
Abstract
Multigenerational caregiving is important because it affects social and economic outcomes. Existing studies usually exclude theoretically and empirically important aspects—emotional care and horizontal care—that may systematically underestimate gender differences. In this study, we comprehensively describe caregiving by gender and age and examine how sensitive estimates are to the inclusion of directions and types of care. Using the Generations and Gender Survey (GGS) in Europe (N = 114,147), we find that women are more likely to provide care than men across the life course, and gender gaps are largest during critical periods for human capital accumulation. Significant gender gaps in favor of more women providing care are found in most countries, especially when emotional caregiving is included, but in some countries, more men provide care at the oldest ages. These findings highlight how measuring caregiving well is critical to understanding the gendered life course.
Keywords
Examining patterns of caregiving and multigenerational caregiving (i.e., the transfer of resources to at least two different generations) by gender and age is important for understanding the ways heavier caregiving duties may disadvantage certain groups over the life course and at critical periods. Although most research has focused on “sandwiched” caregivers, or those who give to a parent and child simultaneously, the consideration of giving to any two different generations (e.g., spouse and parent, parent and grandparent, spouse and adult child) may be increasingly important given longer periods of shared years with spouses and parents and longer transitions to adulthood for children. Exploring multigenerational caregiving may be especially important for understanding the gendered life course in particular, or the ways in which men and women have divergent biographical paths and pacing, linked lives, and turning points that shape inequality (Moen 2001). If women are providing simultaneous care to multiple generations during critical periods for developing human capital and yielding fewer positive outcomes from caregiving (Lin, Fee, and Wu 2012), this may be a source of disadvantage relative to men of similar ages. In addition, some scholars have argued that men’s caregiving is inadequately captured because many in-depth studies focus solely on women’s caregiving (e.g., Bookwala, Newman, and Schulz 2005). There is some evidence that men do provide high levels of caregiving at older ages, sometimes at similar rates as women (Kahn, McGill, and Bianchi 2011; OECD 2011), but few studies have explicitly measured gender gaps in different forms of care at different ages despite changes in men’s other behavior, like housework (Leopold, Skopek, and Schulz 2018).
Multigenerational caregiving is a particularly important issue for aging populations (Dykstra and Hagestad 2016) and, as we argue here, a critical aspect of the gendered life course. Caregiving can have positive effects on both the receiver and giver, for example increasing emotional closeness (Rossi and Rossi 1990), but it can also have negative implications for the caregiver’s own needs and resources (de Oliveira et al. 2015; Lin et al. 2012). Negative outcomes can include emotional strain (Halinski, Duxbury, and Higgins 2018) and constraints on the ability to work or forced exit from the labor force (Pavalko and Artis 1997). These negative effects may compound across the life course and can increase insecurity and intergenerational inequality. By providing care to multiple family members simultaneously, multigenerational caregivers may be at the highest risk of negative outcomes because of the cumulative effects from a “caregiving squeeze” (Pavalko 2011).
Most existing research on gender differences in caregiving focuses on a particular stage of the life course, limiting our ability to see caregiving at different life course stages at the same time (Swartz 2009). To advance scholarship, we examine caregiving across all adult ages in multiple countries to chart the gendered life course. The age at which caregivers provide care for family members can have implications for their own well-being and ability to save or build human capital (Pavalko 2011). Caregivers at young ages may be at the greatest risk for long-term consequences (Becker 2007), and caregivers at older ages are at risk of delayed retirement and reduced savings (Meyer 1990). If women provide more care at multiple points in the life course, this may especially reduce their levels of human capital (Zhan and Montgomery 2003). Despite the importance of understanding caregiving across the life course, more descriptive studies need to document the full extent of gender differences in caregiving by comparing the sensitivity of estimates to multiple definitions across the entire adult life course and in various cultural contexts.
Our study addresses these gaps and answers a call to better count and thereby value care work (England 1992; Folbre 2002). We contribute to the literature by examining gender differences in caregiving to one and multiple generations as well as how the size of the gap is sensitive to the definition by type and direction of care. First, we document patterns of caregiving by both men and women in the last year by country, type of transfer, and direction. We examine the sensitivity of caregiving estimates between definitions used in most studies, which focus on personal care and financial transfers, with those that also include emotional care. This is a significant contribution because emotional care work in general, and particularly within families, is underestimated (Moor and Komter 2012; Thoits 1989), despite its functional value to families and society (Bengtson and Roberts 1991; Rossi and Rossi 1990). Second, we evaluate the sensitivity of multigenerational caregiving estimates to the inclusion of horizontal transfers in giving to any two generations, not just upward and downward transfers. This is a significant contribution to the literature that currently treats multigenerational care as only that given to an adult and child (Dukhovnov and Zagheni 2015; Wiemers and Bianchi 2015), missing additional and potentially costly care given to a spouse, sibling, or friend from the same generation alongside other forms of simultaneous care (e.g., caring for a parent or grandparent). Third, we examine how multigenerational caregiving varies across the life course by gender and age. Gender continues to be a main source of stratification and inequality across the life course (Moen 2001). Therefore, if gender gaps are present across all ages, caregiving may be a critical aspect of the gendered life course. Fourth, we examine country-level differences by testing gender gaps by life course stage and definitions and directions of care. This article emphasizes how types and directions of care included in the definition of caregiving shape the size and pattern of the gender gap in caregiving over the life course.
Background
The Gendered Life Course
The gendered life course framework emphasizes divergent biographical paths and pacing, linked lives, and turning points for men and women (Moen 2001). The fact that women provide more care than men at different points in the life course is thought to contribute to unequal access to resources (Moen et al. 1994; Zhan and Montgomery 2003). Early work in this arena established caregiving as a key component of the gendered life course using small, local samples. For instance, Moen et al.’s (1994) work used retrospective reports of women in New York and showed a monotonic increase in care responsibilities across the life course. Rossi and Rossi (1990) showed variability across the life course using a sample of adult children and parents in the Boston area.
Gender gaps in caregiving have been established at particular points in the life course (e.g., for adults age 50 and older; Da Roit, Hoogenboom, and Weicht 2015) or in one place (e.g., in the United States; Dukhovnov and Zagheni 2015). The gendered life course patterns of care may vary by age and types of care across the entire life course. High caregiving rates for women are common during the middle years of the life course, with women ages 35 to 49 years being the most likely to care for children or the elderly in Europe (Kotowska et al. 2010). Two-thirds of women 35 to 49 years old and 54 percent of European women 25 to 34 years old provide child or grandchild care at least several days per week (Eurofound 2017). In the United States, women are more likely to provide sandwiched care (Dukhovnov and Zagheni 2015) except at the oldest ages (Margolis and Wright 2017), when gender gaps in care narrow, close, or reverse depending on the type and direction of care (Kahn et al. 2011). Trends are similar in Europe (OECD 2011). These pieces of the puzzle suggest that multigenerational care may vary across the life course in more ways than currently captured in literature that uses limited age samples and definitions of care.
Multigenerational Caregiving
Most research on multigenerational caregiving has focused on the “sandwich generation,” a term coined in the early 1980s to refer to the middle-aged Baby Boomers simultaneously caring for elderly parents and dependent children (Pierret 2006). Because sandwiched caregiving measures only include care given to children and parents (Loomis and Booth 1995) or more broadly to an adult and child (Dukhovnov and Zagheni 2015), most studies have focused on samples of middle-age and older adults (Grundy and Henretta 2006; Margolis and Wright 2017). This leaves us without any knowledge about the prevalence of multigenerational caregiving among younger adults (Dykstra 2013). This is a surprising omission considering that in the United States, over half of 19- to 30-year-olds gave support to a parent in the form of emotional care, household help, or a financial transfer (Eggebeen 2005), the same ages that young adults are starting families and careers. Young adulthood may be an especially critical time period to understand caregiving and the gendered life course.
Most existing empirical work explores sandwiched caregiving separately from horizontal care (i.e., care for a spouse, sibling, or friend). For instance, we know that between one quarter and one third of adults ages 50 years and older in Europe provide sandwiched care to a parent and child (Grundy and Henretta 2006). Among Dutch adults, 21.2 percent of adults provide practical care to a sibling, while 77.8 percent provide emotional support to a sibling (Voorpostel and Van Der Lippe 2007). Increasing life expectancy and “longer years of shared lives” with family members (Bengtson 2001) increases the potential years to provide care to more family members. For instance, today’s multigenerational caregivers may be caring for grandchildren and their parents simultaneously, instead of their children and parents (Dykstra 2013), or caring for a spouse alongside caring for an aging parent.
Changing demography may be shifting gender differences in caregiving in interesting ways. Declining mortality rates at older ages for men may mean that spousal care is becoming an increasingly important and critical part of multigenerational caregiving for both men and women, potentially narrowing any gender gap in caregiving in later life (Glauber 2017). Caring for siblings or friends also may become more important in the future as the population of older adults without a partner or children increases (Margolis and Verdery 2017; Verdery and Margolis 2017), siblings share longer lives together (Uhlenberg 1996), and friendships become more important for support as adults age (Huxhold, Miche, and Schüz 2014).
Intergenerational Solidarity
Intergenerational solidarity theory provides an empirical framework for understanding family and interpersonal cohesion through the measurement of multidimensional aspects of caregiving transfers (Bengtson 2001; Bengtson and Roberts 1991). The framework of intergenerational solidarity is multifaceted, and we focus here on functional transfers because they provide services that allows families and greater society to operate. Functional transfers are exchanges of resources (Bengtson and Roberts 1991), and within this framework, there are three main types of functional transfers. The first is time spent on personal care for another person (e.g., child care or elder care). The second is financial transfers (e.g., giving money or a loan to another person). The third type is emotional support (e.g., listening to another person’s problems or emotions) (Bengtson 2001; Bengtson and Roberts 1991). Despite the fact that the theoretical framework includes these three types of functional care, most empirical research documents the prevalence of personal care and financial transfers in different contexts, age groups, and time periods but omit emotional support. For instance, one quarter of European adults are currently providing personal care to a young, elderly, ill, or disabled family member (Ruppanner and Bostean 2014). Among older Europeans (ages 50 years and older), 57 percent of grandparents provided some grandchild care (Hank and Buber 2009). Financial transfers are less common, though the levels depend on the direction. Across Europe, less than 3 percent of adults give financial to generations above them (Deindl and Brandt 2011), while one in five adults in Europe, ages 50 years and older, give money downward to children (Albertini, Kohli, and Vogel 2007).
Population-level empirical studies of emotional support in families are rare (Moor and Komter 2012; Sarkisian and Gerstel 2004). Emotional transfers are important to measure because they are “invisible” labor, often not counted as care work (Erickson 1993; Thoits 1989) despite being vital for personal and family functioning (Bengtson and Roberts 1991) and bonding (Rossi and Rossi 1990). For instance, lack of emotional support is linked to adverse health outcomes, including loneliness and heart conditions in older age (Sorkin, Rook, and Lu 2002). Emotional work at home also can spill over into the caregiver’s workplace and is associated with reduced well-being and increased stress (Wharton and Erickson 1995). Despite its importance, there are few nationally representative estimates of emotional support within families, and studies are often limited to one country (Sarkisian and Gerstel 2004; Schenk and Dykstra 2012).
The types of care given also may depend on the direction of caregiving. Downward transfers are the most common across the life course in Europe (Albertini et al. 2007; Daatland and Lowenstein 2005) but decline as age increases (Kalmijn 2019). Providing personal care and financial transfers upward to parents is uncommon (Albertini et al. 2007; McGarry and Schoeni 1995) except when parents are at the oldest ages and adult children increase their giving to parents (Kalmijn 2019). Caring for a spouse is especially common as people age (Glauber 2017), as are increases in care for siblings (Connidis 1994). Despite a large body of research on intergenerational transfers, very few studies cohesively document patterns of caregiving by type and direction over the entire adult life course by gender (for a recent example using broad care measures, see Kotowska et al. 2010, and for a recent example using time measures, see Dukhonov and Zhageni 2015).
Data
We use data from Wave 1 of the Generations and Gender Survey (GGS), which were collected between 2003 and 2013. The GGS is the best source of data for this project because it provides comparable, nationally representative data of adults in many European countries and includes questions about different forms and directions of care for both men and women. These data allow us to address a few important limitations in prior research such as convenience samples, limited age ranges, samples of only women, lack of an emotional care measure, and measures of multigenerational care that only includes sandwiched care. Appendix Table A1 presents the survey years, response rates, and age ranges of the survey in each country. For more information about response and sampling for the GGS, please see Fokkema et al. (2016) or https://www.ggp-i.org/data/methodology/#toc2.
We include countries in our sample that met the following criteria: (1) countries that surveyed a broad age range of adults ages 18 to 80 years (this excluded Austria), (2) countries with questions about at least two of the following three types and directions of caregiving: personal care, financial transfers, and emotional support (this excluded Hungary, Italy, Estonia, and the Netherlands), and (3) countries with valid GGS weights (this excluded Romania). These exclusion criteria are shown in Appendix Table A1. This yields a sample of 11 of the 17 countries in the first wave of the GGS. The countries in our analysis are Belgium, Bulgaria, Czech Republic, France, Georgia, Germany, Lithuania, Norway, Poland, Russia, and Sweden. The total sample size for the 11 countries was 125,733 respondents. We exclude observations that were missing on our variables of interest, leaving us with an analytic sample of 114,147. We conduct a sensitivity analysis using multiply imputed data and find that estimates and statistical significance for gender differences are similar.
We examine three directions of caregiving: upward, horizontal, and downward, and transfers of different types to up to five individuals. 1 Upward transfers include a mother, father, mother of partner, father of partner, grandmother, or grandfather. Horizontal transfers include a partner/spouse, sister, brother, friend/neighbor/colleague, or previous partner. Downward transfers include general child care, general grandchild care, general care for other children, or personal care for a son, daughter, stepson, stepdaughter, granddaughter, grandson, or partner of a child.
We examine three types of functional caregiving provided over the last 12 months: personal care, financial transfers, and emotional support. For personal care, respondents giving any of the following are counted as caregiving: “personal care such as eating, getting up, dressing, bathing, or using toilets”; helping with any child care tasks for one’s own children, including: dressing, putting to bed, illness, leisure, homework, transportation; “child care to other people”; and “help to look after your grandchild(ren).” For financial transfers, respondents were asked: “Have you or your partner/spouse given for one time, occasionally, or regularly money, assets, or goods of substantive value to a person outside the household? Please think also about land and property you or your partner/spouse transferred during this time.” For emotional support, respondents were asked: “Has anyone talked to you about his/her personal experiences and feelings?” Very few population-based surveys have any items regarding emotional caregiving—an important theoretical concept within functional exchanges in intergenerational solidarity theory. We can capture emotional support given to family members as well as support for nonfamily members.
We use information about the three types of caregiving (personal care, financial transfers, and emotional support) given either upward, horizontal, or downward to create two measures of multigenerational caregiving. First, sandwiched caregiving is when respondents give to family members above and below them, the most traditional definition of multigenerational care. Second, our more inclusive measure captures a respondent caring for at least two different generations of family members or friends/colleagues/neighbors, including upward, downward, and horizontal, simultaneously.
Methods
First, we describe the prevalence and directions of caregiving across all ages by country (Table 1). Second, we illustrate the life course patterns by gender of caregiving, contrasting the exclusion and inclusion of emotional support, across all countries in the sample (Figure 1). Third, to illustrate the directional composition of any caregiving with and without emotional support, we illustrate how the life course pattern of caregiving varies by direction across all countries (Figures 2A, 2B). Fourth, we illustrate how the life course pattern of multigenerational caregiving varies by gender and age across all countries, dependent on the definition of multigenerational caregiving (Figure 3). Fifth, we estimate a series of adjusted, weighted predicted probabilities of providing multigenerational care using logistic regression models, controlling for country and survey year, with gender and age interactions (Table 2). Last, we test whether the gender and age differences that we find overall for all countries (shown in Table 2) are similar for each of the countries in the analysis or whether countries have different age/gender patterns (Table 3). All estimates are weighted to be nationally representative of the countries in our sample.
Percentage of Adults, Ages 18 to 80 Years, Providing Different Forms of Care by Direction in the Last Year.
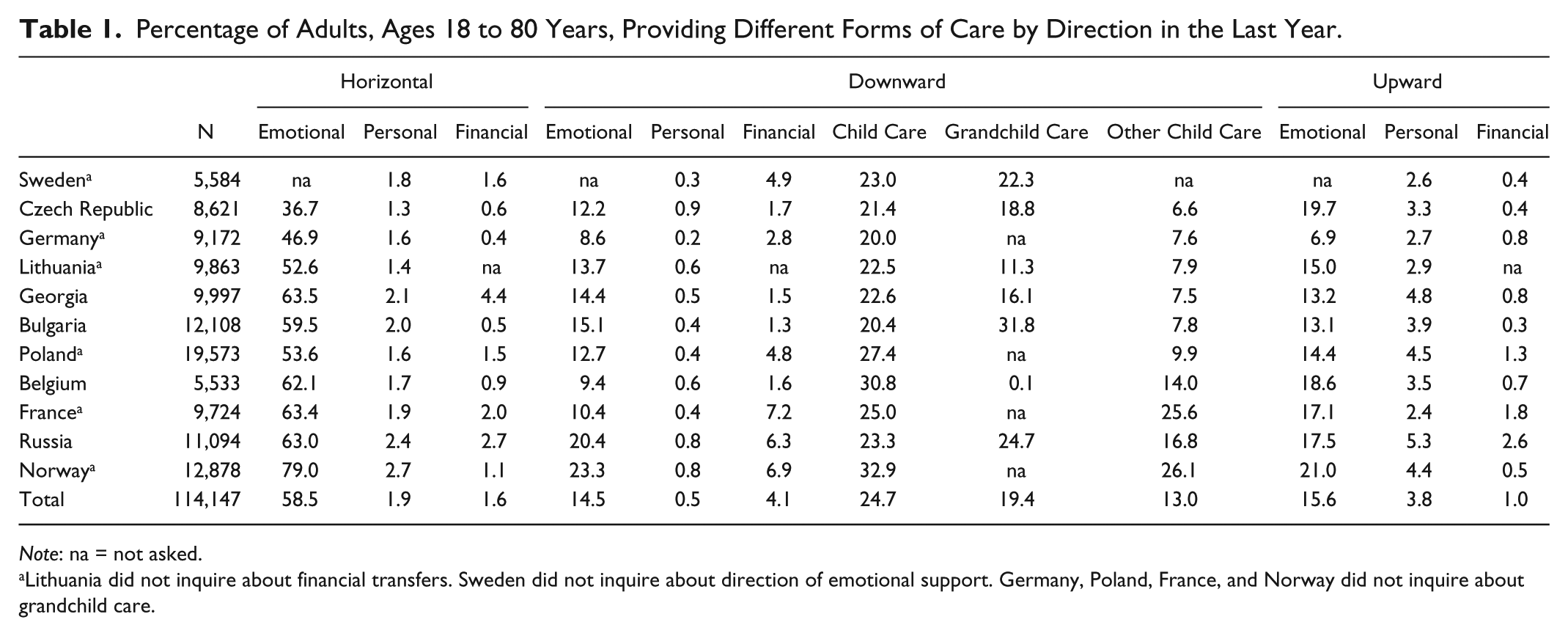
Note: na = not asked.
Lithuania did not inquire about financial transfers. Sweden did not inquire about direction of emotional support. Germany, Poland, France, and Norway did not inquire about grandchild care.

Percentage of respondents by gender and age providing any care to anyone in the last year among all countries, by type of care provided.

Percentage of respondents by gender and age providing different directions and types of care in the last year among all countries. (A) Includes personal care or financial transfers only. (B) Includes personal care, financial transfers, or emotional support.

Percentage of respondents by gender and age providing multigenerational care in the last year among all countries, includes personal care, financial transfers, or emotional support.
Adjusted Predicted Probability of Providing Care by Sex and Age Group, from Weighted Logistic Regression Models Controlling for Country and Survey Year.

Note: Pairwise test between men and women within each age group. Confidence intervals in parentheses.
p < .05. **p < .01. ***p < .001.
Adjusted Predicted Probability of Providing Care for Each Country by Sex and Age Group, from Weighted Logistic Regression Models Controlling for Year. (continues on next page).

Note: Sandwiched = simultaneous care to the generation below and above respondent; at least two generations = simultaneous care for any two generations. N.A. = no respondents report multigenerational care.
Lithuania did not inquire about financial transfers. Sweden did not inquire about direction of emotional support. Germany, Poland, France, and Norway did not inquire about grandchild care.
p < .05. **p < .01. ***p < .001.
Results
Table 1 examines the types of care that respondents provide horizontally, downward, and upward. Emotional support is the most common type of horizontal caregiving (to a partner, sibling, or friend). Across the 11 countries, 58.5 percent of adults provide horizontal emotional support, ranging from 8 in 10 in Norway to 36.7 percent in the Czech Republic. Giving personal or financial support horizontally is much less common (1.9 percent and 1.6 percent, respectively). Downward caregiving is the next most common direction of care, and this category is dominated by child care. One in four adults (24.7 percent) provides care to his or her own child, almost one in five (19.4 percent) provides grandchild care, and one in eight (13.0 percent) provides care to “other” children. Besides child care, downward emotional support is the next largest category of care (14.5 percent), followed by financial transfers (4.1 percent) and personal care (0.5 percent). For upward transfers, emotional support is the most common type of transfer (15.6 percent), followed by personal help (3.8 percent) and financial help (1.0 percent). Across all the countries in our sample, emotional support and horizontal care are substantial categories, and their inclusion will greatly affect estimates of caregiving.
Next, we examine patterns of any caregiving (including horizontal, downward, and upward) by gender and age, with only personal care and financial transfers (grey lines, Figure 1) and then with the inclusion of emotional support (black lines, Figure 1). Including only personal care and financial transfers, we see an “M” shaped curve over the life course where caregiving peaks at ages 30 to 34 years at 81.4 percent for women and at ages 35 to 39 years at 63.2 percent for men. This level then declines in the mid-40s but increases slightly again to another peak at ages 60 to 64 years for women and 65 to 69 years for men. Providing these two types of care is significantly more common among women than men at all ages (ages 18–69 years; p < .001) except at the oldest ages. The gender gaps in providing personal care and financial transfers are largest in young adulthood at ages 18 to 34 years, peaking at a 29-percentage point different for those 25 to 29 years, a 25-percentage point different for 30- to 34-year-olds, and an 18-percentage point difference for those 18 to 24 years.
The top two lines show that estimates of caregiving are substantially higher when including emotional support; the pattern smooths out, and the age patterns shift. Inclusion of emotional support keeps levels of caregiving across the life course above 70 percent for women and 65 percent for men, respectively, except at the very oldest ages (75–80 years). This measure peaks at 30 to 34 years (94.0 percent) for women and 35 to 39 years (82.0 percent) for men, over a 12-percentage point increase for women at this age and almost a 19-percentage point difference for men of this age. This comparison affirms the importance of measuring emotional support for understanding caregiving by both men and women across the life course.
Next, we break down any caregiving by direction to further understand how inclusion of emotional support affects estimates. Figure 2A includes only personal care and financial transfers, and Figure 2B includes personal care, financial transfers, and emotional support. First, we examine downward caregiving. In both figures, downward transfers follow an “M” pattern for both men and women, where most respondents provide care to younger generations in early adulthood and then again in middle age. The levels of downward caregiving are slightly higher when including emotional support, but overall, downward caregiving is well captured by including just personal care and financial transfers.
In Figure 2B, women are more likely to provide downward care throughout the life course until older ages, when differences decline to seven percentage points among those 70 to 74 years old, and then gender trends reverse at the oldest ages. Interestingly, the direction of the gender gap in downward caregiving is consistent across the two definitions of care, but the inclusion of emotional support widens the magnitude of the gap in middle and older ages. For instance, the gender gap in downward care is a four percentage-point difference for those 40 to 44 years old in Figure 2A but widens to a nine percentage point difference in Figure 2B. This suggests that emotional support is an important component of the caregiving that women provide to their children, even at older ages, and critical to measure functional solidarity properly. No matter whether emotional support is included, the largest gender gap in downward care is at ages 25 to 29 years, a 31 percentage-point difference (p < .001).
Figures 2A and 2B also show horizontal and upward caregiving. Horizontal and upward caregiving are not very common throughout the life course when including just personal care and financial transfer (Figure 2A). Among men, the percentage providing horizontal care ranges from 2.3 percent to 5.5 percent, and for women, the numbers are similar (2.4 percent–6.2 percent). Upward care ranges from 0.4 percent to 5.0 percent for men and from 0.4 percent to 8.8 percent for women, depending on age. Horizontal caregiving that includes personal care or financial transfers are uncommon but increase over the life course, peaking at ages 70 to 74 years for women (6.2 percent providing care) and at ages 75 to 80 years for men (5.5 percent providing care). Upward care, when including just personal care and financial transfers, peaks for women at ages 50 to 54 years and 55 to 59 years (8.8 percent for both) and for men between 45 and 49 years (5.0 percent).
The gender gaps in horizontal and upward caregiving are greatly underestimated without including emotional support (Figure 2B vs. 2A). Including all three types of caregiving increases the prevalence of horizontal and upward caregiving across the life course. When we include emotional support, the higher level of caregiving performed by women early in the adult life course is dramatic, reaching 70.6 percent for horizontal caregiving (11 percentage points greater than men) and 36.8 percent for upward care (14 percentage points greater than men) for women 18 to 24 years (p < .001). These results show that estimates of caregiving that only focus on personal care and financial transfers severely underestimate large portions of potentially important emotional support younger family members provide to older family members.
Figure 3 examines the life course pattern of sandwiched caregiving (giving to a generation above and below) and multigenerational caregiving (giving to any two generations). Both definitions of multigenerational caregiving have the same shape, peaking in young adulthood and then slowly decreasing with age, but the levels are very different. Caregiving is much more prevalent when we include care to any two generations rather than just the older and younger generations (sandwiched); this finding emphasizes the importance of including horizontal generations in definitions of multigenerational care to clearly understand the caregiving squeeze. For women ages 30 to 34 years, one in four (26.7 percent) are sandwiched, and this increases to almost two of three (64.8 percent) when including giving in any two directions simultaneously. For men ages 35 to 39 years, one in six (12.5 percent) are sandwiched, compared to over two in five (45.4 percent) being multigenerational caregivers. Gender gaps are largest in young adulthood with a 15 percentage-point difference for those 30 to 34 years who are sandwiched and a 23 percentage-point difference at 25 to 29 years for multigenerational caregivers. Gender gaps are wider for multigenerational care among middle age, compared to sandwiched care, and both definitions remain significant for the majority of the life course (p < .001).
We further test the size of the gender gaps by estimating the predicted probability of providing care by age group and for four definitions of multigenerational care with some simple multivariate models (Table 2, full models shown in Appendix Table A2). These findings echo the descriptive findings shown previously. The sizes of the gender gaps in caregiving are largest with the broadest definitions of multigenerational care and smallest with the narrowest measures. This is due to the huge gender gap in emotional support. Including emotional support is also important for capturing a large gender gap early in the life course, where the gap is twice as large for multigenerational caregiving (for any two generations) than sandwiched caregiving.
We also estimate predicted probabilities for each country in Table 3 and compare the country-level gender gap in caregiving to that for all countries presented in Table 2. Overall, most pairwise comparisons between men and women in each age category continue to be significant across most countries and age groups. However, there are some interesting exceptions where we do not find a significant gender gap within particular countries depending on how we define multigenerational caregiving. The top half of Table 3 shows estimates for both sandwiched and at least two generation caregiving without the inclusion of emotional support. Some estimates indicate that there are not significant gender gaps by age group in some countries, for instance in France and Germany, when we only include personal care and financial transfers. However, the bottom half of Table 3 includes emotional support, and we show that more countries have significant gender gaps in multigenerational caregiving across age groups.
Looking across the life course by each country, gender gaps fluctuate more at the oldest ages (ages 65–80 years in our survey). For instance, the bottom right panel of Table 3 presents estimates of multigenerational care that includes any two generations and personal care, financial transfers, and emotional support. Here, we find that gender gaps reverse at the oldest ages in Bulgaria and Georgia, with men reporting more multigenerational care, but that the traditional gender gap, with women giving more than men, is larger in countries like Lithuania and Norway.
Sensitivity Analysis
To test the robustness of the main results, we also completed several additional analyses. First, we conducted our analysis including only countries with all of the caregiving questions, (Bulgaria, Russia, Georgia, Belgium, and the Czech Republic) and found results similar to the main results. These are shown in Appendix Table A4 and can be compared with Table 3 in the main text. Second, we tested the sensitivity of the main results to the exclusion of missing individual-level data by using multiple imputation (chained imputation, M = 10), and we found similar patterns of results. Gender differences continue to be significant at roughly the same levels across the life course. Third, we examined to what extent estimates of horizontal multigenerational caregiving are to the inclusion of nonfamily members (friends, neighbors, or colleagues). These results can be found in Appendix Figure A1 and Table A5. These additional analyses show some differences in estimates of horizontal care, as expected. Excluding friends reduces the prevalence of caregiving overall by both men and women but more so for women at older ages. This shows that women are more likely than men to be caring for friends across the life course and especially at older ages. Another interesting finding that becomes apparent is that although men have a higher prevalence of caregiving at older ages, this is more likely care given to a spouse since they are more likely than women at these ages to be married.
Last, we examined how estimates of caregiving change when we include coresidence as a fourth dimension of caregiving. Our three main measures of caregiving (personal, financial, emotional) can be to people whether coresident or not, and this fourth dimension includes coresiding with someone as a type of caregiving. Appendix Table A6 shows our estimates of caregiving both with and without including coresidence as a fourth dimension of caregiving. Results on the left side of the table show the percentage of adults performing any caregiving increases with the inclusion of coresidence—this increase is particularly large for horizontal caregiving since coresidence is almost universal with a spouse and much smaller for downward and upward caregiving. On the right side, we find that sandwiched caregiving estimates increase only a small amount in countries where coresidence with older kin is uncommon (e.g., Germany, Sweden) and increase substantially in eastern European countries like Bulgaria, Georgia, and Russia, where it is more common. Across all countries, however, including coresidence in caregiving for any two generations increases estimates substantially since coresidence is almost universal with a spouse, which would be counted as horizontal caregiving.
Discussion
Multigenerational caregiving is an important part of family life, but caregiving is often undercounted and thereby undervalued (England 1992; Folbre 2002; Glenn 2010). Our findings highlight the importance of how caregiving is defined and measured for understanding caregiving as a critical aspect of the gendered life course. We find that the undercount of caregiving disproportionately affects measures of women’s caregiving, particularly when we examine an important aspect of functional solidarity (Bengtson and Roberts 1991)—emotional caregiving.
Our results build on numerous published studies on different age groups, cohorts, and places, which have documented that women are more likely than men to be caring at each life course stage (Dukhovnov and Zagheni 2015; Moen et al. 1994; Robards, Vlachantoni, and Evandrou 2015), with some exceptions at the end of the life course (OECD 2011). Ours is the first study to use multicountry national-level data to clearly document the full extent of the gendered life course of caregiving roles by direction and type of care given. Using a hypothetical cohort, we show that gender gaps are largest at critical periods of the life course for accumulating human capital: at the youngest ages of adulthood and in the middle years. For instance, recent work in the United States has found that providing care for a parent in midlife is associated with a reduction in women’s wages but not men’s wages (Glauber 2019). More research is needed to understand the nexus of individual, family, and structural influences on caregiving (Moen and DePasquale 2017) given that welfare state programs, like cash benefits paid to seniors, often influence women’s participation in care but not men’s (Haberkern, Schmid, and Szydlik 2015).
Capturing emotional support shows that excluding it from many other studies has important implications for both women and men. Our results also show that many young adults are providing emotional support upward to parents or other older family members and women in the middle ages report high levels of emotional support downward for children or other younger family members. Emotional care is important for family cohesion (Bengtson and Roberts 1991), especially for men’s integration into families (Erickson 1993). By including diverse definitions of caregiving across the life course and using a population-based survey of both men and women, our study also responds to critiques of caregiving literature that argue men’s caregiving is not captured (Bookwala et al. 2005). We encourage surveys to further develop questions about the complexities of these types of care, including the ways in which other people encourage caregiving within families (Gerstel and Gallagher 2001). Given the magnitude of emotional support, we urge scholars to work to better understand this type of caregiving and include it in more surveys as a part of functional solidarity.
Our findings also highlight the particular importance of horizontal care in measuring the caregiving squeeze (Pavalko 2011). Sandwiched caregivers are more likely to report stress and work-family balance issues compared to caregivers who only provide to one generation of family members (i.e., child or elder care) at a time (Halinski et al. 2018), but most current studies often do not include horizontal care in multigenerational caregiving and rather focus on sandwiched caregiving (i.e., caring for a parent and child). We find that excluding horizontal caregiving rather than focusing on care to any two generations underestimates the gender gap since women are more likely to provide horizontal care until the oldest ages. With longer years of shared lives (Bengtson 2001), we argue that we cannot fully understand the ways in which women are squeezed by multigenerational caregiving if we omit horizontal care from the combinations of care.
Additionally, our findings using an expanded definition of multigenerational care clearly show the biggest squeezes for both men and women occurring at two critical points in the life course—early adulthood and near retirement age. For young adults who are providing multigenerational caregiving at the same time they are trying to attach to the labor force, these disparities in care could have implications for their early career development and cumulative human capital attainment. It is important to enumerate and track caregiving occurring early in the life course to better understand how cumulative effects, both positive and negative, may build over times for caregivers, especially those in young adulthood (Becker 2007; Hunt, Levine, and Naiditch 2005). For middle-age adults who are near retirement, having more caregiving responsibilities may delay or forgo their ability to retire, potentially impacting the caregivers’ own financial well-being at the end of their life. In addition, understanding multigenerational care and gender differences has important implications for assessing family care needs in workplace and country- or state-level policies (Moen and DePasquale 2017). A recent study estimates that the cost to replace informal caregiving of older family members with formal care would be over $17,000 year in the United States (Cecchini 2018); this cost would only be larger for those giving to multiple family members at once. Overall, the undercounting and undervaluing of caregiving across the life course mutes the contributions of caregivers to society.
It is important to understand when in the life course caregivers are being squeezed as fertility, morbidity, and mortality patterns in these countries shift over time (Albertini and Mencarini 2014; Herlofson and Hagestad 2011; Leopold and Skopek 2015; Zagheni and Wagner 2015) and how patterns may also vary by socioeconomic status (Margolis and Wright 2017), country welfare regimes (Haberkern et al. 2015), and migration status (Spitzer et al. 2003). As multigenerational relationships continue to be important for families and populations continue aging, it is critical to understand the timing of caregiving over the life course. Future research could consider understanding multiple and coinciding roles throughout the life course (e.g., labor force participation) and further explore the demographic explanatory mechanisms behind caregiving across the life course (Albertini 2016; Puur et al. 2011).
The Generations and Gender Survey is valuable because it is the only data source that provides nationally representative, population-level data across adulthood for both men and women for many countries and different types of caregiving. However, our study has limitations. First, our measure of emotional support is very limited in terms of what it captures and by only asking one question. Because emotional caregiving is complex and potentially multidimensional, we encourage survey designers to consider developing a multiitem scale of emotional support similar to items in Krause and Markides’s (1990) social support scale, which focuses on the care receiver only. A second limitation of the data is that not all countries fielded all questions or inquired about the direction of care, and the personal care question is limited to Activities of Daily Living, the most extreme form of care. Both of these limitations mean that our estimates of caregiving are conservative. We encourage nationally representative surveys to consider more in-depth caregiving modules and harmonize measures across countries as much as possible (Emery and Mudrazija 2015; Fokkema et al. 2016). A third limitation is that the questions ask about caregiving “in the last year,” which leaves us unable to provide estimates for how common it is to provide multigenerational care over a larger time period or pinpoint any episodic or long-term care. Fourth, the cross-sectional nature of our data allows us to examine a broad age range, but we cannot examine changes within individuals’ lives or distinguish between age and cohort differences in caregiving. We are encouraged by the recent calls for data sets to collect caregiving data longitudinally and across countries (Fokkema et al. 2016; Seltzer 2015). Finally, coresidence can be seen as a type of transfer, but we did not include it as a type of transfer in our main results because it is difficult to tease apart who is supporting whom (Dykstra 2010). However, our sensitivity analysis shows that all measures of care increase with the inclusion of coresidence as a type of caregiving (Appendix Table A4); this is an important avenue for future research.
Our study emphasizes the importance of measurement for understanding levels of caregiving and the gendered life course. Given the variability we find in caregiving across the life course, our findings imply that we may have been underestimating the effects of caregiving for women on intergenerational inequality and human capital accumulation across the life course. To truly value caregiving, we as scholars must strive to better measure the complexity of caregiving across the life course.
Footnotes
Appendix
Percentage of Adults, Ages 18 to 80 Years, Providing Any Care (Personal Care, Financial Transfers, Emotional Support) by Direction in the Last Year with and without the Inclusion of Coresidence as a Type of Caregiving.

| Any Caregiving | Multigenerational Caregiving | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Excluding Coresidence | Including Coresidence | Excluding Coresidence | Including Coresidence | ||||||||
| N | Horizontal | Downward | Upward | Horizontal | Downward | Upward | Sandwiched | At Least Two Generations | Sandwiched | At Least Two Generations | |
| Sweden a | 5,584 | 3.3 | 47.1 | 3.0 | 70.8 | 55.4 | 8.5 | 1.4 | 2.9 | 2.3 | 48.6 |
| Czech Republic | 8,621 | 37.4 | 48.0 | 21.8 | 77.7 | 60.8 | 35.3 | 11.2 | 31.8 | 16.0 | 67.3 |
| Germany a | 9,172 | 47.7 | 34.3 | 9.7 | 81.4 | 47.1 | 15.4 | 4.3 | 24.8 | 6.1 | 50.5 |
| Lithuania a | 9,863 | 53.1 | 44.3 | 17.1 | 79.0 | 56.9 | 29.5 | 8.4 | 35.1 | 13.4 | 72.1 |
| Georgia | 9,997 | 64.9 | 49.0 | 17.4 | 88.0 | 71.0 | 47.7 | 8.6 | 41.3 | 27.3 | 82.7 |
| Bulgaria | 12,108 | 60.3 | 59.1 | 16.2 | 87.2 | 74.4 | 36.5 | 8.6 | 43.5 | 19.0 | 82.3 |
| Poland a | 19,573 | 54.5 | 47.2 | 18.8 | 86.0 | 62.5 | 35.6 | 9.9 | 37.8 | 17.6 | 72.1 |
| Belgium | 5,533 | 62.8 | 47.0 | 21.7 | 91.1 | 61.6 | 33.2 | 12.5 | 42.1 | 16.3 | 74.0 |
| France a | 9,724 | 64.3 | 52.9 | 20.1 | 92.1 | 62.9 | 27.5 | 12.1 | 45.3 | 15.3 | 71.3 |
| Russia | 11,094 | 63.9 | 61.9 | 22.7 | 88.1 | 76.7 | 38.3 | 14.8 | 50.2 | 25.3 | 81.8 |
| Norway a | 12,878 | 79.7 | 66.9 | 24.4 | 94.7 | 74.1 | 29.4 | 16.8 | 63.1 | 19.4 | 80.8 |
| Total | 114,147 | 56.6 | 51.5 | 18.3 | 85.9 | 65.0 | 32.0 | 10.3 | 40.2 | 17.1 | 72.0 |
Note: Coresidence measures: downward coresidence = children age 14 years and younger; horizontal coresidence = partner, siblings; upward coresidence = parent, grandparent.
Lithuania did not inquire about financial transfers. Sweden did not inquire about direction of emotional support. Germany, Poland, France, and Norway did not inquire about grandchild care.
Acknowledgements
Thank you to CREW for feedback on this article and Tom Emery for help with the data.
Authors’ Note
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Joint Programming Initiative, More Years Better Lives funding from the Canadian Institute of Health Research (MYB-150262) and Social Sciences and Humanities Research Council of Canada (435-2017-0618, 890-2016-9000).
1
Some countries had the option of reporting more than five people, but reports of transfers to more than five people were extremely rare. Therefore, a cap on five persons was used across all items for consistency. Analysis with all cases show no difference in results.