
Abstract
This article investigates partisan beliefs regarding attributions of responsibility for mental illness and support for mental health treatment. In study 1, we utilize a nationally representative data set to investigate these relationships with respect to generalized anxiety disorder. In study 2, we utilize an online convenience sample to assess these relationships in the context of schizophrenia. In both studies, Republicans were more likely than Democrats to attribute mental health disorders to factors that lie within patients’ control and were less supportive of healthcare coverage. In addition, given the rhetorical, erroneous link between schizophrenia and gun violence, we assess participants’ beliefs about gun control in the context of mental health. Paradoxically, we find that people who support gun rights for the mentally ill are the least likely to support healthcare coverage for the mentally ill. We discuss the implications of our findings for shaping U.S. gun debates.
The United States is in the midst of what many are calling a “mental health crisis” (e.g., Snow and McFadden 2017; Plakun 2020). An estimated 47.6 million adults and 7.7 million children suffer from mental illness in any given year (Substance Abuse and Mental Health Services Administration 2019; Whitney and Peterson 2019). Psychological distress, major depression, suicide, and suicidal ideation are on the rise, particularly among adolescents and young adults (Twenge et al. 2019). And there is an immense, unmet need for mental health treatment stemming from stigma, provider shortages, and unaffordability (Cohen Veterans Network and the National Council for Behavioral Health 2018). Consequently, the average delay between the onset of mental illness symptoms and treatment is 11 years (Wang et al. 2004), and nearly 60 percent of adults and 50 percent of children with mental illness go without services for a year or more (Substance Abuse and Mental Health Services Administration 2019; Whitney and Peterson 2019).
Given the current state of mental health in the United States, Democrats and Republicans alike have incorporated mental health reform into their legislative agendas. Last year, Democratic state legislators sponsored approximately 10,000 bills that included the words “mental health,” and Republican state legislators—despite their historical support of deregulation and privatization—sponsored more than 5,000 such bills, twice as many as they did five years ago (Craig 2019). Yet the policies proposed both between and among political parties widely vary. For example, during the Democratic national primary election of 2020, Bernie Sanders emphasized the need to reduce treatment costs, promising free mental health services and prescription drugs, whereas Amy Klobuchar underscored prevention and early intervention, particularly in schools, a plan that resembled efforts by Republican Governor Gary Herbert, who recently expanded the scope of youth suicide prevention programs in Utah’s public schools (Ramseth 2018). President Trump, on the other hand, has said little about mental health except in the context of gun violence. For example, after mass shootings in Texas and Ohio, Trump controversially proposed building and reopening long-term psychiatric institutions, stating, “These people are mentally ill” (Craig 2019).
By looking at the public record, it is fairly easy to ascertain the opinions of lawmakers regarding mental health and mental healthcare reform. Yet given that public policy influences the health and well-being of the general public and that politicians are generally expected to represent their constituents’ preferences, it is important to understand Americans’ views on mental health, particularly along party lines, a matter that has received surprisingly little attention. To our knowledge, only one study has examined support for mental healthcare coverage by party affiliation. In 2014, a public opinion survey found that 69 percent of respondents supported mental healthcare parity—the equal treatment of physical and mental health conditions in insurance plans—and 59 percent supported increasing government spending on mental health treatment, although Democrats were more supportive of both policies than Republicans and Independents (Barry and McGinty 2014). We expand on this work and ask how similar or different Democrats and Republicans are in their understandings of the origins of mental health problems—that is, who or what is at fault when someone is diagnosed with a mental disorder—and in their support for mental healthcare treatment. In addition, if Democrats or Republicans believe mental illness is largely attributable to factors that lie within people’s control, it follows they may be less sympathetic toward people with mental health problems and less motivated to enact federal and state regulations. Thus, we also examine the relationship between partisanship, origin beliefs, and treatment support.
In what follows, we briefly summarize the literature regarding the etiology of mental illness, followed by a discussion of the history and support of mental healthcare coverage in the United States. We then present the results of two studies designed to answer the above questions. In study 1, we utilize a nationally representative data set to investigate these relationships with respect to generalized anxiety disorder (GAD), a relatively common, neurosis-based disorder. Anxiety disorders are among the most widespread mental health disorders in the United States, affecting approximately 19.1 percent of the adult population annually and 31.1 percent of adults over the life course (National Institute of Mental Health 2017a). In study 2, we utilize an online convenience sample to examine these relationships in the context of schizophrenia, a psychosis-based disorder, that affects less than 1 percent of the U.S. population (National Institute of Mental Health 2017b). We chose these two disorders to encompass a spectrum of mental health diagnoses. Moreover, of late, policy makers on both the Left and the Right have rhetorically linked schizophrenia to gun violence, and concerns about gun violence have motivated politicians to propose a surge of new mental health policies. Thus, in study 2, we also assess participants’ beliefs about gun control, allowing us to contribute to U.S. gun debates.
Underlying Causes of Mental Illness and Personal Responsibility
Mental illness is a broad class of psychological disorders that affects mood, thinking, and behavior. For the vast majority of mental health conditions, the exact causes are unknown; however, most researchers agree that mental illness is caused by a combination of biological, psychological, and environmental factors. For example, previous research finds that GAD is more common among individuals with a family history of anxiety (McLaughlin, Behar, and Borkovec 2008), with prolonged exposure to stress (Roemer et al. 1996), and who consume excessive amounts of caffeine or tobacco (Bruce, Scott, and Shine 1992; Piper et al. 2010).
Broadly, the factors underlying mental illness can be categorized as those that fall within, and those that fall outside of, individual control. Factors within people’s control tap into individual-level decisions and people’s ability to make their own free choices. Factors that fall outside of people’s control tap into genetic as well as structural-level influences. This is a useful distinction because inferences about personal responsibility predict social motivation (Munsch and Barnes 2020; Weiner 1993, 1995). For example, in a study of physical and mental health problems, Weiner (1993) found that persons held responsible for their conditions were found to be less likeable, to elicit less pity, and, most importantly, to generate low ratings on willingness to help as measured by charitable donations and offerings of personal assistance. Thus, we ask to what extent Americans believe GAD and schizophrenia are the result of personal choice and if attributions of responsibility differ between Republicans and Democrats.
Although perceptions of responsibility are, to some extent, subjective, the available literature suggests very different heritability coefficients for these two disorders. Researchers estimate that 30 percent of the total variance in GAD is due to genetic influence. The heritability of schizophrenia is much larger, with 80 percent of the variation estimated to stem from genetic factors. Thus, in selecting these diagnoses, we are able to examine the relationship between party affiliation and attributions of responsibility in disorders presumed to have larger (GAD) and smaller (schizophrenia) individual components.
Mental Healthcare Coverage
In addition to assessing perceptions of responsibility, we ask how supportive the American public is of mental healthcare coverage and if support for mental healthcare coverage falls along party lines. In 1996, the Mental Health Parity Act was signed into law after a decades-long battle for equity in coverage for behavioral healthcare. The act requires annual or lifetime dollar limits on mental health benefits to be no lower than limits for medical and surgical benefits offered by a health insurance issuer. Attempts to implement the law, however, have proved challenging for several reasons, including differences in how health plans define medical necessity, limited mental healthcare services offered within provider networks, and lack of oversight on the part of federal and state regulators (Johnson 2018). Consequently, healthcare coverage is often lower for mental health disorders than for other medical disorders (Melek, Perlman, and Davenport 2017).
By and large, research finds widespread support for mental healthcare coverage (Hanson 1998; Barry and McGinty 2014; Maust et al. 2015). For example, results from a national poll of the U.S. adult population indicate that 78 percent of respondents supported mandated insurance coverage for mental health (Maust et al. 2015). Yet, support for mental health coverage was lower than support for virtually all other medical services, and little is known about treatment support for specific disorders by party affiliation. Thus, we expand on this work by ascertaining the degree to which Democrats and Republicans are supportive of mental healthcare coverage using both self-report and behavioral measures.
Study 1: Data and Methods
The data for study 1 come from a nationally representative survey experiment collected through the National Opinion Research Center’s AmeriSpeak panel as part of the Time-Sharing Experiments for the Social Sciences program (Freese and Druckman 2019). AmeriSpeak uses a multistage probability-based panel design and nonresponse follow-up to deliver a sample that is representative of the U.S. household population. Data from 1,963 adults were collected in January and February of 2019.
The study utilized a vignette-based, factorial survey experiment. Each respondent was presented a vignette that described a medical patient who went to the doctor complaining about a set of symptoms and received a diagnosis. The experimental design manipulated patient disorder such that respondents read about a patient diagnosed with either leukemia, HIV, or GAD. However, given our theoretical interest for this article, we restricted the sample to those participants who read about the mental health disorder GAD, yielding a sample of 668 respondents.
In addition to diagnosis, we manipulated patient age (6, 40, or 75 years old); gender (boy/man or girl/woman); race/ethnicity (white, black, or Hispanic); immigration status (recent immigrant or native born); and socioeconomic status, which was accomplished using an occupational proxy (works/parents work in food or financial services). An advantage of factorial survey experiments is that they allow researchers to examine the impact of vignette dimensions, respondent characteristics, and interactions between the two on outcomes of interest (Auspurg and Hinz 2014). Elsewhere we report the results of our manipulated vignette dimensions (Munsch and Barnes 2020). In this article, we focus on the relationship between respondent characteristics—namely, political identification—beliefs about personal responsibility, and support for mental healthcare coverage. As an example, the text presented to a respondent for one condition read Jennifer is a 40-year-old Hispanic female who has lived in the U.S. for the past two years. Jennifer works in the food services sector. Jennifer recently went to the doctor complaining of unrealistic fears, a racing heartbeat, and shallow breathing. After a full examination and assessment, the doctor diagnosed Jennifer with generalized anxiety disorder, a disorder marked by excessive worry that lasts six months or longer.
1
Outcome Measures
Personal Responsibility
After reading the vignette, participants read the following: Health disorders may be attributed to a wide range of factors, such as genetics, air quality, access to safe water and healthy food, dietary choices, exercise, smoking, alcohol consumption, hygiene practices, lifestyle and more. Some of these factors may be outside of a person’s control, while some are within a person’s control.
Participants then were asked to split 100 percentage points of responsibility between factors outside of the patient’s control and factors within the patient’s control. The percentage of responsibility assigned to factors within the patient’s control was converted into a proportion ranging from 0 to 1. This variable serves as our measure of personal responsibility.
Support for Mental Healthcare Coverage
After assigning responsibility, participants read that the doctor prescribed a medication to treat the patient’s disorder and were asked what percentage, if any, of the prescription expenses should be covered by insurance. This percentage was converted into a proportion running from 0 to 1 and serves as our self-report measure, prescription coverage.
Next, respondents read that the patient’s insurance plan does not cover the prescribed medication, and participants were given the opportunity to have their names and zip codes added to a petition urging the insurance provider to cover the medication. The petition was fictitious; however, respondents were led to believe the petition was real until after they completed the survey. This measure, petition, serves as our behavioral measure of support for mental healthcare coverage (0 = did not sign petition, 1 = signed petition).
Respondent Sociodemographic Characteristics
Descriptive statistics for the sample can be found in Table 1. Overall, approximately 55 percent of the sample identified as female. (Male is the referent category.) Participants ranged in age from 18 to 94 years old (M = 49.88, SD = 16.39). Of the sample, 68 percent identified as non-Hispanic white, 11 percent as non-Hispanic black, 14 percent as Hispanic, and 7 percent as some other race or ethnicity. (Non-Hispanic white is the referent category.) A total of 36 percent had at least a four-year degree. (No four-year degree is the referent category.) Income was measured with 18 categories ranging from less than $5,000 per year to more than $200,000 per year. The median household income for the sample was 10, which corresponds to between $50,000 and $59,000 per year (M = 10.20, SD = 4.21). A total of 33 percent of the sample reported having at least one child under the age of 18. (No children under the age of 18 is the referent category.) The four standard regions capture whether the respondent lives in the Northeast (14 percent), the Midwest (29 percent), the South (33 percent), or the West (24 percent). (Northeast is the referent category.) Zip codes were used to determine whether the respondent lives in a metropolitan area (90 percent of the sample). (Not living in a metropolitan area is the referent category.)
Study 1, Respondent Characteristics.

In addition to these variables, and of import to our study, respondents were asked to indicate their party identity on a seven-point scale ranging from strong Democrat to strong Republican, with those who don’t lean, are Independents, or don’t identify with either party categorized in the middle (4). Lower numbers represent stronger identification with the Democratic Party; higher numbers represent stronger identification with the Republican Party. Approximately 50 percent of the sample identified to some extent with Democrats; around 35 percent identified with Republicans.
Analytic Strategy
First, to assess the extent to which Americans believe GAD is the result of personal choice, as well as how supportive the American public is of mental healthcare coverage for GAD, we present overall means and proportions for our dependent variables. Next, to assess the relationship between political identification, beliefs about personal responsibility, and support for mental healthcare coverage, we compare our dependent variables by political identification. For the continuous variables, personal responsibility and prescription coverage, we conduct independent samples t tests. For the binary variable, petition signing, we conduct a two-samples test of proportions. Next, we present results from a series of regression models to assess the relationship between party identity and our dependent variables controlling for vignette characteristics and respondent sociodemographic variables. To predict personal responsibility, we use zero-inflated beta regression. To predict prescription coverage, we use one-inflated beta regression. To predict petition signing, we use logistic regression.
Beta regression is a type of generalized linear model that loosens the normality assumption and allows for beta-distributed proportional dependent variables. Many proportions are unevenly distributed such that values of 0 or 1 are overrepresented. In the case of personal responsibility, there is an overrepresentation of 0s. In the case of prescription coverage, there is an overrepresentation of 1s. 2 When the extremes of a dependent proportion are inflated, residuals from ordinary least squares can be unevenly distributed, violating the homoscedasticity assumption required of ordinary least squares regression. For example, the distribution of personal responsibility may be more heavily concentrated around 0 for Democrats than for Republicans.
Zero-inflated (or one-inflated) beta regression simultaneously models two processes. The model uses logistic regression to distinguish between zeros and non-zeros (or ones and non-ones) and beta regression to model the proportional responses that vary between 0 and 1. These models are run simultaneously, and two sets of coefficients are presented for each model.
In a final set of models, we examine whether the relationship between party identification and support for mental healthcare coverage is attenuated by assessments of responsibility.
Results
Turning first to the overall sample means and proportions for our dependent variables, on average, respondents assigned 45 percent responsibility to the GAD patient. Moreover, only 3 percent of the sample indicated that the patient was in no way responsible for his or her illness. Thus, the American public tends to believe that patients diagnosed with GAD are, at least to some extent, responsible for their diagnoses. Despite this belief, however, Americans are largely supportive of mental healthcare coverage. On average, participants indicated that 87 percent of the patient’s medication should be covered by insurance. Moreover, approximately half of the sample (48 percent) reported that the company should provide 100 percent coverage, and approximately half of the sample (56 percent) agreed to have their names added to the petition.
Table 2 presents unadjusted partisan differences for these same variables. The main comparison groups together those who display any affinity toward a party and compares Democrats and Republicans, excluding those who do not lean toward either party, are Independents, or have no party identification. Regarding personal responsibility, Republicans assigned, on average, approximately 49 percentage points to factors within the patient’s control. Democrats, on the other hand, assigned significantly fewer percentage points—approximately 41 percent—to factors within the patient’s control (p < .01). When asked about their support for coverage, Democrats indicated that 91 percent of the patient’s prescription drug costs should be covered by insurance. This is nearly 10 percentage points higher than Republicans, who indicated approximately 82 percent of the costs should be covered (p < .01). Moreover, about 57 percent of Democrats believed that insurance should cover 100 percent of the costs, compared to only 38 percent of their Republican counterparts (p < .01). In addition, a clear 65 percent majority of Democrats agreed to sign the petition urging the insurance company to cover GAD-related prescription costs. Meanwhile, only 44 percent of Republicans agreed to sign the petition. 3
Study 1, Personal Responsibility and Support for Mental Health Coverage by Political Orientation.
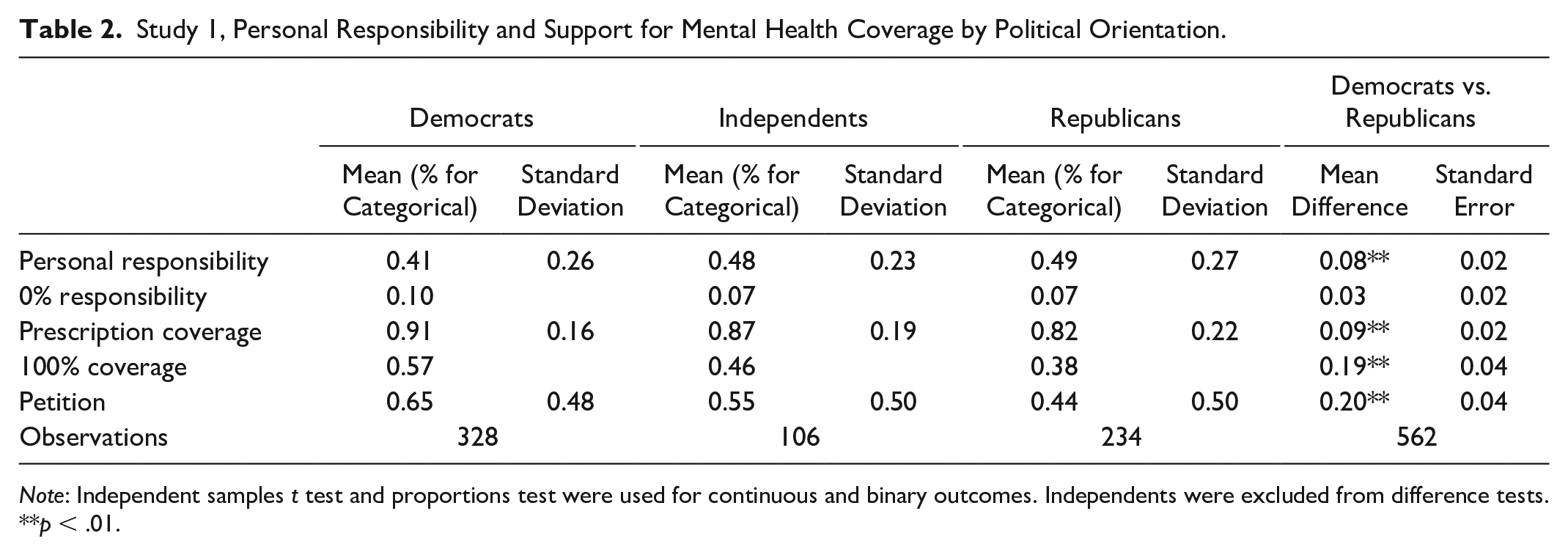
Note: Independent samples t test and proportions test were used for continuous and binary outcomes. Independents were excluded from difference tests.
p < .01.
Table 3 presents results from the zero-inflated beta regression models predicting personal responsibility and one-inflated beta regression models predicting prescription coverage, controlling for vignette characteristics and respondent demographics. Echoing our bivariate findings, respondents who identified more strongly with the Republican party assigned more personal responsibility to the patient (p < .01) and allocated a smaller proportion of prescription costs to the patient (p < .01). Moreover, they were less likely to believe that the insurance company should cover 100 percent of the prescription costs (p < .01). Table 3 also presents logistic regression results for a model predicting petition-signing behavior and reveals that Republican identification is negatively associated with signing the petition (p < .01). Holding all other variables at their observed values, a respondent with a strong Democratic identity would sign the petition about 67 percent of the time. A respondent with a strong Republican identity would sign about 42 percent of the time.
Study 1, Results from Zero- and One-Inflated Beta Regressions.

p < .10. *p < .05. **p < .01.
Note: Standard errors are in parentheses.
The final two models in Table 3 examine the possibility that conservatives allocate less prescription coverage because they perceive mental health patients to be more personally responsible for their diagnoses. Specifically, they estimate a beta regression for prescription coverage, as above, but include perceptions of personal responsibility in the model. Here, responsibility is highly significant and negative in both the proportion (p < .05) and one-inflated parts of the model (p < .01). As people attribute less responsibility to the patient, they recommend greater prescription coverage and are more likely to recommend 100 percent coverage. Yet by including personal responsibility, the effect of party identification on our dependent variables (prescription coverage, 100 percent coverage, and petition signing) is not attenuated in terms of either magnitude or significance. Thus, although it is true that conservatives believe GAD patients to be more responsible for their diagnoses and that conservatives believe GAD patients are less deserving of healthcare as measured by prescription coverage and petition signing, perceptions of responsibility do not account for the relationship between party identification and coverage support.
Study 2: Data and Methods
By way of triangulation, we collected a supplemental nationwide sample of participants via Amazon’s Mechanical Turk (MTurk) to examine the relationship between political orientation and mental illness beliefs in the context of schizophrenia. Each participant was paid $0.50 for participating. Study 2 was virtually identical in design; however, all vignette dimensions were held constant. The vignette read as follows: Michael is a 24-year-old white male who was born and raised in the U.S. Michael has a history of delusions, disorganized thinking, and atypical motor behavior. After a full examination and assessment, a doctor diagnosed Michael with schizophrenia, a mental disorder in which people interpret reality abnormally.
4
Respondents’ demographic characteristics were assessed with the same battery of questions asked of AmeriSpeak panelists upon selection into the sample; however, in addition to assessing partisan beliefs on an ordinal scale—a measure that taps into respondents’ strength of affiliation—we also assessed partisanship categorically by asking participants to self-identify themselves as Democrats, Republicans, Independents, or none.
All dependent variable questions remained the same; however, given political rhetoric linking mental illness and gun violence, we asked two additional questions related to gun control. Specifically, participants were asked to indicate their level of agreement (1 = strongly disagree, 7 = strongly agree) with the statement, “Michael should have the right to buy a gun in the United States,” and to answer an open-ended question (“Why do you think Michael should or should not have the right to buy a gun in the United States?”) to further explain their responses.
MTurk
MTurk is an online crowdsourcing marketplace that matches “workers” with “requesters” who post jobs—or “human intelligence tasks”—for pay that computers cannot do (e.g., rate photographs, transcribe audio recordings, participate in social science research). Given that MTurk provides a convenience sample, the findings from study 2 are not statistically generalizable. Nevertheless, they serve to assess the validity of study 1’s conclusions. Moreover, previous research finds that MTurk respondents are more representative than in-person convenience samples and only modestly less representative than participants in national probability samples (Berinsky, Huber, and Lenz 2012). 5
Given these benefits, MTurk “is arguably one of the most important research tools of the past decade” (Chmielewski and Kucker 2019, advance online publication, no page number), with tens of thousands of scientists utilizing the platform to conduct empirical social science research across a variety of fields. It should be noted, however, that in the summer of 2018, MTurk requesters began reporting a sudden decline in data quality. Subsequent investigation revealed that workers had begun using server farms to hide their true location and/or submit multiple human intelligence tasks. Consequently, methodologists issued new recommendations to ensure data quality. For example, researchers should require workers to live in the United States and have high approval ratings based on previous tasks, screen data for consecutive IP addresses, and duplicate geolocations—indicators of bot-generated data—and incorporate response validity indicators into their research designs (e.g., Moss 2018; Chmielewski and Kucker 2019). Following these recommendations, we contracted with MTurk to collect data from 260 respondents, allowing only U.S. workers with approval ratings of 80 percent to view the task. We then screened the data for consecutive IP addresses (N = 119, 44.9 percent) and duplicate geolocations (N = 127, 48.8 percent). After removing these “respondents,” we removed an additional 28 participants who failed to correctly identify the disorder described in the vignette and another participant who failed to answer any of the dependent variable questions, resulting in a final sample of 88 participants.
All analyses are analogous to study 1; however, due to the small sample size, we are unable to include multiple controls in our regression models. Thus, we discuss our naïve models; however, results including various subsets of controls are substantively similar to the findings presented below. In addition, we examine the relationship between party affiliation and beliefs about gun ownership in the context of mental illness with t tests, regression, and analysis of participants’ qualitative responses.
Results
On average, respondents assigned 24 percent responsibility to Michael, the schizophrenic patient described in the vignette. Not surprisingly, given what is known about the heritability of the two disorders, this is lower than the personal responsibility attributed to the GAD patient in study 1. In addition, 23 percent of the sample, higher than the percentage of respondents reported in study 1, indicated that the patient was in no way responsible for his illness. Nevertheless, these measures reveal that the American public does believe schizophrenia patients—like GAD patients—bear some responsibility for their diagnoses. Similarly, as in study 1, Americans are largely supportive of mental healthcare coverage for schizophrenia. On average, participants indicated that Michael’s insurance company should pay 83 percent of Michael’s medication costs; 38 percent of the sample indicated the company should provide 100 percent coverage; 50 percent agreed to sign the petition.
Turning our attention to party differences, again, our results are largely consistent with those reported in study 1. Self-identified Republicans (M = 0.35, SD = 0.22) assigned more than twice as many percentage points to factors within Michael’s control compared to self-identified Democrats (M = 0.16, SD = 0.19) (p < .01), and only 7 percent of Republicans indicated that Michael was in no way personally responsible for his illness. More than five times as many Democrats (37 percent) indicated Michael was in no way responsible (p < .05). In addition, Democrats believed a higher percentage of Michael’s prescription costs should be covered by insurance (Democrats, M = 0.88, SD = 0.16; Republicans, M = 0.72, SD = 0.22) (p < .01), and 43 percent of Democrats supported full prescription coverage, compared to just 14 percent of Republicans (p < .05). In contrast to study 1, however, we found no significant party differences in petition-signing behavior. 6
Next, we examined the results of zero- and one-inflated beta regression models to assess the relationship between liberal and conservative ideology, measured ordinally, and our dependent variables. As above, more conservative respondents ascribed more personal responsibility to Michael (β = 0.162, p < .01), were less likely to believe Michael carries no personal responsibility (β = −0.562, p < .01), allocated smaller proportions of prescription coverage to Michael (β = −0.155, p < .01), and were less likely to support full coverage (β = −0.455, p < .01). In addition, we examined the results of a one-inflated beta model regressing political ideology on prescription coverage, controlling for personal responsibility, to assess the relationship between ideology, personal responsibility, and support. Again, we find that as people attribute more responsibility to the patient, they recommend less prescription coverage (proportion β = −2.423, p < .01) and are less likely to recommend 100 percent coverage (one-inflated β = −4.267, p < .05). In addition, personal responsibility reduces the magnitude and significance of ideology strength on the amount of prescription coverage recommended, although it does not eliminate the effect entirely, nor does it account for the likelihood of recommending 100 percent coverage (proportion β = −0.106, p < .05; one-inflated β = −0.329, p < .05).
Finally, we assessed participants’ beliefs about gun ownership. Overall, participants were reluctant to support Michael’s right to purchase a firearm (M = 2.70, SD = 2.02), although self-identified Republicans (M = 3.24, SD = 2.43) were significantly more amenable to the purchase than were Democrats (M = 2.23, SD = 1.75) (p < .05). Ordinary least squares regression models reveal that strength of affiliation was also associated with gun rights such that participants with more conservative ideological beliefs were more likely to indicate that Michael should be allowed to purchase a gun (β = 0.208, p < .05). In addition, the results of a one-inflated beta regression model reveal that support for Michael’s right to buy a gun and prescription coverage are negatively correlated. As participants indicated greater support for Michael’s right to purchase a gun, they allocated smaller proportions of prescription coverage to Michael (β = −0.102, p < .05) and were marginally less likely to support full coverage (β = −0.197, p < .10).
Open-ended responses provide further insight. By far, the most common response, regardless of party affiliation, was that Michael should not be allowed to purchase a gun due to assumptions about his mental illness and capacity for violence (e.g., “He should not [be allowed to purchase a gun]. He is not mentally stable and he could cause great harm to people”). Yet several Democrats deviated from this narrative, explaining their response in terms of their desire to restrict access to guns more broadly (e.g., “I don’t support anyone owning a gun.”) Several Republicans and Independents also deviated, expressing hesitancy to restrict Michael’s right to bear arms. These responses ranged from unequivocal (e.g., “I feel everyone should have the right to buy anything”) to ambivalent, often pointing to various contingencies on which the decision should rest. For example, one respondent explained, “I think it would be up to his doctor to decide this” and another explained, “Michael has been diagnosed with a medical condition, he has not been convicted of a felony.”
Discussion and Conclusions
Healthcare reform is of central concern to Republican and Democratic voters, and discussion of universal healthcare—including access to mental healthcare—has dominated recent Democratic debates. Yet, little is known about Americans’ views about mental illness and mental healthcare, particularly along party lines. This article addresses this absence by providing insight into Americans’ beliefs regarding the causes of mental illness and support for mental health treatment, an important undertaking given the current state of mental health in the United States. In study 1, we assessed perceptions of responsibility and support for GAD—one of the most common mental health disorders—utilizing a large, nationally representative sample, allowing us to control for a wide range of variables and to generalize our findings to the larger U.S. population. To increase the credibility and validity of our findings, we then conducted a supplemental study utilizing an online convenience sample to assess perceptions of responsibility and support for mental health in the context of schizophrenia. Schizophrenia affects far fewer people; however, the disorder is chronic, requires lifelong treatment, and is thought to stem largely from genetics. Moreover, schizophrenia is often linked with mass violence in public rhetoric, accounting in part for the sudden uptick in interest among politicians to reform mental healthcare. Thus, we included several questions related to gun control. Given the small sample size, however, we were unable to include a wide range of controls, and our findings are not statistically generalizable.
Across both studies, we find that Americans—regardless of party affiliation—attribute mental illness, at least partially, to factors like personal choice that lie within patients’ control. Nevertheless, Americans are generally supportive of mental healthcare coverage as measured by recommended prescription coverage and petition-signing behavior, echoing previous research that finds widespread support for mental healthcare coverage (Hanson 1998; Barry and McGinty 2014; Maust et al. 2015). With respect to partisan differences, however, Republicans attributed greater personal responsibility to patients than did Democrats and were less supportive of mental health treatment. In study 1, Republicans believed a smaller proportion of prescription costs should be covered and were less likely to sign the petition. In the supplemental study, Republicans believed a smaller proportion of prescription costs should be covered; however, there were no differences in petition-signing behavior.
Curiously, perceptions of responsibility did not account for the relationship between political ideology and support for GAD coverage and accounted for only a portion of the relationship between political ideology and support for schizophrenia coverage. In other words, although conservatives believed patients were more responsible for their diagnoses than did liberals, and conservatives were less supportive of mental healthcare coverage for patients, by and large, conservatives were not less supportive because they believed mental health patients were responsible for their illnesses. Rather, we suspect both findings are driven by Republican individualism. For patients, this translates into encouraging persons diagnosed with mental illness to take responsibility for their health. For institutions, this means renouncing coverage mandates in favor of the free market. Both views are congruent with Republican values. Nevertheless, they present an interesting contradiction, particularly when considered alongside current debates about the link between mental illness and violence.
In short, Democrats and Republicans have adopted different “narrative frames” (Fiss and Hirsch 2005; Kaplan 2008) for discussing gun violence, mass shootings, and other forms of intentional violence. Those on the political Left point to gun access as the primary contributing factor; those on the political Right point to mental illness (Philpott-Jones 2018). To be sure, members of both parties buy into the mental illness narrative. For example, President Obama’s gun control initiative provided support for mental health response training, and in study 2, respondents across both parties routinely indicated that schizophrenia implied the potential for mass violence. Despite the ubiquity of this narrative, however, Democrats are more likely than Republicans to support gun control, believing such regulations will keep firearms away from potentially violent—and presumably mentally ill—persons. Conversely, solutions put forth by Republicans have almost exclusively called for improvements in the diagnosis and treatment of mental illness.
Paradoxically, however, we found that Republicans were more likely to blame mental health patients for their illnesses and were less likely to support mental health coverage, compared to Democrats. We account for this seeming inconsistency methodologically. When assessed in the context of gun violence, support for mental health initiatives reflect partisan bias—the tendency for people to reflexively agree with ideas associated with their own political group. For example, following the Stoneman Douglas High School shooting in Parkland, Florida, Americans were asked, “Do you think that mass shootings in this country are more a reflection of problems identifying and treating people with mental health problems or inadequate gun control laws?” A total of 80 percent of Republicans, compared to 33 percent of Democrats, cited mental health problems as the more important factor (Langer 2018). These two frames—that mass shootings are the result of mental illness or the result of gun accessibility—are so firmly entrenched in Republican and Democratic discourse, that respondents toed their respective party lines. Our research design, however, decoupled support for mental healthcare from gun violence, reducing partisan bias. In study 1, participants were asked about personal responsibility and support for mental health with no reference to guns or mass violence. In study 2, participants were asked about gun rights only after assessing personal responsibility and support. In both studies, Republicans were less supportive of mental health treatment than were Democrats. Moreover, participants who strongly believed the patient should be able to buy a gun were the least supportive of treatment. In light of popular Republican rhetoric (e.g., “Guns don’t kill people; mentally ill people kill people.”) and research linking conservatism with the framing of gun violence in terms of mental illness, our findings are disconcerting. At best, they point to an unbeknownst or unacknowledged contradiction. At worst, they suggest an intentional diversion on the part of conservatives to deflect attention away from conversations about gun control.
We would be remiss not to mention that the research linking mental health and gun violence is far from conclusive (DeFoster and Swalve 2019). Although it is true that the mentally ill are statistically more likely to commit gun violence than the general population and that some of the deadliest mass shooters showed signs of narcissism (Bushman 2018; Philpott-Jones 2018), many medical professionals, public health researchers, policy analysts, social scientists, and disabilities advocates argue that mental illness is a poor predictor of gun violence and that the mental illness frame of mass shootings is based on inaccurate assumptions. In reality, only 4 percent of violent crimes in the United States are committed by people with mental illness; some of the most common psychiatric diagnoses have no correlation with violence, and individuals with mental illness are more likely to be victims of assault than perpetrators (Metzl and MacLeish 2015). Moreover, blaming gun violence on mental illness perpetuates inaccurate stereotypes of the mentally ill (Rubin 2016; Hirschtritt and Binder 2018). Nevertheless, our findings speak to the ubiquity of the mental illness narrative.
Of all group conflicts in the United States, partisanship is one of the most divisive. For more than two decades, the gap between Republicans and Democrats has widened, and most Americans believe that political polarization will increase in the future (Schaeffer 2020). Yet this pattern is far from universal. Americans routinely overestimate differences between Republicans and Democrats (Westfall et al. 2015), and there is a surprising degree of overlap on some issues. Thus, while our primary contribution has been to highlight differences between Republicans and Democrats, we conclude with several nonpartisan policy implications of our work. First, in an effort to acknowledge the preferences of their constituents, policy makers on both the Left and the Right should continue to prioritize efforts to address the mental health crisis in the United States. Similarly, given the overall support for mental health treatment expressed by our participants, efforts to require that insurers comply with the Mental Health Parity Act will likely be well received. In addition, our findings shed new light on Americans’ beliefs regarding the origins of mental illness. Our focus on beliefs, regardless of their veracity, is valuable because beliefs shape proposed solutions and policy conversations. Indeed, perceptions of responsibility were negatively correlated with support. Thus, emphasizing factors like genetics and structural discrimination, and deemphasizing the role of choice, may increase support for mental healthcare reform.
Footnotes
Acknowledgements
For helpful feedback, we thank Mary Bernstein, Shelley Correll, James Druckman, Susan Fisk, Jeremy Freese, Nancy Naples, Daisy Reyes, Catherine Taylor, and Lindsey Trimble O’Connor.