
Abstract
Sociological research has documented myriad associations between individuals’ overall social connectedness and health but rarely considers the shorter-term dynamics of social life that may underlie these associations. The authors examine how being with others (“social accompaniment”) is associated with momentary experiences of symptoms, drawing smartphone-based ecological momentary assessments (n = 12,760) collected from 342 older adults from the Chicago Health and Activity Space in Real-Time study. The authors find that patterns of social accompaniment are distinct from global measures of social integration such as network size. Older adults who are in the company of friends or neighbors are significantly less likely to experience momentary fatigue and stress, even after accounting for global measures of social integration. These results suggest that social accompaniment has unique implications for short-term health outcomes. New theoretical perspectives and empirical analyses are needed to better understand the dynamic nature of everyday social accompaniment and its longer-term implications for well-being.
An extensive literature documents the health implications of social relationships (Smith and Christakis 2008; Valente 2010). Being socially connected carries numerous physical, mental, and emotional health benefits. Likewise, being socially isolated and experiencing loneliness carry significant health risks, with implications for morbidity and mortality (Holt-Lunstad, Smith, and Layton 2010), prompting calls for policy changes that promote social integration (Holt-Lunstad 2017). The robustness of this literature is evident, in part, through the consistency of findings across populations and studies, and in the breadth of social and health measures that have been operationalized in this work. Although it is generally understood that patterns in individuals’ health and social relationships unfold over time in real-world contexts, the vast majority of existing sociological research on this topic relies on summary (often retrospective) measures of respondents’ social lives and health that are captured at a particular point in time (Shiffman, Stone, and Hufford 2008). Indeed, widely used global measures of social connectedness or isolation, such as network size and perceived social support, capture respondents’ assessments of their access to social confidants and social support in general or overall. Missing from this literature, we argue, is a more micro-level, granular consideration of whether momentary experiences of social connectedness have health implications. In other words, we ask whether “social accompaniment,” or being copresent with a social tie, is relevant for health in the moment. Do people feel better when they’re together?
In-person social accompaniment is theorized as a key mechanism through which social connections, broadly considered, shape health. Instrumental, practical, and “just-in-time” supports are among the ways that social ties can benefit individual well-being (House, Umberson, and Landis 1988), and these resources may be most readily available through in-person social company (York Cornwell and Goldman 2021). In-person social accompaniment may be particularly important for older adults who are “aging in place” because it enables others to help them complete routine tasks that may be more difficult to accomplish independently (Litwin and Shiovitz-Ezra 2006).
Focusing on momentary social accompaniment also allows consideration of the complexities in how individuals’ social contexts change and unfold in real time, dynamics that are overlooked by summary measures such as network size or average levels of social interaction. By examining the social context and its health implications in real time, we can gain insight into how broader contextual processes affect daily and short-term health experiences, in ways that may have longer-term health implications (Cohen, Janicki-Deverts, and Miller 2007; Weber, Angerer, and Apolinário-Hagen 2022).
In this article, we examine how being physically copresent with a social tie, hereafter referred to as “social accompaniment,” is associated with momentary experiences of physiological symptoms indicative of distress. We use three waves of ecological momentary assessments (EMAs) collected in 2018 and 2019 as part of the Chicago Health and Activity Space in Real-Time (CHART) study. We begin by examining how momentary social accompaniment is associated with global measures of social integration, such as network size. Are people with larger social networks more likely to be accompanied as they go about their day? Then, we consider how real-time accompaniment is associated with physiological symptoms, after accounting for widely used global measures of social integration. This investigation allows us to elucidate how health-relevant processes that unfold in real time may be distinct from the longer-term associations that are captured through more traditional survey measures. Our findings suggest that social accompaniment, particularly with nonkin, is associated with lower levels of real-time fatigue and stress, even when accounting for baseline measures of respondent social integration and overall health. Real-time engagement in recreational or social activities also plays a role. We discuss the implications of these findings for research on social integration and well-being.
Background
Some of the strongest evidence of the generally health-protective effects of social integration comes from literature documenting the harmful effects of social isolation, or the lack of social integration (Bearman and Moody 2004; Finlay and Kobayashi 2018). Social isolation and loneliness are associated with a range of adverse health outcomes, including increased morbidity, cardiovascular risk, and even mortality (Holt-Lunstad 2020, 2021).
Social ties benefit health through several pathways. First, close social ties are key sources of social support (House et al. 1988; Wellman and Wortley 1990), including assistance with everyday tasks (e.g., grocery shopping, home repairs) and the provision of material needs, such as housing, food, and financial assistance that have direct implications for health and well-being (Berkman et al. 2000; Haines and Hurlbert 1992; House et al. 1988; Hurlbert, Haines, and Beggs 2000). In buffering experiences of stress, social relationships can lessen the activation of the stress response and other physiological responses that can adversely shape health outcomes (McEwen and McEwen 2017; Thoits 1995, 2011; Umberson, Crosnoe, and Reczek 2010). Social support can also include offering advice that benefits health, such as recommending a physician, treatment approach, or exercise regimen. A second pathway is through social control, or lack thereof (Craddock et al. 2015; Umberson 1992). As sources of influence, close social ties can shape an individual’s health behaviors (e.g., diet, physical activity, medication adherence), including health risks (e.g., smoking, alcohol, drug use), through monitoring and informal control mechanisms that can promote or discourage actions that have longer term health implications. Third, social ties are often main sources of social engagement, coparticipation in social activities, and fulfilling social roles, with greater social network relationship diversity benefiting cognitive and physical health, as well as risk of mortality (Ali et al. 2018; Barefoot et al. 2005). Whereas social isolation, or a lack of social ties, is a well-established contributor to adverse health outcomes (Holt-Lunstad and Steptoe 2022), an individual’s perceptions of available social support, companionship, and loneliness, can also have physiological and psychological implications (York Cornwell and Waite 2009).
An important caveat to the research emphasis on the health benefits of social ties is that not all close social ties are supportive or health enhancing. Social relationships can be a major source of stress (Thoits 2011). One’s closest, frequently accessed social ties may include family or friends who demand extensive support or relationships characterized by conflict or ambivalence. The presence of difficult ties in older adults’ social networks is associated with heightened physiological distress and loneliness, although these negative effects can be buffered by the presence of supportive social ties (Offer 2020, 2021). Likewise, having more ties that are unsupportive is associated with increased cardiovascular risk (York Cornwell and Waite 2012). Social ties can also promote harmful health behaviors such as substance use (O’Donnell et al. 2019; Phillips et al. 2018).
Social Ties and Health in Real Time
The vast majority of sociological studies in this area rely on overall summary measures of both social connectedness and health. These measures are typically collected through the administration of survey items capturing the experience or diagnosis of specific conditions (e.g., depression, diabetes), subjective health assessments, biomarkers, tests of mobility, cognition, and other anthropomorphic measures to draw inferences about an individual’s overall condition or a particular dimension of health risk (Pierannunzi, Hu, and Balluz 2013). Although the contributions of this research should not be understated, our focus in this article is on understanding the social context of real-time, or momentary, assessments of well-being, that is, how an individual feels (physically or mentally) at a given moment in time (Chaix 2020; Shiffman et al. 2008). We focus on symptoms of physiological distress, including pain, fatigue, and stress as they are experienced in real time, and shifts in these symptoms over the course of five daily reports collected throughout three one-week observation periods.
Why do real-time symptoms matter? Momentary health assessments can reveal physiological states that contribute to longer-term disease processes (Cohen et al. 2007; Weber et al. 2022) and mental health conditions (Charles et al. 2013). For example, the stress process conceptualizes how momentary psychological and subsequent physiological responses to encounters in the social world can contribute over time to underlying conditions such as cardiovascular disease. Exposure to acute stressors is directly associated with physiological responses such as elevated blood pressure and heart rate (Weber et al. 2022), while repeated or chronic activation of the stress response can cause wear and tear on the body’s physiological capacity to regulate and lead to heightened levels of inflammation and allostatic load (McEwen 1998; McEwen and McEwen 2017). Importantly, physiological symptoms associated with the stress response have also been linked to experiences of pain and fatigue (Hannibal and Bishop 2014; Hoeger Bement et al. 2010).
Whereas momentary symptoms are important given their link to longer-term conditions, they are also consequential in and of themselves, and in ways that may not be reflected in conventional summary measures of well-being. Moment-in-time experiences of pain and fatigue could limit an individual’s ability or willingness to pursue a particular activity, which could constrain participation in potentially health-enhancing social engagement. Likewise, fluctuations in these symptoms throughout the day could carry implications for accessing social and other resources, for example, whether one feels well enough to run an errand, attend religious services or a group activity, or provide some type of instrumental or emotional support to a friend or family member. Indeed, recent evidence suggests that physical copresence with a romantic partner is associated with lower levels of C-reactive protein the following day (Jolink et al. 2023). Global health measures are arguably less sensitive to these momentary fluctuations, as they typically assess an individual’s well-being “on average,” or at one particular moment (e.g., a single blood pressure reading as part of a survey), missing more micro-level yet significant changes.
Social Integration and Social Accompaniment
The pathways through which real-time health fluctuations relate to overall well-being also suggest that social ties carry real-time relevance. In other words, momentary health symptoms may be a function of real-time social accompaniment (e.g., Bernstein et al. 2018). Our definition of social accompaniment, which refers to whether someone is physically present with a social tie at a given moment, recognizes that this social experience can fluctuate throughout short periods, even within a given day. For example, an individual who is grocery shopping with their spouse in the morning would be experiencing social accompaniment during that activity, but would not experience social accompaniment while they are working alone in their office later in that same day. We emphasize that our conceptualization of momentary social accompaniment is limited to scenarios in which an individual is physically copresent with a familiar other (e.g., a friend or family member) with some level of intentionality. The mere presence of other people, for example in a crowded bus or a busy grocery store, is not considered to be social accompaniment. Furthermore, someone who is alone but talking on the phone while shopping is not experiencing social accompaniment, although they could be experiencing real-time social support via the phone call. We consider that social accompaniment may provide better instrumental support, anticipation of needs, and stress buffering than interacting on the phone or other virtual means.
How is social accompaniment relevant for real-time health? For one, the sharing of information, advice, and experiences is likely to take place when people spend time together. Such exchange can also take place virtually, however in-person social accompaniment may offer more fluid exchange around topics that may not come up over a phone call, for example pointing out something in the immediate social environment or having extended time together. Perhaps most indicative of the fact that in-person social accompaniment meaningfully differs from virtual social connection is the accumulating research on adverse mental health outcomes stemming from physical social distancing in the context of the coronavirus disease 2019 pandemic (e.g., Galea, Merchant, and Lurie 2020).
Other mechanisms are more specifically tied to in-person accompaniment. Being in the same physical space as someone else makes the provision of tangible support more feasible, particularly as it relates to caregiving, disability, or acute illness or injury. For older adults who experience mobility challenges, for example, a friend or family member can point out potential hazards in the physical environment, help them navigate stairs and walkways, and carry heavy items. Put simply, social accompaniment offers the potential to ease physical burdens involved in one’s day-to-day activities. Other work suggests that physical copresence allows physiological benefits of affectionate touch, for example, that also benefits health (Jolink et al. 2023)
Social accompaniment can also be an important source of emotional support, buffering against psychological stressors at a given point in time. For example, stress that comes from someone’s job or an upsetting interpersonal interaction might be alleviated through in-person discussion with social ties during or immediately after the precipitating event. In this regard, social accompaniment can have significant implications for stress appraisal, self-esteem, mood, and feelings of self-efficacy in response to triggers experienced throughout the day (Uchino, Uno, and Holt-Lunstad 1999), and in ways that summary measures of social support or social integration are less well suited to capture. The state of being alone can also induce feelings of loneliness (Compernolle et al. 2021) or perceptions of being socially isolated, which may contribute to distress and depression (Hawkley and Cacioppo 2010; Holt-Lunstad 2018), while interacting with others is associated with higher reports of momentary happiness (Bernstein et al. 2018; Kashdan and Collins 2010). Indeed, being in the company of someone else may reduce boredom, or otherwise serve as a distraction from unpleasant symptoms.
Importantly, the health consequences of social accompaniment may differ on the basis of with whom an individual is interacting. Social ties can at times be a source of stress, particularly interactions with family members and partners (Ng et al. 2021; Offer 2020). At the same time, interactions with nonkin (i.e., friends) can be important sources of companionship and social support that is less overlapping and more voluntary than that provided by kin, and in ways that can shape survival and mortality (Carstensen 1992; Ellwardt, Aartsen, and van Tilburg 2017). Indeed, daily encounters with friends in particular, more so than with family and partners, are associated with more pleasantness, which may reflect greater novelty or diversity of social experiences that are more typical of nonkin encounters compared with more routine, habitual activities done with family (Fingerman et al. 2020; Ng et al. 2021).
Finally, social accompaniment may also be associated with real-time symptoms indirectly, as a result of the context or activities associated with spending time with someone else. Engagement in leisure activity has been associated with better mood, less stress, and lower heart rate (Zawadzki, Smyth, and Costigan 2015), and positive social interactions and evaluations of social interaction quality are associated with positive affect (Bernstein et al. 2018; Liu, Xie, and Lou 2019).
We distinguish social accompaniment from overall summary measures of social integration that are traditionally used in social science surveys. For instance, population-based surveys such as the General Social Survey administer personal (egocentric) network name generators that ask respondents to provide information about the individuals with whom they have spoken over a particular period (e.g., the last 6 months). This information is used to create summary measures of respondents’ confidant network characteristics (e.g., size, frequency of interaction), which serve as indicators of individuals’ social integration. Other widely-used survey questions prompt respondents to report on how much social support they feel that they have, the number of close friends or relatives, and social engagement such as religious service attendance and involvement in organized group activities. Common to each of these measures is that they implicitly ask respondents to reflect on their overall, or average, social experiences.
A core argument of this study is that the degree to which an individual is socially connected overall does not necessarily align with how often they experience social accompaniment throughout their day. For example, someone who has a relatively large number of friends or a larger social network may live geographically distant from those individuals, or spend most of their day physically alone or with only a few others. Although they may enjoy health benefits from perceiving themselves to have numerous sources of social support, their health may also suffer from having fewer close social ties to exchange in-person, tangible support or provide more immediate advice or assistance. Likewise, an individual who would be considered socially isolated through traditional measures (e.g., few close friends or family members) may spend much of their day accompanied by others at work, during caretaking, or in social activities.
Prior studies reveal associations between momentary social interactions and momentary experiences of physical symptoms such as fatigue and pain (Bernstein et al. 2018). We focus in particular on whether these linkages exist above and beyond global measures of social integration and overall health, inserting a deeper consideration of individuals’ natural environment in more traditionally used sociological frameworks for studying interpersonal determinants of health (Berkman et al. 2000). We consider that having few sources of overall social connection or a lack of close companionship may introduce some health risks but that other aspects of health may benefit from regularly being in the physical company of others, independent of an individual’s general portrait of social connectivity. In this way, momentary social accompaniment may even contribute to health in ways that exist apart from more widely studied pathways between global social integration and health.
The Present Study
The primary goal of this study is to examine how momentary social accompaniment is associated with real-time fluctuations in physiological symptoms. A key contribution is our examination of whether any relationship between these momentary measures is explained by more traditional summary measures of both social connectedness and well-being. We rely on data collected through smartphone-based EMAs, which provide snapshots of social processes and activities across different settings and moments of the day (Shiffman et al. 2008). EMA is an ideal methodological approach for collecting data in “real-world environments, as subjects go about their lives” (Shiffman et al. 2008), also referred to as an “ecological” approach. EMA questions typically assess a respondent’s current state, asking them to self-report on their real-time affect, behavior, and experience, and the conditions of their current location (Stone and Shiffman 1994). By collecting multiple EMAs from individual respondents over a day or several days, this repeated assessment allows researchers to characterize how individual experiences change over short time frames and across contexts. Smartphone-based EMA collection that “pings” respondents throughout the day to ask them to respond to a set of questions using the phone can also help avoid issues of recall bias that plague traditional retrospective survey measures that ask people to assess some aspect of their everyday life (Chaix 2020; Shiffman et al. 2008).
EMAs and the Older Adult Population
The EMA approach has been widely implemented in psychology and clinical fields to assess health, affective, and behavioral processes that can fluctuate over short time frames and that are shaped by everyday experiences and exposures (Shiffman et al. 2008; Stone and Shiffman 1994), but it has been less widely adopted in sociological studies. Later life is often characterized by age-related declines in well-being and shifts in patterns of social engagement, social relationships, and everyday routines (Alwin, Felmlee, and Kreager 2018), making the EMA approach particularly well suited for better understanding intersections between the social context and health among the older adult population. Indeed, a focus on older adults’ everyday activities, patterns of behavior, and social engagement can deepen our understanding of the aging process and potential areas for intervention within the framework of daily living.
Some large-scale social surveys have included time diary components, such as the National Study of Caregiving and the National Study of Daily Experiences, which administer phone interviews to ask about respondents’ daily activities, affect, stress, and well-being (Han, Kim, and Burr 2020; Moon and Dilworth-Anderson 2015). Smartphone-based EMA approaches have been successfully implemented to collect repeated measures of real-time data from older adults, such as in the Daily Experiences and Well-Being Study (e.g., Fingerman et al. 2020; Ng et al. 2021) and numerous other community-based samples (e.g., Fang et al. 2022; Zhaoyang et al. 2022). These studies have generated new insights about the intersection of global and momentary measures of social life, underscoring the notion that the health implications of global and momentary aspects of social connectedness may be interrelated. For example, recent findings indicate that global social support moderates the effects of momentary solitude on negative affect (Fang et al. 2022), as do higher quality social relationships (Pauly et al. 2018). However, other work using the CHART data shows that older adults who have larger social networks report higher levels of momentary loneliness when alone compared with individuals with smaller social networks (Goldman and Compernolle 2023). Collectively, these studies highlight the advantage of the EMA approach for assessing how older adults’ health is shaped by social life across different contexts and time scales (Smyth et al. 2017).
An older adult sample introduces questions about sample generalizability and selection, which is characteristic of research focusing on the later part of the life course. Earlier experiences and exposures in older adults’ lives, such as childhood adversity, that are unmeasured in our study may contribute to both older adults’ health and patterns in social accompaniment (e.g., Andersson 2018; Haas 2007; Hayward and Gorman 2004). Survival bias draws attention to the fact that an older adult sample necessarily is limited to respondents who survived to ages 65 and older, and who may have therefore experienced greater advantages (health and otherwise). We return to these and other limitations later in the manuscript, but note for now that these considerations imply that our findings may be somewhat conservative to the extent that we draw on a particularly healthy sample of older adults.
Data and Methods
The CHART study is a neighborhood probability sample of 455 community-residing Chicagoans aged 65 and older, with the goal of better understanding how different dimensions of older adults’ social context shape health trajectories. Respondents were selected via population-based sampling from 10 Chicago neighborhoods that were chosen to represent a range of racial/ethnic and socioeconomic backgrounds across the city’s residential areas.
The CHART data are especially well suited for this study because it collects repeated measures of older adults’ momentary symptoms and social accompaniment, in addition to several global measures of respondents’ health and social integration that are often included in larger scale social surveys of health and social context (e.g., the Health and Retirement Survey). The CHART sample was invited to participate in three waves of data collection across 2018 and 2019, with each wave conducted five to six months apart. In-person baseline interviews conducted at the start of each wave collected information about respondents’ sociodemographic characteristics, overall health, and aspects of their social lives. Each baseline survey was followed by one week of Global Positioning System tracking and EMA collection via smartphones (Samsung Galaxy S7).
EMAs were administered five times per day during each of the three seven-day data collection periods by “pinging” respondents using the smartphone at random times during each of the five daily windows: 8 to 10 a.m., 10:30 a.m. to 12:30 p.m., 1 to 3 p.m., 3:30 to 5:30 p.m., and 6 to 8 p.m. These five windows aimed to capture a representative sample of the indoor and outdoor, and private and public spaces where respondents spend their time. EMAs included questions to assess respondents’ perceptions of the physical characteristics of their locations, their experiences of physical symptoms, and their mental and emotional well-being. Figure 1 illustrates the collection of EMAs across respondents’ various daily contexts, including at their homes (orange) and other locations (green).

Map of Chicago illustrating the collection of ecological momentary assessment (EMA) observations from respondents across daily activity locations. Orange dots represent EMAs collected at respondents’ homes, and green dots represent EMAs collected outside of respondents’ homes.
Real-Time Pain, Fatigue, and Stress
To assess whether momentary experiences of physiological symptoms are shaped by real-time social accompaniment, we examine variations in respondents’ real-time experiences of pain, fatigue, and stress. As part of each EMA, respondents were prompted to “think about how you felt at the time you were pinged” and were then asked “Did you feel pain?” “Did you feel tired?” and “Did you feel stressed?” For each outcome, response options included “very,” “moderately,” “slightly,” and “not at all.” Given that few EMA reports indicated the highest levels of these symptoms (<2 percent “very” for pain and stress, <4 percent “very” for fatigue), we dichotomize each of these three measures so that 1 = “very” or “moderately” and 0 = “slightly” or “not at all.” Results are consistent when using continuous measures.
Social Accompaniment
As part of each EMA, respondents were asked, “At the time of the ping, who were you with?” Respondents were asked to select “all that apply” from the following categories: “nobody,” “spouse or romantic partner,” “family member,” “friend,” “neighbor,” “pet,” “other,” or “don’t know.” We code any respondent who only selected “nobody” as being alone when the EMA was administered. Responses of “don’t know” were coded as missing. Anyone who selected any combination of the other categories was coded as having experienced social accompaniment at the time of the EMA ( = 1). 1 Because we expect that social accompaniment may have different consequences for real-time health depending on who a respondent is with and associated social roles, we further disaggregate instances of social accompaniment by creating three variables to capture whether the respondent was with (1) a spouse or romantic partner or a family member (“partner or family member”), (2) a friend or neighbor, and (3) another social partner (“other”) (1 = yes for each variable).
In a second set of analyses, we consider whether the type of activity that an older adult is engaged in during a given EMA is relevant to any relationship between social accompaniment and momentary symptoms. At each EMA, respondents were asked to indicate whether they were participating in any of 16 different activities. Respondents could select multiple activities. We create two dichotomous variables to indicate, separately, (1) whether the respondent was engaging in a recreational or social activity and (2) whether the respondent was engaging in an obligatory activity. We consider that recreational activities represent real-time measures of widely used global measures of social integration, such as religious service attendance and organized group activities. These forms of social engagement could also yield momentary health benefits through diversion, access to peripheral social ties and novel information and advice, and fostering a sense of belonging (e.g., Ellwardt et al. 2017; Fingerman 2009). A respondent is coded as engaging in a recreational activity if they indicate relaxing, exercising or playing sports, socializing, religious participation, nonreligious group or club participation, or volunteering. Obligatory activities are coded as involving personal care, napping or sleeping, household tasks, caring for someone else, paid work, or receiving health care. 2
Covariates
Our models adjust for respondent age, gender, self-reported race/ethnicity (White, Black, Hispanic, or another race/ethnicity), educational attainment (less than high school, high school or equivalent, some college, bachelor’s degree or more) reported at wave 1. We include a fixed effect for respondents’ residential neighborhood. We also account for several global summary measures from the wave 1 baseline survey to capture respondents’ social integration and overall health, which may shape both opportunities for momentary social accompaniment and real-time symptoms. Baseline health measures include self-rated physical health (1 = “good,” “very good,” or “excellent”; 0 = “fair” or “poor”) and whether they currently smoke. Respondents rated how much difficulty they had completing six activities of daily living (e.g., walking across the room, getting dressed), where 1 = “no difficulty” and 4 = “unable to do.” We average these items to create a scale of functional impairment (α = .86).
Global social measures include whether the respondent lives alone, has lived in their neighborhood for at least 20 years, and is currently working, each of which could shape the likelihood of being in the presence of others at a given moment of the day. We also account for how frequently respondents report attending any organized group activities and, separately, religious services (0 = “never,” 1 = “sometimes” [between “once or twice in the last 6 months” to “about once a month”], 2 = “often” [“every week” or “several times a week”]). Finally, we control for personal network size, which was collected at baseline through the administration of the “important matters” name generator (Marsden 1987). Respondents could name up to five individuals with whom they discussed “important matters” over the prior six months. Network size is the sum of named individuals. Average network interaction is calculated as the average frequency at which respondents report interacting with their network members (range: 1 = “daily” to 6 = “not at all”). We reverse-code this scale so that higher values represent more frequent interaction, on average, with network members.
We also account for variables that were collected about respondents’ real-time social context as part of the EMAs, including whether the respondent reported being at home and whether they were outdoors, each of which may be associated with both momentary social accompaniment and momentary symptoms. As symptoms, especially fatigue, are also likely to have diurnal rhythms, we adjust for which of the five daily windows the EMA was administered as a proxy for the time of day. 3
Analytic Strategy
Our analyses draw on EMA data from waves 1, 2, and 3 of the CHART study to maximize the number of EMA observations and to capture potential variations in real-time measures by season or time of year. We first examine descriptive statistics of our key measures. We then consider bivariate distributions of between-person momentary social accompaniment by levels of global social integration measures to shed some light on how strongly global and momentary assessments of social measures correlate with one another.
In the second stage of the analysis, we examine two sets of multilevel multivariable logistic regression models. Our multilevel models are structured so that EMA observations (level 1) are nested within individual respondents (level 2). At level 1, we estimate within-person effects of momentary social accompaniment, as well as other key EMA covariates including being at home, being outdoors, and recreational and obligatory activity engagement. Within-person effects allow us to examine whether momentary symptoms are more or less likely when a given individual is with someone compared with when they are alone. At level 2, between-person social accompaniment allows us to examine whether older adults who are more often in the company of others during the study period, on average, are more or less likely to experience momentary symptoms compared with older adults who are less frequently in the company of others, on average. We person-mean-center the EMA measures to examine within-person effects of the real-time social context on momentary symptoms. We derive between-person measures of these same variables that represent the deviation of person-means from the sample mean. (Bolger and Laurenceau 2013).
Our first set of models examines whether momentary experiences of higher levels of real-time pain, fatigue, and stress are a function of within-person social accompaniment, adjusting for between-person measures and the full set of covariates. The second set of models adds covariates for recreational and obligatory activity engagement to assess the role of real-time social engagement versus more routine activity in shaping momentary symptoms. All models adjust for the time ordering of the EMA observations and include a fixed effect for survey wave (1, 2, or 3). Analyses are conducted using Stata 14.
Analytic Sample
Of the 455 respondents in the CHART study, we excluded 72 who completed the baseline survey but who did not participate in the EMA portion of the study. Of the remaining 383 respondents, 41 were excluded from our analysis because of missing data on one or more of the social, health, and sociodemographic variables taken from the baseline survey. On average, respondents in our sample contributed 37 EMAs across the three waves. Our final analytic sample relied on 12,760 EMA observations that were collected from 342 respondents. Compared with respondents who were excluded because of missing data, those in our analytic sample did not differ significantly by frequency of interaction with network members, network size, attendance at organized events or religious services, functional health, or self-rated physical health.
Results
Descriptive Results
Table 1 includes descriptive statistics for the main variables used in our analyses. As shown in the top panel, respondents reported feeling fatigue, pain, or stress between “moderately” or “very” across 18 percent, 13 percent, and 7 percent of all EMAs in the analytic sample, respectively. In 53 percent of the EMA observations, respondents reported being with someone. Respondents reported being with family or a partner during 37 percent of the EMAs, with a friend or neighbor during 10 percent of the EMAs, and with someone else in 4 percent of EMAs. In 46 percent of EMAs, respondents reported engaging in some form of recreational or social activity, with 44 percent of EMAs surveying respondents during engagement in obligatory activities. The majority of EMAs (74 percent) were completed when respondents were at home, and 85 percent were completed when respondents were indoors. EMA responses were relatively evenly distributed across the daily windows.
Descriptive Statistics of Main Variables Used in the Analyses.

Note: EMA = ecological momentary assessment.
Proportions for EMA-level variables are calculated across all EMAs in the analytic sample.
Categories are not mutually exclusive. Respondents could report being with multiple types of social ties and being engaged in multiple types of activities. Certain activities were ambiguous with respect to whether they were recreational or obligatory in the absence of additional contextual details, and so they were not coded as either recreational or obligatory.
Respondent-level variables are taken from the wave 1 baseline survey.
The lower panel of Table 1 provides respondent characteristics. Just over one quarter of respondents are White (26 percent), 49 percent are Black, 23 percent are Hispanic, and 3 percent identify as members of other racial/ethnic groups. On average, respondents are approximately 74 years old. With respect to global measures of social integration, CHART respondents report having, on average, three personal network members (the maximum is five), with whom they interact between “a few times a week” and “daily,” on average. Approximately 58 percent of respondents attend organized group activities and 72 percent attend religious services with some degree of frequency (between “once or twice in the last 6 months” and “several times a week.”) The majority (73 percent) have lived in their residential neighborhoods for at least 20 years. Approximately 42 percent of respondents live alone and 20 percent are employed at the baseline survey. Most respondents (71 percent) report good, very good, or excellent self-rated physical health and low levels of functional impairment (M = 1.14).
We next examine how real-time social accompaniment is patterned by global or summary measures of social integration. In other words, are people who are generally more socially integrated more likely to be with someone else at a given moment of their day? Figure 2 illustrates the average proportion of EMAs (person-level means) across all three waves of the study period during which respondents reported social accompaniment (i.e., being with someone else), by levels of global social integration. Older adults who lived alone experienced social accompaniment during 37 percent of the EMAs, significantly less than the 65 percent of EMAs during which older adults who live with others reported social accompaniment. However, there is little variation in reports of social accompaniment by network size. Those with a network size of one reported being with someone during 53 percent of the EMAs, compared with 55 percent of the EMAs among respondents who reported a network size of five.

The average proportion of ecological momentary assessments in which older adults reported experiencing any type of social accompaniment (person-means), by levels of overall (global) social integration.
Rates of social accompaniment in the EMAs are significantly lower among respondents who reported the lowest frequency of interaction with network members (45 percent), compared with those who reported moderate and high levels of network interaction (58 percent and 59 percent, respectively). But the correlation between the frequency of interaction with network members and the proportion of EMAs during which respondents report social accompaniment is low (r = .19). Differences in rates of social accompaniment are not clearly associated with participation in social or religious groups. Older adults who reported the most frequent levels of religious service attendance reported similar levels of social accompaniment (52 percent) as those who never attend (53 percent). And we find no significant differences in rates of social accompaniment across frequencies of participation in organized group activities.
Multivariable Results
Next, we consider whether real-time health symptoms are a function of social accompaniment when accounting for EMA and respondent-level controls. Before adding covariates, we ran an unconditional model for each of our three outcomes (not shown) to assess how much of the total variation in each momentary symptom is due to average differences between subjects. Intraclass correlations indicate that approximately 41 percent, 71 percent, and 51 percent of the variance in fatigue, pain, and stress, respectively, is due to mean differences between respondents.
Turning to Table 2, we begin by examining within-person effects, as momentary social accompaniment is our primary predictor of interest (models 1 through 3). Being with a friend or neighbor is associated with significantly lower log odds of experiencing momentary fatigue (p < .01) and stress (p < .01) compared with when an individual is not with friends or neighbors, but this form of social accompaniment is not associated with momentary reports of pain. We do not observe statistically significant associations between being with a partner or family member or being with another type of social tie and momentary symptoms. Being at home is also associated with significantly lower log odds of experiencing momentary stress compared with when an individual is elsewhere (p < .05). A significant association also emerges between the approximate time of day and fatigue and stress, with reports of both symptoms increasing later in the day compared with the morning window (8–10 a.m.).
Log Odds from Multilevel Logistic Regression Models Predicting Experiences of High Levels of Momentary Fatigue, Pain, and Stress.

Note: Values in parentheses are standard errors. All models control for whether EMA observations were drawn from wave 1, 2, or 3, as well as the time ordering of each EMA observation. Models 4, 5, and 6 also include a control for respondent residential neighborhood. EMA = ecological momentary assessment.
p < .05, **p < .01, and ***p < .001 (two-sided tests).
These associations also emerge in models that account for between-person effects, global measures of social integration, and respondent sociodemographic characteristics (Table 2, models 4–6). Being with a friend or neighbor is associated with significantly lower log odds of momentary fatigue (p < .001) and significantly lower log odds of momentary stress (p < .01) compared with times when not with a friend or neighbor. Being at home is also associated with lower log odds of momentary stress compared with being elsewhere (p < .05). Momentary fatigue and stress levels are significantly higher in reports later in the day compared with earlier in the day (morning).
Global measures of social integration appear to be less relevant for real-time symptoms; that is, people who have larger networks are no more or less likely to report momentary pain, fatigue, or stress during their days. Furthermore, we find no significant associations between frequency of interaction with network members, living alone, or religious service or organized group attendance with any of the three momentary symptoms. Older adults who rated their overall physical health as good, very good, or excellent had significantly lower log odds of reporting higher levels of momentary pain (p < .05) and stress (p < .001). Higher levels of functional impairment were associated with significantly higher log odds of experiencing momentary pain (p < .05), whereas smoking status was not associated with experiences of any of the three symptoms.
Results from logistic regression models can also be interpreted in terms of marginal effects (Mood 2010). Figure 3 illustrates the predicted probability that respondents reported higher levels of momentary fatigue, pain, and stress by type of social accompaniment. Older adults who experienced social accompaniment with friends or neighbors at a particular moment of their day had an approximate likelihood of .147 in reporting high levels of fatigue, which was .038 (p < .001) less than the likelihood among older adults who were not in the company of a friend or neighbor at a given moment of their day. Likewise, older adults who were with a friend or neighbor had a likelihood of .051 in reporting high stress, which was .021 (p < .01) less than the likelihood of older adults who were not with a friend or neighbor at a given moment. Levels of predicted symptoms are similar across respondents when they are with or without a partner or family member or another type of tie.

Predicted probabilities of experiencing momentary fatigue, pain, and stress, by type of momentary social accompaniment, based on models 4, 5, and 6 in Table 2.
Although these differences are relatively small, the EMAs were collected across short periods, sometimes within hours of each other. To better understand the relevance of social accompaniment for momentary symptoms, it can be useful to compare the magnitude of effects in terms of the difference in predicted probabilities with those of other covariates in the full models in Table 2. The predicted difference in the likelihood of reporting high levels of momentary fatigue by whether an individual is with a friend or neighbor (.038) is approximately half of the difference in the likelihood of momentary fatigue in the earliest EMA window of the day (.146) compared with the latest window of the day (.224), and it is approximately equal to the difference in the likelihood of experiencing high momentary fatigue among individuals who reported poor or fair self-rated health (.209) and those who reported good, very good, or excellent self-rated health (.174). Differences in reporting stress according to social accompaniment are more modest. However, the difference in the likelihood of reporting high levels of stress earliest in the day (.054) compared with the latest in the day (.083) is just .009 larger than the difference predicted by being with a friend or neighbor (.020). Respondents who reported good, very good, or excellent self-rated health were .063 less likely to report high levels of momentary stress compared with those who reported worse health, a difference of approximately three times that predicted by social accompaniment with a friend or neighbor.
Finally, the models in Table 3 control for the type of activity to discern whether the association between social accompaniment (by a friend or neighbor) and real-time fatigue and stress may be due in part to the types of activities that individuals do when they are with a friend or neighbor. Model 1 indicates that being with a friend or neighbor is associated with significantly lower log odds of momentary fatigue, even when adjusting for the type of activity. However, after accounting for activities, the predicted difference in experiencing fatigue on the basis of whether one is with a friend or neighbor is reduced from .038 (p < .001, based on model 4 in Table 2) to .023 (p < .05). Engagement in a recreational activity is associated with significantly lower log odds (p < .001) of momentary fatigue and engagement in an obligatory activity is associated with significantly higher log odds (p < .001) of fatigue.
Log Odds from Multilevel Logistic Regression Models Predicting Experiences of High Levels of Momentary Fatigue, Pain, and Stress, Accounting for Type of Activity.
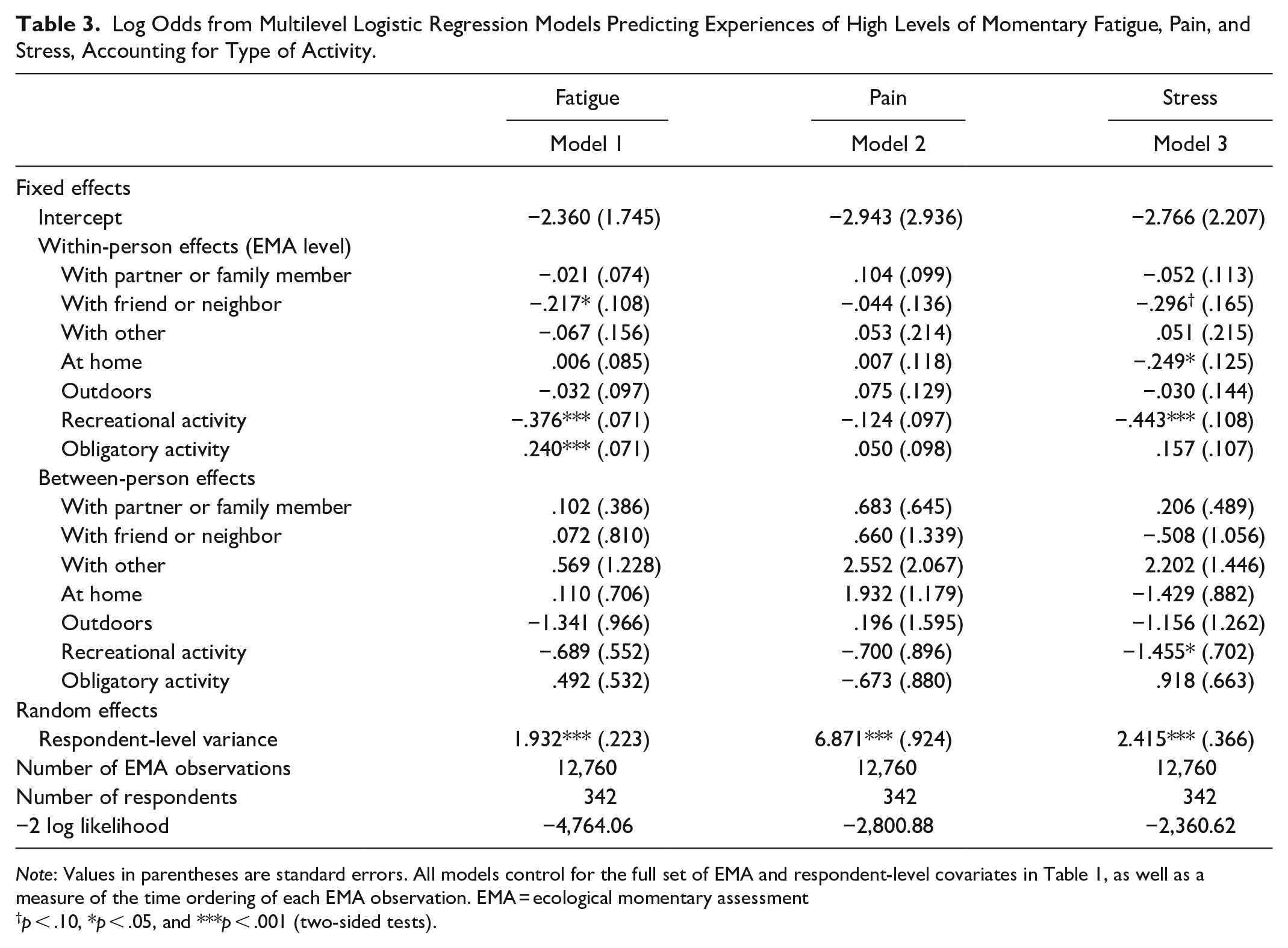
Note: Values in parentheses are standard errors. All models control for the full set of EMA and respondent-level covariates in Table 1, as well as a measure of the time ordering of each EMA observation. EMA = ecological momentary assessment
p < .10, *p < .05, and ***p < .001 (two-sided tests).
Consistent with the findings in Table 2, the second model in Table 3 suggests that momentary pain is neither a function of social accompaniment nor activity. Model 3, however, indicates that when adjusting for the type of activity, the significance of being with a friend or neighbor is marginal. The predicted difference in experiencing real-time stress based on whether one is with a friend or neighbor is reduced from .020 (p < .05, based on model 6 in Table 2) to .014 (p = .056). Real-time engagement in a recreational activity is also associated with significantly lower log odds of momentary stress (p < .001). The statistical significance of being at home is robust to the adjustment for activity type (p < .05). In supplemental models, we interacted being with a friend or neighbor with engagement in a recreational activity at both levels. These interaction terms were not statistically significant.
Discussion
Three main findings emerge from this study. First, our findings suggest that traditional summary measures of social integration overlook variation in the availability of in-person social accompaniment on a day-to-day basis. Summary measures of social integration provide a bird’s-eye view of an individual’s social world—for example, how many close friends and family they have, whether they have someone to call on if needed—even if those ties are not often activated. Momentary social accompaniment is patterned by living arrangements and (to some extent) the frequency of interaction with network measures, but it does not appear to vary significantly according to other measures of social participation, including religious service and organized group attendance. Of particular importance, we found that people with large personal networks spent just about as much time with someone else, on average, as those with small personal networks. These results raise questions about what other social-structural processes contribute to patterns of momentary social accompaniment, separate from more traditional summary measures of social integration.
Second, when people are with friends or neighbors, they seem to feel better. Real-time social accompaniment with friends or neighbors is significantly associated with lower levels of momentary fatigue and stress, even after adjusting for widely used summary measures of physical health and social integration. Other types of social accompaniment (i.e., family or partner, another social tie) were not significantly associated with momentary symptoms. These findings draw attention to the importance of nonkin ties for older adults’ momentary well-being (Fiori, Windsor, and Huxhold 2020; Huxhold, Miche, and Schüz 2014; Litwin and Shiovitz-Ezra 2011; Mair 2019), in ways that may be consequential for longer-term health problems. Indeed, repeated activation of the stress response can contribute to chronic health conditions (McEwen 1998; Schneiderman, Ironson, and Siegel 2005). Being with friends or neighbors may protect individuals from momentary stress experiences. Momentary experiences of fatigue or stress could also lead individuals to withdraw from or avoid other forms of social engagement in ways that contribute to longer-term health issues. Our findings are also consistent with emerging evidence that shorter-term fluctuations in physical copresence may be one way in which social isolation, on a momentary basis, ultimately affects health (Bernstein et al. 2018; Jolink et al. 2023; Ng et al. 2021). Third, although recreational activity is associated with lower levels of momentary stress and fatigue, being with a friend or neighbor is still associated with significantly less momentary fatigue (and with marginally less stress) after accounting for the type of activity in which they are taking part.
Why might nonkin (friend or neighbor) social accompaniment be associated with better momentary well-being? Whereas instrumental support exchange is typically prominent among kin ties, friendships in later life are more voluntary, more effective in preventing loneliness, and are characterized by a sense of mutual concern and companionship that can increase one’s sense of self-worth and self-control in ways that may uniquely benefit health (Ellwardt et al. 2017; Huxhold et al. 2014; Miche, Huxhold, and Stevens 2013). Our findings could reflect differences in how older adults tend to spend time with kin and nonkin in a real-time framework, and how the activities and conditions of their interactions allow individuals to feel better when they are in the company of friends and neighbors. In supplemental analyses at the EMA level, we found that respondents reported engaging in a recreational activity 70 percent of the time when they were with a friend or neighbor, compared with just 52 percent of the time when they were in the company of a partner or family member. At the same time, respondents reported engaging in obligatory activities in 30 percent of EMAs when with friends or neighbors compared with 43 percent of EMAs when with a family member or partner. Thus, it could be that social accompaniment with friends or neighbors is associated with lower levels of momentary fatigue and stress because of greater diversion, sense of social engagement, or enjoyment brought about by the types of activities that older adults typically do with their friends and neighbors. Obligatory activities such as caregiving and housekeeping, which are more often conducted with kin, may evoke greater stress, strain, or conflict that could contribute to momentary fatigue.
These differences may also reflect broader structural and functional differences between nonkin and kin social ties. Kin ties tend to be frequently accessed sources of social support who are often socially connected to other kin and are more likely to coreside with an older adult than nonkin ties. Nonkin ties may interact less frequently, represent more peripheral relationships, and allow for access to distinct social contexts and novel sources of information and support (Charles and Carstensen 2010; Ellwardt et al. 2017; Feld 1981; Fingerman 2009; Wellman and Wortley 1990). Being with friends or neighbors may therefore be more engaging and stimulating social interaction if this social accompaniment includes catching up with someone, or exchanging personal news, opinions, or advice that is more novel and unique relative to information exchanged with more frequently accessed kin ties. Indeed, other research using the EMA approach demonstrates that social interactions with friends include the discussion of less stressful topics of conversation (Ng et al. 2021). Social encounters with more peripheral social ties throughout the day are associated with greater physical activity (Fingerman et al. 2020), which may also explain why we find that being with friends or neighbors is associated with less fatigue and less stress in ways that are partially explained by recreational activity.
Interestingly, social accompaniment was not significantly associated with momentary pain in our models. This result is not entirely surprising given that unconditional models suggest that most variance in momentary pain is between subjects. Indeed, worse overall self-rated physical health and functional limitations were associated with significantly higher levels of momentary pain, suggesting that fluctuations in pain may be largely a function of person-level differences in chronic conditions or general physical well-being.
Limitations
Smartphone-based EMA collection is generally advantageous to paper-based or other retrospective measures of daily experiences (Shiffman et al. 2008). However, EMA results may suffer from selection bias. We do not find evidence that EMA response rates or delays in response time were patterned by person-level social accompaniment, but it is still possible that when respondents are experiencing higher levels of pain, fatigue, or stress, they are less likely to complete the EMAs and also less likely to spend time with others. Momentary social accompaniment may also distract a respondent from turning their attention from in-person conversation or an engaging activity to respond to the EMA. If this is the case, we might consider that our results are conservative estimates. Indeed, our findings indicate that respondents feel better when with friends and neighbors and engaging in recreational activities. To the extent that the same momentary social circumstances that predict better health also predict nonresponse, we may find stronger associations if respondents who did not respond to a “ping” because of real-time social engagement had responded. Additional research is needed to better understand the social and health contexts of EMA nonresponse.
Our sample is also limited to respondents who agreed to the EMA collection, were willing to carry the phone, and were comfortable enough using the phone to respond to the EMA “pings.” Although all respondents received in-person training on how to use the phone, approximately 16 percent of CHART respondents did not complete any EMAs. It is possible that our study would yield different results if data on momentary social accompaniment and health were collected from a broader sample of older adults who may be less comfortable using smartphones.
Future research should consider whether these associations between social accompaniment and momentary symptoms vary across social groups. For example, differences in everyday lived experiences that are tied to race/ethnicity such as experienced or expected discriminatory interactions (Hicken, Lee, and Hing 2018) may differentially shape the health benefits of social accompaniment across racial/ethnic groups. Likewise, older adults’ socioeconomic status may render certain forms of social accompaniment especially critical for exchanging instrumental social supports that could significantly influence momentary symptoms such as stress. Although our emphasis is on physical copresence, future work should also consider the momentary health consequences of other forms of real-time social integration that do not take place in person (e.g., talking on the phone, text messaging).
Finally, we cannot rule out the possibility that other confounding variables explain our findings. Potential confounders could include other contextual details that characterize instances of social accompaniment, such as the degree of active or passive engagement during social accompaniment (Rinderknecht, Doan, and Sayer 2021), as well as the perceived quality of social interactions and closeness of the social relationship, which can also shape physical symptoms (Bernstein et al. 2018; Fingerman et al. 2020; Zhaoyang et al. 2019). Neighborhood context and social environments may also structure opportunities to interact with kin and nonkin, and differences in these conditions may also contribute to differences in stress (York Cornwell and Goldman 2020). Personality traits, too, may play a role in patterns of social accompaniment and social engagement (Zhaoyang et al. 2022). It is also still possible that for some respondents the observation periods in the CHART study were particularly socially active or withdrawn periods, or periods of poorer health (e.g., acute illness or injury, conflict with a friend), and do not represent typical or “average” patterns of social accompaniment or symptoms.
Conclusion
Our findings suggest that variations in everyday social accompaniment have important implications for health and well-being (Jolink et al. 2023). The unique value of being with a friend or neighbor is consistent with other research pointing to the growing importance of older adults’ nonkin ties (e.g., Mair 2019; Margolis and Verdery 2017) and local ties (York Cornwell and Goldman 2021). Future research should consider how being with particular types of ties on a momentary basis may confer certain health benefits or risks due to characteristics of the dyad such as role obligations, social exchanges, and closeness, and how these associations are conditioned by aspects of the broader social context.
Global indicators of social integration are meaningful measures of individuals’ overall access to social resources and support, which have profound consequences for global indicators of health, well-being, and quality of life (Berkman et al. 2000; Cohen et al. 2007; Uchino et al. 1999). It is unclear how well momentary health measures could be used to predict, for example, the onset of disease, changes in self-rated health, and other key metrics of overall health. The feasibility of generating insights through the inclusion of global social integration measures as part of large-scale social surveys is also well established. Implicit in many frameworks linking global measures of social integration and health, however, is the notion that being copresent with social ties is a crucial mechanism through which individuals access social resources and support. With smartphone-based EMA data collection, repeated over days and weeks, we can get a glimpse into the dynamic and transitory aspects of social accompaniment in daily life, and explicitly examine this mechanism. Our data suggest that patterns of copresence with social ties are orthogonal to structural aspects of integration and embeddedness such as network size and overall participation in social groups. Further research is needed to better understand how shorter-term fluctuations in social accompaniment contribute to health trajectories, which may occur through effects on real-time physiological responses, or by shaping global patterns of social integration over the long term in ways that ultimately influence overall health. We suggest that theoretical frameworks and empirical studies incorporate patterns of social accompaniment to more comprehensively understand how social structure and social relationships affect well-being.
Footnotes
Acknowledgements
We thank Kathleen Cagney, Christopher Browning, Kevin Brown, Liang Cai, and Lydia Homandberg for their comments and feedback on earlier versions of this article, as well as Daphne Blakey, Julia Ward, and Yuchen Gu for their research assistance.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported by the National Institute on Aging of the National Institutes of Health under award R01AG050605. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
1
2
We considered that certain activities, such as eating a meal or shopping and running errands, are more ambiguous with respect to whether they are recreational or obligatory in the absence of additional contextual details. We therefore chose to include only activities that were more likely to be either recreational or obligatory in the coding of these variables.
3
In supplemental models, we also controlled for concentrated disadvantage in the census tract where respondents were at the time of the EMA, as real-time symptoms may also be shaped by real-time exposure to structural disadvantage (e.g., York Cornwell and Goldman 2020), however this variable was not statistically significant in predicting momentary fatigue, pain, or stress.