
Abstract
The pandemic provoked by the coronavirus disease 2019 (COVID-19) devastated poor urban neighborhoods across the world, particularly in the Global South, although empirical data on this remain limited. In this article, the authors present data collected through a mixed-methods, participatory action research approach on the impacts of the pandemic in Cidade de Deus, a “favela,” or poor informal settlement, in Rio de Janeiro. The authors find that the indirect consequences of COVID-19, in particular economic and mental health problems, were experienced as more severe than the direct effects of the virus itself, despite high rates of infection and mortality. The study also revealed that residents relied heavily on one another through local systems of mutual aid to address immediate crises. These findings suggest that the pandemic provoked a complex and diverse set of challenges and actions in the economic, social, physical, and mental spheres of poor urban neighborhoods.
An estimated 1 billion people across the world live in poor urban neighborhoods often referred to as “slums” (UN Habitat 2016), areas of high population density where many or most residents lack adequate access to water, sanitation, electricity, and durable or secure housing and where urbanization was “unplanned” (i.e., built by residents rather than by the government or a private firm) (Lilford et al. 2019). Across the Global South, these poor urban neighborhoods contained the highest density of coronavirus disease 2019 (COVID-19) cases and constituted the “most at-risk urban locations” in the pandemic (Sahasranaman and Jensen 2021). Although news outlets made it well known that the rapid spread of the coronavirus in these areas had significant impacts on residents’ physical health and death rates, a still nascent literature points to many other consequences. Social distancing measures, lockdowns, government-imposed curfews, economic shutdowns, the overcrowding of hospitals, inflation, police surveillance, and many other factors that accompanied the pandemic have also affected the lived experience of poverty during this global crisis.
This study contributes to the growing empirical research on the impact of the COVID-19 pandemic on poor urban neighborhoods. The findings are based on a mixed-methods study that took place between September 2020 and May 2021 in Cidade de Deus (CDD), the first of Rio de Janeiro’s many “favelas,” or poor informal neighborhoods, to report a positive COVID-19 case. The study followed a participatory action research (PAR) approach. It was led by a team of local residents in collaboration with outside researchers, and provided multiple opportunities for dozens of other CDD residents to help design, execute, and analyze the study. Methods included community forums, the collection of personal narratives, a survey, and collective analysis of survey findings.
Most notably, we found that the loss of jobs and income had the greatest impact on the majority of CDD residents, thanks to a spike in unemployment and extreme poverty. The second greatest impact reported by residents was on mental health, with 88 percent of survey respondents experiencing worsening mental illness. The impact of COVID-19 on death and physical health problems was the third greatest problem, thanks to high death rates from both COVID-19 and untreated chronic diseases. However, our study also revealed that the majority of participants had engaged in giving and receiving mutual aid within the neighborhood, reflecting the community’s ability to be resilient in a context of crisis. Our findings suggest the pandemic provoked a complex and diverse set of challenges and actions in the economic, social, physical, and mental spheres of poor urban neighborhoods.
Urban Poverty, Inequality and the COVID-19 Pandemic
Poverty and inequality have long been documented features of urban society (DuBois 1899; Engels 1887) and persist today. According to the 2020 “World Cities Report,” 20 percent of the world’s population lives in inadequate housing, and 1 billion people reside in slums and informal settlements, located primarily in cities of the Global South (UN Habitat 2020). These areas tend to experience not only poverty and housing insecurity but many accompanying challenges, including lack of access to good health care and education, as well as poor sanitation and infrastructure (Davis 2007; Fischer, McCann, and Auyero 2014; Weinstein 2014). Although many factors are responsible for exacerbating urban poverty, the COVID-19 pandemic had a significant impact on informal settlements, severely aggravating challenges for residents in these areas (Economic Commission for Latin America and the Caribbean 2021). However, empirical research on the effects of the pandemic in these communities remains in its infancy as social scientists begin to reckon with the immediate and potential long-term effects of both the virus and the political, economic, and social changes provoked by the pandemic on urban poverty.
Among existing studies, one of the most common findings is that COVID-19 case rates were often higher in poor communities than in other urban spaces (Henao-Cespedes et al. 2022; Sahasranaman and Jensen 2021). As many studies noted, population density combined with a lack of access to clean water or proper ventilation intensified the spread of the virus, while the presence of comorbidities increased the likelihood of severe complications and death (Corburn et al. 2020; Pereira et al. 2020). In many poor areas, this was exacerbated by low use of masks and social distancing measures, provoked partly by a lack of knowledge about how COVID-19 spreads (Islam et al. 2021) and partly by the inability for people who were homeless or living in informal housing to physically isolate (Morgan 2020; Wasdani and Prasad 2020). As Wasdani and Prasad (2020) noted in the case of Indian slums, “social distancing [was] more an aspiration than an attainable reality” (p. 414). Once vaccines against COVID-19 became available, people in poor urban areas were less likely to get them, or to get them quickly, because of fears over negative side effects (Ticona et al. 2021), lack of trust in the health care system (Alam et al. 2022), and a lack of access to vaccines (Lines et al. 2022).
In addition to the rapid spread of COVID-19, the pandemic created severe economic and social consequences. Of particular concern was the impact of mandatory lockdowns, which led to increasing unemployment and income loss, as well as physical and social isolation, thus aggravating struggles for the urban poor. For instance, a mixed-methods study in Uganda showed that slum dwellers experienced decreased access to food and education, a drop in income, loss of employment, and increase in teenage pregnancy and domestic violence (Nuwematsiko et al. 2022). Food insecurity was pervasive among poor residents in São Paulo, Brazil (Manfrinato et al. 2021), and Nairobi, Kenya (Onyango, Crush, and Owuor 2021). Additionally, a longitudinal study in seven slums in Bangladesh, Kenya, Nigeria, and Pakistan demonstrated that access to health care decreased dramatically during the pandemic, seriously affecting non-COVID-19-related physical and mental health issues (Ahmed et al. 2020). Meanwhile, Nyadera and Onditi (2020) argued that curfews, lockdowns, and other social distancing measures were a “cruel joke” on Kenya’s poor residents, who were forced to choose between their physical safety and their economic survival (p. 839). Furthermore, in many cities across the Global South, the enforcement of social distancing measures gave way to strict surveillance and punitive policing, often directed at poor communities (Bekema 2021; Finn and Kobayashi 2020).
Despite these challenges, many studies documented the creative responses of the urban poor to health, economic, and social issues during the pandemic. Auerbach and Thachil (2021), for instance, found that community leaders in Indian slums played a key role in demanding resources from government officials for their communities. In Latin America, including Brazil, Colombia, Mexico, Bolivia, and Chile, “networks of initiative” emerged, spearheaded largely by already existing community-based organizations (CBOs), to obtain and distribute emergency aid to residents in poor neighborhoods (Duque Franco et al. 2020; Ortega and Orsini 2020). In many poor neighborhoods in Asia and Africa, community health workers and local pharmacists also played a crucial role in offering informal medical advice and care, and helping connect people with medication and treatment (Ahmed et al. 2020). Furthermore, several studies examined the effectiveness of the “chasing the virus” campaign in Dharavi, Mumbai’s largest slum, which successfully contained the spread of COVID-19 for several months (Golechha 2020; Kaushal and Mahajan 2021). Although the literature on resilience during the pandemic is still emerging, these findings follow a long line of studies documenting the creative efforts of the urban poor to work to address the harmful impacts of natural disasters, poverty, and other “chronic shocks” to their well-being (Fahlberg et al. 2020; Golden 2019; Hall and Lamont 2013; Hallegatte et al. 2016; Jabeen, Johnson, and Allen 2010).
Our study contributes to this growing body of literature to provide empirical evidence on the impact of the pandemic in one of Rio de Janeiro’s most well-known favelas, Cidade de Deus or “City of God.” Through a mixed-methods, PAR approach, we captured what residents experienced as the most severe impacts of the pandemic on their lived realities. By focusing on what residents deemed important, we attempted to capture the depth, nuance, and diversity of consequences, both direct and indirect, of the COVID-19 pandemic on the lives of the urban poor.
CDD: A Storm within a Storm
To better understand the impacts of the pandemic in Latin America’s urban slums, we focus on CDD, a “favela,” or poor informal neighborhood in Rio de Janeiro of approximately 60,000 inhabitants (Portela 2017). On March 21, 2020, CDD became the first of Rio’s favelas to report a positive COVID-19 case. Four months later, a study by the Brazilian Institute of Public Opinion and Statistic across six large favelas found that CDD had the highest infection rate, with 28 percent of the sample testing positive for the coronavirus (Motta 2020). 1 In comparison, only 0.5 percent of Brazil’s population, and 0.6 percent of Rio de Janeiro State’s population, had a reported case at that time. 2 Since then, 205 people from CDD were reported to have died of COVID-19, although a lack of systematic testing and reporting may underestimate deaths.
In addition to the high infection and death rates in CDD, the neighborhood’s preexisting challenges with poverty, housing precarity, and physical and mental health issues made its residents particularly vulnerable to the pandemic. According to our study, 48 percent of respondents lived below the poverty line before the pandemic began (less than US$2/day), while another 29 percent lived on less than US$5/day. Public institutions in the neighborhood are extremely underfunded and shut down regularly. Its residents, 80 percent of whom identify as Black or pardo (brown or mixed race), are routinely discriminated against in formal employment. One third of residents have not completed primary school, and they are half as likely to attend university as other Rio de Janeiro residents (Fahlberg, Potiguara, and Fernandes 2020). The neighborhood also suffers from constant violence between drug traffickers who control the neighborhood and the military police, who regularly invade the area and initiate shootouts. By the time the pandemic hit, CDD’s residents had contended with decades of suffering from “chronic shocks” to their well-being, which made basic daily activities inordinately challenging and required that residents deploy strategies of survival and resilience to keep going (Fahlberg et al. 2020). The pandemic thus imposed many problems on top of a host of unfulfilled or violated human rights.
A PAR Approach
Like other poor urban neighborhoods, CDD has been the object of many social science studies, but its residents have rarely been given the opportunity to collect data about their own community. To ensure that we were capturing the issues of greatest relevance to residents and to reverse the colonial relationship between the academy and poor communities (Fahlberg 2022), our team adopted a Participatory Action Research, or PAR, approach (Fals-Borda and Rahman 1991; Hall 1992). PAR is based on three tenets: (1) the full participation and leadership of members of marginalized research communities in every stage of the research project, including the design of the research questions and methods, the collection and analysis of the data, and the publication of findings; (2) shared learning and the coproduction of knowledge between formally trained researchers and community members; and (3) collaboratively designed social actions that contribute to the well-being of the research community (Fine and Torre 2021; Wallerstein et al. 2017).
Our research team, which has been actively collecting data on CDD using a PAR model since 2017, 3 is composed of both formal researchers and CDD residents trained as “community researchers,” who meet regularly to determine collectively what issues are most urgent for residents, how data can be created and leveraged to address these issues, and what methods and theories are most applicable to the local environment. 4 The principal investigator trained team members on research ethics, data collection, and analysis. Meanwhile, “community researchers” and other team members provided valuable information to outside researchers about the local context. All five team members met weekly on Zoom to codesign study questions and research instruments, collect and analyze the data, and determine policy recommendations and action steps.
Shortly after the pandemic began, the research team met virtually to discuss the importance of collecting data on how the neighborhood was being affected by the virus and the unfolding economic and social changes. As one community researcher noted, stories about CDD are often written by outsiders with little insight into what matters to residents. It was essential, he argued, that a record be created by the residents themselves about this moment, what was happening, and how it was affecting people. Our team also hoped that sharing our findings with the media, policy makers, and activists in other favelas would help bring greater understanding, visibility, and resources to CDD. In the following section, we describe how the principles of PAR were incorporated into each phase of data collection.
Research Methodology
This study took place in four phases, which were designed to capture a diversity of experiences and perspectives on the impacts of the pandemic in CDD. All phases were conducted online because of social distancing restrictions. This was facilitated by the fact that Brazil is the fifth “most wired” country in the world. A 2010 study found that the majority (69 percent) of CDD’s households owned at least one cell phone and that nearly half (43 percent) owned a computer (Souza 2010). These numbers were likely much higher at the time of our study. Although many residents cannot afford subscriptions to a monthly Internet data plan, they are often able to access Wi-Fi in various stores, “LAN houses” (computer centers), local organizations, or the homes of friends or neighbors. CDD residents are extremely active in Facebook and WhatsApp text messaging groups, many of which have been created specifically to distribute news and information about the neighborhood. Given our team’s personal and professional connections to CDD, we were able to access participants via these groups. However, the study likely did not capture the most impoverished residents without phone or Internet access or digital literacy skills.
Phase 1: Discussion Forums
In September and October 2020, our team led two discussion forums on Zoom with people who had actively worked to provide relief aid to CDD’s residents in the first six months of the pandemic. We recruited participants using a snowball approach, first by directly contacting those our team members knew to be involved in organizing local relief efforts and then asking invitees to invite any providers we might have missed. The forums were attended primarily by CDD residents, including representatives from CDD’s CBOs and informal collectives, most of whom have been offering a host of social services to CDD residents for many years and who led local relief efforts when the pandemic began. The forums were also attended by some government workers from the local welfare office, local public schools, and CDD’s public health clinic who had volunteered with local relief efforts, and well as local religious leaders who were active in providing aid. A total of 28 people attended the community forums.
During the discussion forums, we asked participants what they observed in their time providing services, including which demands were most urgent and most common, as well as which groups of people were in greatest need of aid. Participants were also asked what types of data would be useful to them in order to plan additional interventions, demand resources from the state and private funders, and inform the broader public about the challenges faced by CDD residents.
Phase 2: Personal Narratives
In December 2020, our team collected written accounts from a variety of CDD residents on how the pandemic affected them. To recruit participants, our team created a short video of our team members explaining our study and its objectives in simple, accessible language. We disseminated the video on several Facebook pages and WhatsApp groups that are widely followed by CDD residents. In the video, we asked residents to tell us how the pandemic had affected them. The video was accompanied by a link in which participants could submit anonymous personal narratives of how the pandemic had affected them. The goal of this was threefold. First, our team wanted to hear directly from CDD residents, rather than relying solely on the accounts of local service providers, as not all residents had sought assistance from the providers in our discussion forums. We also wanted to capture qualitative, firsthand accounts in which residents could identify what was most urgent and relevant in their lives. Our question, “How has the pandemic affected you and your family?” was intentionally broad, to allow a wide range of responses on the basis of what residents had experienced. Finally, we wanted to determine which issues were of greatest relevance to inform the design of a survey in the following phase. We received 138 submissions, which our team read through and coded for common themes.
Phase 3: Survey Questionnaire
In December 2020 and January 2021, our team worked with dozens of local service providers, many of whom had attended our discussion forums, and other residents to codesign a survey that could quantify the extent of the impact of the pandemic on the basis of the themes and suggestions identified in the first two phases. Research team members drafted dozens of questions in a Google document, which was then shared in a WhatsApp group created by and for service providers and residents active in aid distribution. Participants could comment on or revise questions, add their own questions, edit response options, and vote on which topics and questions to keep and which to remove. We then piloted the final survey questions on several group members and made further revisions to promote internal validity and reliability of the survey instrument. A final survey of 65 questions was disseminated across multiple online platforms. 5 It contained questions about how the pandemic had affected income and employment, mental and physical health, educational access, children and adolescents, family relations, conditions of local infrastructure, the giving and receiving of assistance, and people’s opinions about the virus, the vaccine, and the government’s response. Participants were also asked about their their income and employment status before the pandemic and currently (at the time of the survey) in order to capture changes over time.
The link to the survey was widely distributed across more than a dozen Facebook pages and WhatsApp groups throughout February 2021 and early March 2021, over a total of four weeks. During that time, 815 people responded to at least some survey questions, and 648 completed all questions of the survey. Questions included individual- and household-level questions. 6 Survey respondents were representative of the racial, income, and geographic distribution of the neighborhood, while 78 percent of respondents were women and 0.2 percent identified as transgender or other gender.
Phase 4: Collective Analysis
Once collection of survey data was complete, the team prepared several charts and graphs displaying some of the main descriptive findings of the data, as well as some bivariate relationships. Service providers and other residents were invited to two discussion forums over Zoom in which the research team presented the graphs and asked participants to share their reactions and analyses of the findings. Participants also advised our team on what to do with the findings: they suggested that we publish our findings in an easily accessible format in Portuguese that both policy makers and favela residents could understand. In total, our team published three reports with a summary of the data, as well as the team and participants’ analysis of the findings. We published these on our Web site and disseminated them to various news outlets and local Facebook and WhatsApp groups. The reports were widely cited by Brazil’s main news platforms, including GloboNews, Record, Band News, and others. Favela-based community newspapers also disseminated our findings. This enabled CDD’s main concerns to be cast in the public spotlight. Some residents noticed an increase in donations from local businesses to CDD’s CBOs shortly after our study was disseminated in the news. In at least one case, a funder decided to provide four months of financial support to local CBOs after being presented with our report by one of the coauthors.
Main Findings
Income and Employment
The most significant impact of the pandemic was the loss of jobs and income. Survey respondents were asked, “If you had to choose the one thing that most affected your and your family’s lives since the beginning of the pandemic, what would it be?” As Figure 1 demonstrates, the majority of survey respondent reported that the loss of income and employment had the great impact on their lives during the pandemic (59 percent), with mental health ranking second. Illness and death from COVID-19 ranked third.

The problems that had the greatest impact on respondents during the pandemic.
The impact of job and income loss also emerged as the main theme in our discussion forums and in residents’ narratives. Service providers who had led local relief efforts noted in the discussion forums the severe impact that the loss of employment had on residents. The most common request among residents, for instance, was for food and other basic items, which residents could no longer afford. Forum participants noted being surprised when people they knew to have previously led economically stable lives were standing in line waiting for food baskets. Residents’ narratives provide further insight into these impacts. Forty-six percent of personal narratives mentioned loss of work, and another 33 percent mentioned concerns over income loss. For instance, one respondent shared this with us: Since March my life has completely changed. I lost my job, my husband too. When I was called to go back to work, I couldn’t return because my son doesn’t have day care. My husband is doing odd jobs that appear from time to time. What this means is that our income, which was once guaranteed, today is no longer. We are not starving but things are difficult. . . . We are in a difficult situation with a three-year-old and no income. Not to mention that everything has gotten very expensive. We are not living, we are surviving, it is very difficult for the poorest people.
The pandemic exacerbated the struggles of daily survival. Those who previously had reliable, even if low income, became burdened by extreme poverty and the fear of not knowing whether they would have enough to survive each week. Many others who were already very poor found themselves in desperate situations.
People lost work for many reasons. 32 percent of survey respondents reported having formal employment before the pandemic. This dropped to 20 percent during the pandemic, according to our survey. In their personal narratives, many respondents reported being let go when their workplaces were required to shut down. Others reported that they stopped working because of fear of contracting the coronavirus on public transit and at work. Our survey also found a drop in informal employment, from 24 percent before the pandemic to 17 percent in March 2021. Many respondents who submitted narratives reported that they had lost clients from informal jobs, such as those who worked in catering or cutting hair, when their regular customers—CDD residents with stable incomes—lost formal employment.
As Figure 2 demonstrates, loss of jobs had severe impacts on an already poor neighborhood. Figure 2 displays data from two survey questions, in which respondents were asked what their incomes had been before the pandemic and what their incomes were at the time of the survey (February and March 2021). We present the total household income per capita, grouped by social class. 7 As the data show, the percentage of people living in extreme poverty nearly doubled, from 12 percent to 20 percent, while the number of people living on less than R$291 (US$56) a month increased from 48 percent to 63 percent. The middle and upper classes were hollowed out. Shortly before the launch of our survey, the Brazilian Institute of Geography and Statistics reported that the cost of groceries had gone up by 19 percent (Elias 2021). Loss of income coupled with higher costs of basic goods created a severe challenge to survival.

Change in socioeconomic class between March 2020 and March 2021.
School closures, discussed below, further restricted employment, particularly for mothers, who were forced to stay home to watch their children. Consequently, income loss was especially significant among female-headed households. As can be seen in Figure 3, our survey found that households headed by women were significantly more likely to enter the lowest class than male or mixed-headed households. 8
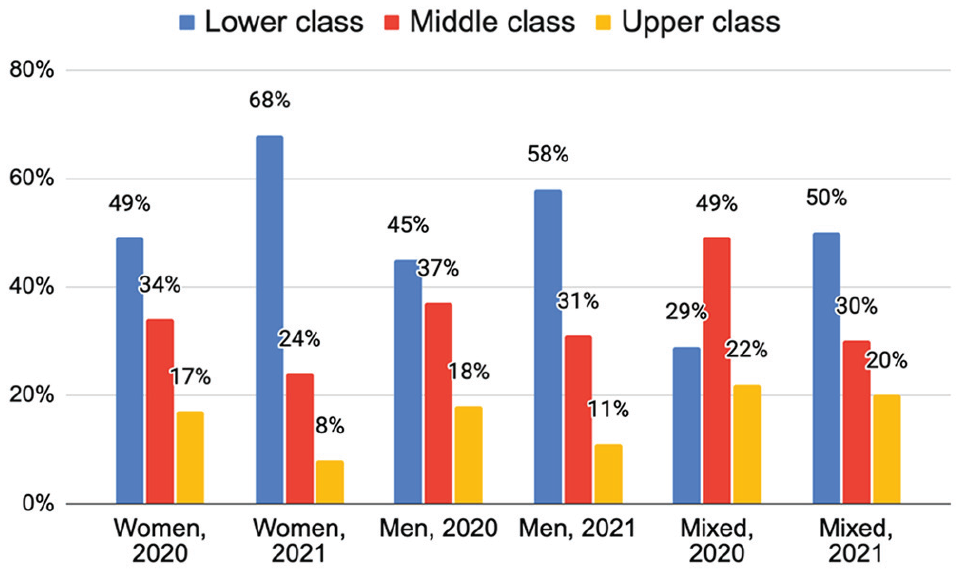
Change in socioeconomic class between March 2020 and March 2021, by gender of head(s) of household.
This has not only gendered implications but age implications as well. Several participants who submitted personal narratives reported that older women in the household were forced to return to work to help cover expenses when younger adults lost their jobs. As one person reported, The pandemic has affected my family, like all families. Unemployment, lack of food, lack of medicine, lack of money. My mother, now she got a job that pays so-so, but her boss is the devil, without workers, and she no longer has the age to put up with such things but she is putting up with it out of sheer necessity. I have a six-year-old son and until now I’m still unemployed, I’ve sent several résumés . . . but so far nothing and this frustrates me because my son needs things and I have nowhere to get them.
In February 2021, 52 percent of our survey respondents reported they were now unemployed, up from 31 percent in March 2020. This rate was three times higher than unemployment across the state of Rio de Janeiro, demonstrating that the burden of the economic recession and the lockdowns was carried overwhelmingly by the city’s poorest residents. When our survey participants were asked if they were able to pay their monthly expenses, the majority (83 percent) of our survey respondents reported having being unable to do so.
The economic impact was racialized as well. Although income was roughly similar among Black, pardo, and White residents before the pandemic, Black residents were more likely to lose employment and income during the pandemic. The percentage of Black residents in the lowest class increased by 14 percent, while white residents saw an increase of 11 percent. Not surprisingly, community leaders in discussion forums noted that Black women made up the vast majority of those standing in line to receive a food basket.
Mental and Physical Health
In discussion forums and residents’ narratives, we found that the pandemic created severe mental health problems. Anxiety and stress over contracting COVID-19 and affording basic needs were pervasive. In many of the submitted narratives, respondents reported being concerned about their children and adolescents, who displayed high levels of anxiety, depression and obesity. This finding matched data from our survey, in which we asked respondents whether they experienced worsening symptoms related to a variety of mental health issues, as well as physical conditions that are often exacerbated by psychological problems. Figure 4 presents the conditions that respondents reported worsening during the pandemic.
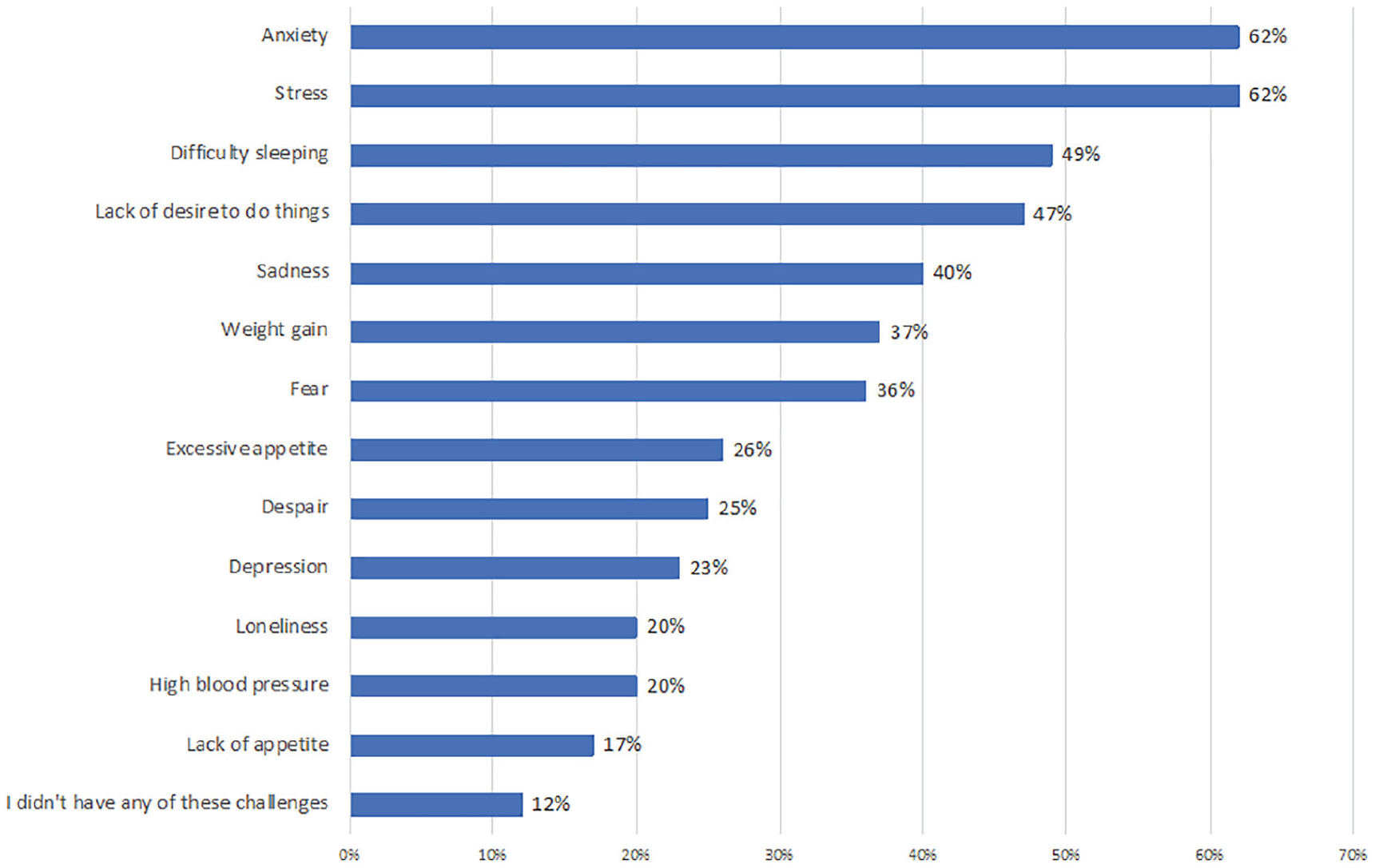
Worsening mental health problems and related physical problems during the pandemic.
As we can see, the vast majority of respondents (88 percent) experienced worsening mental health and related physical consequences (such as weight gain) during the pandemic. The most common problems were stress and anxiety, followed by difficulty sleeping and a lack of desire to do things, which are both symptoms of depression. This is how one parent described their experience in a submitted narrative: Goodness, here at home we often feel as if we were living in a horror fiction movie. It is visible to see how much our daughters are stressed, irritated and even depressed. I had all the symptoms [of COVID-19] very severely. They fear the worst. They are not comfortable leaving the house or going to nearby places like the bakery. Sometimes they, especially the older ones, say that she doesn’t know how to talk to people. They lost a little of the notion of day, sleep alteration. I already get treated for depression and I had all the symptoms in a severe way. I’m terrified of getting [the coronavirus] again.
As in many other densely populated neighborhoods, social distancing and quarantining during the pandemic were near impossible feats for most residents. As one social service provider noted in the discussion forum, most people live in small homes with many family members, often with only one bedroom for the entire household. This had two significant impacts. For one, survey respondents identified that family conflict increased during the pandemic. According to personal narratives and conversations in discussion forums, we found that this was due to having to share tight spaces for extended periods of time, as well as arguments between parents and adolescents, who wanted to break quarantine to see friends. A second challenge we identified was an inability among residents to isolate from other household members, which allowed the virus to quickly spread across the household. One respondent submitted the following narrative: The pandemic came like a bullet for me, I was isolated with all my family, but that didn’t stop my mother, my father and everyone from being contaminated very close to me, my mother got very sick, we didn’t do the test to confirm, but she had all the symptoms, we took care of her at home and I ended up contracting the virus (I didn’t test to confirm) but we managed to save my mother. But I lost my father to COVID-19. On May 11th my father was interned and in his report it was written that he was contaminated with corona virus. Ah, no one is prepared to lose anyone, right, my brothers and I still can’t understand his departure.
The majority of households (68 percent) in our survey had at least one person with COVID-19 symptoms, and 38 percent of respondents believed they had COVID-19, either because they had a positive test result (9.4 percent) or because they experienced symptoms. Sixty-one percent of our respondents reported losing close friends or family members to COVID-19. The experience of loss was a racialized phenomenon: the rate of death from COVID-19 among Black residents was 12 percent higher than among white residents.
Although deaths from COVID-19 in CDD were high—respondents reported a total of 41 deaths in our sample of 648 households—respondents reported 59 deaths from other causes. The most common causes, according to survey respondents, were chronic illnesses, followed by other diseases, accidents, and violence. Service providers noted in the discussion forums that many residents with chronic illnesses were fearful of contracting COVID-19 if they visited hospitals and clinics, and many were unable to get appointments because of the overloading of coronavirus cases. In other words, even with high infection and death rates from the coronavirus, deaths from untreated diseases were more life threatening than COVID-19. The challenges that CDD residents faced before the pandemic, such as lack of access to proper medical care, safe places to exercise, and affordable nutritious food, created a double pandemic where preexisting conditions coupled with the coronavirus to create a landscape of extreme risk.
Education and Youth
When the pandemic began to spread in March 2020, public schools across Rio de Janeiro shut down and sent children home. According to our survey, more than half of respondents’ children (57 percent) were offered weekly packets of educational activities that parents could either print from home (although few people have printers) or pick up and bring home for children to work on (requiring that parents break quarantine). Another 43 percent were provided online learning options. However, according to survey respondents, fewer than one third of school-aged children have access to the Internet at home. Children were thus unable to participate in these activities. Not surprisingly, our survey found that one third of children ages 6 to 14 spent less than one hour a week on schoolwork, and another 45 percent spent one to two hours a week. Only 8 percent spent more than five hours a week on schoolwork. The lack of schooling in CDD reflects a much larger issue across Latin America and the Caribbean, where 120 million children lost or ran the risk of losing a full school year (Saavedra and Di Gropello 2021).
Survey findings indicated that children in middle-class homes in CDD spent more weekly hours on homework than those in the lower class, though in both classes the amount of time fell grossly below a normal school week. The lack of schooling or a routine outside the home had a severe impact on many children. One parent reported in a personal narrative, I think the worst part of it all was how much it affected our psyche. My youngest son went into depression and was also taken by anxiety. I would find him in the corner of the room, curled up in a fetal position and staring at nothing. When I asked what he had, worried, he tearfully replied that he wanted our routine back, he wanted our busy life and he couldn’t stand being locked up at home anymore. He can’t sleep properly. And all the time looking for something to eat. He lies in bed and fidgets for one, two hours. When he falls asleep it is already past midnight, so the next day he wakes up at noon. Totally unregulated. Gained 10 kg. Can you imagine a nine-year-old 10 kg overweight?
Our survey revealed that in 82 percent of households with a child between the ages of 6 and 14, at least one child experienced worsening mental health problems, while 80 percent of households with adolescents reported the same. Anxiety, stress, and trouble sleeping were the most common problems for children and adolescents.
Adolescents faced additional barriers. More than 20 percent of households with adolescents reported in the survey that at least one adolescent began working during the pandemic to help with household costs, and in 12 percent of homes, at least one adolescent quit school. Although schools did eventually reopen and, by law, required children to return to school, adolescents who dropped out of high school during the pandemic may be unlikely to return. For both children and adolescents, the loss of schooling during the pandemic will have a lasting impact on the economic and educational opportunities available to CDD’s young residents compared with wealthier children able to learn remotely.
Adult education was also affected. One quarter of survey respondents had been enrolled in college courses or other classes when the pandemic hit. Of those, 73 percent had to quit their studies because the courses were put on hold or to stay home with children or look for a job. Black respondents were much more likely to leave schooling than whites (75 percent vs. 64 percent). Some of these adults may be able to return to their studies as the economy begins to reopen, while many others may now be unable to afford the cost of these programs because of income loss. The long-term job prospects for CDD’s adults have been severely harmed by the loss of educational opportunities.
Receiving and Giving Aid
The Brazilian government has been widely criticized for its neglect during the pandemic, having offered little support to Brazil’s struggling citizens. One exception was the emergency aid provision passed by the Brazilian Congress in April 2020, which provided unemployed Brazilians with a monthly stipend of R$600 (US$116) for five months. Some people received R$300 (US$58) for four additional months. The majority of survey respondents (71 percent) reported receiving emergency aid. However, many people reported in their narratives that this assistance was far from sufficient in covering monthly expenses. As one participant noted, “This blessed aid, for those who live on rent, isn’t anything, you know, especially with children. I have a three-year-old son and a four-month-old baby so it gets very difficult. Sometimes I pay rent and buy almost nothing for the house.”
To make up for the insufficiency of the government’s slow and limited response to the pandemic, CDD residents mobilized almost immediately to offer help. Mutual assistance within kinship networks became essential. In our survey, we asked respondents if they had relied on financial assistance from family and friends to help pay for monthly expenses before the pandemic, both before the pandemic and at the time of the survey. According to our survey, the reliance on financial donations from family and friends to help cover costs tripled from before the pandemic to a year into the pandemic, from 7 percent to 22 percent of respondents, respectively. Survey respondents also reported relying heavily on locally run CBOs for assistance with food baskets and other needs. As Figure 5 demonstrates, nearly half of survey respondents reported received help from collectives or CBOs in CDD, and another 18 percent received help from family and friends in CDD. Fewer than 20 percent received help from outside CDD, and only 3 percent reported receiving helping from public agencies.

Receipt of aid from groups within and outside Cidade de Deus (CDD).
Respondents from all socioeconomic levels reported needing assistance from CBOs. Among those who received help from local CBOs, the majority (63 percent) reported that that aid was essential to their family’s survival. The high rates of dependence on outside assistance among families that had been middle class before the pandemic suggests that some socioeconomic differences have diminished as unemployment and poverty surged, the virus spread, and residents collaborated for survival.
Finally, we found that respondents were also extremely active in offering assistance to friends and family members. Seventy-eight percent of survey respondents offered help to people in need. The most common forms of assistance reported were providing food (44 percent) and emotional support (36 percent), followed by helping care for children (17 percent) and giving money (11 percent). As in many other poor urban areas, mutual assistance is essential to residents’ survival. However, as became clear from the discussion forums and narratives, giving aid also comes at a great financial and emotional cost for people who are already struggling themselves. CDD has a long history of resilience and collective action in times of crisis, yet these efforts take an enormous toll on residents who forfeit their own time, energy, and economic well-being to care for those in dire situations (Fahlberg 2018).
Legacies of the Pandemic in Poor Urban Neighborhoods
On the basis of these findings, we identify several important themes that may apply to cases far beyond CDD and that help us think about the long-term impact of the pandemic in poor urban neighborhoods. The first is that although the coronavirus had a strong impact on residents’ physical health, the greatest concern to poor urban residents was extreme economic loss. The closing of businesses, widespread layoffs, and a drop in customers created massive unemployment and income loss. This in turn created such direct threats to survival that trying to find food and pay basic expenses became a more urgent matter than dealing with the deaths of family and friends. The second greatest challenge was not physical but psychological, as revealed by the stress and anxiety created by the inability to feed one’s family, buy needed medication, and worry about contracting the coronavirus. This suggests that the most urgent demand for resources in poor areas may be centered primarily around economic and psychological needs. It also reveals how inequality creates different challenges for the poor than for wealthier residents, who could focus their resources, time and energy on preventing the spread of the virus and grieving the deaths of loved ones.
Another important theme is that the coronavirus did not stand out for its physical impact but simply added another layer of challenges to an already dire situation. As noted, more people in CDD died of causes other than COVID-19 during the height of the pandemic. In a context of poverty, food and water insecurity, and inconsistent or inexistent medical care, residents with chronic illnesses continued to suffer, and deaths from accidents and violence remained prevalent. Despite the overwhelming concern among the press, policy makers, and society more generally over the deaths from COVID-19, many of the “chronic shocks” that disrupted the everyday lives of the urban poor before the pandemic remained. Preventing and treating COVID-19 will not be sufficient to address the many forms of inequality and scarcity that characterized these neighborhoods before the pandemic.
A third theme is the long-term effects of the pandemic on growing inequality between poor people, particularly Black people and women, and other urban residents. In contrast to wealthier children who had access to computers and regular Wi-Fi and could continue their studies online, CDD’s children lost more than a year of schooling. When they returned to in-person schooling nearly two years after the pandemic began, they were not only far behind middle- and upper-class peers but suffered with exorbitant rates of stress, depression, and anxiety. Many parents who took our survey reported that their children and adolescents were afraid they had fallen too far behind to keep up in school. Children in poor areas will thus be at a growing disadvantage when competing for entry into public universities or jobs, even many years after the pandemic is over. Adults who had to drop out of schooling will also experience much slower economic mobility. As noted, these effects were particularly acute among women, female-headed households, and Black favela residents, demonstrating that, in addition to class inequality, the effects of the pandemic have also been gendered and racialized. Unless significant resources are put toward educational supports for children and adults in favelas, the economic disparities already exacerbated by the pandemic will affect an entire generation, and likely future generations as well.
Finally, our findings demonstrate the importance of local systems of mutual support for promoting residents’ survival and well-being in response to crisis. This reminds us that the urban poor are not just victims of social inequality but also agents who respond to problems with immediate and creative solutions. As many service providers noted in the discussion forum, CDD’s residents are used to finding local solutions to issues in a context of governmental neglect. These findings are consistent with a broader literature on the importance of social resilience in informal settlements (Fahlberg et al. 2020; Golden 2019; Hall and Lamont 2013; Hallegatte et al. 2016; Jabeen et al. 2010). However, there is a high cost to sharing resources when one has very few resources already, often resulting in poor families become even poorer as they help friends and family members avoid starvation, severe illness, and death. In the long run, this denies poor residents the opportunity to live stable lives and obtain economic and social mobility.
Policy Recommendations
We draw on our collective learning from CDD residents in proposing a set of recommendations to aid in the postpandemic recovery in favelas, though many of these may also be relevant in other poor urban areas. The first recommendation is that more economic and social assistance is desperately needed to promote employment and address extreme poverty. The majority of survey respondents (69 percent) agreed that the government should help with food and other basic resources and 71 percent wanted help with employment. The lack of state support during the pandemic was also a pervasive theme in discussion forums, as service providers had to locate private donations to help people in crisis. Postpandemic recovery will require many more resources, including a strong commitment by the municipal, state, and federal governments to providing high-quality physical and mental health care for those with chronic illnesses, as well as school remediation for children who missed one or more years of learning. Finally, the state should provide adults and working-age adolescents with relevant training and college courses and assistance in finding stable employment in order to promote economic recovery in favelas. Given the extreme impacts of the pandemic on Rio’s favelas, aid directly to the hardest areas will be essential to addressing the expansion of urban inequality.
Furthermore, our findings suggest that more funding should be invested in informal collectives and CBOs run by poor urban residents, who were on the frontlines of pandemic relief efforts and have the local knowledge and mobilization capacity to channel the most relevant and useful forms of aid directly to those who most need it. By strengthening the service and organizing capacity of these mediators, the private and public sectors can ensure that investments in larger welfare systems are accessible to the most vulnerable urban citizens. Finally, it is essential that both public and private funding agencies plan recovery responses in collaboration with poor residents and the local organizations that serve them to ensure a fair, responsive, and efficient distribution of resources to the people who most need it.
Conclusion
One respondent noted in their personal narrative, This pandemic came to show us that we have to have a government that takes care of the people, we are in a social isolation that prevents us from working to eat and pay the bills, in fact we already live a social isolation in all human aspects.
In our discussion forums and informal conversations with other residents, we heard similar comments about the feeling of abandonment by the state and the sense that social isolation was not a new phenomenon in favelas. For many CDD residents, favelas have always been on the margins of society, left to fend for themselves in a context of governmental and societal neglect. Social isolation during the COVID-19 pandemic was not a new experience but a reflection of their daily lived realities. At the same time, favela residents have become the experts in survival and collective action, having had few alternatives throughout their community’s history. Ultimately, our study demonstrates the complexity and diversity of impacts the pandemic has had on this poor urban neighborhood, including not only the physical effects of the coronavirus but also the severe toll on employment and income, mental health, and education. These intersecting challenges also sparked a variety of mobilization efforts as individual residents and a host of informal groups and CBOs sprung to action to help those most in need.
Footnotes
1
2
A study published on June 17, 2020, showed that 1,009,699 had tested positive for COVID-19 across the country, representing roughly 0.5 percent of the population. Meanwhile, Rio de Janeiro had a reported 87,317 cases, representing roughly 0.6 percent of the state’s population. It should be noted, however, that these rates reflect only those who were tested because of symptoms of illness and cannot be compared with rates in CDD, where residents were randomly tested.
4
The team that undertook this study was composed of two outside researchers, including the principal investigator, an American professor based at [Tufts University] University who has been conducting ethnographic and survey research in CDD since 2014 and a Brazilian sociologist based at Fiocruz, Brazil’s federal health research center, who has also been conducting research in CDD for many years. The team also included an undergraduate Brazilian student from [Tufts University] supervised by the principal investigator, and two Black women from CDD, both of whom have college degrees. All five are listed as coauthors, in order of their contributions to the research process and writing of the manuscript.
5
To access the questionnaire, respondents had to first consent to the survey, confirm that they were 18 years or older, and self-identify as residents of CDD. To incentivize completion of the survey, respondents were offered the chance to participate in a raffle for 1 of 20 gift cards of R$100 (US$20). When the survey was complete, participants were directed to a new link at which they could input their information.
6
We avoided double responses of household-level questions by providing a shortened survey of only individual-level questions to participants who reported that someone else from their household had already taken the survey.
7
Our categorization of socioeconomic classes follows those of the federal government’s Secretariat for Strategic Issue (Secretaria de Assuntos Estratégicos) (![]() ). It is important to note that tiers defined as “low middle class” and “middle middle class” constitute low incomes—less than US$5/day—that more accurately reflect the experiences of a vulnerable or partially vulnerable “working class.”
). It is important to note that tiers defined as “low middle class” and “middle middle class” constitute low incomes—less than US$5/day—that more accurately reflect the experiences of a vulnerable or partially vulnerable “working class.”
8
Although surveys often allow only one person to be listed as the “head of household,” our survey allowed respondents to check off all the individuals who made significant financial contributions to household expenses. We then grouped households on the basis of whether those identified as significant contributors were all women (mothers, grandmothers, aunts, female respondents, etc.), all men (fathers, husbands, uncles, male respondents, etc.), or a combination of men and women.