
Abstract
Prior research has shown the theoretical importance and empirical feasibility of health lifestyles but has not examined their patterns over the life course or their dynamic associations with socioeconomic status (SES) and adult roles. The authors develop and apply a life-course approach to understanding individuals’ health lifestyles across the transition to adulthood, using U.S. data from the National Longitudinal Study of Adolescent to Adult Health (n = 6,863). The results show that ascribed SES is associated with adolescent health lifestyles, and those health lifestyles are associated with later health lifestyles. The results also demonstrate the developmental specificity of health lifestyles. Dissimilarities and variations in the clusterings of behaviors and their associations with SES, along with patterning of adult roles, support a contextualized, life course–focused interpretation of health lifestyle development. The authors highlight the need for an integrated life-course model of the development of health disparities that combines both stability and change.
Like income inequality, socioeconomic disparities in health and mortality have widened in the past 20 years (Sasson and Hayward 2019). Although macrolevel and institutionalized factors are important for understanding growing inequalities, health behaviors and lifestyles have also contributed. Research has demonstrated a strong and robust association between health behaviors and socioeconomic status (Cutler and Lleras-Muney 2010; Lawrence 2017; Pampel, Krueger, and Denney 2010). Compared with college graduates, those without high school diplomas are almost 4 times as likely to currently smoke, nearly 5 times as likely to abstain from exercise, and, reflecting diet and physical activity behaviors, nearly twice as likely to be obese (Pampel et al. 2010).
Perhaps more disconcerting, however, is the increase in disparities: the least educated have increasingly compromised health compared with their more highly educated counterparts. Among some subgroups, those with the lowest education appear to be living shorter lives compared with 20 years ago (Case and Deaton 2017; Sasson and Hayward 2019). Alcohol, drugs, suicide, and heart disease are culprits in the recent mortality rise (Case and Deaton 2017; Masters, Tilstra, and Simon 2018), but poor diet, obesity, and limited exercise have also become increasingly concentrated among lower socioeconomic groups, contributing to health inequalities (Chetty et al. 2016).
Despite convincing evidence of growing health inequalities and the role health behaviors play, we know little about how socioeconomic differences in health behaviors emerge. Global forces affecting employment and economic opportunities and general trends in income inequality certainly affect health (Truesdale and Jencks 2016) but say little about why individuals with different socioeconomic status engage in different health behaviors. Research has examined the influence of factors that mediate the relationship between education and healthy behavior (Cutler and Lleras-Muney 2010) and focused on isolating the causal impact of education (Lawrence 2017). We seek to extend this microlevel approach with two additional insights. First, we argue that separate health behaviors can be better understood when viewed as part of a person’s underlying health lifestyle. Second, we bring the life-course perspective (Elder 1994; Ferraro and Shippee 2009) more explicitly to bear in understanding the emergence of socioeconomic inequalities in health lifestyles in early life.
Conceptualizing health behaviors as part of broader, underlying health lifestyles can shed light on the relationship between socioeconomic status (SES) and health behavior. Health lifestyles are clusters of health behaviors within individuals that are rooted in group-based identities and norms (Cockerham 2005). Documenting how individuals adopt different health lifestyles and express identities and social class through them links health behaviors that are otherwise treated as distinct, offering a more integrated perspective on health disparities.
Inequalities in health lifestyles among adults emerge over the life course, which means that a full understanding requires attention to early life when these lifestyles form (Elder 1998). In the transition to adulthood, individuals transcend the influence of their parents to adopt their own identities and habits. This life stage serves as an important turning point for health, as early experimentation can either become a lifelong habit or be redirected in healthy ways. Furthermore, it is an important developmental phase when daily activities may shift, long-term career opportunities appear, and health behaviors become habits lasting for decades to come (Benson 2014).
Thus, we follow a nationally representative cohort of individuals across the transition to adulthood as they adopt adult roles and identities and achieve adult social statuses. We build on prior research that documented prevalent health lifestyles in the adolescent, early young adult, and late young adult life stages and their associations with young adult health (Lawrence, Mollborn, and Hummer 2017; Burdette et al. 2017). Prior research has not examined how health lifestyles are patterned across the life course, nor has prior research examined their associations with SES and adult roles. Thus, we develop a theoretical model of the development of health lifestyles over the transition to adulthood and their associations with SES and adult roles and apply this model to analyses predicting the previously documented health lifestyles, answering new research questions.
We examine processes leading to adult health inequality by addressing a key question that links health lifestyles with a life-course perspective: to what extent are health lifestyles, including their associations with SES, redirected or reinforced during the transition to adulthood? We describe two potential theoretical frameworks: path dependency, which focuses on early influences setting in motion a relatively stable trajectory, and developmental specificity, which highlights the potential for change in response to context, transitions, and life stages. Our results contribute to understanding why individuals of different SES engage in different patterns of health behaviors, an unsolved puzzle that is fundamental to addressing social inequalities in health.
Health Lifestyles
The health lifestyles concept brings together core sociological theories on group-based identities, the routinization of individual behavior, life course development, and social inequality. Health lifestyles link health behaviors to subjective definitions of group membership, values, and norms, meaningfully organizing diverse behaviors that researchers often treat separately. Health lifestyles are not arbitrary groupings of behaviors but rather are collective phenomena representing a coherent set of practices (Cockerham 2005). These groupings of individual health behaviors reflect broader, socially based meanings that are lost when treating health behaviors as separate. For example, college students often view smoking, alcohol use, and limited sleep as part of a lifestyle that is linked specifically to parties, clubs, and socializing, expecting that lifestyle to change upon leaving college (Nichter 2015). Smoking, alcohol use, and limited sleep among similarly aged workers who are not enrolled in college may instead reflect a response to chronic stress that could continue well into adulthood.
Health lifestyles can be concordant or discordant (Saint Onge and Krueger 2017). At the extremes, a positive concordant health lifestyle involves the avoidance of multiple, uniformly unhealthy behaviors, whereas a negative concordant health lifestyle involves the maintenance of multiple, uniformly unhealthy behaviors. Discordant health lifestyles involve a mix of healthy and unhealthy behaviors. The constellations of behaviors documented in prior research imply that changes in one specific behavior may be difficult to effect without other changes to the underlying lifestyle. For example, someone entering marriage may change multiple behaviors as part of a shifting lifestyle, as this transition is associated with less substance use but also compromised diet and exercise (Ross, Hill, and Mirowsky 2016). Recent research has pointed to the usefulness of health lifestyles in understanding behavioral patterns (e.g., Daw, Margolis, and Wright 2017; Olson et al. 2017) and has demonstrated important associations with mortality and morbidity (Lawrence et al. 2017; Burdette et al. 2017; Saint Onge and Krueger 2017).
Health Lifestyles and SES
Health lifestyles are theoretically rooted in long-standing sociological research on lifestyles and social class. Marx and Engels ([1848] 1970), Veblen ([1899] 2007), Weber ([1922] 1978), and Bourdieu (1984) have described the importance of social conditions for individuals’ lifestyles. Weber’s notion that social class plays out in everyday life through group-based lifestyles comprising behaviors and consumption patterns has been applied to health behaviors (Cockerham 2005; Frohlich and Potvin 1999). Consistent with these arguments, the associations between health behaviors and SES are well established (Cutler and Lleras-Muney 2010; Pampel et al. 2010), and research suggests that overarching health lifestyles are also related to SES (Mollborn et al. 2014; Skalamera and Hummer 2016).
Furthermore, lifestyles are expressions of socioeconomic identities (Weber [1922] 1978). People choose health lifestyles to express their identities, selecting from among lifestyle options available to members of their group in a particular context (Cockerham 2005). As social contexts change, people’s health lifestyles may also change. The transition to adulthood includes frequent geographic mobility (Brazil and Clark 2017), resulting in shifts in social contexts, peer groups, and group-based identities that may also vary by age and available lifestyle options. Beyond change in health lifestyles resulting from changing contexts, SES itself often shifts during the transition to adulthood (Lui et al. 2014). Ascribed SES, or the SES of one’s family in childhood and adolescence, may decrease in importance as young people form independent households and build human capital by starting careers or forgoing income to complete an education. At the same time, achieved 1 SES—the SES that is the result of one’s choices and is shaped by, but distinct from, ascribed SES—begins to form in young adulthood, resulting in potential identity changes. SES may not be fully achieved in young adulthood, but anticipation and expectation of achievements are beginning to influence behaviors and choices. Young adult achieved SES may be a key factor for understanding health lifestyles, even though SES is dynamic across adulthood.
SES constrains health behaviors through multiple, changing mechanisms (Freese and Lutfey 2010), including stress, financial resources, self-efficacy, community resources, and social support (Pampel et al. 2010). A broad and well-established literature demonstrates the joint stratification of SES and individual health behaviors, and similar processes may operate for health lifestyles. Prior research indicates that youth health lifestyles are indeed patterned by family SES (Daw et al. 2017; Mollborn et al. 2014; Mollborn and Lawrence 2018) and that education predicts healthier lifestyles (Skalamera and Hummer 2016).
Health Lifestyle Development over the Life Course
Despite the emergent SES-health relationship during adolescence and adulthood and the importance of time and place for human behavior (Elder 1998), little research has examined the developmental, temporal process of lifestyle adoption. The transition to adulthood, when individuals establish their social identities and develop their own habits and behaviors (Harris 2010; Rindfuss 1991), is likely critical for this process. The transition to adulthood is usually defined as spanning from about ages 18 to 30.
In early life more so than in adulthood, health behaviors can be restricted to particular life stages because of social and biological development. For example, we would not examine cigarette smoking or sexual risk among young children. Guidelines for healthy behaviors also differ across life stages. For example, experts recommend fewer hours of sleep for adults compared with adolescents (Paruthi et al. 2016; Watson et al. 2015). Thus, we argue that an accurate measurement of health lifestyles will necessarily be specific to life stages.
Specific health behaviors demonstrate marked patterns across the transition to adulthood, evidencing associations with markers of adulthood (Bachman et al. 2002; Frech 2012; Jeffery and Rick 2002). For example, smoking prevalence shows substantial changes across the transition to adulthood and is associated with educational attainment, employment, financial well-being, marriage, and parenthood (Pampel, Mollborn, and Lawrence 2014; Staff et al. 2010). Health lifestyles are also likely related to the completion of adult role transitions, such as marriage, paid work, financial independence, establishing a household, and parenthood. Normative behaviors may shift as individuals assume adult roles and experience changes in freedoms and responsibilities (Bachman et al. 2002). Getting married, starting a job, and becoming a parent are associated with changes in specific health behaviors (Umberson, Crosnoe, and Reczek 2010).
We present two opposing frameworks theorizing the developmental process of health lifestyles in the transition to adulthood. Because health lifestyles have reciprocal relationships with SES and adult roles, the frameworks focus on associations between health lifestyles and SES and adult roles and the patterns of those associations. The first perspective, termed “path dependency,” highlights the inter- and intragenerational and institutional reproduction of inequality. Here, health lifestyles are established early and, although there may be some developmental changes, generally follow from earlier health lifestyles. Similarly, SES shapes health lifestyles early in life and maintains close connections as individuals transition to adulthood, regardless of adult roles. In contrast, the second perspective, called “developmental specificity,” focuses on turning points, agency, and critical developmental stages, emphasizing the relationship between health lifestyles and life stage–specific conditions. In this framework, health lifestyles are expected to be relatively volatile across early life, changing with new adult roles and with inconsistent connections to SES.
Path Dependency
The path dependency approach expects consistency across the transition to adulthood in individuals’ health lifestyles and their associations with SES. Although measurement of health lifestyles will differ across life stages, this view would be supported by relatively consistent substantive results over age. Research has indicated the importance of early conditions for later outcomes, both empirically (Haas 2008; Hayward and Gorman 2004) and theoretically through cumulative dis/advantage theory (DiPrete and Eirich 2006) and cumulative inequality theory (Ferraro and Shippee 2009), which identify additive and multiplicative effects of social conditions over time. Furthermore, a strong sociological tradition asserts the significance of ascribed SES for experiences and opportunities throughout life, maintaining the status quo across generations. For example, Bourdieu and Passeron (1990) described how schools treat children who exhibit different social class signals differently, with important consequences for their educational outcomes.
Parenting is another important way that children are prepared to exhibit the same social class as their parents. Parents of higher social status encourage their children to develop a sense of entitlement and get what they need from institutions, whereas parents of lower status defer to authority, and these parenting styles continue to be influential through the transition to adulthood (Lareau 2011, 2015). School and family reinforce the expression of SES across the early life course, and SES shapes the transition to adulthood (Furstenberg 2008).
Prior research suggests that this view is particularly relevant for health lifestyles. Health lifestyles are an expression of habitus, Bourdieu’s (1977) concept describing the “durable” dispositions resulting from the interaction between an individual and their environment. Supporting this view, health behaviors and health lifestyles show associations with ascribed SES across life, with the health lifestyles of preschoolers being patterned by parent SES (Mollborn et al. 2014). We therefore test whether this perspective applies to health lifestyles across the transition to adulthood by analyzing whether individual health lifestyles demonstrate (1) similar composition in different life stages, (2) consistency within individuals over time, (3) consistent associations with SES over time, and (4) weak associations to adult roles.
Developmental Specificity
Developmental specificity focuses instead on change across life stages. This approach would expect that health lifestyles are specific to life stage, beyond just differences in measurement. The transition to adulthood offers many potential turning points for individuals. A time of “firsts” (Staff, Ramirez, and Vuolo 2015), it is described as demographically dense, in reference to high potential for marriage, childbearing, and migration (Rindfuss 1991). This developmental stage offers individuals the opportunity to continue or change their trajectories of health lifestyle, SES, and identity.
A developmentally specific approach would conceptualize habitus as a dynamic system, responding to new environments and contexts, rather than a durable disposition. In this approach, individuals may change their health lifestyles and/or their SES because of other life course events (or turning points) or other shifts in social contexts. Supporting this, some health behaviors are related inversely to SES during the early years of young adulthood but, with new events and roles associated with work and family, in later life stages display positive associations (Pampel et al. 2014; Patrick et al. 2012). The variation in these relationships across life stages suggests that they may be developmentally specific. For example, socioeconomically privileged college-goers may engage in unhealthy substance use in these early years, desisting as they transition out of college (Nichter 2015). Socioeconomically disadvantaged individuals may instead be busy working, increasing their substance use later as they age across young adulthood.
Limited research suggests that a developmentally specific perspective may describe health lifestyles. Mize (2017) reports relationships between types of social roles and health lifestyle membership, providing evidence that life-course context may be related to health lifestyles. We therefore assess whether health lifestyles are volatile over the transition to adulthood. A developmentally specific approach would expect that (1) health lifestyle compositions differ according to developmental stage, (2) individual’s health lifestyles are inconsistent over the life course, (3) associations between health lifestyles and SES change across age, and (4) adult roles are strongly associated with health lifestyles after controlling for ascribed SES.
The Present Study
We extend our previous study, which described predominant health lifestyles among a U.S. cohort that recently reached young adulthood, articulating and testing how these health lifestyles are patterned across this developmental stage and their relationships to SES and adult roles. To adjudicate between the path dependency and developmental specificity perspectives, we examine if and how health lifestyle groupings remain similar or differ across adolescence, early young adulthood, and late adulthood (research question 1); individuals change health lifestyles with age (research question 2); SES is associated with health lifestyles in each stage (research question 3); and adult roles are related to health lifestyles (research question 4).
Interpreting these results, we conclude whether health lifestyle development is best characterized by early influences and relative stability or by concurrent factors and volatility. We use longitudinal, nationally representative data from a cohort that has recently reached adulthood, offering information on the same individuals’ health behaviors in adolescence (ages 15–17), early young adulthood (ages 20–24), and late young adulthood (ages 26–31).
Methods
Data
We use the National Longitudinal Study of Adolescent to Adult Health (Add Health), a longitudinal, nationally representative survey (Harris et al. 2019). Add Health first surveyed 20,745 adolescents in grades 7 to 12 in 1994–1995 (wave I). The first follow-up was conducted on a subsample one year later (wave II). Wave III was administered in 2001 and wave IV in 2007–2008. In this study we use respondent interviews at waves I, III, and IV. This dataset offers detail on a wide range of health behaviors and social factors across the transition to adulthood. We adjust for sampling weights and clustering to account for clustering and unequal probability of selection and also account for stratification in regression analyses. For the latent class analysis (LCA) at each wave, we include all respondents with valid weights for that wave and who are 15 to 17 years old at wave I (wave I, n = 10,647; wave III [ages 20–24], n = 8,025; wave IV [ages 26–31], n = 8,312). For the regression analyses, our analytic sample comprises respondents who were aged 15 to 17 at wave I and who were reinterviewed at waves III and IV (n = 6,863).
Measures
Health Lifestyle Indicators
We operationalize health lifestyles broadly, drawing on a wide range of measures to capture health-related behaviors at waves I, III, and IV. We define “health-related” as shaping the risk for injury, illness, infection, or chronic disease and limit the scope to behaviors. All of these behaviors are likely related to structural constraints and opportunities shaped by families, schools, neighborhoods, policies, and other contexts, but we do not use such influences as inclusion criteria. We include measures for physical (in)activity, substance use, diet, safety, health care, sleep, and sexual risk behaviors. Similar studies (e.g., Burdette et al. 2017; Daw et al. 2017; Olson et al. 2017; Saint Onge and Krueger 2017) have incorporated subsets of these domains but, to our knowledge, have not used all of them, excepting our previous study. As mentioned earlier, measures differ slightly across survey waves because of developmental differences in life stages (Lawrence et al. 2017).
We create categorical measures, identifying thresholds on the basis of the observed distributions of data, substantive meaning of the cutoffs, and recommended guidelines. We combine categories or measures for parsimony. For example, smoking and chewing tobacco are combined to create one categorical variable for tobacco use. Our methodological approach is sensitive to the number, type, and choice of measures, and we therefore explored numerous alternative operationalizations and specifications for variables. These alternatives had generally similar substantive patterns. The results presented here indicate general patterns found across specifications and were the best fitting and most substantively interpretable (Lawrence et al. 2017). Table 1 summarizes the measures used in our analysis.
Measures Used in Latent Class Analyses to Generate Health Lifestyles, by Wave and Domain.

Note: Categories compare yes (or any) with no (or none) unless categories are indicated.
Independent variables include ascribed SES, achieved SES, adult roles, and controls. SES is represented by income and education to allow comparison over time. Ascribed SES is measured at wave I. We use the highest education of either parent; categories include less than high school, high school diploma or equivalent, some college, and four-year college graduate. Income-to-needs ratio is the ratio of household income relative to the 1995 or 1996 U.S. Census Bureau–defined poverty threshold by household size.
Achieved SES includes educational attainment, household income-to-needs ratio, and occupational status at early (wave III) and late (wave IV) young adulthood. Because respondents are different ages with differing levels of educational enrollment, we use different categories of educational enrollment for early and late young adulthood. For the former, we use categories of less than high school, high school, some college or currently enrolled in school, and college graduate. For the latter, we use categories for less than high school, high school diploma or equivalent, some college, four-year college graduate, and graduate or professional degree. Income-to-needs ratio is calculated as described for wave I but uses thresholds from the wave IV interview year. Occupational status includes not employed or working less than 10 hours per week, professional or managerial occupation, and nonprofessional or managerial occupation.
Adult roles are also measured in early (wave III) and late (wave IV) young adulthood. They include family structure (unmarried without children, married without children, unmarried with children, and married with children) and a comparison of those who live independently to those living with parents. In line with previous research (Pampel et al. 2014; Waite and Gallagher 2001) and for parsimony, we consider marriage as an adult role and therefore combine single and cohabiting respondents. There is considerable overlap between SES and adult roles; for example, finishing school and entering the job market are considered markers of adulthood, but educational attainment and employment are also considered components of SES.
Wave I controls include respondent age, gender, race/ethnicity, nativity, adolescent family structure, grade point average, religiosity, depressive symptoms, and self-rated health, all shown to be influential for health behaviors and status attainment (Bradley and Greene 2013; Fletcher and Kumar 2014; Jackson, Knight, and Rafferty 2010; Kao and Thompson 2003; Lehrer 2004; Lopez-Gonzalez, Aravena, and Hummer 2005).
Gender classifies individuals as male or female. Race/ethnicity is captured by mutually exclusive categories of non-Hispanic white (referred to as white hereafter), non-Hispanic black (referred to as black), Hispanic, and other race/ethnicity, including those of Asian/Pacific Islander or Native American/American Indian descent, or individuals who report “other.” Nativity is dichotomized as U.S.-born versus not. Family structure in adolescence indicates two biological parents versus other structures. Religiosity is coded into mutually exclusive categories on the basis of frequency of attendance at religious services: no religion or never attending services or attending less than once per month, at least once per month but less than weekly, and weekly or more. Grade point average uses self-reported grades (A, B, C, D, or lower) during the most recent grading period in English and language arts, mathematics, history and social studies, and science. Adolescent depressive symptoms sums, then standardizes, responses to 19 items asking about the respondent’s feelings. Adolescent self-rated health ranges from 1 (“poor”) to 5 (“excellent”).
Analytic Approach
To assess groupings of behaviors across life stages (research question 1), we examine health lifestyles at three time points. We use LCA to separately estimate health lifestyles at each wave (adolescence, early young adulthood, and late young adulthood). LCA uses a structural equation modeling approach to identify a categorical latent variable that is represented with observed indicators (see Collins and Lanza 2013). The categorical latent variable is health lifestyle, and the observed indicators are different health behaviors. LCA’s focus on a categorical latent variable makes this approach appropriate for identifying health lifestyles (Abel 1991). Using LCA allows us to include different health behavior indicators in each wave, which is important because we argue for measuring health lifestyles according to the relevant behaviors for that age, as opposed to using only a select set of behaviors that are applicable across ages.
We use the SAS package PROC LCA (Lanza et al. 2007; The Methodology Center, Penn State 2015). Analyses adjust for sampling weights and clustering to ensure national representation. We choose the number of classes considering fit statistics (see Appendix Table A and Figure A), theoretical and substantive coherence, and in line with the previous study (Lawrence et al. 2017). For waves I and III, we select the solution that demonstrates meaningful groupings, does not have any trivially small classes, and reflects good (but not the best) fit statistics, following best practices (Lanza et al. 2007; Nylund-Gibson and Choi 2018). For wave IV, we use the same criteria, but the chosen solution also reflects the best fit statistics. We compare results to multiple other possibilities, finding that they are generally robust to alternative specifications.
To assess stability or change in health lifestyles over time (research question 2), we examine associations between health lifestyles of different life stages. We assign each individual to the health lifestyle with the highest probability for each stage. Weighted cross-tabulations compare how many individuals from each health lifestyle in a particular wave are represented in other waves’ lifestyles.
To assess relationships between health lifestyles and SES (research question 3) and adult roles (research question 4), we estimate multinomial logistic regression models predicting health lifestyles at each wave. We use a stepwise approach that first identifies the health lifestyles and then distinguishes associations between these lifestyles and covariates. This approach is imperfect and has been shown to produce attenuated associations (Lanza and Cooper 2016), yet we find it to be the most feasible and interpretable for our study. An alternative approach that estimates classes and associations simultaneously has also been shown to produce biased associations and problematic class enumerations (Nylund-Gibson and Masyn 2016). Thus, we use a stepwise approach that separately classifies and analyzes the data.
For adolescence, we estimate models with controls. For early young adulthood (wave III), we estimate models with controls, adolescent health lifestyles, and concurrent SES and adult roles. For late young adulthood (wave IV), we estimate models with controls, adolescent and early young adult health lifestyles, early young adult SES and adult roles, and concurrent SES and adult roles. We present results from multinomial models comparing each group with the referent of the healthiest lifestyle, a meaningful point of comparison that is substantively interesting and easy to understand. The healthiest lifestyle is also the most useful comparison for interventions or other policies seeking improvements in population health. Although other contrasts may be useful, focusing on one clear and consequential comparison allows a coherent interpretation of results and a reasoned set of conclusions.
We restrict the sample by age because health behaviors and health lifestyles are age dependent, and tests of measurement invariance show that models separated by age such as ours better fit the data. LCA retains all eligible cases at each wave using full information maximum likelihood to account for item missingness. To retain the full sample for further descriptive statistics and regression analyses, we use multiple imputation using a chained equations approach (White, Royston, and Wood 2011), allowing each variable imputation model to use the distribution appropriate to measurement level. We create 30 data sets using all independent and dependent variables.
Results
We first identify health lifestyles in the three stages (research question 1). Our LCAs yield six, five, and four health lifestyle classes for adolescence (wave I), early young adulthood (wave III), and late young adulthood (wave IV) respectively (see Table 2). Appendix Tables B to D present the class-conditional probabilities for all indicators. We name each group according to the substantive criteria that distinguish the group from the population average and other groupings.
Means of Health Lifestyle Classes across Health Lifestyles of Different Stages.
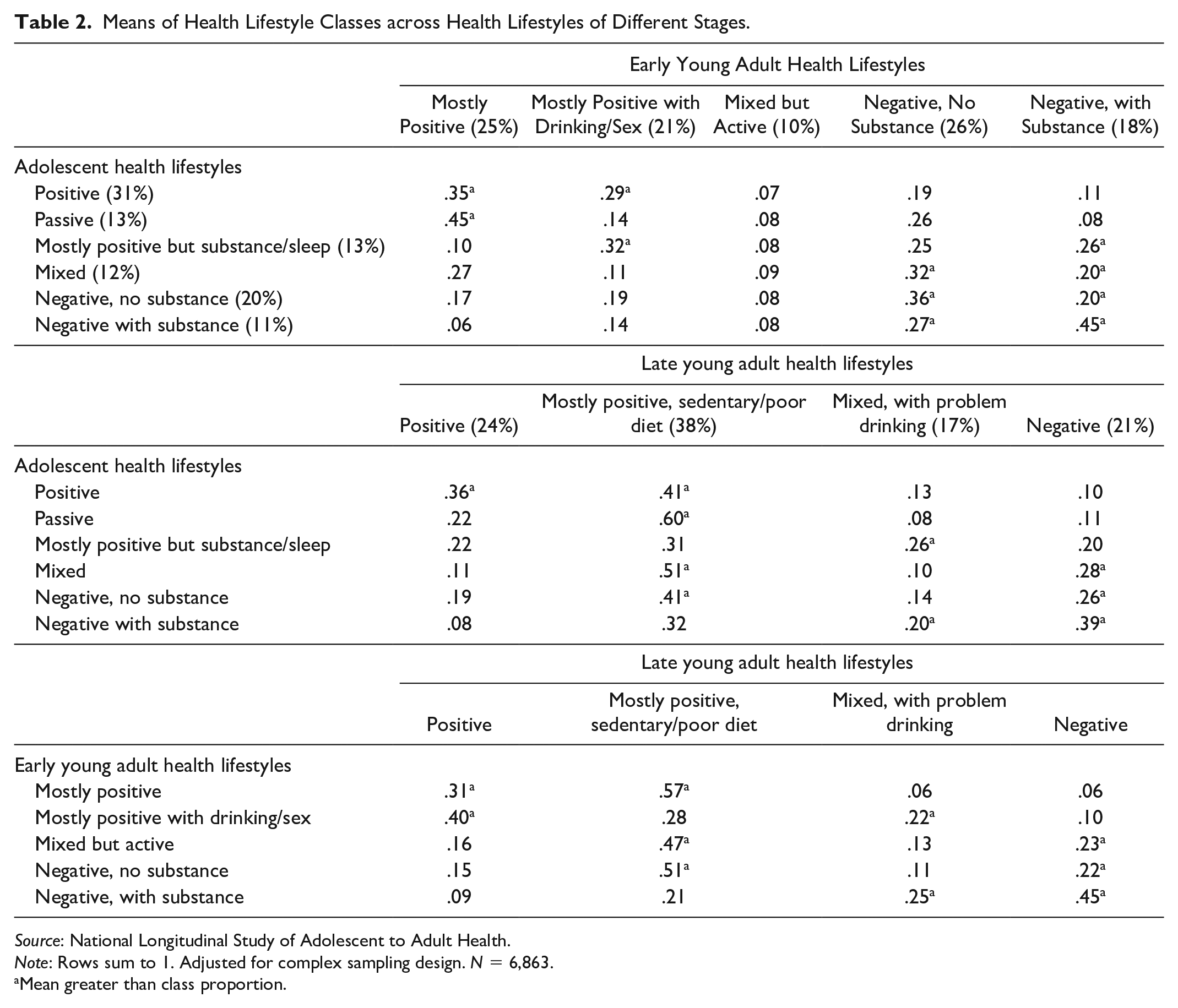
Source: National Longitudinal Study of Adolescent to Adult Health.
Note: Rows sum to 1. Adjusted for complex sampling design. N = 6,863.
Mean greater than class proportion.
For adolescence (ages 15–17), a positive group (31 percent) exhibits generally healthful behaviors, and a mostly positive but substance/sleep group (13 percent) displays healthful behaviors but also engages in substance use and has sleep problems. This wave also includes a passive group (13 percent) that appears to refrain from both healthful and harmful behaviors and a mixed group (12 percent) that demonstrates favorable activity, sleep, drug use, and sex behaviors but also unfavorable screen time, tobacco use, diet, safety, and health care. There are two negative groups that demonstrate generally insalubrious behaviors, but one group engages in substance use (11 percent) and the other does not (20 percent).
For early young adulthood (ages 20–24), no group is consistently positive on all indicators. The mostly positive group (25 percent) has mostly healthful behaviors but displays low rates of physical activity. Another mostly positive group (21 percent) has multiple salubrious indicators but has high rates of problem drinking and risky sex. A mixed group also emerges (10 percent), with healthful activity but poor sleep and safety. Similar to adolescence, two negative groups are differentiated by substance use (18 percent) or abstention (26 percent).
For late young adulthood (ages 26–31), a positive group (24 percent) displays a consistently healthy profile, alongside a consistently unhealthy negative group (21 percent). Another group is mostly positive but has poor activity and diet (38 percent), and a mixed with problem drinking group (17 percent) shows a complex pattern but also remarkably high rates of problem drinking.
Overall, these results demonstrates a discordant or mixed pattern of behaviors in terms of health implications, defying simple categorization according to a unidimensional, concordant continuum of healthfulness. Each life stage has more and less positive clusters, with substance use, diet, and physical activity levels often being defining characteristics. Yet clusterings show important differences by life stage, beyond those we would expect from measurement alone. For example, each stage has a mostly positive group with a different risk behavior: sleep in adolescence, sex risk for early young adulthood, and sedentariness for late young adulthood. Notably, health lifestyles are generally less healthy in early young adulthood compared with either adolescence or later young adulthood. In early young adulthood, all of the health lifestyles include some compromised behaviors, and a sizable proportion of individuals (45 percent) are in the generally negative groups (either with or without substance use). Thus, we conclude that lifestyles are fairly dissimilar across life stages, supporting developmental specificity.
Turning to individuals’ patterning of health lifestyles (research question 2), Table 2 and Figure 1 compare patterns of individuals’ health lifestyles at different life stages. Figure 1 illustrates the proportions of health lifestyle classes and their relationships to one another. Each ribbon’s size corresponds to the percentage from the lifestyle on the left who are in the lifestyle on the right. For example, among those in the wave I positive group, 35 percent go on to adopt the wave III mostly positive lifestyle, 29 percent to the mostly positive with drinking/sex, and smaller proportions to the other lifestyles. It is important to note that because we theoretically and empirically construct the lifestyles separately for each wave using different health behavior measures, they are not directly comparable over time. However, we can look at some general trends.

Health lifestyles at waves I, III, and IV.
As displayed in Figure 1 and Table 2, many individuals remain in a similar health lifestyle from one life stage to the next, but there is also considerable movement. A few examples illustrate the relative consistency and movement. Among those in the adolescent positive health lifestyle, only about one third go on to the early young adult mostly positive group. Other groups display less stability. Those in the adolescent negative with substance group are distributed across the late young adult groups, with about one third in mostly positive, sedentary/poor diet, one fifth in mixed with problem drinking, nearly two fifths in the negative group, and 8 percent in the positive group. Adolescents in this negative lifestyle may be experimenting with different behaviors, from which unhealthy habits may persist.
A given individual shifting across the spectrum from a lifestyle composed of consistently unhealthy habits to a consistently healthy lifestyle appears unlikely, but smaller shifts are common. For example, the large majority (88 percent) of those in the early adult mostly positive group go on to belong to the positive or mostly positive, sedentary/poor diet lifestyles. In the middle panel, among those in the passive group in adolescence, 60 percent are in the mostly positive, sedentary/poor diet group in late young adulthood, which is similar in its inactivity and substance use abstention. Only 8 percent and 11 percent of the passive adolescents belong to the mixed, with problem drinking and negative groups, respectively. Together, some lifestyles demonstrate stronger relationships to other lifestyles, whereas others demonstrate more irregularities. Thus, we conclude that these results partly support path dependency but also display developmental specificity.
We now turn to associations with SES (research question 3). Tables 3 to 5 present regression models assessing multivariate relationships between social factors, adult roles, SES, and health lifestyles at each life-course stage. SES demonstrates significant associations for each stage, although with differing patterns. For adolescence (Table 3), higher ascribed SES (greater parental education or greater household income-to-needs ratio) is associated with reduced log odds of membership in the passive and mixed groups compared with the positive group, net of controls and adolescent factors. Interestingly, ascribed SES does not display consistent patterns for membership in groups with substance use compared to the referent.
Coefficients and Significance from Multinomial Logistic Regression for Adolescent (Wave I; Ages 15–17) Health Lifestyle (Referent: Positive).

Source: National Longitudinal Study of Adolescent to Adult Health.
Note: Adjusted for complex sampling design. N = 6,863. GPA = grade point average; HS = high school; NH = non-Hispanic; SES = socioeconomic status.
p < .05, **p < .01, and ***p < .001 (two-tailed).
For early young adulthood (Table 4), ascribed SES is significantly associated with group membership compared with the referent but generally shows an inverse relationship, such that higher parental education is associated with greater log odds of less healthy group membership (mostly positive with drinking/sex, negative no substance, and negative with substance) compared with the referent. These associations are similar but with some higher magnitudes in a supplementary base model that does not include adolescent health lifestyles, wave III adult roles, or wave III achieved SES (see Appendix Table G). These results indicate that higher ascribed SES is, perhaps surprisingly, associated with increased health lifestyle risk during early young adulthood (ages 20–24).
Coefficients and Significance from Multinomial Logistic Regression for Early Young Adult (Wave III; Ages 20–24) Health Lifestyle (Referent: Mostly Positive).

Source: National Longitudinal Study of Adolescent to Adult Health.
Note: Adjusted for complex sampling design. N = 6,863. GPA = grade point average; HS = high school; NH = non-Hispanic; SES = socioeconomic status.
p < .05, **p < .01, and ***p < .001 (two-tailed).
For late young adulthood (Table 5), ascribed SES is not significantly associated with health lifestyle membership compared with the referent, net of other factors. However, in a base model only including controls (see Appendix Table H), having a college-educated parent is associated with reduced log odds of belonging to the mostly positive, sedentary/poor diet (corresponding odds ratio = .48) and the negative (corresponding odds ratio = .55) groups compared with positive, and the former group also demonstrates reduced log odds for income-to-needs ratio (corresponding odds ratio = .95). These relationships are no longer significant once wave IV achieved SES and adult roles are included, suggesting that these background factors may operate through other social factors. We therefore conclude that higher ascribed SES is associated with reduced risk for health lifestyles that are less healthy in adolescence, increased risk for health lifestyles that are less healthy in early young adulthood, and little to no direct associations during late young adulthood.
Coefficients and Significance from Multinomial Logistic Regression for Late Young Adult (Wave IV; Ages 26–31) Health Lifestyles (Referent: Positive).

Source: National Longitudinal Study of Adolescent to Adult Health.
Note: Adjusted for complex sampling design. N = 6,863. GPA = grade point average; HS = high school; NH = non-Hispanic; SES = socioeconomic status.
p < .05, **p < .01, and ***p < .001 (two-tailed).
Achieved SES in early young adulthood, a life phase in which adult socioeconomic attainment may still be emerging, demonstrates a somewhat complicated pattern with early adult health lifestyle membership (Table 4). Greater educational attainment is associated with increased odds of belonging to the mostly positive with drinking/sex and decreased log odds of belonging to the negative, no substance, compared with mostly positive. Income-to-needs ratio is not significantly related to early adult health lifestyle. For occupation, having a nonprofessional job increases the log odds of belonging to the mostly positive with drinking/sex and negative, no substance groups, compared with mostly positive. Together, these findings suggest that higher SES in early young adulthood does not confer much advantage for health lifestyle, in line with research arguing that experimentation in “emerging adulthood” is concentrated among those more privileged (Hendry and Kloep 2010).
Unlike SES in early young adulthood, achieved SES demonstrates generally protective associations with late young adult health lifestyles (Table 5). Greater educational attainment is associated with lower log odds of belonging to the negative group, and greater household income is related to reduced log odds of being in the mostly positive, sedentary/poor diet and negative groups compared with positive. Occupational status does not conform to the pattern, with those in professional or nonprofessional jobs (compared with not employed) more likely to belong to the mostly positive, sedentary/poor diet and negative classes than the positive referent, net of the covariates. Models that do not consider earlier health lifestyles or wave III SES and adult roles are substantively similar to these results, but with generally larger magnitudes and more significant associations (see Appendix Table I).
Summarizing associations with ascribed and achieved SES (research question 3), we conclude that patterns are more consistent with a developmentally specific than a path-dependent perspective. Associations between ascribed SES and health lifestyles do not appear similar across the three life stages, with directions of associations reversing in early young adulthood and no significant results in the full model for late young adulthood. Achieved SES also demonstrates varying associations with early versus late young adulthood health lifestyles, with patterns generally reversed across these two stages.
Turning to research question 4, we examine associations between adult roles in early and late young adulthood and health lifestyle membership. The results for early young adulthood (Table 4) show that being married or having children generally reduces the log odds of being in the mostly positive with drinking/sex, mixed but active, or negative with substance use groups compared with the referent but does not relate to negative, no substance. Living away from parents in this life stage is associated with increased membership in three of the four less healthy groups compared to the reference group.
Similarly, in late young adulthood (Table 5), family structure is significantly associated with health lifestyle membership. Marriage (with or without children) is associated with reduced log odds of being in each of the less healthy options compared with the referent. Unlike early young adulthood, however, living separately from one’s parents does not relate to late young adult health lifestyles. These results are similar in models that do not include earlier health lifestyles or wave III achieved SES and adult roles (see Appendix Table I). In early and late young adulthood, significant associations between adult roles and health lifestyles that emerge with controls for background ascribed and achieved SES provide evidence supportive of a developmentally specific perspective.
Discussion
Prior research has documented the prevalence and health consequences of health lifestyles over the transition to adulthood (Lawrence et al. 2017; Burdette et al. 2017). Understanding the life-course patterns and dynamic social contexts of these health lifestyles offers insight into how and why individuals adopt different health lifestyles. In this study, we aimed to describe health lifestyle development over the transition to adulthood and its relationship to SES and adult roles. We presented competing theoretical frameworks: (1) path dependency, which expects consistency in health lifestyles across the transition to adulthood, and (2) developmental specificity, which highlights transitions and changes in health lifestyle trajectories. We then analyzed the composition of health lifestyle groupings, patterns of health lifestyles over life stages, and associations between health lifestyles and SES and adult roles to identify the framework that best characterizes health lifestyles over the transition to adulthood. We conclude that both frameworks are relevant for understanding health lifestyles but that developmental specificity is more salient. We explain this conclusion further.
Health lifestyles cannot be conceptualized as spontaneously arising in adulthood but instead have origins in early-life social experiences and health behaviors. Adolescent health lifestyles are strongly patterned by ascribed socioeconomic characteristics, suggesting that early experiences shape health lifestyles. In turn, adolescent health lifestyles are related to early and late young adult health lifestyles. Thus, we find utility in a path dependency perspective, and particularly in its articulation of early contexts and factors setting in motion behavioral patterns.
However, the results complicate a cumulative dis/advantage explanation. They support claims that emerging adulthood is a unique and risky life phase for many individuals (Arnett 2000; Frech 2012). Perhaps more important, our findings also imply that rather than being an anomaly with no consequences, emerging adult health lifestyles have considerable influence on later health lifestyles when many respondents have settled into their adult lives. Additionally, these early young adult health lifestyles affect later health and well-being (Lawrence et al. 2017). Thus, the consequences of emerging adult health behaviors, even if they are somewhat transitory, remain crucial. This life phase may be a catalyst for the development of socially patterned risky health behaviors that persist into the future.
Additionally, the differences in associations between health lifestyles and SES across life stages suggest that in the transition to adulthood, individuals settle into their SES-based identities, in part through their health lifestyles. Early young adulthood demonstrates an inverse association between ascribed SES and health lifestyles and no consistent pattern for achieved SES. We interpret these findings as indicative of the transitional status of this life stage, particularly in a historical context allowing individualization of the life course (Shanahan 2000), and as demonstrating the importance of understanding the dynamic nature of SES. Associations with SES thus appear to be developmentally specific, and socioeconomically based identities may become more salient in adulthood than in earlier life.
Importantly, our results call into question the durability of SES for explaining health lifestyles and suggest that research should seek to identify the conditions under which associations are evident or absent. Furthermore, associations between health lifestyles and adult roles suggest that investigating continuity and change across life-course transitions may offer additional insight as to how and why individuals maintain or change their health lifestyles. We cannot speak to SES-health lifestyle connections in middle or older adulthood, but future research may consider a developmentally specific framework for these or other life stages.
These results support calls for an integrated theory joining the path dependency and development specificity perspectives (Pampel et al. 2014). Our results suggest the importance of recognizing that adolescence sets the stage for later behavior but does not determine it: life-course changes in adulthood have the potential to redirect disparities in healthy lifestyles. Norms in adolescence and young adulthood leave room for experimentation that affects youth from all backgrounds. SES differences in health lifestyles are modest in adolescence and early adulthood. However, roles that steadily emerge through late young adulthood are increasingly differentiated by achieved SES. Adult roles may reinforce path dependency among lower SES groups, which tend to continue less healthy behaviors into adulthood. In contrast, role transitions may redirect health lifestyles for high-SES groups. Despite much experimentation at younger ages, these groups come to reject risky health lifestyles as they complete advanced education, establish long-term relationships, and enter into occupational careers.
Achieved SES and adult roles thus have both overlapping and independent influences. Considering the combined influences of family SES, achieved SES, the stage-setting influence of early health lifestyles, and the potential redirecting influence of later roles for advantaged SES groups can help make sense of the complexity of life-course changes in health lifestyles and is consistent with rising social inequalities in health.
This study has several limitations. First, because our data are observational, we focused on associations and could not identify causal relationships. Second, we investigated the transition to adulthood, but important processes occur before and after this life stage. Third, we sought to maximize our understanding of health lifestyles in the three stages; other approaches (e.g., latent transition analysis) may better identify trajectories of specific behaviors or SES but omit a fuller picture of health lifestyles. Finally, more complex modeling efforts, although beyond the scope of our study, can build substantively, theoretically, and methodologically on our approach. A promising avenue for additional analysis would be to examine the influence of timing, sequencing, or duration of adult transitions on health lifestyles. Furthermore, application of LCA is an active area of research, and we anticipate that more precise methods available in the future will provide opportunities for further insight.
Our attention to widening disparities in health and health behavior across SES may stimulate research into the meaning of SES for routinized, everyday patterns of behavior such as health lifestyles. The results suggest that early experiences, although important, are not the sole source of adult inequalities in health lifestyles. Rather, they develop and change across the transition to adulthood, as individuals progress toward their own achieved SES and settle into identities that conform to that status.
Supplemental Material
Supplemental_data_051320 – Supplemental material for Health Lifestyles and the Transition to Adulthood
Supplemental material, Supplemental_data_051320 for Health Lifestyles and the Transition to Adulthood by Elizabeth Lawrence, Stefanie Mollborn, Joshua Goode and Fred Pampel in Socius
Footnotes
Acknowledgements
We are grateful for general support from the Colorado Population Center (P2C HD066613) and Carolina Population Center (P2C HD050924), funded by the Eunice Kennedy Shriver National Institute of Child Health and Human Development. We thank Richard Jessor, Jennifer Pace, Bethany Rigles, and Laurie James-Hawkins for their feedback and Ben Domingue for suggesting river plots.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is based on work supported by a grant from the National Science Foundation (SES 1423524) and by the National Institutes of Health under Ruth L. Kirschstein National Research Service Award (F32 HD 085599). This research uses data from Add Health, a program project directed by Kathleen Mullan Harris and designed by J. Richard Udry, Peter S. Bearman, and Kathleen Mullan Harris at the University of North Carolina at Chapel Hill and funded by grant P01-HD31921 from the Eunice Kennedy Shriver National Institute of Child Health and Human Development, with cooperative funding from 23 other federal agencies and foundations. Special acknowledgment is due Ronald R. Rindfuss and Barbara Entwisle for assistance in the original design. Information on how to obtain the Add Health data files is available at the Add Health Web site (![]() ). No direct support was received from grant P01-HD31921 for this analysis.
). No direct support was received from grant P01-HD31921 for this analysis.
Supplemental Material
Supplemental material for this article is available online.
1
We do not intend achieved to indicate a completed state, as SES will change over the life course. However, even SES positions that change may influence current health lifestyles.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.