests).
Social desirability, which was measured at the end of the study, is the average of participants’ responses to a 10-item version of the Marlowe-Crowne Social Desirability Scale (Fischer and Fick 1993). Participants gave true-false answers to statements such as “I have never intensely disliked anyone.” For the full scale, see the Appendix in the supplemental material. High scores indicate socially desirable responses (α = .53).
Political liberalism is the average of participants’ responses on two 101-point sliders placed below the prompts “Politically, I am:,” with the anchors “extremely liberal” and “extremely conservative,” and “I see myself as:,” with the anchors “100% Democrat” and “100% Republican.” We divided values by 10 and recoded them so that high values indicate liberalism (α = .80).
Ambivalent sexism is the average of participants’ responses to a 12-item version of the ambivalent sexism inventory, and benevolent attitudes toward men and hostile attitudes toward men are the average of participants’ responses to 6-item subscales of the ambivalence toward men inventory (Glick and Whitehead 2010). All three inventories are shown in the Appendix in the supplemental material. Participants report their level of agreement with each statement using a 101-point slider, anchored with “strongly disagree” and “strongly agree” (ambivalent sexism α = .81; benevolent attitudes α = .74; hostile attitudes α = .71). We divided values by 100.
Trust is the average of participants’ agreement with five statements, such as “Most people are basically honest.” For the full index, see the Appendix in the supplemental material. Response options ranged from “strongly disagree” (1) to “strongly agree” (9). High values indicate trust (α = .71).
Results
Analysis Plan
Tables 2 and 3 display models relevant to our four research questions. Table 2 presents models with education as a moderator, and Table 3 presents models with the other 10 moderators. We present the education models in a separate table because those models require 7 more rows than the other models. Table 2 also presents a model that includes only the manipulated variables (Model 1). In Table 3, the variable that is used as a moderator is listed below the model numbers, the first of each set of models is a main-effects model, and the second of each set is a model that interacts the variable listed in the heading with the hospitalization conditions. For example, the “Female Teammate” heading listed below Models 2 and 4 indicates that female teammate is interacted with the hospitalization conditions in Model 4. In Table 3, we present the coefficients for all of the moderators and interaction terms in the same set of rows, a presentation approach that condenses the table. The coefficient for the moderator is in the “Moderator (listed in column heading)” row, and the coefficients for the interaction terms are in the “Moderator × teammate hospitalized for schizophrenia/depression/leg surgery” rows.
All of the models control for education, teammate gender, participant gender, social desirability, age, parents’ education, and semester, but the coefficients for the controls are not displayed in the tables unless the control is functioning as a moderator. The first six interaction models (Model 3 in Table 2 and Models 4–8 in Table 3) examine the moderating role of variables that are also controls, so those six interaction models have the same main-effects model: Model 2. Thus, all of the columns with the “Model 2” heading show the same model but with a different fourth coefficient displayed. For example, the first Model 2 column in Table 3 displays the coefficient for female teammate in the Moderator row (b = .004, SE = .015), the second Model 2 column in Table 3 displays that same model but with the female participant coefficient displayed in the “Moderator row” (b = −.022, SE = .017), and so forth. Models 9, 11, 13, 15, and 17 are different main-effects models because they control for an additional variable (one that is not a control in all of the models), and the coefficient for that additional variable (the moderator) is displayed in the “Moderator” row. For example, Model 9 includes the variables included in Model 2 plus political liberalism, and the political liberalism coefficient is displayed in the “Moderator” row (b = −.002, SE = .003); Model 11 includes the variables included in Model 2 plus ambivalent sexism, and that coefficient is displayed in the “Moderator” row (b = −.008, SE = .056); and so forth.
As noted previously, the second column in each set of models shows the coefficients from a model that interacts the listed moderator with each of the hospitalization conditions. For example, Model 4 shows that having a female (rather than a male) teammate does not significantly moderate the effect of the schizophrenia condition (b = −.015, SE = .044), the depression condition (b = −.008, SE = .044), or the leg surgery condition (b = −.025, SE = .043). And, of course, the moderator coefficient in the interaction models shows the effect of the moderator in the control condition (i.e., when the hospitalization conditions are at zero), so Model 4 also shows that the effect of having a female teammate is not significant in the control condition (b = .016, SE = .031). The full models are displayed Tables A1 and A2 in the Appendix in the supplemental material, with Table A1 displaying the full models from Table 2 and Table A2 displaying the full models from Table 3.
We use the traditional cutoff for significance (p < .05). Given the large number of interaction models we are running, a handful of the interaction terms are likely to be significant by chance. Under those circumstances, some researchers use a lower probability level (e.g., p < .025) for classifying effects as significant. If we had done so and used a .025 level, neither of the two moderation effects we describe as significant would have counted as significant. We revisit this point in the discussion.
Research Question 1: Variation by Diagnosis
In our first research question, we ask if the effect of a psychiatric label on deference differs by diagnosis. Model 1 shows that participants who are working with a teammate hospitalized for schizophrenia (b = .055, SE = .021, p = .010) or depression (b = .044, SE = .022, p = .044) resist influence at a higher rate than those who are working with a teammate with no hospitalization history, suggesting that both diagnoses elicit competence-based discrimination. But the difference between the two effects is not significant (b = .012, SE = .022, p = .579), suggesting that the size of that discriminatory effect is similar. Model 2 shows that these patterns hold when controlling for participant attributes, as we would expect with random assignment.
Research Question 2: Psychiatric versus Nonpsychiatric Health Problems
In our second research question, we ask if deference patterns toward individuals with psychiatric and nonpsychiatric health problems differs. Models 1 and 2 suggest they do because the resistance to influence found with teammates hospitalized for a mental illness was not found for teammates hospitalized for leg surgery (Model 1: b = .029, SE = .022, p = .174), results in line with Lucas and Phelan’s (2012) findings for physical disability. Yet the differences in deference between the schizophrenia and leg surgery conditions (Model 1: b = .026, SE = .021, p = .225) and between the depression and leg surgery conditions (Model 1: b = .014, SE = .022, p = .509) are also not significant, putting leg surgery in a middle category between psychiatric illness and no illness and suggesting that a portion of the effect in the mental illness conditions may be due to the hospitalization information. Thus, as we note in the Discussion, it would be valuable in future studies to explore the effect of mental illness diagnoses without information about hospitalization.
Research Question 3: Variation by Gender
In our third research question, we ask if the effect of a psychiatric label on deference varies by participant gender or teammate gender. Models 4 and 5 show that neither teammate gender nor participant gender moderates the effect of teammate hospitalization, suggesting that the answer to both questions is no. Because teammate gender is randomly assigned, we also examined Model 4 without controls for participant attributes (not shown), and the results hold.
We also examined gender moderation in six additional models across four types of analyses: (1) with both sets of gender interactions added to Model 2; (2) with both sets of gender interactions and the female teammate by female participant interaction added to Model 2; (3) with just the female teammate by female participant interaction added to Models 2, 4, and 5; and (4) with the three-way interaction of hospitalization condition by female participant by female teammate and all the two-way combinations of those three. None of the interaction terms were significant in any of those six models, further suggesting that the effect of hospitalization history on deference is not moderated by teammate or participant gender.
Yet Models 4 and 5 do show some nonsignificant gender differences. As shown in Model 4, although the effect of teammate schizophrenia does not differ significantly by teammate gender (b = −.015, SE = .044, p = .729), the effect of teammate schizophrenia is significant when the teammate is male (b = .064, SE = .029, p = .026) but not when the teammate is female (b = .049, SE = .033, p = .133). And as shown in Model 5, although the effect of teammate schizophrenia does not differ significantly by participant gender (b = .046, SE = .046, p = .325), the effect of teammate schizophrenia is significant among female participants (b = .072, SE = .026, p = .005) but not among male participants (b = .027, SE = .039, p = .489). Thus, although neither gender difference is significant, future work examining the role of teammate and participant gender may be valuable.
Research Question 4: Robustness to Participant Attributes
In our final research question, we ask if the effect of a psychiatric label on deference varies by other (nongender) participant attributes. The interaction models in Tables 2 and 3 show that only 2 of the 32 nongender interaction terms are significant. Model 8 shows that the effect of parents’ education differs significantly between the depression and nonpatient conditions (b = −.020, SE = .009, p = .032), with parental education increasing resistance to influence from nonpatient teammates (b = .018, SE = .007, p = .007) but not from teammates with depression (b = −.002, SE = .007, p = .750). The difference in the effect of parental education between other sets of conditions approaches significance, with the difference between the depression and schizophrenia conditions coming closest (b = −.019, SE = .010, p = .055) and showing that parental education increases resistance in the schizophrenia condition (b = .017, SE = .007, p = .020) but not in the depression condition, as noted previously. We expected parental education to foster egalitarian status beliefs about mental illness. These results differ somewhat from those expectations, showing instead that parental education fosters self-confidence when working with nonpatients and individuals with schizophrenia but not when working with teammates with depression.
Model 12 shows that the effect of ambivalent sexism differs significantly between the schizophrenia and nonpatient conditions (b = −.341, SE = .156, p = .029), with ambivalent sexism reducing resistance to influence from teammates with schizophrenia (b = −.262, SE = .117, p = .025) but having no effect with nonpatient teammates (b = .079, SE = .102, p = .438). We expected ambivalent sexism to be negatively associated with egalitarian status beliefs about mental illness and, in turn, to increase resistance to influence from individuals with a mental illness. These results suggest, instead, that ambivalent sexism is associated with less (rather than more) resistance to teammates with schizophrenia. Thus, neither of the two significant moderation effects fit neatly with our expectations. But the larger pattern across the various models is an absence of moderating effects, suggesting that the deference patterns identified in Models 1 and 2 are largely similar across participant attributes.
Additional Models
We also ran dozens of additional models, and none altered our findings. We examined the moderating effect of five additional variables (semester, education with ordinal coding, English as a primary language, number of psychology courses, and number of sociology courses, with both course variables operationalized multiple ways), and none of the interaction terms reached significance. We also added both the female teammate by female participant and the female teammate by moderator (separately and together) to all the main-effects and the nongender moderation models, creating dozens of additional models not covered in the 6 described in the Research Question 3 section, and none of the new interaction terms reached significance, nor did any of the other interaction terms change in a meaningful way. These noneffects further suggest that participant attributes and temporal variability (as captured with semester) are not moderating the hospitalization effects.
Discussion
Many studies suggest that individuals behave in discriminatory ways toward individuals with a mental illness, including discriminatory behavior rooted in perceptions of incompetence (e.g., Hipes et al. 2016). Yet the four studies that have examined this question within the scope conditions of SCT show some varied findings, raising questions about the robustness of the effects and the uniformity of the status beliefs that are hypothesized to drive that discrimination. Therefore, we revisited this question with a design aimed at clarifying some of the ambiguities. We examine the effects of two diagnoses (schizophrenia and depression) and a nonpsychiatric health problem (the need for leg surgery). As with the other studies, we examined individuals’ willingness to accept problem-solving suggestions from teammates with a mental illness in a two-person task group. But we build on the other studies by crossing participant gender with teammate gender and by examining the moderating role of numerous participant attributes.
We found that both schizophrenia and depression elicited competence-based discrimination and did so at a similar level, whereas our nonpsychiatric health problem (hospitalization for leg surgery) did not. We also found that neither teammate gender nor participant gender moderated these effects and that only 2 of the remaining 32 interaction terms reached significance. In additional robustness checks, we examined additional moderators (e.g., semester, education coded differently, number of sociology courses) and various combinations of the interaction terms, and our findings across these dozens of additional models remained unchanged. As we noted earlier, given the volume of interaction effects we ran, a handful of the terms are likely to be significant by chance. In this context, some researchers use a lower probability level for classifying effects as significant. If we had done that with a .025 level, neither of the two moderation effects we described as significant would have counted as significant. Together, these results suggest that both psychiatric diagnoses function as a status characteristic, that this nonpsychiatric health problem does not, and that these patterns are almost entirely unrelated to teammate gender and the numerous participant attributes we examined.
According to SCT, widely shared status beliefs shape performance expectations in a consistent way, leading most group members to expect, perhaps subconsciously (Kroska et al. 2023), that those in the status-advantaged category will perform better on the task than those in the status-disadvantaged category. Together, these predictions suggest that deference behavior in task groups will be largely unrelated to group members’ demographic and attitudinal attributes. Our study provided support for that idea, suggesting that the status beliefs about mental illness that drive deference in task groups are fairly uniform. Nonetheless, as we discuss next, future studies exploring these processes would be useful.
Future Studies
Although we found little systematic within-condition variation in deference behavior, considerable within-condition variance remained unexplained. Thus, future studies examining possible moderators would be valuable. Studies show that some networks factors are associated with a willingness to be socially close to individuals with a mental illness. These network factors include overall contact with individuals with a mental illness (Alexander and Link 2003; Hipes and Gemoets 2019), friends and family members with a mental illness (Markowitz and Engelman 2017), strong ties to individuals with a mental illness (Perry et al. 2022), and close ties that are strengthened by the mental illness (Felix and Lynn 2022). Contact with individuals with a mental illness is also associated with higher competence ratings of vignette characters with a mental illness (Hipes and Gemoets 2019). Thus, future studies examining the moderating role of network features would be useful. Future studies could also explore the moderating role of stereotypes about mental illness (e.g., beliefs that individuals with a mental illness are weak, dangerous, and/or unpredictable) (Fox et al. 2018), given the link between stereotypes and other outcomes, such as support for increased government funding for mental health treatment (Barry and McGinty 2014).
Future work exploring gender differences in the status processes we examined would also be worthwhile, given the nonsignificant gender differences we identified. And it may be useful to make gender more salient in these studies by, for example, including gendered pronouns into the instructions that reference the teammate. Future studies could also explore other operationalizations of mental illness, including operationalizations that do not include hospitalization information. Finally, future studies using a broader base of participants would be helpful. As others have noted (e.g., Henry 2008), college students’ political liberalism could produce an underrepresentation of discriminatory behaviors in studies with college student samples. Ultimately, the ideal samples would be probability samples. Although obtaining such samples is not possible with laboratory experiments, recent progress with online status experiments (Manago, Mize, and Doan 2021) suggests that it may be possible to obtain broader and potentially representative samples with online studies of status processes.
Supplemental Material
sj-pdf-1-srd-10.1177_23780231241286678 – Supplemental material for Psychiatric Labels and Status: Exploring Variations by Gender, Diagnosis, and Participant Attributes
Supplemental material, sj-pdf-1-srd-10.1177_23780231241286678 for Psychiatric Labels and Status: Exploring Variations by Gender, Diagnosis, and Participant Attributes by Amy Kroska, Sarah K. Harkness, Kelsey N. Mattingly and Mollie A. Lovera in Socius
Footnotes
Acknowledgements
We thank Marie Brunk for assistance with data collection and Rob Clark for very helpful suggestions.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a National Science Foundation grant (No. 1227141) awarded to Amy Kroska. Any opinions, findings, and conclusions or recommendations expressed in this material are those of the authors and do not necessarily reflect the views of the National Science Foundation.
Supplemental Material
Supplemental material for this article is available online.
1
For example, if all 551 cases are retained, the focal coefficients in Model 2 are highly similar to those reported in Tables 2 and ![]() (schizophrenia: b = .060, SE = .020, p = .003; depression: b = .039, SE = .020, p = .059; leg surgery: b = .028, SE = .021, p = .168).
(schizophrenia: b = .060, SE = .020, p = .003; depression: b = .039, SE = .020, p = .059; leg surgery: b = .028, SE = .021, p = .168).
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.