
Abstract
Geographical residence predicts health and well-being. Population health, life expectancy, and mortality are partially the outcome of the characteristics of one’s social policy context. Yet how do such links occur? We extend focus from health outcomes to health behaviors and from a policy context to a broader political context. Using 20 waves of the Centers for Disease Control and Prevention Behavioral Risk Factor Surveillance System between 1993 and 2021 in combination with the Correlates of State Policy Project, we find that right-leaning political contexts—both policies and public attitudes—are predictive of riskier health behaviors. Counterfactual simulations show that these associations are due less to states becoming more different over time but rather, with political contexts increasing in their predictiveness over time. Results from this study broaden the pathways linking local politics to health and identify a key antecedent, health behaviors, that helps explain political context’s influence on health.
Geography matters for health and well-being. Whether comparing across nations or neighborhoods, studies have repeatedly demonstrated how multiple dimensions of place influence the health of local residents (Beckfield, Olafsdottir, and Bakhtiari 2013; Olafsdottir 2007). In the United States, scholars have identified state-level policy context as a core predictor of health disparities, such as general health and mortality (Kemp, Grumbach, and Montez 2022; Montez 2020; Montez and Farina 2021; Montez and Grumbach 2023; Montez, Hayward, and Zajacova 2021). Research in this area draws on findings that over the past several decades, state-level policies and regulations have not only grown in their importance relative to those at the federal and local levels (Brady, Baker, and Finnigan 2013; Lobao 2016; Montez et al. 2020), but many states have enacted large sets of policies and regulations that coherently align with partisan ideologies. This trend has resulted in both more broadly liberal and conservative policy contexts (Caughey and Warshaw 2016; Grumbach 2018; Montez et al. 2020). Recent studies have identified policy context as a fundamental cause of health and well-being (Phelan, Link, and Tehranifar 2010). That is, rather than health being responsive to the specific constraints of a specific policy, the broad system of policies and regulations creates a social context that places structural influence on population-level health and well-being (Kemp et al. 2022; Montez et al. 2020).
Research linking policy context to health has sensibly focused on what can be conceptualized as “end” results: broad health outcomes such as general self-rated health or mortality rates. Yet end health results are themselves fundamentally influenced by health behaviors (Cockerham 2005; Saint Onge and Krueger 2017; VanHeuvelen and VanHeuvelen 2019, 2021). Indeed, some health economists argue that equalizing health behavior participation would be more consequential than implementing universal health insurance (Einav and Finkelstein 2023; Nandi, Glymour, and Subramanian 2014). Furthermore, contra the popular notion that individual behaviors are in the sole domain of individual discretion, medical sociologists have shown health behaviors to be influenced by broader social structures (Cockerham 2000, 2005; Mollborn, Rigles, and Pace 2021; Short and Mollborn 2015; VanHeuvelen and VanHeuvelen 2019). And as we argue in the following, there are good reasons to anticipate that health behaviors could similarly be influenced by policy context as end result health (Kemp et al. 2022; Montez and Grumbach 2023).
However, although policy context structures end result health outcomes, health behaviors may also be influenced by additional characteristics of local politics. For example, local political parties could work with local constituencies to motivate certain behaviors or norms or be the target of broader political coalitions hoping to enact local changes (Hertel-Fernandez 2019). Moreover, research on social attitudes and behaviors shows that partisan social identities have increasingly organized sets of seemingly unrelated values and behaviors (Boutyline and Vaisey 2017; DellaPosta 2020; DellaPosta, Shi, and Macy 2015; Jost 2017). There is little reason to suspect health behaviors to be independent from nonhealth views and behaviors, suggesting health behaviors might be used to signal one’s partisan affiliations (Deryugina and Molitor 2021; Hill et al. 2022).
Thus, we argue that policy context may coexist in a broader political context differentiated not only by liberal and conservative policies but also liberal and conservative attitudes and political representation (Dowd-Arrow, Burdette, and Smith 2023; Fox, Feng, and Yumkham 2017). These dimensions are certainly related but do not fully reduce to one another. For a descriptive example, West Virginia moved more rightward in its partisan attitudes more quickly than its partisan policies during the 2000s. 1 Therefore, in this study, we expand existing work by considering multiple mechanisms linking health behaviors to a broader set of dimensions of political context than is typically examined in similar research: policies, public attitudes, and political party control.
We use 20 waves of the Centers for Disease Control and Prevention (CDC) Behavioral Risk Factor Surveillance System (BRFSS) collected between 1993 and 2021 with Correlates of State Policy Project data measuring hundreds of state-level policies and attitudes to address the following set of research questions:
Research Question 1: To what extent does state-level political context associate with health behaviors?
Research Question 2: Can we adjudicate the contribution between different dimensions of political context—policy context, public attitudes, and political party control—to state-level variation in health behaviors?
Research Question 3: How have changes to political context contributed to changes in health behaviors?
Altogether, this study provides a thorough assessment of the link between political context and health behaviors, introducing evidence of a novel mechanism linking politics at the state level to population health.
Background
Politics Predict Health Outcomes; Health Behaviors Predict Health Outcomes
Health behaviors provide a unique opportunity to examine the pathways linking political context and health because health behaviors play a critical role in shaping health outcomes (Einav and Finkelstein 2023). Studies have repeatedly found significant associations between behaviors such as diet, exercise, patterns of smoking or alcohol consumption, and a wide range of specific health conditions, including chronic illnesses (Byrne et al. 2016; Pampel 2001), functional impairment (Sharkey 2008), broad measures of health (Tsai et al. 2010), and mortality (CDC 2008; Cockerham 2023; Li et al. 2018). However, behavioral change represents a complicated approach for reducing health disparities and improving population health because health behavior formation and adoption are shaped in multiple ways and are influenced by wider systems of social structures (Cockerham 2005, 2023; Link and Phelan 1995; Montez et al. 2020; Short and Mollborn 2015). For instance, studies find health behaviors frequently depend on structural factors and institutional configurations, such as socioeconomic status, education, ethno-racial and gender identities, local organizations, labor market institutions, and the health care infrastructure (Montez et al. 2019; Phelan et al. 2010; Williams and Mohammed 2013; Wright and Perry 2010). Of particular interest for our study is the recent focus on policy contexts.
State-level policy context, or the direction of a large aggregated set of policies in a liberal or conservative direction, has been shown to be highly consequential for health outcomes, including life expectancy and physical health (Kemp et al. 2022; McFarland, Hill, and Montez 2023; Montez and Grumbach 2023). Studies in this line shift focus on the link between policy and health in a subtle but critical way. The core insights of this research, particularly the work of Montez and colleagues, is that policy context affects health not only through direct linkages between policies targeting specific behaviors or health issues but also operates as a more fundamental structural cause (Montez et al. 2020, 2022; Montez and Grumbach 2023). This focus differs from typical health policy research in behavioral economics and public health, which has traditionally privileged the identification of tight coupling between the substance of narrowly defined policies and subsequent behavioral change. Instead, studies of policy context call attention to the way states establish generally liberal versus conservative contexts by passing multiple, bundled policies across a range of domains that ultimately inform state residents’ health outcomes through a variety of overlapping pathways, including individual resources, access to care, and environmental exposures. Liberal policies tend to be associated with improved health outcomes and mortality (Montez et al. 2022) and physical health outcomes (Kemp et al. 2022). For instance, Montez et al. (2020:688) find “policies on tobacco, labor, immigration, civil rights, and the environment were strongly associated with longevity among women and men, with more liberal versions of each policy within a state predicting a nearly 1-year increase in that state’s life expectancy.” Drawing attention to state contexts as a macro-level predictor of health outcomes offers critical insights for improving health and reducing health disparities. Specifically, policy polarization research highlights underlying factors that may not be accounted for by studies more narrowly focused on altering health solely through behavioral interventions or specific policy interventions (Montez et al. 2022; Montez and Grumbach 2023).
Politics Likely Predict Health Behaviors
Although the focus on end health results is sensible, it is unlikely that structural political mechanisms only become consequential at the culmination of health outcomes, leaving structurally informed health behavioral inputs untouched. Insofar as policy context is one of the core structural influences of individual behavior (Boyer and Lutfey 2010; Conrad and Barker 2010; Mechanic and McAlpine 2010), state policy should be a structural source of health behaviors. Moreover, state-level policymaking has taken on a disproportionate role in politics (Brady et al. 2013; Lobao 2016), suggesting that this level of analysis might be increasingly consequential for all forms of health, including behaviors. Beginning with the Carter and Raegan administrations (Gerstle 2022), federal regulatory and policy actions increasingly devolved to the state level (Brady et al. 2013), and substate local policy institutions grew increasingly enervated and shifted responsibility and activity to the state level (Montez and Grumbach 2023). Thus, state-level governance has become the load-bearing policy context for passing and implementing consequential policies, likely making this the key policy context for individual health behavior responsiveness.
Policy Context, a Dimension of Political Context
We begin with an assessment of the association between state policy context and health behaviors. However, our focus on health behaviors, rather than end result health outcomes, introduces some complexities that merit additional consideration. It is sensible to focus on policies as the key mechanism of end result health outcomes because policy consequences and feedback loops can accumulate over a state resident’s life course. Policies limiting health insurance availability, lower cigarette taxes, or easing access to guns might operate incrementally, such as by complicating the ability to manage a chronic condition, reducing the incentive or ability to seek out health care, or marginally increasing the probability of experiencing injury or death from a hazardous situation. None of these minor probability shifts may be tightly bound to an immediate time relative to policy change, but rather, the accumulation of such higher probabilities over a period of years naturally would result in diverging end result health outcomes. Thus, Montez et al. (2022) show that many health effects emerge following a multiyear lag structure, such as a rise between suicide-driven mortality and right-leaning gun policies.
Yet a policy context may well coexist with other dimensions of a broader political context for health behaviors. Policies obviously influence certain health behaviors. For example, California’s Tobacco Education and Media Campaign remains a famous example in the causal literature for its short- and long-term dampening effect on smoking (Liu and Tan 2009), and taxes on sugary drinks might disincentivize or price out some residents from consuming particular products (Andreyeva, Long, and Brownell 2010). Insofar as left policies are organized around a logic of incentivizing certain health-positive behaviors and right policies are organized around individualizing decision-making, one might anticipate that policy context differences will predict health behaviors that mimic policy contexts’ predictiveness of health outcomes.
However, individual behaviors are not always responsive to the specific details of policymaking. For example, individuals may not alter behaviors, in expected directions or at all, in response to policy implementation, as demonstrated by the inconsistent effects associated with calorie-labeling requirements on restaurant menus (Kiszko et al. 2014). Moreover, many health-behavior-oriented policies often have surprising or unintended outcomes. For example, there are concerns over the unintended health consequences resulting from unmet health care needs for patients who delayed or went without health care due to changes in provider policies during the COVID-19 pandemic (Gonzalez et al. 2021).
Critically, health behaviors themselves might get incorporated into broader partisan identities that organize views and behaviors (Erikson, McIver, and Wright 1987). For example, DellaPosta et al. (2015) convincingly show the consolidation of seemingly unrelated behaviors—such as latte consumption and preferences for pickup trucks—as part of a broad process whereby political polarization patterns seemingly unrelated views and behaviors. He later uses the logic of an oil slick whereby the increase of polarization over time has spread across an increasing number of views and behaviors (DellaPosta 2020). Thus, whether or not specific sets of policies have been passed that may nudge individuals toward certain practices, resonant social identity, such as partisan affiliation, might organize the logic of how reasonable it is to pursue certain health behaviors (Boutyline and Vaisey 2017). Indeed, durable partisan identities have been used to explain wide-ranging behavioral outcomes across market research, dating patterns, and geographical sorting beyond individual composition (Gimpel et al. 2020; Huber and Malhotra 2017; Jost 2017). The politicization of health risk behaviors related to COVID-19 highlights how policy contexts and beliefs may influence individual health beliefs and behaviors (Bruine de Bruin, Saw, and Goldman 2020; Cameron et al. 2023). For example, studies find significant variation in COVID-19 vaccination rates along measures of political affiliation, with Democrats being more likely to be vaccinated compared to Republicans or Independents (Dowd-Arrow et al. 2023). It is unlikely that only policy context provided the motivating mechanisms influencing individual behaviors.
The influence of partisan identity may also occur through social mechanisms signaling group membership, social identity, or peer effects, all informing views of normative routine health behaviors (Kannan and Veazie 2018). Research shows individual health behaviors to be responsive to the peer-based local context (Einav and Finkelstein 2023; Finkelstein, Gentzkow, and Williams 2021). For example, Sacerdote (2001) found drinking frequency of a college student’s dormitory predicted their subsequent drinking patterns, and several studies have found small but detectable peer effects for smoking behaviors (Angrist 2014; Card and Giuliano 2013; Fletcher 2010). Insofar as one’s health behaviors respond to peer identities, local views and attitudes might similarly contribute to a broader political context (Choi and Fox 2022). The political attitudes held by state residents, regardless of whether residents are sufficiently involved to press lawmakers to pursue certain policy outcomes, might make certain health behaviors normative, under the reasonable assumption that health beliefs and health behaviors are not immune to the broad process-organizing patterns of behavior around partisan identity or political ideologies (Fox et al. 2017). Public attitudes are, of course, not fully reducible to policy context because the majority of residents typically do not vote in local elections (MIT 2023). Thus, for health behaviors, we require an assessment of not just a policy context but also a political context.
In total, we develop the following argument. Policy context represents one critical way that politics can affect health. Yet policies do not represent the only way politics can influence health. Views, norms, beliefs, power, and behavior organized around politics may also have an influence over the broader set of views and behaviors of state populations. Although these dimensions are related, they are not perfectly so. For example, Caughey and Warshaw (2018) use changes in broad collections of policies to predict changes in political attitudes. Policies sometimes reflect the partisan views of publics but not always or to exact degrees. We therefore conceptualize a broader political context that includes but is not limited to policies. This broad political context includes the attitudes that publics hold, the local political representation of political parties, and the policies and regulations passed, all of which might predict, to some degree, the health behaviors of state residents. We do not conceptualize these different dimensions as competing for a single predictive pathway linking politics to health behaviors but, rather, as representing a broadened set of mechanisms through which the well-established connection between politics and health may operate. Although these dimensions will often overlap, we argue that this broader conceptualization of political influence is particularly well suited to study health behaviors.
How Might Political Context Influence Health Behaviors?
If the aforementioned argument holds, then a logical follow-up question is how partisan attitudes relate to health behaviors. From our discussion of the policy context and public opinion literatures, we see two possible ways that political context could associate with health behaviors.
Studies of policy context represent one possibility: Public attitudes or state policies become more different across states. As discussed previously, Montez and her team convincingly show that state policies have become increasingly different over time with great consequence for health outcomes and mortality (Montez et al. 2020, 2023). The basic logic of these findings is that greater political differences between states translate to greater health differences between states because politics create increasingly different social contexts that ultimately result in different health and mortality outcomes. We define this conceptual change as a “spread effect” because it argues that a greater spread between state political contexts creates greater differences in health.
However, the oil slick model discussed previously suggests an alternative way that health behaviors may be used to signal partisan affiliation. Insofar as political partisanship becomes increasingly important over time in organizing otherwise discrepant individual attitudes and behaviors, any political difference between states might increase in its predictiveness of health behaviors over time. Thus, independent of any change in state-level polarization over time, partisanship might increase in its predictiveness of health behaviors simply because partisanship itself grows in importance of sorting behaviors across partisan groups. We define this possibility as an “intensity” effect because it refers to a preexisting stock of political characteristics intensifying in their relative predictiveness of health behaviors.
Data
We use 20 waves from the CDC’s BRFSS from 1993 to 2021. The BRFSS is the largest continuously conducted health survey in the world. Annual surveys typically include samples between 100,000 and 500,000 respondents, and sampling procedures are designed to produce representative samples for each state included in the survey wave. 2 Respondents ages 18 and older are included in our samples. The appendix in the supplemental material includes more information on data management.
Dependent Variables: Health Behaviors
We focus on key health behaviors consistently available in the BRFSS that are associated with health outcomes. These include: (1) current smoking status; (2) heavy drinking, or whether the respondent has two or more alcoholic drinks per day; (3) nonexercise, or whether the respondent participated in no nonwork exercise in the past month; (4) obesity status; (5) whether respondent eats fruits less than daily; (6) whether respondent eats vegetables less than daily; (7) whether respondent eats leafy greens less than daily; (8) no routine checkup in the past year; and (9) no flu shot in the past year. We binarize our outcome items in these ways to produce comparable measures across survey waves and states. Each binary item indicates riskier health behavior—for example, smoking, nonexercise, or infrequent consumption of vegetables. The appendix in the supplemental material includes additional discussion of our theoretical conceptualization of health behaviors as structurally informed.
Political Context
We focus on three primary indicators of political context.
Policy liberalism
Warshaw and Caughey (2018) use a dynamic Bayesian factor-analytic model for mixed data using around 150 individual state policies to construct state-by-year policy liberalism scores between 1936 and 2020. The bundle of state policies includes “all politically salient state policy outputs on which comparable data are available for at least five years” (Caughey and Warshaw 2018). The most commonly used policy liberalism scale comes from Grumbach (2018), which covers 1970 to 2014. We find that the two aggregated policy measures have a correlation of 0.99 in this period. The benefit of Caughey and Warshaw’s measure is that it allows for a longer period of coverage. This measure is coded so that higher values indicate a more right-leaning policy bundle.
Public attitudes
This scale, again from Caughey and Warshaw, is constructed with a dynamic hierarchical group-level item-response model (Caughey and Warshaw, 2018). State-year mass opinion data are collected from over 300 domestic policy questions across over 1,000 public opinion surveys from around 1.5 million respondents between 1936 and 2020. Caughey and Warshaw construct two measures, economic mass opinion, which covers issues such as taxes, social welfare, and labor regulation, and social questions covering issues such as alcohol, abortion, gay rights, and school prayer (Caughey and Warshaw, 2018). We use principal components analysis, which, when used on two items, necessarily constructs a first factor with equal weights for the two items, to construct an aggregate measure of mass opinion liberalism. This first component captures about two-thirds of the total variance of the two items. This scale is coded so that higher values indicate more right-leaning mass opinion.
Political party control
Political party control is measured as the average percentage of state Senate and House seats held by Republicans. 3 Data come from the University of Kentucky’s Center for Poverty Research (2023). We conceptualize this variable as occurring partially between public attitudes and policy context insofar as public partisan attitudes are partially predictive of election outcomes and election outcomes are partially predictive of policy change. All variables are coded so that higher values indicate a more right-leaning political context.
It is unlikely that contemporaneous partisan measures have an immediate effect on health behaviors, a point demonstrated by Montez et al. (2020; Montez and Grumbach 2023). We therefore lag our main partisan items by two years. This lag timing allows for individual health behaviors to follow the implementation of partisan outcomes and also allows us to include sensibly lagged state-level control variables, discussed more in the following.
Table 1 shows descriptive statistics for main dependent variables, partisan independent variables, and individual-level controls. The most frequent risky health behaviors are no flu shot in the last year (64 percent) and consuming leafy greens less than daily (77% percent), compared to low rates of smoking (19 percent), eating vegetables less than daily (17 percent,) and heavy drinking (6 percent). The right columns in Table 1 show decade-specific between-state standard deviations of health behaviors, separating the sample into three groups with even year distributions in our BRFSS sample: 1993 to 2002, 2003 to 2012, and 2013 to 2021. We see that six of the health behavior items—obesity, smoking, flu shot, doctor visitation, fruit consumption, and vegetable consumption—experienced some form of divergence over time, although fruit consumption converged in the 2013 to 2021 period. 4 Heavy drinking marginally converged, and exercise and leafy green consumption converged over the period. Overall, the trajectory of the majority of health behaviors is growing interstate variation over time. Controls are discussed in the appendix in the supplemental material.
Descriptive Statistics of Key Variables.
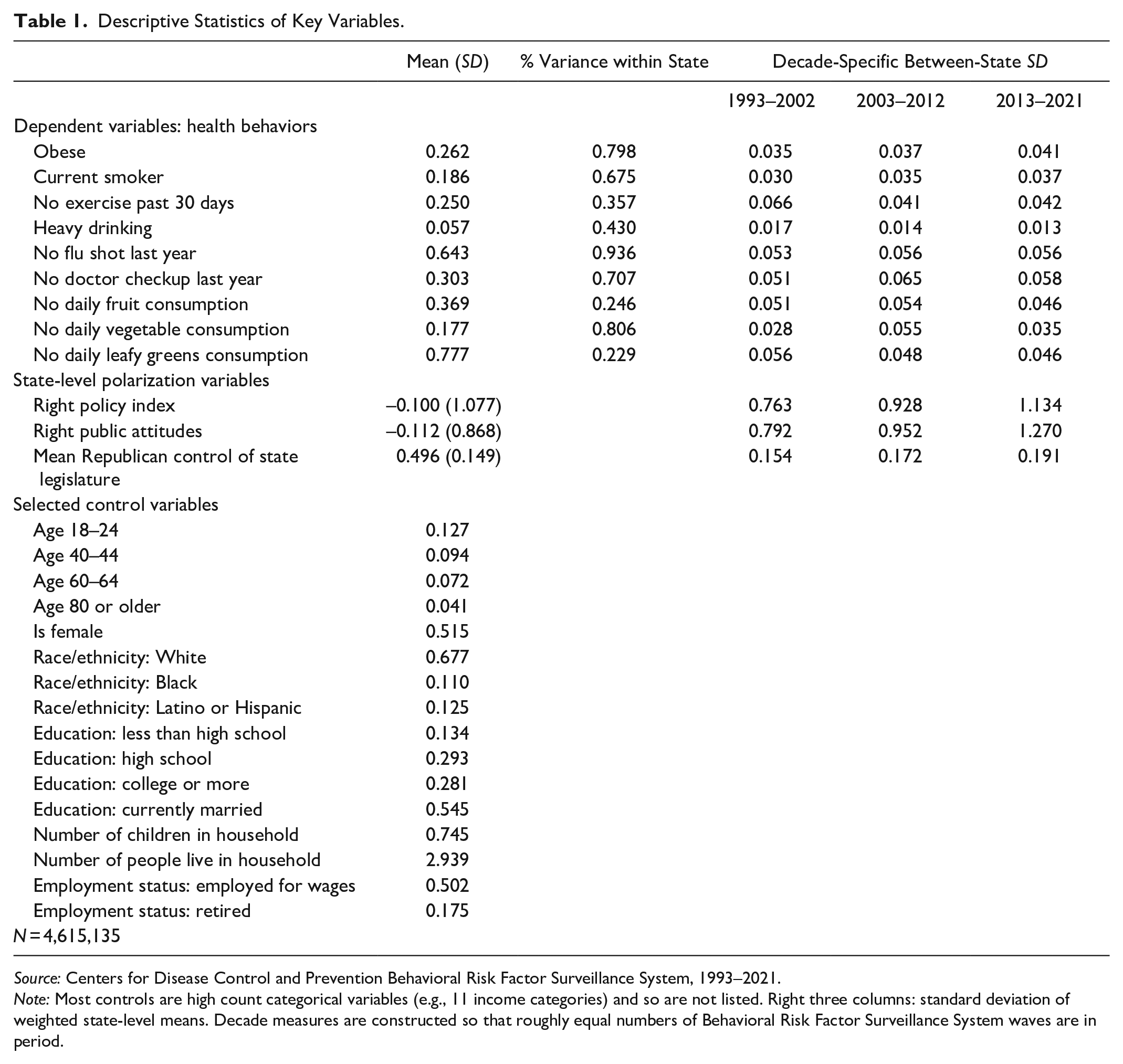
Source: Centers for Disease Control and Prevention Behavioral Risk Factor Surveillance System, 1993–2021.
Note: Most controls are high count categorical variables (e.g., 11 income categories) and so are not listed. Right three columns: standard deviation of weighted state-level means. Decade measures are constructed so that roughly equal numbers of Behavioral Risk Factor Surveillance System waves are in period.
Methods
We take different methodological approaches to answer our four research questions. First, to assess the general association between political context and health behaviors, we estimate pooled linear probability regression models using the 1993 to 2021 BRFSS samples. 5 In main results, we show regression models with all individual and state controls, with and without state effects. 6 The combination of these results shows the overall association between political context and health behaviors mixing within- and between-state differences and then showing only associations within states. In the appendix in the supplemental material, we include a more exhaustive set of regression models to assess the overall association.
To answer our second research question, we take two approaches. First, we examine model fit statistics across different combinations of political context characteristics and measurements of time. We anticipate that better fitting models will align between a particular political context measure and their specific trajectories of becoming more different across states.
Then, we conduct principal components analysis (PCA) on our three dimensions of political context. The benefit of PCA is that it rearranges the observed variation of these items into a set of uncorrelated components, allowing us to assess the relative contributions of “off diagonal” combinations, such as states with left-leaning policies and right-leaning public attitudes. Because we theoretically develop expectations that public attitudes make a contribution alongside policies, our primary focus here is to assess the extent to which public attitudes predict health behaviors beyond their correlation with other political context dimensions.
To address our third research question, we estimate a set of counterfactual simulations. Figure 1 shows a conceptual model of how health behaviors could be sorted across political contexts via either spread effects or intensity effects.

Conceptual model of counterfactual simulations.
The left panel of Figure 1 shows the first mechanism: Variation of political context can change over time. For example, imagine in 1994, California had a cigarette tax of $0.25 and Mississippi had a cigarette tax of $0.15. By 2020, California’s tax increased to $1.00 and Mississippi’s declined to $0.05. Thus, a year-specific standard deviation in cigarette tax policy is larger in 2020 than in 1994. In our spread effect counterfactual, we hold the year-specific standard deviation of political context constant at an initial time period. In the conceptual diagram in Figure 1, doing so would reduce “Time 2 Standard Deviation” to the size of “Time 1 Standard Deviation” in the left panel. The red and the blue lines represent year-specific regression lines fit between a health behavior and political context.
Second, the right panel of Figure 1 shows the slope of the fit between health behavior and political context changing between Time 1 and Time 2. In terms of regression, this implies that a 1-unit change in political context in Time 2 associates with a larger expected change in health behaviors than a similar 1-unit change in Time 1. In our second counterfactual, we set the slope in Time 2 to be equal to Time 1 and use a year-specific 1 SD change in political context to compute discrete changes in a predicted health behavior. This results in a difference between observed and counterfactual:
We can then compare the two counterfactual differences,
Results
Descriptive Trends of Key Variables
Figure 2 shows political context measures between 1985 and 2021. The left six panels show state-specific trends, with real values in the top row and deviations from state means in the bottom row. We lift out California and Mississippi, states with the most extreme average left and right policies. Dark gray lines are smoothed local polynomial of all state-years. Average policy composition changed little over time, whereas attitudes became more left-leaning from 2007 onward, and Republican control of state legislatures increased by about 17 percentage points over the period. The large right panel shows the change in standard deviations for standardized versions of these three variables and illustrates the patterns observable in the left panel: Although the timing differs, we observe substantial increases in the spreads. Policy context diverged across the whole period of study: The standard deviation increased by 0.8 from 1985 to 2021. Attitudes diverged after 2001, increasing by 0.4 SD. Republican legislature control narrowed by about 0.3 between 1985 and 1992 and then increased by 0.4 after 2009.

Political context trends over time.
Figure 3 shows state means of the nine health behaviors. The dark gray line is a local polynomial smoother of the aggregate sample, and lighter gray lines are the trajectories of individual states. As in Figure 2, we highlight California and Mississippi.
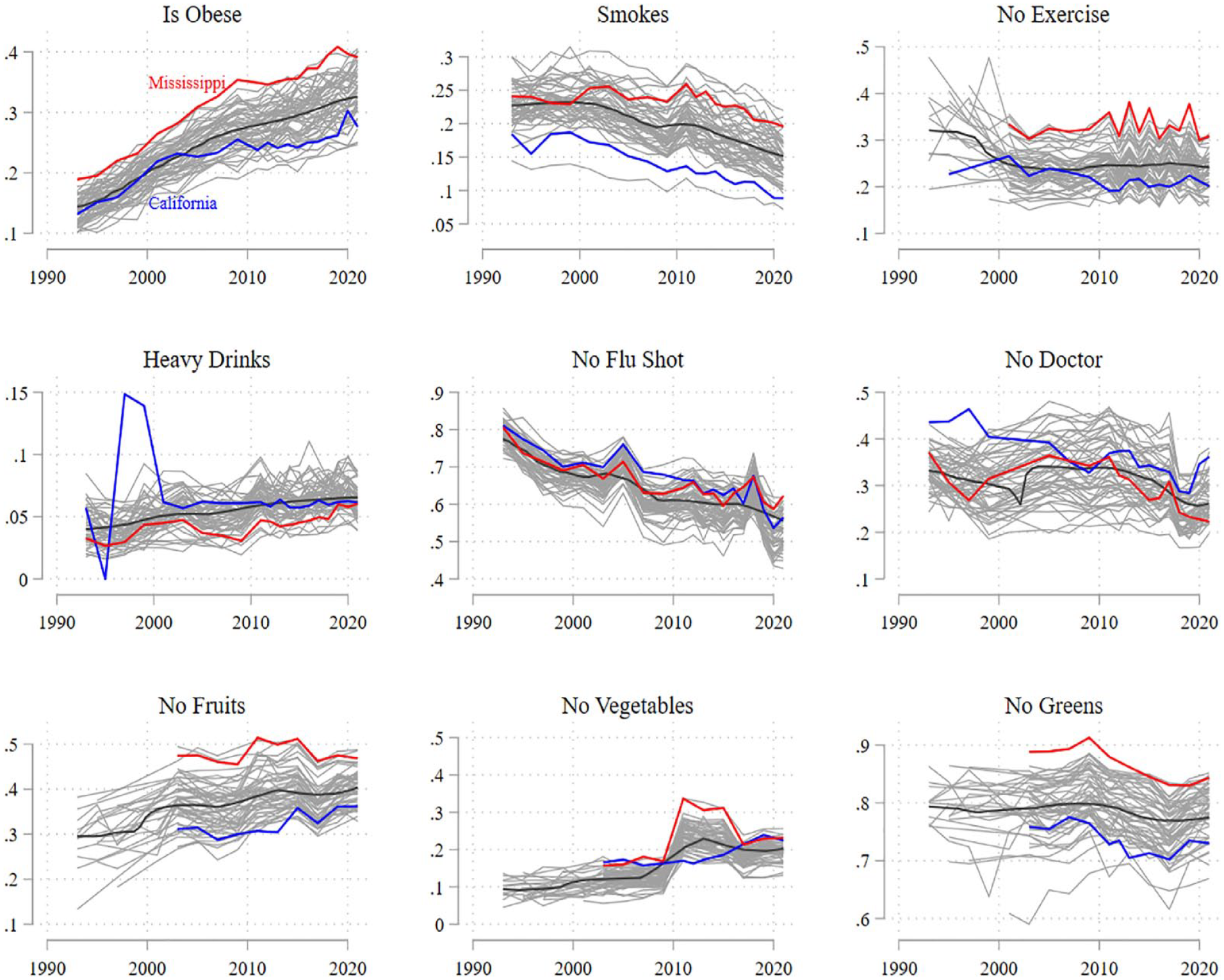
Mean state-level health behaviors over time
We observe three improving health behaviors. The proportion of smoking respondents declined from 25 percent in 1993 to 15 percent in 2021. The proportion of respondents not receiving flu shots declined from 80 percent to 60 percent, and the proportion with no regular checkup declined from 34 percent to 26 percent between 2009 and 2021. For two items, we observe little meaningful change. No exercise and no leafy greens remained relatively unchanged across the period of study. Heavy drinking experienced a modest increase from a low baseline, from about 4 percent in 1993 to about 7 percent in 2021. Finally, three health behavior items worsened over the period of study. Obesity rates increased from 15 percent to 30 percent, and the proportion of respondents not eating fruits and vegetables increased from 30 percent to 40 percent and 10 percent to 20 percent, respectively.
Looking at California and Mississippi, we see more negative health behaviors in the latter. Mississippi consistently has higher obesity rates, smoking rates, nonexercise, and infrequent fruit, vegetable, and leafy green consumption, whereas California has higher rates of heavy drinking and lower rates of regular checkups. Of course, these descriptive differences across extreme cases may be confounded by a variety of individual and state factors, so we next turn to regression analyses.
Research Question 1: Aggregate Associations
Our first goal is to determine whether dimensions of political context—policies, public attitudes, and political party control—associate with health behaviors. Table 2 shows results from full regression models with (top panel) and without (bottom panel) state-fixed effects for each of the nine health behavior outcomes and three political context characteristics. The preponderance of evidence supports our expectation that state political context is predictive of health behavior participation, particularly with more right-leaning states tending to have worse health behavior outcomes. For obesity, smoking, exercise, doctor visitation, fruit consumption, and greens consumption, we observe that more right-leaning political contexts associate with risky health behaviors. Magnitudes of associations range between around 0.005 and 0.02. Two results move against our expectations. More left political contexts have higher probabilities of heavy drinking and flu shot nonuptake. 7
Linear Probability Models Predicting Health Behaviors with State-Level Political Context and Controls.

Source: Centers for Disease Control and Prevention Behavioral Risk Factor Surveillance System, 1993–2021.
Note: Standard errors are in parentheses. Coefficients are from linear probability models and therefore are similar to average marginal effects estimated following logistic regression models. See appendix in the supplemental material for list of individual and state controls. All listed models include individual controls, state controls, and year fixed effects.
p < .10. *p < .05. **p < .01. ***p < .001 (two-tailed test).
The bottom panel of Table 2 shows results after including state fixed effects. These models extend the answer to our first research question by focusing specifically on changes in political context in states. For obesity, nonexercise, doctor visitation, fruit consumption, and greens consumption, we find similar results to models without fixed effects: More right-leaning political contexts are associated with riskier health outcomes. For vegetable consumption and heavy drinking, we observe different results: In-state rightward changes are associated with more frequent heavy drinking and less frequent vegetable consumption. 8 Results for smoking are nonsignificant, suggesting that any political context association reflects between-state associations rather than within-state trajectories.
What of the relative magnitude of these coefficients? In the appendix in the supplemental material, we show a comparison of core economic and demographic state-level standardized coefficients from models without and with state fixed effects. For both models and for all health behaviors, the range of standardized coefficients for political context variables, between 0.005 and 0.02, are typical as large or larger than the standardized coefficients for GDP per capita, unemployment rate, poverty rate, proportion with a college degree, and proportion over 65. Insofar as these contextual variables are broadly considered consequential for health behaviors, the coefficients for political context characteristics in Table 2 can be considered relatively large as well.
In total, results support the expectations we developed in response to our first research question. We find 35 of the 54 coefficients show right-leaning political contexts—whether measured by policies, attitudes, or party control—to associate with riskier health behaviors. We find 12 of the 54 coefficients show left-leaning political contexts to associate with riskier health behaviors, the large majority referring to heavy drinking and flu shot nonuptake. However, it should be noted that some of the nonsignificance and left-leaning associations are due to the high correlation of these three political context items. In sensitivity analyses included in the appendix in the supplemental material, we take an agnostic and flexible approach to model building and estimate 1,620 political context coefficients, again finding that 70 percent of coefficients indicate an association between right-leaning political contexts and riskier health behaviors but that 90 percent of these associations are positive when political contexts are added individually. Thus, the answer to our first research question is that political context is predictive of health behavior participation, with right-leaning political contexts typically associating with riskier health behaviors.
Research Question 2: Adjudication of Political Context
Our second research question focused on whether we could identify the contribution of public attitudes as a complementary dimension of political context along the more established characteristic of policy context. This question introduces some methodological complexity because of the high correlation of the three political context characteristics. We take two approaches to answer this question. First, we make a simple comparison of regression models with one of the political context variables included—policy context, public attitudes, or political party. We show results without and with state fixed effects using linear probability models and all other state and individual controls included.
Across the 36 total model comparisons, we observe that 19 prefer regression models including public attitudes. These preferred models are evenly split across models without and with state fixed effects. Additionally, we observe that 15 models prefer social policy context compared to both public attitudes and political party. We only find a small number of instances where Bayesian information criterion statistics prefer political party over public attitudes or policy context. What is most relevant for these results is that policy context sits alongside mass public attitudes as key dimensions of political context predicting individual health behaviors. As anticipated in the literature review, we find that a broader system of political characteristics is necessary to best explain the association between political context and health behaviors.
We further interrogate the conclusion developed from Table 3 by combining the variance of our political context measures. We conduct a PCA on our policy, party, and attitude measures to recombine their total variance into an alternative set of uncorrelated components. PCA results are included in the appendix in the supplemental material. The main component draws equally on all political context characteristics roughly equally and differentiates left and right political contexts. We estimate a second component that differentiates states with right-leaning attitudes and left-leaning policies from states with left-leaning attitudes and right-leaning policies. We include both of these measures in regression models predicting health behaviors.
Bayesian Information Criterion Statistic Comparison of Linear Probability Models with Different Political Context Characteristics.

Source: Centers for Disease Control and Prevention Behavioral Risk Factor Surveillance System, 1993–2021.
Note: Values listed in the table represent differences of Bayesian information criterion statistics relative to a baseline regression models that include public attitudes interacted with a linear spline of year with a knot at 2001. Negative values are in bold and indicate that the baseline model is preferred. All models include individual and country controls listed in the Data section and use linear probability models.
Table 4 shows results. Unsurprisingly, the aggregate political context measure replicates main results from Table 4. More right-leaning states and states moving rightward are associated with riskier health behaviors—higher obesity and smoking and less exercise, doctor visitation, and fruit, vegetable, and greens consumption.
Linear Probability Models Predicting Health Behaviors with Principal Components Analysis Combination of Political Context Characteristics.

Source: Centers for Disease Control and Prevention Behavioral Risk Factor Surveillance System, 1993–2021.
Note: Standard errors are in parentheses. Coefficients are from linear probability models and therefore are similar to average marginal effects estimated following logistic regression models. See appendix in the supplemental material for controls.
p < .10.
p < .05.
p < .001 (two-tailed test).
When we turn attention to the off-diagonal combination of policies and attitudes, 11 of the 18 coefficients show that states with more right-leaning attitudes and left-leaning policies have riskier health behavior outcomes. The exceptions mostly refer to heavy drinking and flu shot nonuptake. 9 These findings bolster the conclusion we drew from Table 3 to help us answer Research Question 2. Following past studies, we clearly find that policies are central to local political contexts producing riskier health behaviors. However, our evidence shows that public attitudes provide an additional pathway linking political context to health behaviors that is not fully redundant with policy context.
In total, the answer to our second research question is that for health behaviors, policy context is complemented by public attitudes. Both characteristics are predictive of individual health behaviors. Furthermore, beyond the predictive general right-left distinction that is critically driven by policies, places with right-leaning public attitudes but left-leaning policies tend to follow the aggregate patterns from Research Question 1. Rather than placing policies and attitudes in a horserace, we argue that these findings show that public attitudes provide a complementary pathway linking political context to health.
Research Question 3: Mechanisms Linking Political Context and Health Behaviors
Our final research question assesses the nature of the connection between political context and health behaviors. Previous research provides two possible mechanisms linking context and health behavior. Places could be becoming more different, which would mechanically create larger gaps in health behaviors across places (what we call a spread effect). Alternatively, political psychology and opinion research suggests that political identity has become increasingly central in consolidating views and behaviors. If this applies to health behaviors, then we might expect to see an otherwise stable difference across places become increasingly consequential in sorting health behaviors across places (intensity effect).
We compute the difference between predicted health behavior outcomes under observed conditions and counterfactual conditions. A value of 0 for the difference indicates that the counterfactual conditions produce little change to what was observed. Values that are absolutely more different than zero indicate greater contribution of a counterfactual condition.
Figure 4 shows results from our counterfactual manipulations. The left two panels show the differences in predicted health behaviors between observed and counterfactual conditions under intensity (left panel) and spread (middle panel) conditions. The nine small figures to the right revisualize results specifically for each health behavior, with values indicating the difference between observed and counterfactual conditions.
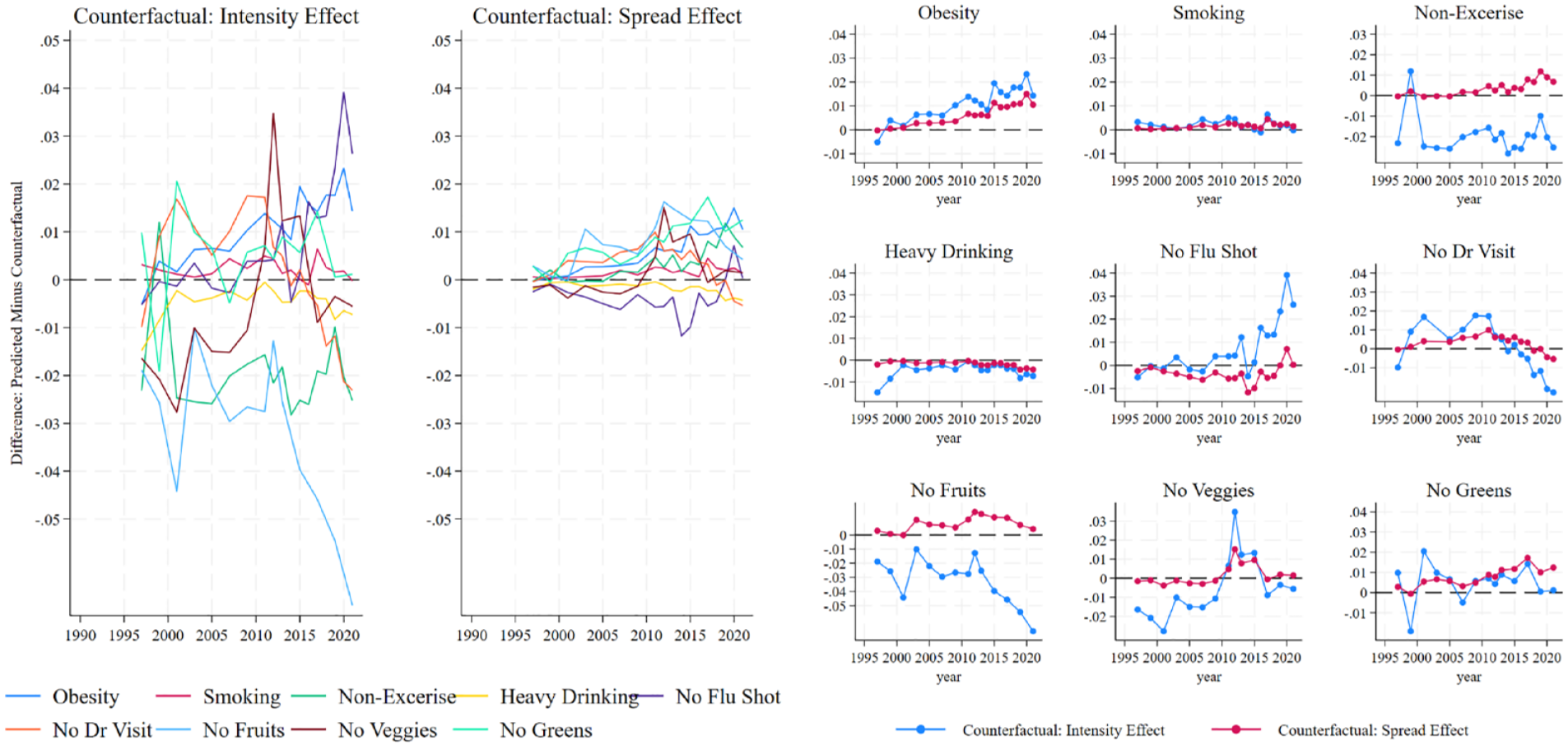
Counterfactual trends in intensity and spread effects for right public attitudes.
Results in Figure 4 clearly show that intensity effects—changes over time in the slope between political context and health behavior—produce relatively larger differences from observed trends compared to those produced by spread effects—changes over time in the year-specific variation of political context. Most of these gaps range between 0.02 and −0.02, with some—fruit nonconsumption and doctor nonvisitation—reaching between 0.04 and −0.05. The magnitudes of intensity effects can be compared to those of spread effects, which range between −0.01 and 0.01. For two health behaviors—smoking and heavy drinking—spread effect differences are close to 0.
Although both counterfactuals contribute to changes in health behaviors, our results can be interpreted as follows: Had state public attitudes remained at their mid-1990s levels, we would nevertheless expect to see much change in health behaviors across states based on public attitudes. And in contrast, if we held the intensity of sorting to mid-1990s levels but allowed for states to follow their observed divergence of public attitudes, we would expect much smaller differences in health behaviors across states.
Figure 5 replicates results using state policy context instead of public attitudes. We make a few brief points because conclusions largely replicate those drawn from Figure 4. Intensity effects create much larger differences between observed and counterfactual trends, but the relative gaps are more modest compared to those in Figure 4, ranging from about 0.02 to around −0.01. Spread effects are also more modest, ranging from around −0.005 to around 0.005. Similar to public attitudes, had states stayed at their relative policy levels in the mid-1990s, we would nevertheless expect to see substantial sorting across policy contexts over time. And in contrast, had the intensity of sorting across policy contexts stayed at its mid-1990s levels, we would have expected to see much less health behavior sorting, even allowing for policy context to diverge as observed. 10

Counterfactual trends in intensity and spread effects for right policy context.
In total, the answer to our third research question is that political context contributes to health behaviors less through the well-documented polarization of policies and attitudes across states over the past several decades and more due to the increasing association between health behaviors and political context. California and Mississippi were more similar to one another on policies and attitudes in the early 1990s than today. Our findings suggest that had this similarity remained constant through the present, we would nevertheless expect political context to increase in its predictiveness of health behavior participation.
Discussion
Because policymaking has consolidated to the state level, state-level political context has emerged as a core predictor of the geographically unequal distribution of health and well-being outcomes in the United States (Kemp et al. 2022; Montez et al. 2020, 2022). Using 20 waves of the CDC’s BRFSS covering a 30-year period, we contribute to this new line of research by demonstrating that political context does not just structure end-point health outcomes but also predicts participation in nine health behaviors across diet, exercise, tobacco use, alcohol use, and health care participation. Moreover, the nature of health behaviors rather than health outcomes required us to broaden focus from policy context to political context. Here, we show that health behaviors are effectively predicted not only by policy differences across states but also differences in attitudes held by different publics. Finally, we find that for both policies and attitudes, the intensity of aligning on stable stocks of differences, rather than growing distances in policy or attitudes between states over time, better explains health behavior participation.
Our findings make two core contributions to the literature on subnational inequalities in health and politics. First, our assessment of the evolving link between political context and health behaviors across a 30-year period indicates that over time, right-leaning and right-moving states tend to be consolidating risky health behaviors. This finding is particularly evident when it comes to the association between right-leaning state-level contexts and risky health behavior indicators of obesity, a lack of exercise, infrequent vegetable consumption, infrequent greens consumption, and smoking. These conclusions are drawn across a wide variety of modeling specifications and across different indicators of political context—policies, public attitudes, and state-level Republican control. The findings in this article also illustrate the importance of examining multiple health behaviors simultaneously. This claim is best evinced by the heterogeneity of trends across different food consumption patterns, particularly between leafy green consumption—a more stringent measure of healthy eating decisions—and the broader measure of vegetable consumption, one that could include less healthy eating decisions due to its inclusion of potatoes. We suspect that consumption of leafy greens captures more specific health-oriented behaviors, whereas more generally, food consumption represents a heterogeneous system of symbolism and views that likely becomes differentially mapped to partisan identities.
These findings align with recent research demonstrating the patterning of end-point health outcomes—self-rated health and mortality—by state-level policy context (Kemp et al. 2022; Montez et al. 2022; Montez and Grumbach 2023). Our results provide a mechanism to these established findings, extending the influence of politics earlier into the behavioral underpinnings of health outcomes. That behaviors follow a similar pattern provides a theoretically grounded mechanism that helps to explain why policy context has become so consequential for the stratification of end-point health outcomes. Indeed, health economists have recently argued that the equalization of health behaviors across the population would have a greater impact on health outcomes than the universal expansion of health insurance coverage (Einav and Finkelstein 2023). Previous studies have made a convincing argument of policy context as a critical structural factor for health (Montez et al. 2022; Montez and Farina 2021; Montez and Grumbach 2023), which necessarily requires the conceptualization of politics as a more encompassing, multicausal, and multifactorial input into health rather than a tightly coupled link between a specific policy goal and a specific health outcome (Montez and Grumbach 2023). Therefore, we see our findings as contributing to this line of research and the call to consider upstream or fundamental causes of geographic health inequalities through the lens of politics (Montez 2020; Montez and Grumbach 2023). Our findings suggest behavioral patterning as one critical pathway linking policy as a macro-level structural force and health as an outcome.
Second, we document two novel wrinkles in the connection between policy context and health behaviors that help explain their linkage. Given previous studies of political identity and behavior consolidation, we necessarily broadened our study from policy context to political context, finding that both policies and public attitudes effectively predict health behaviors. Then, using counterfactual simulations, we show that rather than a function of the increasing absolute differences in political contexts between states, health behaviors are diverging across states more intensely. That is, public attitude and policy differences across states could have remained unchanged since 1993 or 2001, and we would still have expected to see substantial alignment of health behaviors with political context.
We interpret these results as reflecting the importance of political identity and peer effects as fundamental organizers of seemingly otherwise unrelated beliefs and behaviors as a core driver of health behavior’s link to political context (Boutyline and Vaisey 2017; DellaPosta 2020; DellaPosta et al. 2015; Finkelstein et al. 2021; Frank 2021). Indeed, if our findings followed a narrower logic of health behavioral responses to specific dosages of specific policy treatments, one would reasonably anticipate the spread, or distance, of polarization measures to be the main contributor of behavioral variation because relatively larger policy gaps would represent relatively larger potential treatment dosages. Instead, our findings suggest that political context has intensified in its capacity to sort and organize health behaviors across states, which suggests a more value and identity base for health behavior participation.
Although these counterfactual findings apply to behaviors, we are skeptical of their direct contribution to end-point outcomes. Montez and colleagues provide a convincing theoretical mechanism and empirical evidence that health outcomes respond to more polarized policy contexts (Montez, 2020; Montez et al. 2020). Insofar as identity and peer effects contribute to end-point health outcomes, we suspect this would occur through the mediated effect of health behaviors. In this sense, our findings contribute to this research line by incorporating an identity-based mechanism of political context as a key structural factor. The importance of public attitudes for health behaviors highlights the need to consider both the policy context and political beliefs to more fully understand the consequences of politics for health. In connecting our findings to fundamental cause theory, it may be that the influence of political identity on health behaviors could operate as a countervailing mechanism to the more fundamentally structuring dimensions of policy divergence. Specifically, political attitudes may encompass “competitive valuations” (Clouston and Link 2021) in which individuals’ political identity or beliefs may promote their engaging in more harmful health behaviors or serve to signal their group membership. The importance of group membership and political beliefs for health risk behaviors has received some attention in studies employing a health lifestyles theoretical perspective (Cockerham 2023; Dowd-Arrow et al. 2023), including efforts to understand why certain political attitudes or affiliations may be associated with riskier health behaviors (Hill et al. 2022). We believe our findings offer an important first step in connecting the literatures on the consequences of policy divergence and political identity for health and believe future work would benefit from more deeply engaging these related but often distinct research streams.
There are several questions we could not address in this study that merit future consideration. First, we cannot identify intrastate variation based on micro-level partisan identity. The BRFSS does not include political party information, but other microdata sources could show whether a broader Republican logic influences local Democratic health behaviors, for example. We recognize that our results might reflect imbalanced partisan compositions across states and thus risk ecological fallacy issues. Future work with micro-level partisan measures is needed. Furthermore, we rely on peer effects and identity mechanisms to explain the linkage between attitude divergence and health behaviors. However, these results are necessarily speculative and should be explicitly tested. Public attitudes and social policies are correlated, and it is reasonable to ask whether the identification of some common partisan factor is preferred over the separate analysis of each. Finally, we cannot track individuals over time sorting into political contexts. The extent to which individuals with established health behaviors sort on local political contexts compared to individuals adapting to the norms of local political contexts remains an open question.
In the current article, we focus on health behaviors, not end-point health outcomes. We intentionally focus on health behaviors to theoretically and empirically extend the established literature on end-point health outcomes. We examine health behaviors that have been well established as associating with health outcomes; however, our analysis does not attempt to examine health behaviors as a mediator for health outcomes. Future research using panel data could reconcile the association between behaviors and outcomes across political context.
In terms of causality, we primarily rely on two sets of literatures that have demonstrated robust causal associations: Health behaviors are predictive of health outcomes (Einav and Finkelstein 2023), and policy context predicts end-point health and mortality (Montez et al. 2020). Although we recognize that our article itself is not fully causally identified, we operate in a literature with established causal connections. The concerns of causal connections primarily refer to historical scope, spatial heterogeneity (e.g., region-specific effect heterogeneity), and subgroup heterogeneity (e.g., Republican vs. Democrat, socioeconomic status) intersected with spatial and historical heterogeneity. Future work can help identify when and where these associations are particularly likely to hold.
Finally, in this study, we draw on established literatures to theorize how different dimensions of political context may influence health behaviors. However, future work is needed that directly explores and offers greater theoretical understanding for the mechanisms linking political contexts to health. For example, recent work focused on vaccine hesitancy has documented the importance of specifically examining the various effects of political leaders, political attitudes, and the environment in which one lives for engaging in health behaviors (Choi and Fox 2022). The current study demonstrates an extension of political context influence to health behaviors and an expansion of political factors beyond policy. Yet more work is needed on the specific interrelationship of political context dimensions, the timing of their influence, and the extent of geographical context that influences health. We hope future research develops from our broad demonstration on the link between political context factors and health behaviors.
In total, our findings verify and expand the recent line of research linking political context and health outcomes. We show that this link occurs earlier in the process of health by stratifying health behavior participation, and our results suggest an identity mechanism that runs in parallel with a policy context to explain the recent place-based political stratification of health and well-being.
Footnotes
Funding
The authors gratefully acknowledge support from the University of Minnesota Life Course Center on the Demography and Economics of Aging (P30AG066613), funded through a grant from the National Institute on Aging.
Supplemental Material
Supplemental material for this article is available online.