
Abstract
Do migrants adopt the contraceptive norms dominant in their destination context? To explore this question, the authors adopt a multisited analysis in which they standardize and integrate data on women’s contraceptive use from two different sources: the Trajectoires et Origines survey collected in France (the receiving country) and the Demographic and Health Survey collected in Turkey (the sending country). Descriptive analyses indicate that contraceptive use of migrant women from Turkey in France is more comparable with that of nonmigrant women in France compared with nonmigrant women in Turkey. To address migrant selectivity on observed characteristics in multivariate analyses, nonmigrant groups in France and Turkey are reweighted with entropy balancing to resemble migrants on observed characteristics. Multivariate results indicate that there are sizable differences in contraceptive use between Turkish migrants and nonmigrant Turkish women, which undermines the hypothesis of selection on observables. Yet there are no significant differences between migrants and nonmigrant French women in contraceptive methods, thus supporting an adaptation perspective. Supplementary analyses highlight several pathways that could help explain these findings.
Contraceptive use is influenced by the wider social context in which individuals are embedded. International migration changes these contexts in important dimensions that are consequential to migrants’ subsequent reproductive and family lives. In the destination setting, migrants are exposed to information and norms about contraceptive methods (Lindstrom and Hernandez 2006), access to new health care infrastructure (Cotton 2019), employment opportunities that alter preferences for fertility regulation and abilities to act on those preferences (Bloom et al. 2009), and changing patterns of partnership formation (Betancourt, Colarossi, and Perez 2013; Boyle et al. 2008). These changes raise a host of questions: Do migrants adopt the contraceptive norms dominant in the destination? Alternatively, do premigration contraceptive practices continue to dominate migrants’ reproductive lives in the postmigration period? Is adoption of contraceptive methods (or lack thereof) linked to inequalities in migrants’ reproductive health care access? Or, alternatively, do norms and preferences learned in the origin shape migrants’ contraceptive choices?
Sociologists of migration have a long history of exploring processes of adaptation and acculturation among migrants. 1 Yet analyses of whether migrants adopt the contraceptive norms of the destination have been limited in important dimensions, in part because of data constraints (Tapales, Desai, and Leong 2019). Often surveys that collect information about sexual and reproductive health do not include oversamples of migrants, and surveys focused on migrants do not collect modules on sexual and reproductive health (Bilsborrow 2016; Tapales et al. 2019). 2 Furthermore, quantitative studies of the relationship between international migration and contraceptive use have focused primarily on destination contexts. For example, scholars have compared the contraceptive use of migrants to native-born residents of destination countries (Garcés-Palacio, Altarac, and Scarinci 2008; Iwarsson et al. 2019; Omland, Ruths, and Diaz 2014; Tapales, Douglas-Hall, and Whitehead 2018) or compared contraceptive use across migrant generations (Diaz et al. 2019; Poncet et al. 2013). Although these studies offer important insights, to fully understand whether migration is associated with contraceptive adaptation one would need to consider contraceptive use in countries of origin.
Ideally, a study of contraceptive adaptation would include longitudinal person-level information about contraceptive use among the same individuals before and after migration. Given that longitudinal studies of this sort are almost nonexistent, a next best approach is to adopt a multisited approach that include respondents from both origin and destination (Beauchemin 2014; Jiménez and Fitzgerald 2007). Micro-level empirical explorations of migrant reproduction that include information on respondents from both origin and destination countries have focused on fertility (Behrman and Weitzman 2022; Impicciatore, Gabrielli, and Paterno 2020; Lübke 2014; Singley and Landale 1998), but quantitative studies that conduct multisited analyses of migration and contraception outcomes have been more limited (Behrman et al. 2022; White and Potter 2013).
In this study, we conduct a multisited analysis of migration and contraceptive use by standardizing and integrating data on women’s contraceptive use from two different sources, one collected in France (the receiving country) and one collected in Turkey (the sending country). Our focus on Turkish migrants in France is particularly interesting because Turkey and France had similar rates of fertility and overall contraceptive use in the period of study, but vast differences in the types of contraceptive methods used (Bajos and Moreau 2018; Hacettepe University Institute of Population Studies 2009). Hormonal short-acting contraception (SAC) were the most widely used method in France, whereas traditional methods (particularly withdrawal) were the most used method in Turkey. Compared with traditional methods, modern methods are significantly more effective at preventing unintended pregnancies; while traditional methods such as withdrawal are effective with consistent and correct use (4 pregnancies per 100 women) and moderately effective with common use (20 pregnancies per 100 women), most modern methods—including implants, intrauterine devices (IUDs), oral contraceptives, injectables, and sterilization—are very effective with consistent and correct use (<0.6 pregnancies per 100 women) and very effective to effective with common use (World Health Organization 2018). 3 In addition, traditional methods such as withdrawal rely heavily on men’s actions (Kulczycki 2004), whereas modern methods—such as oral pills, implants, or IUDs—may allow women to have more control over their own bodies and fertility goals. 4
In our multivariate empirical analyses, we start by comparing the contraceptive outcomes of three groups of respondents: (1) migrant women from Turkey in France, (2) nonmigrant women in Turkey, and (3) nonmigrant women in France. To address migrant selectivity on observed characteristics, the latter two groups are reweighted with entropy balancing to resemble migrants from Turkey in France on observed characteristics. Our analysis shows how multiple data sources can be combined to provide important multisited insights into migrant contraceptive use when longitudinal data are not otherwise available. In doing so, we contribute to a growing literature that centers questions of migration and contraception in broader sociological conversations of migration as a social process. This type of analysis is crucial to better understand whether migrants can realize their contraceptive and reproductive goals on their own terms.
Factors That Influence Contraceptive Adaptation among Migrants
There are several reasons why migrants might adapt (or not adapt) to the contraceptive norms of the destination context. In what follows, we draw on extant literature to describe the different pathways that may facilitate or impede contraceptive adaptation among migrants. We group our explanation into four broad categories: (1) changes in contraceptive knowledge, (2) changes in contraceptive norms, (3) changes in contraceptive access, and (4) changes in contraceptive demand. It is important to note that these factors are often interrelated and interact with one another as they influence contraceptive trajectories.
Changes in Contraceptive Knowledge
Knowledge about the availability and efficacy of different types of contraceptive methods is an important predictor of contraceptive use among migrants (Garcés-Palacio et al. 2008). On one hand, new access to health care systems in the destination setting could be an important source of information. For instance, the French maternity system plays an important role in providing information about reproductive health to migrants (Sargent 2006). At the same time, migrants may gain knowledge about contraception through more informal channels, including traditional media (e.g., television, newspaper, radio), social media, public service campaigns, and social networks (Lindstrom and Hernandez 2006). Social networks in particular have been shown to be important channels for learning about new contraceptive methods (Kohler 1997) and for assessing the acceptability of contraceptive methods in contexts of uncertainty (Unger and Molina 1998). Although the presence of strong social networks can facilitate the transmission of information between newcomers and more established migrants (Kohler 1997; Unger and Molina 1998), the absence of social networks or migrant communities might leave new migrants in the dark about how to access contraception (White, Ocampo, and Scarinci 2017).
Changes in Norms
Migration may correspond with changes in norms about the acceptability of using contraceptive methods. In part, this could be because migration allows individuals to enter new social spaces, such as the workplace (Hirsch and Nathanson 2001), and become part of new social networks, which exposes migrants to new gender ideologies and norms (Maternowska et al. 2010). For example, migration may fundamentally change the importance women place on their fertility compared with women in origin countries (Hirsch and Nathanson 2001). Migration may also alter gender dynamics in important dimensions. As part of their migration experience, men may also become more likely to view reproduction as shared responsibility (Maternowska, Withers, and Brindis 2014), which may correspond with more egalitarianism in patterns of contraceptive decision making. However, migrants may also retain close connections to religious and social institutions from their origin country that may limit contraceptive use (Hirsch and Nathanson 2001; Sargent 2006). For example, Sargent (2006) examined Malian migrant women in France and found that the gendered discourse on contraception revolves around interpretations of Islam. She concluded that Malian migrant women weigh religious tenets, their husbands’ authority, and personal interest within the structural constraints of marriage, the migrant community, and the French maternity system.
Changes in Contraceptive Access
Women’s abilities to access effective methods of contraception such as the pill and IUDs is shaped by their abilities to navigate health care systems (White et al. 2017). Most of the scholarship that links health care access to contraceptive use among migrants focuses on destination contexts, such as the United States, where health care provision to migrants is often limited. For example, migrant Mexican women in the United States have lower use of effective contraceptive methods than nonmigrant counterparts in Mexico, which may be because migrants in the United States have limited eligibility for publicly funded contraceptive, whereas IUDs and female sterilization are accessible free of charge in Mexico (White and Potter 2013). As a result of limited access to health care systems in destinations, migrants may be likely to use the method that is most accessible even if it is not their preferred method (Alvarez-Nieto et al. 2015).
On the other hand, migration may be linked with increased access to health care, and thus more regular access to effective contraceptive methods, particularly in European destination settings characterized by universal health care schemes (Busse et al. 2006). 5 Nonetheless, migrants may remain unaware of their eligibility for subsidized family planning services (Maternowska et al. 2010). In addition, language barriers (Harari, Davis, and Heisler 2008) and lack of information about where to obtain contraception (Flippen and Schut 2022) can also hinder migrant women from using more effective methods of contraception.
Migration may also correspond with changes in earnings and employment, which can indirectly affect migrants’ abilities to afford contraception (particularly in settings that require a copay for more effective methods). At the same time, migrant women’s entry into paid employment may correspond with economic power and enhanced abilities to negotiate contraceptive use with their partners (Maternowska et al. 2010). Yet high costs of living in destination settings may necessitate women’s entry into labor force (Hirsch and Nathanson 2001) and provide a disincentive for pregnancy and thus a desire for fertility regulation. In fact, if the reason for migration is economic, pregnancy may be considered as “a failure” to migratory project (Alvarez-Nieto et al. 2015).
Changes in Demand
Migration changes lifecycles processes in ways that can have implications for contraceptive demand. For example, migration may correspond with partner separation for extended periods, which can disrupt contraceptive trajectories (Flippen and Schut 2022). In contexts in which migration for marriage is prevalent, a migration might signal the start of a new relationship and corresponding decisions about whether to start a family (Davin 1999). Some women may want to delay childbearing following a migration (thus desiring an uptake in contraception), whereas others may want to accelerate the transition into childbearing (thus preferring to limit contraception) (White et al. 2017). Ultimately, the relationship between births and migration is bidirectional: while births can be delayed because of migration, migration too can be initiated and delayed because of births (Lindstrom and Giorguli-Saucedo 2007).
Case Study Context
Turkey and France have significantly different cultural and political landscapes of sexuality and contraception. In what follows, we provide a brief overview of the contraceptive contexts in both settings.
Contraception in Turkey
The contraceptive prevalence rate was about 73 percent in Turkey in 2008 (the year data for our study was collected). 6 During this period, withdrawal (a traditional method) was the most widespread family planning method and was used by 26.2 percent of married women of reproductive age (Hacettepe University Institute of Population Studies 2009). The next most common types of contraception included the IUDs (17 percent), followed by male condoms (14 percent) and female sterilization (8 percent). On the other hand, use of the pill was fairly low (5 percent), which represents a major departure from the French context described later (Hacettepe University Institute of Population Studies 2009).
In the period of the study, public health centers, which were staffed with at least one family planning–certified physician and a midwife, were important providers of modern contraceptives such as IUDs, sterilization, and hormonal short-acting methods (Ozaydin et al. 2020). These health centers provided modern contraceptives free of charge and played an important role in providing family planning services to vulnerable groups such as migrants and uninsured individuals (Öcek et al. 2014). Pharmacies also played an important role in the provision (without a prescription) of male condoms, pills, and emergency contraception in Turkey (Karadon et al. 2021). Many unmarried women in Turkey reported preference to pay to obtain contraception at pharmacies rather than at free public health centers to avoid social stigmas related to premarital sexual activity (Karadon et al. 2021).
Questions remain about why reliance on traditional methods was so high in Turkey during this period given the widely available access to modern methods in public health centers or pharmacies. The enduring prevalence of withdrawal in Turkey likely reflected a combination of factors including social norms that positioned withdrawal as more “natural” and less “harmful” than hormonal methods, anxiety about the side effects of hormonal methods, the sanctioning of withdrawal by leaders in the religious establishment, and the perceived convenience of this method (Cindoglu, Sirkeci, and Sirkeci 2008; Karadon et al. 2021; Kulczycki 2004; Yanikkerem, Acar, and Elem 2006).
Contraception in France
Contraceptive use in France was almost universal among nonmigrant French women in the period of our study (Bajos et al. 2012; Vigoureux and Le Guen 2018). The pill has been the most widely used method in the French contraceptive system for the past 40 years (Roux 2021), which significantly differs from Turkey, where use of the pill is low. Heterosexual couples in France often rely upon condoms at early stages of sexual activity, transition to the pill when sexual life becomes more stable, and eventually adopt IUDs once desired family size has been achieved (Bajos et al. 2012, 2014; Le Guen et al. 2017). Although the proportion of pill users has decreased since the early 2000s, this has been offset by an increase in the use of other hormonal short-acting methods such as the contraceptive implant, patch, and vaginal ring (Bajos et al. 2012). In 2010, 45.0 percent of women aged 15 to 49 years used the pill, 4.6 percent used both the pill and condoms, 4.0 percent relied on other short-acting hormonal methods (including implants [2.6 percent], vaginal rings [1.0 percent], and contraceptive patches [0.4 percent]), 20.7 percent used IUDs, 12.2 percent used condoms, 6.2 percent used other methods such as withdrawal or the rhythm method, and 4.2 percent used contraceptive sterilization 7 (Bajos and Moreau 2018).
Although condoms are widely and cheaply available for purchase commercially in France, most of the widely used modern contraceptive methods in France—including the pill, implants, and IUDS—require outside medical intervention in the form of a prescription or insertion by a trained medical professional (Le Guen et al. 2017, 2020). The French health care system, a universal system financed by government national health insurance, reimburses the cost of contraceptives that require outside medical intervention (Bajos et al. 2014).
Access to highly effective forms of contraception is widely available to migrants through public health care schemes in France (André and Azzedine 2016). Documented migrants have full access to the publicly subsidized French health care system via common-law benefits and thus have access to short-acting hormonal contraceptives or long-acting reversible contraception (LARC). Undocumented migrants are eligible for state medical aid (aide médicale de l’etat), which is a more limited form of health care coverage available to those who have resided in France for an uninterrupted period of three months (Makooi and Wallis 2019). State medical aid nonetheless covers costs of contraception and abortion for undocumented migrants, thus ensuring that undocumented population have access to a range of reproductive health services. Yet there may be barriers to accessing state medical aid for migrants, such as the additional administrative costs and reimbursement periods that may discourage health care professionals from treating state medical aid–insured patients, the difficulty of proving that an applicant has resided in France for an uninterrupted period of three months, and varying practices of the health insurance local branches, which are responsible for processing state medical aid applications (Wittwer et al. 2020).
Migration to France from Turkey
In contemporary France, migrants born in Turkey constitute 4.3 percent of all immigrants in France (~175,000 people) (Insee 2017). Scholars have pointed to a combination of both economic and cultural factors, including the large Turkish diaspora, as important determinants of sustained emigration from Turkey to France and other European countries (Dedeoğlu and Genç 2017). The historical trajectory of large-scale Turkish migration to France started in the period following World War II. As part of the bilateral labor agreements, a large population of male labor migrants from Turkey migrated to France and other European countries in the 1960s, a period referred to as the “guest worker” era of migration (Akgündüz 2008; Danış and İrtiş 2008). The guest worker period ended with the economic downturns of the 1970s and the French government made active efforts to encourage return migration and discourage labor migration. Nonetheless, many Turkish migrants opted to stay in France and were able to bring wives and extended family members through family reunification policies, which became a dominant channel through which new immigrants came to France in the 1970s and 1980s (Laurence and Vaisse 2006). From the 1980s onward, many political asylum seekers from Turkey migrated to France, especially after the coup in 1980 and political disputes in the eastern and southeastern regions in Turkey in the 1990s (Danış and Üstel 2008). Accordingly, migration between Turkey and Europe was defined largely by state repression, political exile, and Kurdish separatism in the 1980s and 1990s (Adamson 2019).
Data and Sample
We incorporate existing data from two distinct data sources: the Trajectoires et Origines (TeO) survey and the Demographic and Health Survey (DHS). TeO is a cross-sectional, nationally representative survey of respondents in metropolitan France that includes an oversample of immigrants. TeO was collected by the French Institute for Demographic Studies and the French National Institute of Statistics and Economic Studies between September 2008 and February 2009. The DHS is a standardized cross-sectional survey that is nationally representative of women of reproductive ages (15–49 years) collected throughout the world by host country governments in collaboration with ICF International. We use the DHS survey wave from 2008 for Turkey. We create standardized variables that are consistent across TeO and the DHS and append the two data sources to create a harmonized data set. This enables comparisons of migrant women in France to nonmigrant women in Turkey and to nonmigrant women in France who are comparable on observed characteristics such as education and age.
Our sample is composed of nonpregnant married women of reproductive age (15–45 years). We focus on married women because the Turkey DHS interviews only ever-married women, 95 percent of whom are currently married. The analytical sample is defined using listwise deletion (see Table A1 in the Appendix for more details) and includes three categories of respondents. First are married nonmigrant women in Turkey, who are surveyed through the DHS (n = 5,650). This group excludes return migrants who are in Turkey after living abroad (n = 85). Second are married migrant women from Turkey who arrived in France at age 15 or older, who are surveyed through TeO (n = 141). We exclude Turkish migrant women who arrived before the age of 15 (n = 84) because the 1.5 generation is qualitatively different (Milewski 2007, 2010). Although the migrant sample size is small, these are roughly consistent with small samples of migrants common in the literature (Wolf and Mulder 2019). Third are married, native-born (i.e., no history of migration in the past two generations) women in France, who are also surveyed through TeO (n = 817). Because of high rates of nonmarital cohabitation in France, the “married category” in the TeO data is composed of both married and cohabiting respondents (for both Turkish women in France and French women), though for simplicity we refer to them as “married.”
Measures
Contraceptive Outcomes
Our analyses consider the range of contraceptive outcomes reported by respondents in our sample. This includes an indicator for current use of traditional methods (withdrawal, rhythm methods, lactational amenorrhea), an indicator for current use of coital SAC (condoms, diaphragms, cervical caps), an indicator for current use of hormonal SAC (oral contraceptive pills and injectables), an indicator for current use of LARC (implants and IUDs), and an indicator for female sterilization. 8 In cases of multiple reported contraceptive methods, the DHS uses the most effective method as the main method. The TeO sample is recoded to correspond (i.e., 1 migrant respondent and 13 French respondents report using two contraceptive methods and are recoded to the most effective method). Details about variable standardization can be found in Table A2.
Migration Status
Our analysis defines respondents as (1) migrant women from Turkey in France, (2) nonmigrant women in Turkey, and (3) nonmigrant women in France with no family histories of migration in the past two generations.
Background Characteristics
To account for the ways in which migrants differ from nonmigrant women in France and Turkey on observed characteristics, we control for the following measures 9 : an indicator for respondent education (secondary school or higher vs. less than secondary school), indicators for the education of the respondent’s mother (less than primary, secondary or higher, education unknown), indicators for the education of the respondent’s father (less than primary, secondary or higher, education unknown), indicators for respondent’s sibling size (zero, one, two, three, four, five or more), an indicator for whether the respondent reports Kurdish ethnic origin, indicators for age in five-year groupings, a continuous measure of current parity, an indicator for whether the respondent expresses a desire to get pregnant in the near future (i.e., the next 12 months or sooner), a dichotomous indicator for whether the respondent is currently employed, a dichotomous indicator for whether the respondent currently has health insurance, a continuous measure of the respondent’s ideal family size, and a dichotomous indicator for whether the respondent currently wears a religious symbol or visible religious item. 10 Details about variable coding and standardization between the DHS and TeO can be found in Table A2.
Methods
We start by asking whether the contraceptive patterns of migrants from Turkey in France resemble those of nonmigrant women in Turkey or native-born nonmigrant women in France. To this end, we provide a multisited, micro-level descriptive comparison of levels of contraceptive use for migrant women in France, nonmigrant women in Turkey, and nonmigrant women in France. We hypothesize that adaptation will be supported if the contraceptive patterns of migrants from Turkey in France more closely resembles those of nonmigrant women in France than nonmigrant women in Turkey. Nonetheless, this descriptive exercise provides a rudimentary assessment of adaptation that does not consider the fact that migrants are a selected group who may be different on observed characteristics from both women in origin and destination settings.
To explore whether there is evidence of adaptation after accounting for observed differences between migrants and counterparts in origin and destination, we run a series of multivariate linear regressions that explore the association between migration and contraceptive use among two subsamples of respondents: (1) migrants from Turkey in France (treatment) versus nonmigrant women in Turkey (control 1) and (2) migrants from Turkey in France (treatment) versus nonmigrant women in France (control 2). To account for the ways in which migrants differ in observed dimensions from women in origin and destination contexts, both control groups are reweighted to resemble migrants from Turkey in France on background characteristics in multivariate models.
We use an entropy balancing approach to conduct the reweighting (Hainmueller and Xu 2013; King and Nielsen 2019; Zhao and Percival 2017). Entropy balancing is a method used to match treatment and control assignments that differ on observed background characteristics. Conceptually, entropy balancing is similar in spirit to propensity score matching, whereby an artificial control group is created by matching each treated unit with a nontreated unit of similar characteristics. Given our small sample size of migrant respondents, entropy balancing is preferable for our purposes compared with propensity score matching or other matching strategies (such as coarsened exact matching) because it does not need a large sample size or drop segments of the sample where there is no overlap between treatment and control.
To conduct the entropy balancing exercise, we specify a set of balance conditions (e.g., the mean background characteristics of the control group needs to match those of the treatment group). An entropy balancing algorithm is used to find a set of matching weights that best fulfills the given conditions (implemented using the ebalance command in Stata 17). We then conduct a multivariate regression analysis of the association between migration and contraceptive outcomes using the matching weights to ensure the control group resembles the treated group on observed characteristics. In this case, our treatment is “migration from Turkey to France,” and we have two different control groups (French nonmigrants in France and Turkish nonmigrants in Turkey), so we construct two different sets of entropy weights.
We hypothesize that there will be evidence supportive of adaptation if observed background differences between treatment and control groups fail to explain differences in contraceptive use. To the contrary, if observed background differences between groups explains differences in contraceptive use, this suggests that selection on observed characteristics, not adaptation, accounts for differences between groups. The biggest limitation of this approach is that we cannot account for unobserved ways in which migrants differ from respondents in the two control groups (which is taken up in further detail in the “Discussion” section).
Results
Descriptive Overview of Contraceptive Patterns of Migrants from Turkey in France, Nonmigrant Women in France, and Nonmigrant Women in Turkey
To start, we provide a descriptive overview of contraceptive use among migrants from Turkey in France, nonmigrant women in France, and nonmigrant women in Turkey. The patterns observed in Table 1 for nonmigrants in Turkey and France are consistent with well-documented patterns of contraceptive use in each country described in the preceding section. Among partnered women of reproductive age in France, the majority (81 percent) of women in our sample are currently using contraception. Hormonal short-acting methods dominate (47 percent), followed by LARC (23 percent) and condoms (5 percent). Both sterilization and traditional methods are quite low (about 1 percent each). Likewise, in Turkey the majority (78 percent) of partnered women of reproductive age in our sample are using contraception at the time of survey. Yet, in contrast to what is observed in France, among women in Turkey, traditional methods are the most widely used method (30 percent), followed by LARC (19 percent) and coital methods (17 percent). Hormonal methods are significantly less prevalent among women in Turkey (7 percent). Even though sterilization (9 percent) is also low in Turkey compared with other methods, this is still higher than the rate among French women.
Descriptive Statistics Comparing Married Turkish Migrants in France with Turkish Women in Turkey and French Women in France.

Note: All measures are dichotomous except living children (range = 0–14), ideal family size (ranges = 0–33), siblings (ranges = 0–14), and wife age (range = 15–45). Weighted using sampling weights provided by the Demographic and Health Survey and Trajectoires et Origines. Numbers in boldface type indicate statistically significant difference (p < .05) between Turkish migrants in France and the subsample in question.
Table 1 demonstrates that 70 percent of Turkish migrants in France in our sample are using contraception. Overall, the contraceptive use of migrants from Turkey in France appears to resemble more closely that of nonmigrant women in France than nonmigrant women in Turkey in two major respects. First, like nonmigrant women in France, the most common contraceptive method among migrants from Turkey in France is hormonal SAC (35 percent). Second, use of traditional methods is low among migrants (2 percent), which is significantly lower than among nonmigrant women in Turkey. Reliance on sterilization and coital SAC among migrants (5 percent and 2 percent, respectively) are also lower than among their nonmigrant counterparts in Turkey, although differences in LARC use among the three groups are not as dramatically different from each other. It is worth noting that the percentage of Turkish migrants who are not using contraception (30 percent) is significantly higher than that of Turkish women in Turkey (19 percent) or French women in France (22 percent). This is a striking finding, especially given that Turkish migrants in France are significantly less likely than the other two groups to report that they would like to have a child in the next year. 11
Multivariate Analyses of the Association between Migration and Contraceptive Use Comparing Migrants from Turkey in France to Nonmigrant Women in Turkey
On one hand, migrants from Turkey in France appear to have contraceptive behavior that is more like nonmigrant women in France than nonmigrant women in Turkey, which supports the idea that migrants adapt to the contraceptive norms of destination. On the other hand, Table 1 does not account for the observed ways in which migrant women differ from their nonmigrant counterparts in Turkey. As Table 1 also shows, migrant women from Turkey in France are significantly more likely than nonmigrant women in Turkey to have progressed beyond primary school and more likely to have parents who have progressed beyond primary school. Given that migrants constitute a selected group, it is plausible that they would have had different contraceptive use irrespective of migration.
To explore whether differences in observed characteristics explain the differences in contraceptive use between migrant women from and nonmigrant women in Turkey, we reweight women in the origin country to resemble their migrant counterparts on observed background characteristics. Multivariate analyses in Table 2 show that migration to France is associated with dramatic differences in women’s contraceptive use when nonmigrant women in Turkey are reweighted to resemble migrant women from Turkey in France on observed characteristics. Consistent with the patterns observed in Table 1, migration from Turkey to France is associated with a 27 percentage point higher probability of currently using hormonal SAC (p < .001) and a 24 percentage point lower probability of currently using traditional methods of contraception (p < .001). Migration is also associated with 11 and 7 percentage point lower probabilities of using coital SAC and sterilization, respectively, although there are no significant differences in LARC use by migration status. Taken together, these results suggest that selection into migration on observed characteristics does not explain the differences in contraceptive use between Turkish migrants in France and women in Turkey.
Multivariate Analysis of the Association between Migration and Contraceptive Use Using Entropy Weights to Make Turkish Women in Turkey Resemble Turkish Migrants to France on Observed Characteristics.

Note: Values in parentheses are robust standard errors. Linear probability model: Models include controls for respondent education, age, number of siblings, parity, ideal family size, preference for childbearing soon, employment, health insurance, religious symbol, maternal education, paternal education, and Kurdish origin. LARC = long-acting reversible contraceptive; SAC = short-acting contraceptive.
p < .001.
Multivariate Analyses of the Association between Migration and Contraceptive Use Comparing Migrants from Turkey in France to Nonmigrant Women in France
Although migrants from Turkey have contraceptive use that looks descriptively more like that of nonmigrant women in France than nonmigrant women in Turkey, there are nonetheless important differences between the two groups. For example, hormonal SAC use (the most prevalent method for both groups) was 12 percentage points higher among nonmigrant women in France compared with migrants from Turkey in our baseline estimates in Table 1. Likewise, migrants from Turkey have lower levels of schooling than nonmigrant women in France, come from larger families, and have parents with lower levels of schooling (Table 1). To explore whether differences in observed characteristics explain the differences in contraceptive use between migrant and nonmigrant women in France, we reweight women in France to resemble migrant women from Turkey on observed background characteristics (Table 3).
Multivariate Analysis of the Association between Migration and Contraceptive Use Using Entropy Weights to Make French Women in France Resemble Turkish Migrants to France on Observed Characteristics.

Note: Values in parentheses are robust standard errors. Linear probability model: Models include controls for respondent education, age, number of siblings, parity, ideal family size, preference for childbearing soon, employment, health insurance, religious symbol, maternal education, and paternal education.
Multivariate analyses presented in Table 3 show that migration from Turkey to France is associated with no significant differences in traditional, coital SAC, LARC, hormonal SAC, or sterilization methods when nonmigrant women in France are reweighted to resemble migrant women from Turkey on observed characteristics (i.e., coefficients on these point estimates are small in magnitude and results are not statistically significant at p < .05). The fact that there are no significant differences in contraceptive use once we account for observed background differences between migrant women in our sample and nonmigrant women in France is supportive of an adaptation perspective. Table 1 provides additional information on the factors might contribute to adaptation. It is worth noting that access to health insurance is almost universal among both Turkish migrants in France (99 percent) and French women (100 percent). Given that health insurance is important for accessing hormonal SAC (Le Guen et al. 2017), this suggests that integration into the French health care system might play an important role in the high levels of hormonal short-acting methods seen among Turkish migrants. Similarities in health care coverage are particularly striking given that in other dimensions the groups are quite different. For example, significantly higher proportions of French women are employed (81 percent) compared with Turkish migrants in France (24 percent), and Turkish migrants on average have more children (2.39) compared with French women (1.56).
Discussion
At the beginning of this article, we posed a question: do migrants adapt to the contraceptive norms of the destination context? In the absence of panel data, we constructed a multisited data set that matched Turkish migrants in France to nonmigrant French and Turkish women who were comparable on observed characteristics. Our multivariate results yielded several findings of interest. First, there was little evidence that migration was associated with differences in the probability of use of LARC when Turkish migrants in France were compared with either Turkish women in Turkey or native French women. We suspect this finding relates to the fact that public health care systems in both countries made LARC widely accessible to women in both origin and destination settings. In this respect, our findings differ from studies of Mexican migrants in the United States, where lack of access to affordable highly effective contraception has been cited as a potential reason for lower levels of highly effective contraception such as LARC among migrants compared with women in Mexico (White and Potter 2013).
Second, we found that Turkish migrants in France had significantly higher probabilities of using hormonal SAC methods compared with Turkish women in Turkey though no significant differences in the probability of hormonal short-acting methods compared with French women. These results are generally supportive of the contraceptive adaptation perspective and could reflect that the French health care system promoted hormonal SAC, whereas use of hormonal SAC was much less prevalent in Turkey at the time of study. At the same time, Turkish migrants had significantly lower probabilities of relying upon traditional methods, sterilization, or coital SAC methods compared with Turkish women in Turkey (though there was no evidence of significant difference in the probability of using these methods when Turkish migrants were compared with French women in France). Once again, these results align with the contraceptive adaptation perspective given that sterilization and reliance on traditional methods were both more prevalent in Turkey at the time of study then in France.
Although we hypothesize that integration into the French health care system may play an important role in the uptake of hormonal SAC and continued use of LARC, additional information is needed to fully unpack the mechanisms through which this may occur. Future qualitative research should explore in further detail how women navigate the health care system and in turn how they made contraceptive decisions. For example, what role to health care workers play in providing new and helpful contraceptive knowledge? Were migrants’ interactions with health care workers positive experiences or was there evidence of coercion? Does heightened use of hormonal SAC among Turkish migrants reflect informed choices or pressure from the medical establishment? It is also important to acknowledge that a range of other factors may have influenced migrant women’s contraceptive use including access to new social networks and employment opportunities and more general processes of adaptation and incorporation into new social institutions.
The biggest limitation of our analysis is that we could not account for unobserved selectivity into migration on factors such as gender ideology or religiosity that might have predicted both propensities to migrate and to use modern contraception. Considering the above, we cannot definitively establish whether migration affected contraceptive adaptation; instead, we emphasize that our results are suggestive of contraceptive adaptation. There is a need for more multisited data on a wide range of reproductive health outcomes that includes contraception including longitudinal studies or combination of multiple data sources when panel data are not available.
In addition, we should also note the important changes in the political and policy landscape in both Turkey and France over the past decade, which are likely to influence the trends since the data were collected. For example, the implementation of the Health Transformation Program in Turkey in 2010 likely decreased the provision of family planning services (Öcek et al. 2014; Ozaydin et al. 2020). 12 Researchers have also suggested that the broad conservative turn in Turkey has undermined the autonomy of sexual health policy by subjecting it to population policy (Yilmaz and Willis 2020), and “politics of the intimate” that overemphasizes motherhood and procreation (Acar and Altunok 2013) has likely affected service delivery at the institutional level (MacFarlane et al. 2016). Similarly, we should note the increased political polarization in France in the recent years, with far-right candidates using anti-immigrant sentiment and calling for less state aid for migrants (News Wires 2022). Yet there have also been important policy updates in France which are likely to improve the contraceptive landscape, such as the implementation of free birth control to all women up to age 25 starting in 2022 (Associated Press 2021). 13 This policy change is particularly important in light of the French pill scare in 2012 and 2013, 14 after which contraceptive trajectories became more diverse among French women (Bajos et al. 2014), which also created new social inequalities in accessing medical contraceptives (Le Guen et al. 2020).
Our study makes clear a need for a more serious consideration of contraceptive and other reproductive health outcomes in sociological scholarship on migration processes. At the same time, our study illuminates the importance of ensuring that migrant populations have full access to a range of highly effective contraceptive methods. Yet it is also crucial that scholars and policy makers alike adopt a reproductive justice framework that supports migrant women’s reproductive wishes and allows them to make informed decisions on their own terms. Such a perspective is particularly important given the politicization of migrant fertility and past uses of family planning as a tool for the population control of migrant populations (Amiri 2020; Manian 2020). Providing widely available and accessible reproductive health care in which migrants have comparable health care coverage as nonmigrant residents is key to achieving these goals.
Footnotes
Appendix
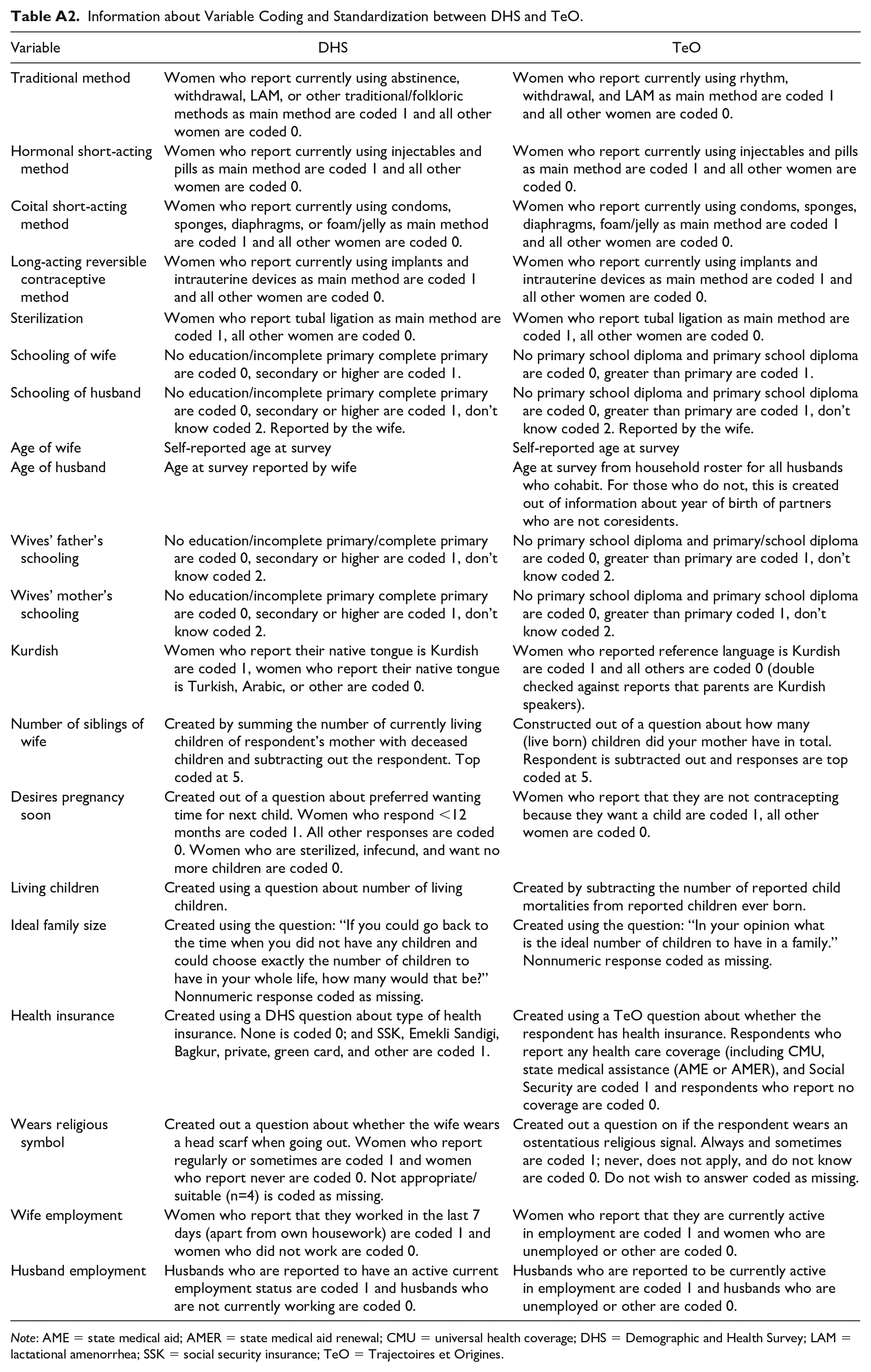
Information about Variable Coding and Standardization between DHS and TeO.
| Variable | DHS | TeO |
|---|---|---|
| Traditional method | Women who report currently using abstinence, withdrawal, LAM, or other traditional/folkloric methods as main method are coded 1 and all other women are coded 0. | Women who report currently using rhythm, withdrawal, and LAM as main method are coded 1 and all other women are coded 0. |
| Hormonal short-acting method | Women who report currently using injectables and pills as main method are coded 1 and all other women are coded 0. | Women who report currently using injectables and pills as main method are coded 1 and all other women are coded 0. |
| Coital short-acting method | Women who report currently using condoms, sponges, diaphragms, or foam/jelly as main method are coded 1 and all other women are coded 0. | Women who report currently using condoms, sponges, diaphragms, foam/jelly as main method are coded 1 and all other women are coded 0. |
| Long-acting reversible contraceptive method | Women who report currently using implants and intrauterine devices as main method are coded 1 and all other women are coded 0. | Women who report currently using implants and intrauterine devices as main method are coded 1 and all other women are coded 0. |
| Sterilization | Women who report tubal ligation as main method are coded 1, all other women are coded 0. | Women who report tubal ligation as main method are coded 1, all other women are coded 0. |
| Schooling of wife | No education/incomplete primary complete primary are coded 0, secondary or higher are coded 1. | No primary school diploma and primary school diploma are coded 0, greater than primary are coded 1. |
| Schooling of husband | No education/incomplete primary complete primary are coded 0, secondary or higher are coded 1, don’t know coded 2. Reported by the wife. | No primary school diploma and primary school diploma are coded 0, greater than primary are coded 1, don’t know coded 2. Reported by the wife. |
| Age of wife | Self-reported age at survey | Self-reported age at survey |
| Age of husband | Age at survey reported by wife | Age at survey from household roster for all husbands who cohabit. For those who do not, this is created out of information about year of birth of partners who are not coresidents. |
| Wives’ father’s schooling | No education/incomplete primary/complete primary are coded 0, secondary or higher are coded 1, don’t know coded 2. | No primary school diploma and primary/school diploma are coded 0, greater than primary are coded 1, don’t know coded 2. |
| Wives’ mother’s schooling | No education/incomplete primary complete primary are coded 0, secondary or higher are coded 1, don’t know coded 2. | No primary school diploma and primary school diploma are coded 0, greater than primary coded 1, don’t know coded 2. |
| Kurdish | Women who report their native tongue is Kurdish are coded 1, women who report their native tongue is Turkish, Arabic, or other are coded 0. | Women who reported reference language is Kurdish are coded 1 and all others are coded 0 (double checked against reports that parents are Kurdish speakers). |
| Number of siblings of wife | Created by summing the number of currently living children of respondent’s mother with deceased children and subtracting out the respondent. Top coded at 5. | Constructed out of a question about how many (live born) children did your mother have in total. Respondent is subtracted out and responses are top coded at 5. |
| Desires pregnancy soon | Created out of a question about preferred wanting time for next child. Women who respond <12 months are coded 1. All other responses are coded 0. Women who are sterilized, infecund, and want no more children are coded 0. | Women who report that they are not contracepting because they want a child are coded 1, all other women are coded 0. |
| Living children | Created using a question about number of living children. | Created by subtracting the number of reported child mortalities from reported children ever born. |
| Ideal family size | Created using the question: “If you could go back to the time when you did not have any children and could choose exactly the number of children to have in your whole life, how many would that be?” Nonnumeric response coded as missing. | Created using the question: “In your opinion what is the ideal number of children to have in a family.” Nonnumeric response coded as missing. |
| Health insurance | Created using a DHS question about type of health insurance. None is coded 0; and SSK, Emekli Sandigi, Bagkur, private, green card, and other are coded 1. | Created using a TeO question about whether the respondent has health insurance. Respondents who report any health care coverage (including CMU, state medical assistance (AME or AMER), and Social Security are coded 1 and respondents who report no coverage are coded 0. |
| Wears religious symbol | Created out a question about whether the wife wears a head scarf when going out. Women who report regularly or sometimes are coded 1 and women who report never are coded 0. Not appropriate/suitable (n=4) is coded as missing. | Created out a question on if the respondent wears an ostentatious religious signal. Always and sometimes are coded 1; never, does not apply, and do not know are coded 0. Do not wish to answer coded as missing. |
| Wife employment | Women who report that they worked in the last 7 days (apart from own housework) are coded 1 and women who did not work are coded 0. | Women who report that they are currently active in employment are coded 1 and women who are unemployed or other are coded 0. |
| Husband employment | Husbands who are reported to have an active current employment status are coded 1 and husbands who are not currently working are coded 0. | Husbands who are reported to be currently active in employment are coded 1 and husbands who are unemployed or other are coded 0. |
Note: AME = state medical aid; AMER = state medical aid renewal; CMU = universal health coverage; DHS = Demographic and Health Survey; LAM = lactational amenorrhea; SSK = social security insurance; TeO = Trajectoires et Origines.
Acknowledgements
This work is supported by grant SES 1918274 from the National Science Foundation to Drs. Julia Behrman and Abigail Weitzman and is also supported by grant P2CHD042849, Population Research Center, awarded to the Population Research Center at the University of Texas at Austin by the Eunice Kennedy Shriver National Institute of Child Health and Human Development. The funding sources had no role in the study design; collection, analysis, and interpretation of data; writing of the report; or the decision to submit the report for publication. We are grateful to Centre Maurice Halbwachs for granting access to the data (Trajectoires et origines [TEO]—version complete—2008: [2008, fichier electronique], INED et INSEE (producteur), Centre Maurice Halbwachs [CMH, diffuseur]). We are thankful to Michelle Eilers and Isabel McLoughlin Brooks for excellent research assistance.