
Abstract
This article is the first to explore variations in alcohol, drug overdose, and suicide deaths in the United States by marital status before and after the outbreak of COVID-19 pandemic. Using the Multiple Cause-of-Death file and the American Community Survey (2000–2021), we found the nonmarried exhibit mortality rates 2 to 3 times higher in alcohol and suicide deaths and 4 to 5 times higher in drug-related deaths compared to the married population, net of education. This magnitude of marriage advantage is comparable to educational differences in these deaths. The marriage advantages are more pronounced for males than females (except in suicide, where gender differences are minor) and for White individuals compared to Black and Hispanic individuals. Furthermore, the marriage advantage widened substantially during the COVID-19 pandemic. We advocate for viewing these deaths not only through an economic lens but also as manifestations of “social pathology,” urging consideration within broader societal shifts.
The increase in mortality due to suicide, alcohol, and drug overdose has become the main factor leading to stagnation or decline in U.S. life expectancy over recent decades, apart from the COVID-19 pandemic (Case and Deaton 2015, 2017; National Academies of Sciences, Engineering & Medicine 2021; Stein et al. 2017). Previous studies often attribute the rise in mortality from suicide, alcohol, and drug overdose to worsening economic and occupational conditions. Case and Deaton’s (2015) study is the first to demonstrate this unique mortality phenomenon, highlighting the deterioration among the less educated, especially within the non-Hispanic White population. They label this phenomenon “deaths of despair” (Case and Deaton 2017, 2023). Subsequent studies find that this phenomenon is not limited to non-Hispanic White populations but extends to the entire population (Alexander, Kiang, and Barbieri 2018; Gaydosh et al. 2019). Various economic and occupational factors, including financial losses, housing, wages, labor market policies, occupation types, job insecurity, and nonstandard work arrangements, have been identified as associated with the levels and trends of these three causes of mortality (Dow et al. 2020; Hawkins et al. 2021; Kuo and Kawachi 2023; Monnat 2017).
Interpreting deaths from suicide, alcohol, and drug overdose as deaths of despair evokes Durkheim’s (1951) theory of anomic suicide. However, Durkheim indicated that suicide varies with “the degree of integration of the social groups of which the individual forms a part” (Durkheim 1951:209). According to Durkheim (1951:209–10), being strongly integrated into social life could “hold individuals under control,” allow them to “share in the collective energy and support them when exhausted,” and provide a transcendental purpose or meaning of life. Marriage, as a crucial institution for social integration, should be one of the key factors in understanding the rising mortality from three causes among U.S. adults.
More recent studies have shown that marriage establishes social norms (Cherlin 2004) and a sense of transcendental purpose/meaning of life (Burton 1998; Musick and Bumpass 2012), contributing to reducing risky and health-threatening behaviors and encouraging health-aware behaviors (Lewis and Butterfield 2007; Umberson 1992). The married population has been found to have lower levels of substance use, such as alcohol and drug use (Dinescu et al. 2016; Liang and Chikritzhs 2012). Marriage also plays a crucial role in stress reduction (Thoits 2011; Uchino 2006) and is a strong predictor of mental health outcomes, such as depression and anxiety (Cotten 1999; Hsu and Barrett 2020; Soulsby and Bennett 2015). Furthermore, marriage provides economic benefits so that people can buffer stress and have better living conditions, better access to health services, and higher quality of care (Killewald 2013; Ludwig and Brüderl 2018; Mikucka, Arránz Becker, and Wolf 2021).
Although theoretically important, very few empirical studies have directly examined the role of marriage in affecting the patterns of deaths from alcohol, drug overdose, and suicide in the United States (Chapman, Verdery, and Monnat 2021). In this article, we examine the association between marital status and these three causes of death. Previous studies have found that nonmarried individuals, especially those who are divorced, consume more alcohol (Liew 2012; Power, Rodgers, and Hope 1999) and have higher risks of suicide (Denney et al. 2009). Additionally, being never married, divorced, or widowed has been associated with higher risks of opioid misuse (Chapman et al. 2021). Building on these empirical findings and the protective role of marriage reviewed previously, we expect the unmarried population to have much higher death rates than those who are married.
Marriage has gained increasing significance in recent decades amid societal changes in the United States. As Americans become less religious (Pew, 2019), the pursuit of meaning and purpose in life is more often dependent on marriage. Increased economic uncertainty and decreased employment stability disadvantage unmarried individuals, who lack economic benefits such as the marital wage premium, spousal health insurance, and tax privileges (Anderson, Dobkin, and Gross 2012; Jovanovic, Lin, and Chang 2003; Ludwig and Brüderl 2018; Mikucka et al. 2021). The opioid crisis, with the rising misuse of prescription opioids, heroin, and fentanyl (Ciccarone 2019), further exacerbates the vulnerability of unmarried individuals, increasing their risk of opioid-related misuse and deaths (Chapman et al. 2021; Martins et al. 2017). All these contribute to the heightened vulnerability of the unmarried population, potentially accelerating their death rate.
Additionally, marriage as an institution has been declining during the last few decades, which is manifested in delayed marriage, union disruption, and one-person households, especially among young and middle-age adults (Bumpass and Lu 2000; Cohen 2021; Kennedy and Ruggles 2014; Klinenberg 2013; Ruggles 2015; Wu 2017). The married population has become more selective or privileged than the unmarried population (Cohen 2023; Tumin and Zheng 2018), which is also likely to produce an increased marriage gap in deaths from alcohol, drug overdose, and suicide over time.
The marriage gap in the three causes of death may also vary by gender and race/ethnicity. Previous studies have shown that deaths in all three causes of death are higher for males than females (Shiels et al. 2020) and that the protective role of marriage on health is more salient for males than females (Bulloch et al. 2017). Marital patterns also vary substantially by race/ethnicity. Black individuals marry later than White and Hispanic individuals and have a higher likelihood of never marrying and marital instability (Bloome and Ang 2020; Raley, Sweeney, and Wondra 2015; Zhang and Sassler 2023). The patterns and trends in death in the three causes also vary by race/ethnicity. Prescription opioids overdose during the 1990s and 2010s have been found mainly among White populations, and the increase in heroin and synthetic opioid deaths after 2010 are seen among both Black and White populations (Alexander et al. 2018; Mason et al. 2022). White individuals also seem to have higher rates and a faster increase in deaths from suicide and alcohol (Shiels et al. 2020).
The COVID-19 pandemic is likely to exacerbate the rising mortality from suicide, alcohol, and drug overdose. Unequal care, social isolation, disruptions in routine, unemployment, and financial insecurity during the pandemic (Hossain et al. 2020; Yao, Chen, and Xu 2020) and mental health challenges strain the behavioral health resources that are crucial for preventing deaths of despair (Entrup et al. 2023). Indeed, studies have shown that overdose deaths, alcohol-related deaths, and event rates for suicidal ideation rose substantially during the COVID-19 pandemic in the United States (Ammerman et al. 2021; Angus et al. 2023; Monnat 2022; Rahimi-Ardabili et al. 2022), although there is no evidence indicating an increased completed suicide rate in 2020 (Keyes et al. 2024; Pirkis et al. 2021).
The protective role of marriage appears to be particularly important in addressing the challenging impacts of the pandemic and buffering against the negative pandemic-induced impacts on mental health. Additionally, the outbreak of COVID-19 led to a decline in marriage and divorce during the early months of the pandemic (Wagner, Choi, and Cohen 2020; Westrick-Payne, Manning, and Carlson 2022), potentially altering the composition of the married population. These recent changes are expected to profoundly reshape the dynamics between marriage and deaths of despair.
To sum up, we examine how marital status is associated with three causes of deaths before and during COVID-19. We use the 2000–2021 Multiple Cause-of-Death file combined with the American Community Survey (ACS) to calculate the mortality rates for the population age 25 and older. The mortality due to suicide, alcohol, and drug overdose does not change uniformly, and the increase in extrinsic mortality is overwhelmingly driven by drug-related mortality (Masters, Tilstra, and Simon 2017; Stein et al. 2017). Thus, we analyze the three types of death separately. Considering existing studies that emphasize the importance of education in explaining the increase (Case and Deaton 2015, 2017; Gutin and Hummer 2020; Knapp et al. 2019; Shiels et al. 2020; Stein et al. 2017), we stratify our analysis by education to see if the relationship between marital status and the death rates persists net of education. We also examine whether the association between marital status and the three deaths varies by gender and race/ethnicity. Our study enriches the discussion about the deaths of despair crisis in the United States and deepens our understanding of the decline of marriage and population health.
Data and Method
Data
The vital statistics of the Multiple Cause-of-Death file from the Centers of Disease Control and Prevention (2000–2021) includes all death certificates in the United States, which provide the demographic variables including sex, race, age at death, marital status, Hispanic origin, education, and underlying and multiple causes of death (coded by ICD-10). We restrict our analysis to United States adults ages 25 and older. The Multiple Cause-of-Death file only provides the counts of deaths. To calculate mortality rates, we use population denominators estimated from ACS data with population weights (Case and Deaton 2015; Singh, Rodriguez-Lainz, and Kogan 2013).
Variables
Marital status is coded into currently married, divorced, widowed, and never married. For readability, we combine divorced, widowed, and never married into one category, currently unmarried, when examining marriage advantage by gender, education, and race. Education is also coded as a binary variable: less than BA versus BA or more. Age is coded into five-year age groups (25–29, 30–34 . . . 80–84, 85+). We calculate the death rates for non-Hispanic White, non-Hispanic Black, and Hispanic populations separately.
Deaths from alcohol, suicide, and drugs are defined based on ICD-10 codes and are consistent with Case and Deaton’s (2015) analysis. The deaths related to alcohol include alcohol-related disorder, alcohol, and chronic liver diseases (ICD-10: F10-F10.9, K70-70.9, K73-74.9). Deaths related to drug overdose include deaths from drug poisonings, drug dependency, and abuse (ICD-10: F11-16, F19-F19.9, X40-X45.9, X 85-X 85.9, Y10-Y15.9). And deaths from suicide include deaths from self-inflicted harm (ICD-10: U03-U03.9, X60-X84.9, Y87.0).
Analysis Plan
In the first part of analysis, we calculate the overall trends in age-standardized mortality rates from alcohol, drug overdose, and suicides from 2000 to 2021. The ACS 2000 population is used as the standard population. Then we calculate the death rates by marital status to examine the marriage advantage in the three causes of death by marriage mortality ratio—the ratio of the nonmarried to married mortality rates (Cohen 2019; Durkheim 1951). We include mortality rates for the three types of deaths by education to compare the marriage advantage with educational differences (see Appendix). To quantitatively measure the temporal changes in these mortality rates, we use joint point regression analysis to test whether trends are statistically significant. The average annual percentage change is calculated to indicate the percentage change of the mortality rate per year on average from 2000 to 2021 (Clegg et al. 2009). We stratify the analysis by education to see whether the marriage advantage in morality exists within each educational attainment group and how the marriage advantage varies across education. We also examine the gender and race/ethnicity difference in marriage advantage.
Results
Figure 1 shows the trends in mortality caused by alcohol, drug overdose, and suicide in the United States from 2000 to 2021 for the population age 25 and older. The rates are standardized based on the age structure of the U.S. 2000 standard population. The mortality rates of all three types of deaths increased over the past two decades. Of particular significance is the sharp rise in mortality attributed to drug overdose, which increased from about 6 deaths per 100,000 to 46 deaths per 100,000, averaging a 9.0 percent (p < .05) annual rise during the studied period. The alcohol-related deaths increased by 2.2 percent per year (p < .05). Suicide increased by 1.1 percent per year (p < .05). Notably, deaths from alcohol and drug overdose climbed even more rapidly after the outbreak of COVID-19. From 2019 to 2021, the death rates from alcohol and drug overdose increased by 15.2 percent (p < .05) and 18.6% (p < .05) per year on average, respectively. In contrast, mortality caused by suicide increased from 2007 to 2018 but did not increase significantly during the pandemic.
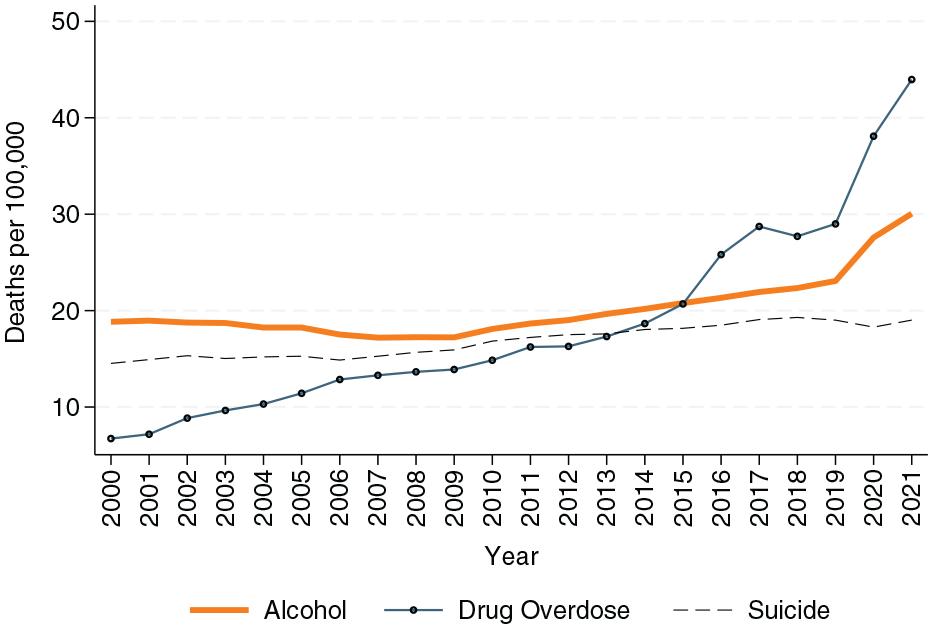
The trends of death rates from alcohol, drug overdose, and suicide for U.S. adults ages 25 and above (2000–2021).
Table 1 reports the pre- and postpandemic age-standardized mortality rates from alcohol, drug overdose, and suicide by marital status. Across all three causes of death, the married population shows lower mortality rates compared to those who are divorced, widowed, or never married. For example, in 2000, the ratio of mortality rates for widowed, divorced, and widowed versus the married was about 2:3 for alcohol-related death and 2.1:2.7 for suicide. The marriage advantage is especially large for deaths from drug overdose, where the ratio of unmarried to married mortality is about 4:5.
The Age-Standardized Mortality Rates in Alcohol, Drug Overdose, and Suicide before and after the Outbreak of the COVID-19 Pandemic by Marital Status.

Note: All rates are age standardized with the U.S. 2000 standard population. The tests of significance are only for average annual percentage change.
p < .05.
The differences in mortality rates by marital status are of comparable magnitude to mortality differences by education. For example, the unmarried/married ratios of mortality rate caused by alcohol in 2021 range from 2.9 to 3.3, which are comparable to the ratios of the same mortality rate between people with and without a bachelor’s degree (between 2.2 and 3.3; see Appendix Table S1). Similar patterns can also be observed among other causes of deaths and across years.
Although mortality rates increased for all three causes of death, the rise was less pronounced among the married population compared to their unmarried counterparts. As shown in Table 1, between 2000 and 2021, the alcohol-related mortality rate for the married population increased by 4.6 (from 12.5 to 17.1, per 100,000), whereas among their not married counterparts, the mortality rates increased by 18.7 for the divorced, 20.9 for the widowed, and 15.6 for the never married. Similarly, married people show a 9.4 increase in the death rate caused by drug overdose compared to a dramatic increase ranging from 71.9 to 96.9 among the not married population.
As such, over time, the marriage advantage in terms of mortality rates has become more prominent. As evident from the last panel in Table 1, for each nonmarried category (i.e., the divorced, widowed, and never married), we observe an increased unmarried-married ratio of mortality rates over time, especially for the mortality caused by drug overdose. This widening marriage accelerated during COVID-19. During the pandemic, the surge in all three types of deaths was much higher among the divorced, widowed, or never married population than the married population. For example, from 2019 to 2021, the alcohol-related death increased on average by 9.63 percent per year (p < .05), whereas the number was about 16.26 percent for the divorced (p < .05), and about 19 percent for those widowed and never married (p < .05). The deaths from drugs did not change that much for the married, and suicide deaths from the married even declined a little bit from 2019 to 2021.
Figure 2 presents the unmarried-married ratios in mortality by education and gender. Stratifying the analyses by education helps examine the independent association of marriage with mortality net of education. Because the mortality rates of the divorced, widowed, or not married in Table 1 present similar patterns, we combine all three into one category (unmarried) to make the results and figures more concise. As shown, within each category of education, the marriage advantages (the unmarried-married ratios) remain substantial, and the sizes of the ratios are comparable to the overall size presented in Table 1. This suggests that the marriage advantage in three types of mortality rates is substantial, robust, and independent of education.

The unmarried/married ratio in mortality rates from alcohol, drug overdose, and suicide for U.S. adults ages 25 and above (2000–2021) by gender and education.
Furthermore, for alcohol- and drug-related deaths, the ratio is much larger among males than females. For example, the unmarried-married ratios in alcohol-related deaths are about 2:3 for females, but the ratios are 3:4 or even higher for the males. Similar gender differences are found for drug-related deaths. But the ratios in suicide present similar sizes between males and females. The size of ratios seems to be larger among those with a bachelor’s degree, especially for alcohol deaths since 2015, male drug-related deaths, and suicide. For alcohol- and drug-related deaths, the increase in unmarried-married ratios since 2015 is also steeper among those with a bachelor’s degree.
Ratio is a relative measure of marriage advantage, and small denominators in ratio calculations might lead to misleading conclusions. In Appendix Figure S1, we report the same analysis as in Figure 2 but present the absolute mortality rates for a robustness check. The absolute magnitude of deaths rates is much higher among the less educated population, and within each education group, the mortality rates are higher for the unmarried than for the married. In most cases, married people with less education have very close levels and similar increases in mortality rates as those with a bachelor’s degree but not married. Still, in each case, the survival advantage of marriage is consistently stronger for males than for females.
Figure 3 presents the racial differences of the unmarried-married ratios by gender. Consistent with the patterns observed earlier, the advantage of the married over their unmarried counterparts is pronounced across all three types of deaths within each racial group. However, this advantage is not evenly distributed across race/ethnicity. The unmarried-married ratios are most prominent for the White population, although they are also observed among Black and Hispanic populations. For example, for alcohol-related deaths, the ratio has risen to about 4.5 for White males but only to about 3 for Black and Hispanic males.

The unmarried/married ratio in mortality rates from alcohol, drug overdose, and suicide for U.S. adults ages 25 and above (2000–2021) by gender and race.
The reasons leading to lower unmarried-married mortality ratios for Black and Hispanic individuals vary by cause of death. Appendix Figure S2 presents the absolute mortality rates by race and marital status. For alcohol-related deaths among Hispanic individuals and drug-related deaths among Black individuals, the lower ratios stem from higher mortality rates among married individuals, especially females. Conversely, for alcohol-related deaths among Black individuals, drug-related deaths among Hispanic individuals, and suicide among both Black and Hispanic individuals, the lower ratios result from lower mortality rates in the unmarried group compared to the married White group.
Discussion and Conclusion
This article is the first to examine the association between marital status and deaths from alcohol, drug overdose, and suicide among the U.S. population ages 25 and above from 2000 to 2021. We find the death rates from alcohol, drug overdose, and suicide have risen in the United States, especially after 2010 to 2015. Married people have a survival advantage in deaths from alcohol, drug overdose, and suicide net of education. The mortality rates among the unmarried population rose to 2 to 3 times higher than the married population in alcohol-related death, 4 to 5 times higher in deaths from drug overdose, and 2.1 to 2.7 times higher in deaths from suicide. This magnitude of marriage advantage is comparable to the educational differences in the three types of deaths.
The growing number of deaths from alcohol, drug overdoses, and suicide is argued to result from changes in the economy (Hawkins et al. 2021; Kuo and Kawachi 2023). However, it is crucial to recognize that these trends are not exclusively associated with economic factors. We view them in part as a form of “social pathology” (Rogers and Hackenberg 1987) and consider them along with broader shifts in society. In this article, using the Multiple Cause-of-Death file from the Centers for Disease Control and Prevention (2000–2021), we reveal that marriage, as a crucial social institution, is an important factor in understanding the three types of deaths.
The marriage advantages in three deaths are consistent with Durkheim’s (1951) argument about marriage as an institution of social integration and with previous studies about marriage’s protecting effect on health (Cherlin 2004; Duncan, Wilkerson, and England 2006; Thoits 2011; Uchino 2006). Furthermore, we find that the mortality gap by marital status has been widening over time, both before and especially during the pandemic (2020–2021). Several social changes might contribute. First, marriage has become more selective in the United States, making the married population more privileged (Cohen, 2023). This trend may result in those with poorer health being less likely to marry. Studies found that the health-related marriage selection—those healthier are more likely to get married—is more pronounced among those of lower socioeconomic status (Choi and Marks 2011; Waldron, Hughes, and Brooks 1996). However, our study finds that the association between marriage and deaths in alcohol, suicide, and drug overdose is stronger among higher-educated adults. This seems to minimize the concern that our results are primarily driven by selection. The disadvantages for unmarried individuals in three types of deaths might be exacerbated by heightened levels of economic uncertainty and educational disparities (Binder and Bound 2019; Hayward and Farina 2023) and by the opioid crisis in the United States (Caudillo and Villarreal 2021). Their vulnerability has deepened, leading to a rapid rise in the death rate among the unmarried population.
We find that the survival advantage of marriage is stronger for drug-related deaths than for alcohol-related deaths and suicide. The unmarried/married mortality ratios surged the most for drug-related deaths between 2000 and 2021. The mechanisms behind these differences are not well understood, but one possibility is the unique opioid crisis in the United States, which increases the risk for unmarried individuals. The availability and use of prescription opioids (e.g., OxyContin), followed by heroin and fentanyl misuse (Alpert et al. 2022; Ciccarone 2019; Ruhm 2019), have significantly increased death risks in the United States, disproportionately affecting unmarried Americans (Altekruse et al. 2020). We recommend further studies on this topic.
We find gender differences in the marriage advantages. In fact, most of the deaths from alcohol, drug overdose, and suicide happened among males, and mortality increased faster among males than females in all three types of deaths (Masters et al. 2017). The marriage advantages are higher for males than females for alcohol- and drug-related deaths. This is consistent with previous studies that highlight the protective effect of marriage being larger for males than for females (Brockmann and Klein 2004; Duncan et al. 2006; Gardner and Oswald 2004; Kiecolt-Glaser and Newton 2001; Mikucka et al. 2021). We find that the unmarried-married ratios are similar between males and females for suicide and that the absolute magnitude of mortality rates for females is substantially large (although still much lower than the males).
We also find race differences in the marriage advantage. White individuals have higher unmarried-married ratios in these three types of deaths, suggesting a greater level of marriage protection among the White population. The high ratio among the White population is due to high death rates among unmarried White individuals (especially men) in drug overdose and alcohol-related deaths. Additionally, married Black and Hispanic individuals have relatively high levels of deaths in alcohol- and drug-related deaths, making the ratios not that large compared to married White individuals. Deaths in suicide present unique patterns: Among both married or unmarried populations, the White population has higher mortality rates than Black and Hispanic populations.
This article is also the first to examine the marriage-mortality association across the three types of death during the COVID-19 pandemic. Our results show that alcohol- and drug-related deaths surged with a steeper speed during the pandemic, whereas deaths from suicide appear to be less affected. This is consistent with previous studies on trends in three types of deaths (Angus et al. 2023; Rahimi-Ardabili et al. 2022). We also find the surge of deaths in alcohol- and drug-related deaths is mainly concentrated among the unmarried population, making the marriage gap rise substantially for both males and females across all educational and race subgroups.
There are a few limitations to our analysis that should be taken into account. First, the mortality records data we use do not include information about some individual characteristics, including income, occupation, social ties, lifestyle, and prior health conditions. Neither could we track the longitudinal process of the individuals’ marital status and deaths. These limit our ability to distinguish causal effects or correlation between marital status and three types of deaths (Tumin and Zheng 2018). Furthermore, we do not distinguish whether the increasing mortality advantage over time is due to marriage becoming more selective or the protective effect of marriage becoming more essential. All these limitations should be considered in future studies.
Future studies should explore the differences in the marriage advantage in contrast to different unmarried groups (divorced, widowed, and never married). In this article, we observed that divorced individuals have higher rates of alcohol-related deaths and suicide, whereas the never married or widowed have higher drug overdose deaths. Previous research has discussed these differences extensively in all-cause mortality (Denney et al. 2009; Næss, Mehlum, and Qin 2021; Power et al. 1999; Rendall et al. 2011; Shiue et al. 2022). Future research should examine these subtle differences in deaths from alcohol, drug overdose, and suicide, especially with longitudinal data at the individual level.
Despite these limitations, this article highlights marriage as a crucial social institution that offers protective effects against deaths from suicide, alcohol, and drug overdose. To reduce these deaths, public health interventions should address the needs of vulnerable populations, including unmarried individuals, especially men. The study also suggests further research to estimate to what extent declining marriage rates affect these mortality rates and whether this effect varies among different groups of unmarried people (divorced, widowed, and never married). Future research should also explore the interplay between marital status, economic conditions, and mortality rates and consider variations by gender, race, age, socioeconomic status, and broader social contexts, such as drug use environments and policies.
Supplemental Material
sj-docx-1-srd-10.1177_23780231241275429 – Supplemental material for Marital Status and Deaths from Alcohol, Drug Overdose, and Suicide in the United States: 2000–2021
Supplemental material, sj-docx-1-srd-10.1177_23780231241275429 for Marital Status and Deaths from Alcohol, Drug Overdose, and Suicide in the United States: 2000–2021 by Hangqing Ruan, Melody Ge Gao, Yajie Xiong and Philip N. Cohen in Socius
Footnotes
Author Contributions
Hangqing Ruan: Conceptualization (lead); data curation (lead); methodology (lead); formal analysis (lead); project administration (equal); writing – original draft (equal); writing – reviewing and editing (equal). Melody G. Gao: Conceptualization (supporting); project administration (equal); writing – original draft (equal); writing – reviewing and editing (equal). Yajie Xiong: Data curation (supporting); formal analysis (supporting); writing – original draft (supporting). Philip N. Cohen: Reviewing and editing (equal).
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.