
Abstract
Children have been theorized as vulnerable to the health consequences of climate change, but data limitations have hampered prior studies of climate-related disasters in the United States. In this article, the author exploits the interruption of a health survey in Houston by Hurricane Harvey, linked to local flooding data (n = 1,123, ages 5–17 years). Multivariable models on a matched sample show that Harvey led to worse parent-reported health among children six to nine months later, particularly in flooded communities. Further evidence suggests that household life disruption and home damage were key mechanisms and that severe exposure correlated with larger health declines among immigrants, including Hispanic and Asian or other-race children and those younger than 10 years. Integrating these findings with life-course theory and climate science, the author argues that through disasters, climate change should be conceptualized as a risk factor for heath and intragenerational disparities within cohorts and for intergenerational inequalities as newer cohorts experience more extreme weather.
Climate change poses serious and pervasive threats to human well-being through multiple pathways, including from exposure to increasingly severe extreme weather events, such as tropical cyclones, floods, and heat waves. Social scientists have long theorized children as a population subgroup particularly vulnerable to these climate-related disasters 1 because of their reliance on schools and families for support and their premature stage of physiological development (La Greca et al. 1996; Norris et al. 2002; Peek 2008). Given life-course perspectives on early life exposures (Case and Paxson 2010) and the fact that newer birth cohorts will experience more extreme weather because of climate change (Thiery et al. 2021), the climate-health nexus in childhood is of critical interest empirically and theoretically to social demographers applying a life-course perspective to inter- and intragenerational processes, environmental sociologists studying climate change and disasters, and medical sociologists interested in understanding the fundamental causes of health disparities.
Scholars from a variety of disciplinary backgrounds have examined the relationship between exposure to extreme weather and health early in life. Researchers have found that across a variety of health outcomes, including infant birth weight, height in adolescence, and depressive symptoms, exposure to extreme weather is associated with reductions in well-being (Peek et al. 2018). Yet despite this growing body of evidence, several gaps remain. First, data limitations have hindered prior efforts at estimating effects in the United States. Existing evidence comes almost exclusively from data gathered on exposed children in the postdisaster context, an understandable feature given that many disasters occur suddenly, even if increasingly expectedly. As noted in recent reviews, published research that includes an unaffected control group or predisaster data in the United States is extraordinarily sparse, especially for children (Arcaya, Raker, and Waters 2020; Peek et al. 2018). Among the handful of exceptions in the United States (e.g., La Greca, Silverman, and Wasserstein 1998), all use data collected from convenience rather than population-representative samples (Kousky 2016). Among the causal evidence that exists on children’s health from representative data sources, most study exposure in utero, rather than during adolescence, and are on disasters that occurred in developing contexts (e.g., Andrabi et al. 2021; Cas et al. 2014; Rosales-Rueda 2018). Consequently, there is continued need for research on the health consequences of climate-related disasters in the United States experienced after gestation or infanthood, using estimation strategies that approximate causality.
In this article, I begin to address these limitations by leveraging restricted-access data from the Health of Houston Survey (HHS) 2017–2018, a study of health in the city of Houston and Harris County, the nation’s fourth largest city. The survey was in the field in summer 2017, interrupted by Hurricane Harvey in August, one of costliest disasters in U.S. history, and resumed six months later. I link these survey data to flooding estimates from the Federal Emergency Management Agency (FEMA) using the ZIP code of residence. Adults were interviewed and asked a series of questions about a randomly selected focal child living in the household. Within-neighborhood estimators and a difference-in-differences (DID) model show that Hurricane Harvey led to worse generalized health status for children as reported by a parent or grandparent. Additional evidence suggests that postdisaster children’s health correlates most strongly with disaster-induced disruption to household life and home damage, compared with household income loss. Further associational evidence shows a larger, negative relationship between health and severe household exposure for immigrant children, Hispanic, Asian or other-race children, and those in middle childhood (ages 5–9 years).
With these findings, I argue that disasters caused by climate change should be integrated into understandings of primary risk factors for health during childhood. Comparing my main effect estimates to those published on another life event—that is, an eviction (Hoke and Boen 2021)—the DID estimator is substantively similar in magnitude. By integrating my results with life-course theory (Mayer 2009) and the science of climate change, I outline four implications of this research for the climate-health nexus. First, as climate change increases the severity and patterning of extreme weather events that cause disasters such as Hurricane Harvey, sociologists should conceptualize exposure as part of the life course, especially for newer birth cohorts living in vulnerable parts of the United States, such as along the Gulf Coast. Second, my evidence points to middle childhood, the youngest age group examined, as a potentially sensitive or critical period for exposure. Third, because early life conditions matter for later life health, childhood exposure to climate-related disasters may exacerbate intragenerational health disparities, along core axes of stratification, such as nativity and race/ethnicity. Finally, because newer birth cohorts will be more affected by extreme weather, climate-related disasters should also be conceptualized as a potential site for intergenerational disparities in health.
Background
Changes in weather patterns and severity are occurring around the globe because of anthropogenic forcing, with both direct and indirect implications for population health. Exposure to extreme weather events, such as tropical cyclones and heat waves, can cause mortality, long-term morbidity, and adverse mental health (Ebi et al. 2021), while climatic changes can also more indirectly affect health by inducing human conflict (Hsiang, Burke, and Miguel 2013) and altering land use and infectious disease spread (Mahmud et al. 2020). Sociologists have long noted that the consequences of disasters, including those related to climate change, vary across subgroups (Tierney 2019). One population subgroup of particular interest is children and youth.
In a strand of research linking conditions in utero to health at birth or early in life, a growing number of studies, most conducted by economists, have examined exposure to extreme weather linked to climate change, including hot temperatures and tropical cyclones. For example, several high-quality studies have shown that among those exposed in the later stages of gestation to the Indian Ocean tsunami in Indonesia and the El Niño flooding in Ecuador experienced adverse health, as evidenced by children’s height in adolescence (Frankenberg et al. 2017; Rosales-Rueda 2018). Less causal evidence on children’s health has accumulated from climate-related disasters experienced during adolescence. Among several exceptions, Andrabi et al. (2021) found that the 2005 Pakistan earthquake led to height deficits among exposed toddlers younger than three years, Baez and Santos (2007) documented that Hurricane Mitch significantly increased children’s malnutrition in Nicaragua, and natural disasters in India increased acute illness in children younger than five years (Datar et al. 2013).
Nearly all causal evidence, however, exists on children in developing contexts. Yet the effects may vary across countries because of differences in economic development, the organization of health care, and sociopolitical environment. In the United States, stunted growth may not be as strongly linked to disaster exposure, given the low rates of malnourishment. Additionally, evidence from a U.S. disaster is necessary for domestic policy makers and pediatricians working to identify risk factors and key points of intervention that may promote children’s health and well-being in the face of climate change.
A growing body of associational evidence from the United States links disasters to children’s depressive symptoms (Lai, Auslander, et al. 2014), psychosomatic complains (Hensley and Varela 2008), and posttraumatic stress (La Greca et al. 2010). Other studies also demonstrate a relationship between exposure and physical health conditions (Lai, La Greca, and Llabre 2014). Losing belongings, witnessing the destruction of a home and subsequent stress in parents, and having to unexpectedly switch schools and make new friends may all be factors that adversely affect children’s well-being (Peek et al. 2018). Compared with adults, children may suffer more for social reasons, such as their reliance on school and families for support, and for biological reasons related to the premature stage of their physiological development (Kousky 2016). However, endogeneity may bias these findings on the basis of postdisaster sampling because despite the common refrain that disasters are exogenous, sociologists have noted that their effects are influenced by a host of preexisting social, economic, and political factors (Tierney 2019). For example, not only does living in a poor neighborhood causes adverse health outcomes, but there are also health selection effects into neighborhoods, such that those with poorer health are more likely to reside in or move into poorer neighborhoods (Arcaya et al. 2014). Given the history of residential segregation and the spatial sorting of low-income and racially marginalized groups into hazard-prone areas, including flood plains in Houston (Lu 2017), this means that prior associational strategies may be confounded. One strategy increasingly common in the disaster literature is to condition on predisaster health (Raker et al. 2019); however, few studies on children in the United States have been able to use this adjustment strategy.
Additionally, effect difference across demographic subgroups has formed a primary interest for sociologists studying health disparities. With respect to race, class and gender, scholars have conceptualized girls, those in low-income families, and racially marginalized children as particularly at risk for health adversity, constituting socially vulnerable groups (Peek 2008). In general, null and mixed findings preclude generalizable conclusions about which groups are most vulnerable to declines in health after exposure during childhood (Peek 2008). However, although racial differences are less conclusive given comparatively fewer studies (Jones et al. 2001), the bulk of evidence suggests younger children and girls are particularly vulnerable to health adversity. As noted by Peek et al. (2018:251), although many studying disasters have emphasized potential differences in effects, prior research tends to use demographic characteristics as control variables rather than axes of variation. Indeed, most evidence on demographic risk factors come from interpreting coefficients on control variables rather than interacting them with measures of exposure. Finally, because the timing of exposure matters, differences in the effects across age groups can point to salient or critical periods for exposure (Elder 1994).
The Case of Hurricane Harvey
In the U.S. context, understanding the health implications of exposure to hurricanes is salient given the evidence that human activity is exacerbating the severity and altering the spatial patterning of tropical storms along the Atlantic and Gulf coasts (Emanuel 2005; Knutson et al. 2010). Five years ago, Hurricane Harvey made landfall near Corpus Christi in late August 2017, as part of the historic 2017 Atlantic hurricane season. Physical damage was valued at $125 billion, making it one of the top three costliest disasters in U.S. history, alongside Hurricane Katrina in 2005 and Hurricane Sandy in 2012 (Blake and Zelinksy 2018). The category 4 storm cell slowed and intensified over Houston and dropped an unprecedented 36 to 48 inches of rain, causing catastrophic flooding (Emanuel 2017). Risser and Wehner (2017) estimated that elevated air and water temperatures due to climate change increased Harvey precipitation between 30 percent and 38 percent. About 100 people died because of direct and indirect storm exposure. By any metric, Hurricane Harvey was a disaster, and it was so because of human-caused changes to the climate.
Several prior studies have examined the consequences of Hurricane Harvey for population health. Analyses on a convenience sample of adults fielded shortly after the disaster found that property damage was associated with greater mental health symptoms three weeks after the hurricane (Schwartz et al. 2018). A recent study using the HHS showed that adults experienced an estimated increase of 1.31 days per month of poor mental health and 1.12 days per month of poor physical health (Bozick 2021). The consequences for adult health varied across commonly studied demographic groups. Fitzpatrick (2021) found that those who were younger and non-White were more likely to experience higher levels of posttraumatic stress symptoms. No study to my knowledge has examined the effect of Hurricane Harvey on children’s health using a comparison sample of otherwise observably similar, unexposed children. To fill this gap, I leverage the interruption by Hurricane Harvey during the fielding of a large-scale health survey in Houston to ask three research questions: (1) What was the effect of Hurricane Harvey on children’s generalized health status? (2) To what extent and what types of household-level exposures were detrimental to children’s health? and (3) How did the health effects of severe exposure vary by race, nativity, class, and gender?
Data and Methods
Data and Coding of Variables
Primary data for the empirical analysis are cross-sectional data from the 2017–2018 HHS, a large-scale survey of Harris County and City of Houston residents administered by the University of Texas Health Science Center at Houston. The HHS began in late May 2017, was interrupted by Hurricane Harvey in August 2017, and resumed data collection six months later in February 2018. Data collection concluded just before May 2018. Adult respondents with children in the household were asked a series of questions about one randomly selected focal child between 0 and 17 years of age, but only if respondents were parents or grandparents. I restrict my analysis to children older than 5 years (n = 1,123, ages 5–17 years). Listwise deletion omits children with missing health data (n = 25) and household ownership (n = 11), resulting in a sample with valid responses for n = 1,087 children. Because of imbalance across the predisaster and postdisaster samples by flooding level, the primary multivariable strategies use a matching procedure discussed below, resulting in an analytic sample of n = 742.
I operationalize children’s health using parents’ reports of their children’s generalized health status, a variable that captures a global assessment of well-being from the parent’s perspective. Each parental or grandparental informant was asked, “In general would you say this child’s health is excellent, very good, good, fair [coded 5], or poor [coded 1]?” I model this health measure coded as ordinal, 1 to 5, as well as with two dummy variables. The first identifies children in excellent (1) versus other (0) health, and the second codes children in good, fair, or poor (1) versus very good or excellent (0) health. Together, this outcome coding allows a comprehensive test of where in the distribution of generalized health change occurred because of Harvey.
General assessments of children’s health and well-being have long been used in sociological research, and parents’ reports using this scale and others have been found to correlate strongly with other indicators of children’s physical and mental well-being (Pless and Pless 1995; Waters et al. 2000). For example, Fosse and Haas (2009) reported that in the National Longitudinal Survey of Youth 1997, there was concordance between parents’ and children’s own reports of self-rated health, which correlated with chronic health conditions, emotional problems, and obesity. Because disasters are theorized to affect children’s physical, emotional, and mental well-being, this global assessment helps capture an overall effect. Moreover, generalized questions about health status, like the one used here, have among the highest interrater reliability (Eiser and Morse 2001). Finally, this variable allows a comparison with other studies with similar identification strategies that examine the health effects of other life-course events, such as evictions (Hoke and Boen 2021).
I use five independent variables at the child level: a mutually exclusive categorical variable for race/ethnicity (non-Hispanic White, non-Hispanic Black, non-Hispanic Asian or other, and Hispanic), a dummy variable for nativity (first-generation immigrant or not), a categorical variable for age (5–9, 10–14, or 15–17 years), a dummy variable for gender (female or other), and a dummy variable for health insurance (yes or no). These five measures are used given that they feature prominently in the existing disaster-specific health literature (Peek et al. 2018) and in the broader sociological and epidemiological literature on health disparities across social groups. From the adult informant, I gather additional household-level measures: a dummy variable for homeownership (owned residences or not), a dummy variable for marital status (married/cohabitating or other), a continuous variable for other children in the household (zero to five), and dummy variable for poverty status (below federal poverty line or above). I also retain information on the gender of the informant (female or male) and their age using a 10-part categorical variable raging from 20 to 85 years. See the Online Appendix for more details on the coding of children’s nativity and household marital status.
Information from the ZIP code of residence and from the adult informant are used to compose objective measures of local flooding from Hurricane Harvey. To each child’s ZIP code, I use FEMA data estimating flooding extent at 3 × 3 m pixel resolution. Pixels were defined as flooded if there was evidence of greater than 1 foot of water from high water marks, using various sources, including U.S. Geological Survey and other inspection data (University of Texas Advanced Computing Center 2017). I overlay the pixel data with ZIP code (ZIP code tabulation area) boundaries to estimate the proportion of ZIP codes flooded by Harvey. The mean proportion of pixels flooded per ZIP code was .12 (SD = .09). I defined no or minimal flooding as flooding below the 25th percentile of flooding (38 ZIP codes) and flooded if more (102 ZIP codes). The coding of local flooding was selected given that it yielded the greatest balance across observable characteristics in pre- to post-Harvey samples across treatment category, but alternative strategies yielded substantively similar findings. It is important to note here that for those interviewed after Hurricane Harvey, I used responses to a question about the ZIP code of residence at the time of Harvey, suggesting that 8.3 percent (n = 50) of children had moved since, and perhaps because of, Harvey.
From the post-Harvey sample, I also use three binary measures for household-level exposure severity: disaster-induced household income loss (1 = yes, 0 = no), home damage or flooding (1 = limited, fair amount, or complete damage; 0 = no damage), and household life disruption because of Harvey (1 = life is still somewhat or very disrupted, 0 = not disrupted or mostly or fully back to normal). A summed score of the three binary measures (0–3) estimates household-level exposure severity (α = 0.68). Note that because these measures of household-level exposure may be endogenous to parents’ reports of children’s health, I consider these as associational and suggestive evidence. Nevertheless, I provide supplemental results that these household experiences in part explained the effect estimates that use ZIP code–level flooding.
Matching Procedure
Coarsened exact matching (CEM) is a nonparametric matching strategy to deal with imbalance on covariates across pre- and post-Harvey samples. CEM is increasingly preferred over other procedures because of its efficiency, unsensitivity to measurement error, and model independence. It uses an algorithm to first coarsen specific variable values and then match observations on the basis of those values (Iacus, King, and Porro 2009). I matched children on the basis of the aforementioned five child-level variables (race, gender, health insurance, age, and immigrant status), four household-level variables (homeownership, marital status, number of other children in the household, and poverty status), and two ZIP code–level variables (adult poverty from the 2013–2017 American Community Survey and flooding level from Hurricane Harvey). The matching procedure was highly effective at reducing imbalance to zero difference between pre- and post-Harvey both overall and within no or minimal flooding and flooded ZIP codes (see Online Appendix Table A1). However, this balance procedure came at the cost of pruning 31 percent of cases, resulting in a matched sample size of n = 742. I make this trade-off because, as explained later, it helps assure the identifying assumptions necessary for the DID quasi-experimental framework to be used to approximate causality.
Analytic Strategy
The analytic strategy proceeds in three stages corresponding to the research questions. First, I estimate the effect of Hurricane Harvey on a matched sample. I then examine potential mechanisms by including information from the adult informant on household-level exposure. I conclude by conducting a test for effect heterogeneity across sociodemographic groups, namely, race/ethnicity, nativity, poverty level, gender, and age.
I begin with a naive model that regresses children’s generalized health status on an indicator, Tij, for treatment status that takes 1 if in the treated sample (i.e., surveyed after Hurricane Harvey) and 0 otherwise. I then use a fixed-effect estimator that compares children’s health before and after Hurricane Harvey within ZIP codes, which serve as the neighborhood-level unit. Relative to other associational models, this strategy accounts for the socially patterned, spatial sorting into hazard-prone areas. I fit the following equation:

where yij is the parental report of generalized health for child i in ZIP code j. The vector
The third modeling strategy is used to approximate causality. I fit a DID estimator that identifies the effect of Hurricane Harvey using across–ZIP code variation in flooding level and temporal variation in survey timing. Using the dummy variable (D) that indicates a flooded ZIP code, children in the post-Harvey sample are assigned the category none or minimal (0) or flooded (1), and children in the pre-Harvey sample are assigned the corresponding placebo. I fit the following model predicting parent report of the health of child i in ZIP code j:

Here the parameter of interest is β3, which compare pre- with post-Harvey changes in children’s health in flooded neighborhoods to changes in children’s health in the neighborhoods with none or minimal flooding. In the DID framework, there are several threats to the estimator: unit stability, compositional differences, and divergent trends.
First, as mentioned above, for the post-Harvey sample I use the ZIP code of residence at the time of Harvey rather than the current ZIP code, which helps ensure that there was no contamination of the subsamples by exposure. Second, the framework assumes that comparable compositions across (D,
Mechanisms and Heterogeneity
I conduct two additional analyses to address the second and third research questions. The first assesses assess the adjusted associations between three household-level exposures and children’s health within neighborhoods. I reestimate equation 1 restricted to the postdisaster sample but recode Tij to each of the three household-level exposures (income loss, home damage, and household life disruption) to examine how within-neighborhood variation in exposure correlates with children’s health outcomes, net of a robust set of controls. The final analysis examines effect heterogeneity across subgroups. I include Eij as a continuous variable for the severity of household-level exposure (control sample coded 0) and interact it with each of the five subgroups, G (racial group, gender, age group, nativity, and poverty status). For each demographic subgroup (e.g., children ages 10–14 years), I estimate the group-specific association between exposure severity score and generalized health status, as indicated by β2.

Results
The embedded choropleth maps in Figure 1 show little spatial difference in the pre-Harvey (Figure 1A) and post-Harvey (Figure 1C) samples. At the ZIP code level, there was a strong correlation in the count of children across samples (r = .62), providing assurance against regional sampling bias. Figure 1B visualizes the coding of flooding across the 140 ZIP codes in the City of Houston and Harris County. The black dots display binned average outcomes for the pre-Harvey sample (85–0 days before Harvey) and blue dots for the post-Harvey sample (164-245 days later). The average generalized health status of children before and after the disaster was 4.26 and 4.14, respectively, on the 1-to-5 scale. In concordance with other studies, the vast majority of children were reported to have very good or excellent health. Comparing the two lines shows the naive estimated pre- to post-Harvey change of –0.12 on the 1-to-5 scale.

Temporal and spatial descriptive statistics: average generalized health status across time and sample concentration and flood coding across ZIP codes.
Table 1 presents the main effects of Hurricane Harvey on parental reports of their children’s generalized health status. The naive baseline estimate shows that on average, across Houston, children’s health declined by .461 points on the log-odds scale (p < .01). The fixed-effect model that identified the within-neighborhood average effect from survey timing reduced this estimate by about 5 percent. From this model, Hurricane Harvey was associated with a 0.440-point reduction in the log-odds scale of children’s health (p < .05). Holding all other variables at their means, the predicted probabilities for control children’s generalized health status were as follows: poor, .005; fair, .04; good, .15; very good, .23; and excellent, .58. For children after Harvey, the predicted probability for poor health was .008, for fair health .06, for good health .19, for very good health .26, and for excellent health .49. The next models recoded the outcomes of two binary measures and showed that within neighborhoods, the post-Harvey sample had a marginally significant decrease in the probability of having excellent health (p < .10) and a significant increase in the probability of having poor, fair, or good health (p < .05).
Estimates of the Effect of Hurricane Harvey on Children’s Generalized Health in Houston, 2017 to 2018 (n = 742).

Note: FE = fixed effect; GFP = good, fair, or poor.
p < .10. *p < .05. **p < .01.
I next estimate DID models that identify the effect by pairing neighborhood variation in flooding with the timing of the survey. Results are reported in Table 1, columns 5 to 7. Children in flooded neighborhoods experienced a significant .715-point reduction in the log-odds scale of parent-reported health. The coefficient, .505, on the flooded variable was marginally significant, suggesting better health in communities that would become flooded by Harvey. The two linear probability models showed more robust evidence that flooding decreased the probability of having excellent health relative to the other categories (coefficient = –.205, p < .05). Finally, although in the expected direction, the last model detected no significant change in the probability of good, fair, or poor health relative to very good or excellent health. Thus, across these associational and causal strategies, the evidence suggests that Hurricane Harvey led to worse health for children, in the probability of having excellent health, particularly in flooded communities.
Next, I examine potential mechanisms theorized to explain the effects of disasters on children. Table 2 reports within-neighborhood, adjusted associations between three Harvey-related household exposures and children’s health separately, followed by the exposure score as a summed measure in the fourth column. Because these models are estimated on solely the post-Harvey sample and not on the matched sample, I control for all factors used in matching. First, household income loss was marginally significantly associated with a .462-point reduction in the log-odds scale. Home damage was significantly associated with a .793-point reduction (p < .01) in the log-odds scale of health, and household life disruption was similarly associated with a .678-point reduction (p < .01). The summed score detected that each additional household exposure was strongly associated with a .471-point reduction in health (p < .001). As such, home damage and household life disruption, as well as a summed score of all three exposures, coincided most strongly with reductions in health. Importantly, Table A2 in the Online Appendix shows that the inclusion of the exposure score wholly (for the within-neighborhood model) and partially (for the DID model) explained away the effects in Table 1, providing further evidence that household-level exposure operated as a key mechanism.
Adjusted Associations between Harvey-Related Exposures and Children’s Generalized Health Status (n = 602).

Note: FE = fixed effect; HH = household.
p < .10. **p < .01. ***p < .001
Finally, to assess differences in the effect by subgroup, Figure 2 presents the predicted distributions of generalized health status within sociodemographic groups for those in the control group (pre-Harvey, thus zero exposures) and for those in the treatment group who were severely affected (post-Harvey, two exposures). Note that 24.3 percent of the post-Harvey sample experienced two or three exposures. The predicted outcomes are recovered from average marginal effects from equation 3, and the estimate provided in the right-hand column corresponds to the group-specific coefficient on the variable for number of household-level exposures. I find that the predicted change in health due to Harvey is similar and marginally significant when broken down by gender, with the estimated effect for girls (coefficient = –.245) as slightly, but not substantially larger than for boys (coefficient = –.226). Across age group, the effect was largest and statistically significant for those younger than 10 years (p < .05), the youngest age group examined. By racial groups, the effects for Hispanic (p < .05) and Asian or other-race children (p < .10) were the largest in magnitude, suggesting declines in health greater for these two groups. The estimated group-specific effect for White and Black children were indistinguishable from zero. I also detected that the effect of Harvey exposures was substantially large and significant for first generation children (foreign-born). This makes sense given Hispanic and Asian or other-race children are also considerably more likely to be among the foreign born in Houston. For first-generation immigrant children, each additional exposure was associated with a .620-point reduction on the log-odds scale of health (p < .05), while the estimated coefficient for native-born children was insignificant at –.173. Although the point estimates suggest a relatively larger decline among those above poverty, and a slightly positive relationship for those in poverty, neither estimate was distinguishable from zero. Importantly, even severely affected children living above poverty had better health than control children living in poverty. I return to this finding in the discussion.
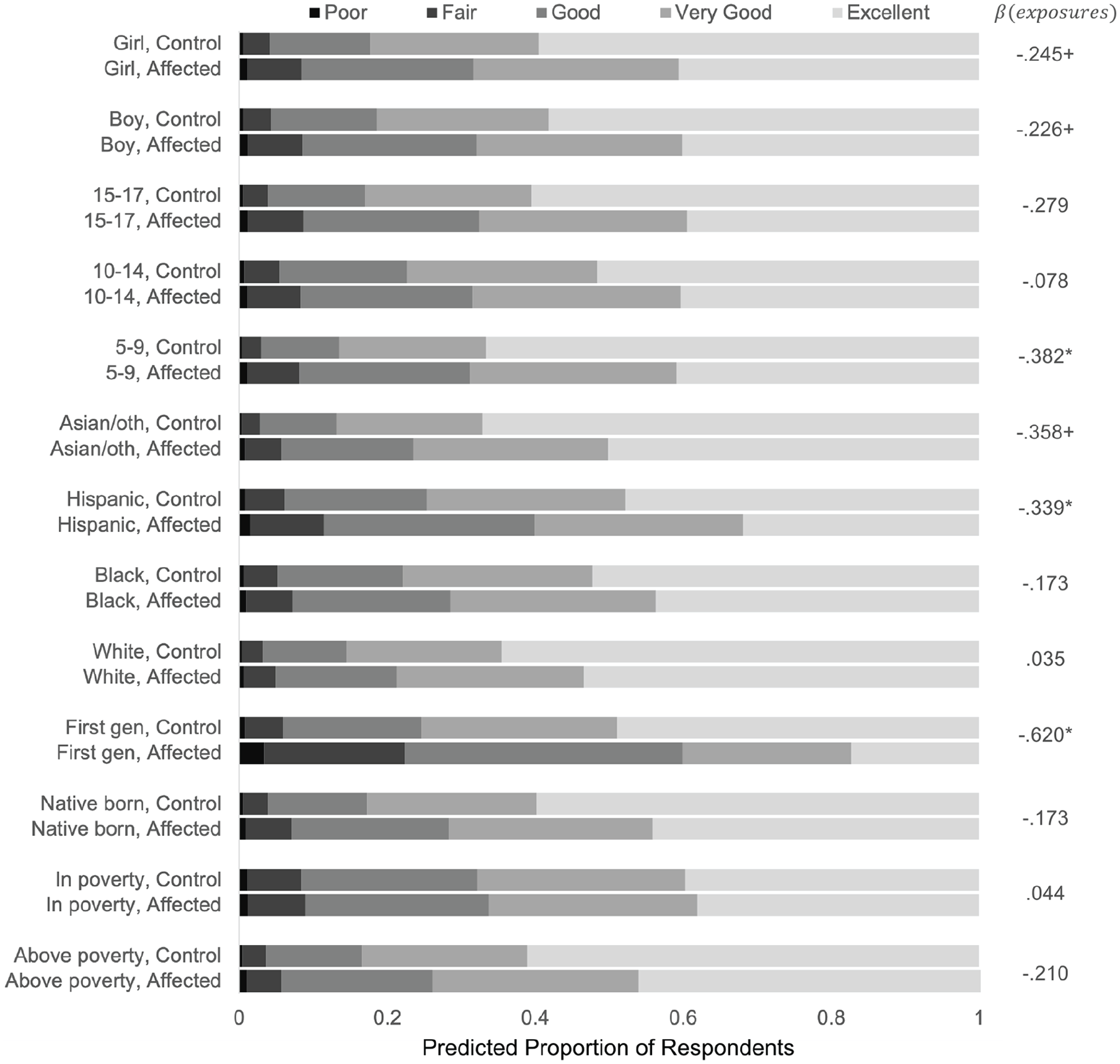
Predicted generalized health status across the control group and severely exposed, by demographic group.
Supplemental Analysis
The key untestable assumption in the DID estimator is that in the absence of Harvey, the trends over time in flooded and nonflooded communities would have been the same. To assess this, I conducted a placebo simulation study as a check for parallel trends using the pre-Harvey sample. I estimate the DID estimator at randomly selected dates from three days into surveying to August 24, 2017, which allows for sufficient pre- and post-Harvey placebo event samples. I simulate this model 300 times. The results are presented in Online Appendix Figure A1, which plots the point estimates and 95 percent confidence intervals for every simulated event. The mean estimate on the DID coefficient was .093 and fewer than 5 percent of the random events were statistically significant at p < .05 using two-tailed tests, providing evidence against divergent trends.
Discussion
In this article, I answer calls made by scholars for more research on exposure to disasters among children and adolescents (Anderson 2005; Peek et al. 2018) and on children in the context of climate change more broadly (Currie and Deschenes 2016). Applying statistical techniques to a natural experiment in a novel source of data, the findings report some of the first combined causal and associational estimates of exposure to a climate-related disaster on children’s health in the United States, building upon insights from prior work to address three research questions. First, results show that Hurricane Harvey led to poorer health for children in Houston as reported by their parents or guardians. Second, greater declines in health were experienced by children living in households that experienced home damage and disruption to normal functioning. Finally, associational evidence from within–ZIP code variation in household-level exposure severity suggests that immigrants, including Hispanic and Asian or other-race immigrants, and children younger than 10 years in Houston were particularly vulnerable to greater declines in health.
Indeed, Hispanics are the racial group most likely to reside in 100-year flood plains in Houston and therefore were mostly likely affected (Maldonado et al. 2016; Smiley 2020). According to the American Community Survey 2013–2017 estimates, the Hispanic population also had the highest poverty rate in Harris County at 23 percent. The use of Asian/other as a category was imperfect and heterogenous grouping. Still, journalistic reports suggest that Harvey exposure for the Vietnamese and Chinese communities may exacerbate health effects because of high rates of prior trauma and a large concentration of immigrants from these groups in Galveston Bay, which was highly affected (Najarro 2017). Importantly, low-income children had the poorest health before Hurricane Harvey. No substantive change in health among this group could be due to therapeutic community building (Drabek and McEntire 2003) but also potentially because other groups had “further to fall” in their health statuses, including the groups for whom the detected effects were the largest: young children and foreign-born children. The latter interpretation has been formalized as the Blaxter hypothesis, which posits that the most advantaged groups experience greater negative health consequences relative to the least advantaged groups (Blaxter 1990). As such, future research, especially those motivated by health disparities, should be attentive to the magnitude of effect estimates and to whether effects widen or depress health differences between groups. In the case of Hurricane Harvey, it is important to note that the worst flooded areas in Houston were middle class (Strochak and Ganesh 2017), a pattern that differs from other U.S. disaster cases such as Hurricane Katrina. Finally, my categorization of family poverty begets further inquiry to distinguish middle-class from upper-class families among those living above poverty.
I glean several theoretical insights by integrating the empirical findings with life-course theory and climate change science. First, given disasters’ increasing severity, sociologists would benefit from conceptualizing acute exposure to climate-related disasters as a life-course event, particularly for newer birth cohorts living in vulnerable parts of the United States, such as along the Gulf Coast. Relative to another event, an eviction, which is increasingly conceptualized as part of the life course for marginalized populations, my estimates for children’s health from the DID models were of similar magnitude, on the basis of a study by Hoke and Boen (2021). Second, I offer evidence that points to middle childhood as a potentially sensitive or critical period for exposure. Third, because early life conditions may matter for later life health (Hayward and Gorman 2004), childhood exposure to climate-related disasters may exacerbate health disparities within cohorts across the life course. In this population, I found that core axes of stratification were nativity and race/ethnicity. Finally, climate-related disasters should also be understood as a potential site for intergenerational disparities in health, as newer cohorts experience more extreme weather. Future research should interrogate the latter two implications with longitudinal data.
Several limitations are necessary to consider and point to future possible inquiries. First, this study relies on adult informants’ reports of children’s health, which may not entirely reflect how children experience their health (Bellman and Paley 1993). Yet the use of parental and school professional reports on children is common in studies of disaster (e.g., Lowe et al. 2013), and studies suggest that parental reports are reliable for children’s medical conditions and health service use (Pless and Pless 1995). Second, data were gathered on children in a narrow time window postdisaster, six to nine months later. Although this temporal distance from the event is common in previous studies (e.g., Lai et al. 2014), I could not estimate change across time, which is a relative strength of previous studies and may help test the implications of this study for health over the life course. Similarly, the narrow time frame of data collection meant that I could not account for seasonal trends in health, as month of year was perfectly colinear with pre- to post-Harvey treatment. This may bias the within-neighborhood estimator or the DID estimator only if seasonal trends varied by community flooding level. Future research should attend to seasonal change. Third, I used associational evidence to estimate correlations between exposure severity and sociodemographic group variation in health effects. Statistical power limited the ability to conduct the more rigorous triple differences analysis, another avenue for future research. Fourth, the health effects of climate-related disasters likely differ on the basis of the hazard, so these results may not generalize to health consequences linked to droughts or other chronic exposures such as sea level rise. Finally, given that the HHS was confined to the health of residents in the City of Houston and Harris County, my estimators may be biased by postdisaster migration out of Houston. However, the direction of this bias is not clear. On the one hand, children displaced outside of Houston may have been more likely to have worse health, which would understate the effect. On the other hand, children displaced outside of Houston may have been in better health, in which case I would have overstated an effect. Given research suggesting a mutually reinforcing relationship between poor health and residential displacement (Arcaya et al. 2014) and suggesting strong social pressure to remain among middle-class, and therefore likely healthier at baseline, residents (Rhodes and Besbris 2022), it seems probable that my estimates are conservative and understate a greater effect on children now living outside of Houston.
Shortly after Hurricane Harvey, Carroll and Frakt (2017) argued with the title of their commentary that “children must remain a focus in the recovery from Hurricane Harvey.” In this vein, my research also makes important contributions beyond a scholarly understanding of climate-related disasters and children’s health. For example, health care providers in Harris County would benefit from monitoring youth from immigrant backgrounds, namely, Hispanic and Asian or other-race children, from badly affected communities. For policy makers making decisions on disaster response, investments in resilient housing and quick-response FEMA aid for housing repair may help offset the adverse disruption that leads to children’s health problems. The findings also suggest that programs that allow a return to normalcy, such as through reopening of schools and a return to civic life, may have added benefits of promoting children’s health. Most important and beyond these adaptions, this research also identifies core health benefits to mitigating the emission of greenhouse gases that cause climate change and more extreme weather events such as Hurricane Harvey.
Supplemental Material
sj-docx-1-srd-10.1177_23780231221135971 – Supplemental material for Climate-Related Disasters and Children’s Health: Evidence from Hurricane Harvey
Supplemental material, sj-docx-1-srd-10.1177_23780231221135971 for Climate-Related Disasters and Children’s Health: Evidence from Hurricane Harvey by Ethan J. Raker in Socius
Footnotes
Acknowledgements
Thank you to Stephen Linder, Dritana Marko, and Robert Bozick for facilitating data access and for conversations about the project. I appreciate assistance from Paul Lesack and Evan Thornberry with the flood maps. This project was approved by University of British Columbia Research Ethics Board protocol H22-00318. Support during revisions came from the Peter Wall Institute for Advanced Studies. All errors are my own.
Supplemental Material
Supplemental material for this article is available online.
Notes
Author Biography
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.