
Abstract
Sociological research has demonstrated that peers play a role in patterns of deviance. Yet, examinations of competing mechanisms in continued patterns of deviance are less well developed. We simultaneously examine multiple peer mechanisms of action on prescription drug misuse. Results identify drug sources, peer group norms, and a desire to enhance social experiences as important factors in the frequency of misuse, non-oral administration, and dependence, whereas peer pressure had no effect net of other peer factors. The results emphasize the importance of considering multiple peer mechanisms in shaping deviance, and as such, future scholarly examinations should focus on multiple dimensions of peer effects to fully understand patterns of continuing deviance.
Introduction
The role of peer groups in deviance has been a central focus of sociological research for nearly a century. Despite such a storied research history, the relationships between peers and deviant behaviors continue to be evaluated and explained. To further this literature, we study multiple mechanisms of action through which peers are associated with continuing patterns of deviance, using prescription drug misuse as the analytic object of focus. Building on previous sociological and criminological research, we delineate four pathways—peer network accessibility, peer drug associations, peer pressure, and the pursuit of pleasant times with peers—through which peer groups play a role in deviance. As Warr (2002:78) emphasizes, “It is well enough to say that behavior responds to reinforcement, but it is another to actually identify or isolate the precise sources of reinforcement that operate in everyday life.” In this tradition, we investigate the four peer mechanisms on patterns of substance use through mixed-methods analysis. Importantly, we examine these peer factors simultaneously on outcomes of interest to evaluate holistically the role of peer mechanisms. Furthermore, our focus on patterns of misuse among active users—frequency of misuse, escalation to non-oral administration, and signs of prescription drug dependency—underscores the mechanisms by which drug-using peer groups play a role in continuing patterns of use. As such, we further extend the implications for the study of peer effects on the continuation of deviance beyond simply whether or not individuals engage in the behavior. With prescription drug misuse a major drug trend during the twenty-first century (McCabe, Teter, and Boyd 2006), this phenomenon serves as an opportunity to examine the role of peers in continuing patterns of drug use and provides a vehicle to apply and expand sociological theories of peers and deviance more broadly.
Peer Effects and Drug Use
A long line of sociological theory and research has elucidated the social influences underlying individual deviant behavior, with a strong focus on the effects of peer groups. Sutherland (1939) generated this research direction through his classic work on differential association, a theory that stressed the importance of group affiliation and norms in learning deviant behavior. Its successor, social learning theory (Burgess and Akers 1966), added that differential association, definitions, and imitation are accompanied by a fourth component, differential reinforcement, which describes the social rewards and costs associated with behavior. Becker’s (1963) prominent work also emphasized this process of reassigning positive labels to drug use and to drug-using groups through social interaction. Beyond his contribution to understanding the role of peer groups at initiation, Becker described what happens once use becomes regular and how users construct a new framework for their practices, namely, obtaining a personal supply, a system for keeping the behavior secret, updated definitions favorable toward drug use, and increased interactions with experienced users. Thus, the role of peers in deviance has long been an important focus within sociology and remains a key area of inquiry.
In the field of substance use research, a large share of the literature on peers has focused on alcohol, tobacco, and marijuana use among adolescents, with less emphasis on other drugs or later life course stages. Scholars have centered attention on the role of friends specifically as they, rather than a general social crowd, act as key influences on substance use (Urberg 1992; Urberg, Degirmencioglu, and Pilgrim 1997). Adolescents who are more highly involved with substance-using peers show an increased risk for personal use (Hussong 2002). Furthermore, peer effects may intensify as a distancing from family norms and increasing importance of friends occurs during the transition from adolescence to young adulthood (Thornberry 1987). During this transition, young people more fully embrace the norms of their peers, who are more likely to shape substance-using decisions. Yet, while numerous studies have found similarities between individuals and their peers on behaviors and attitudes related to drug use, the focus has largely been on the relationship between peers’ substance use and personal use. In other words, having peers involved in deviant activities is associated with a higher odds of deviant behavior (Agnew 1991; Guo et al. 2002; Haynie 2001; Knecht et al. 2010; Mercken et al. 2010; Weerman 2011). Moving beyond examinations of any deviance by peers to consider the actual mechanisms of influence is particularly important as studies have identified the role of misperceptions of peer behavior in deviance (Boman et al. 2014; Young et al. 2011).
Whereas peer use has been identified as a predictor of personal use in numerous studies (e.g., Jensen 1972; Johnson, Marcos, and Bahr 2006; Thornberry et al. 1994; Warr 1993; Warr and Stafford 1991; Weerman 2011) and innovations in network methods have allowed for greater distinctions between selection and influence processes underlying peer use (Snijders and Baerveldt 2003; Steglich, Snijders, and Pearson 2010), questions about multiple or competing mechanisms of action have received less attention. As Warr (2002:44) noted, “it may be true, for example, that having delinquent friends is a strong predictor of delinquent conduct, but that is a little like saying that hanging about the swamps increases the chances of contracting malaria. It may be an accurate statement, but it is not particularly informative.” Associations between individual behaviors and peers remain understudied with regard to the mechanisms by which these influences occur, particularly given the possibility of several influences operating simultaneously. Next, we describe several possible mechanisms through which peer effects may operate.
Peer Networks of Acquisition
Becker (1955) was among the first scholars to argue the importance of drug supply through peers. Starting from the premise that the illegal status of marijuana consumption restricts distribution, Becker emphasized the need to participate in a drug-using social group to gain access for initial use and for the user to increase participation with that group to continue use. During this stage, drug use is dependent on accessibility and availability. As individuals progress toward regular use, they seek access to their own supply. This is accomplished through the peer network, which, reliant on relationships of trust, introduces the user to dealers and connections otherwise inaccessible. Indeed, great support exists in the literature for friends acting as “middle men” or “brokers” in drug transactions (Belackova and Vaccaro 2013; Parker 2000). On the other hand, Becker omitted in his discussion that friends continue to share with each other and also exchange drugs freely within their social networks.
Peer networks are a common means for the circulation of substances among young people. Friendships come with expectations of sharing and reciprocation, and exchanges of substances are fairly common within drug-using peer groups, especially for marijuana, tobacco, and alcohol (Belackova and Vaccaro 2013; Pettigrew et al. 2012). For example, cannabis users commonly report sharing with others, primarily with friends of close age, as well as making regular shared purchases (Coomber and Turnbull 2007). Friendship networks also act as valuable circles of distribution and insulate individuals from the risks of illicit drug markets (Belackova and Vaccaro 2013; Riley and Hayward 2004). Further, sellers commonly cite selling drugs to friends and acquaintances to fund their own supply (Sales and Murphy 2007; Taylor and Potter 2013). Some suggest that these transactions are based on friendship and trust, claiming to exclusively sell to friends, acquaintances, and friends of friends (Taylor and Potter 2013). Unmistakably then, peer groups play a great—and perhaps understated—role in drug availability and accessibility, which has clear implications for patterns of individual use.
Peer Drug Associations
Considerations of how young people perceive social benefits and costs within their peer networks has been an important component of studies of substance use dating back to Sutherland’s (1939) seminal work on how definitions of deviance within peer groups shape individual deviant behaviors. Young people may perceive both positive and negative norms toward drug use within their peer networks, and these normative perceptions—and misperceptions—shape the perceived social benefits and costs of drug use. Peer drug associations account for these social costs and benefits as perceived by the individual, which in turn may affect the practices of substance use by the individual. Essentially a measure of perceived group-level normative context of substance use, peer drug associations have explained individual use in past studies (Oetting and Beauvais 1987).
Perceptions of peer norms are a context for personal use, both for onset and continuation (D’Amico and McCarthy 2006; Kawaguchi 2002). Scholars have identified the important role of discrepancies between perceived peer deviance and actual patterns of deviance (Boman et al. 2014; Young et al. 2011). Perceptions of friends’ substance use have proven better predictors of substance use than friends’ actual use (Iannotti and Bush 1992). Additionally, integration into a group with strong consensus on drug norms directs members to duplicate peers’ behaviors such that group homophily has a reinforcing influence on the behaviors of individuals (Haynie 2002). Theories of collective behavior also imply that the presence of others provides the inspiration or means to attract individuals into risky or illegal activities (Warr 2002).
Perceptions of peers’ practices may also play a role in the experience of normalization of use within the peer group and wider social networks (Parker, Aldridge, and Measham 1998). In other words, the ways in which young people perceive their peers’ practices and attitudes toward use may lead them to perceive the use of a substance as normal and unremarkable. Accounting for how young people perceive the normative contexts within their peer groups thus remains a key element of assessing peer effects and deviance.
Peer Pressure
Peer pressure has long been theorized, both academically and popularly, as a central influence of deviance; namely, that young people experience pressure from friends or others to engage in that behavior. The implication is that peer processes expose individuals at vulnerable life stages to pressures from their peer networks to engage in deviant acts. This is often framed around potential pressures of fitting in with the group or engaging in behaviors expressly desired by the group. In such a manner, peer pressure has received considerable attention with respect to substance use among adolescents and young adults.
Friendships come with rewards and sanctions, which may influence substance use. For example, alcohol use has been tied to popularity aspirations and often balances in favor of excessive drinking (Yanovitzky, Stewart, and Lederman 2006). Sanctions could also take the form of ridicule, with the fear of rejection or humiliation being an important mechanism of control that a dominant group can exert on members or aspiring members (Dijkstra et al. 2010; Warr 2002). Not conforming to group pressures also may be perceived as a threat to loyalty and status as individuals feel they must conform to the practices of the group to prove their devotion as well as form strong bonds with other members (Dijkstra et al. 2010; Warr 2002). The expression of loyalty through conformity allows youth to solidify relationships but may lead to illegal or harmful activities. Individuals with high need for social approval have increased vulnerability to emulating peers’ directional changes in substance use (Caudill and Kong 2001; Urberg et al. 2003) and are socially rewarded for conforming to peers’ substance use, particularly for males (Balsa et al. 2011).
A simple desire by adolescents and young adults to be popular is not, however, the biggest risk factor for substance use; rather, studies have indicated peer pressure and conformity with peers are greater risk factors than popularity, generalized conformity, or dysphoria (Santor, Messervey, and Kusumakar 2000). Conformity with peers was found to occur more strongly in cases of high peer acceptance and high friendship quality (Urberg et al. 2003), suggesting again that strong peer bonds make individuals susceptible to conform to their peer group’s non-normative behavior. These peer pressures may be amplified by the fact that youth “feel most happy, alert, and intrinsically motivated” in the company of their peers (Csikszentmihalyi and Larson 1984:75). Forms of social pressure from peers may thus influence patterns of deviance not only in the initiation of deviant behavior but in continuing or escalating existing patterns of deviance as well.
Pursuit of Pleasant Times with Others
The pursuit of pleasant times with others is the final type of peer influence that we examine. The experience of good times together is a major reason why individuals become and remain friends, and substance use may play a role in such experiences (Niland et al. 2013). As young people engage in social activities together, more subtle forms of social influence may operate toward regular misuse and escalation of misuse. As such, the importance of individuals’ desires to participate with peers in social situations may be conducive to deviance, particularly substance use. Studies have shown that collective recreational drug use events can facilitate social bonding within peer networks (Sheehan and Ridge 2001). More specifically, research has identified that drug use aids in the generation and maintenance of solidarity among members of a group (Kavanaugh and Anderson 2008). Several studies also provide evidence that friends who use drugs together have more intimate friendships (Kandel and Davies 1991; Zimmerman and Wieder 1977) and that they tend to be “sticky friends” (Warr 1993).
The act of drug use within the peer context may be a means of achieving pleasant times with others beyond the pharmacological effects of the substance. Individuals often perceive deviance, such as drug use, as a “sneaky thrill” (Katz 1988), a practice that is desirable primarily due to its action, not its result. Groups of users are accomplices to creating and recreating a shared ritual, which can strengthen social bonds; it involves keeping a collective secret and maintaining appearances. It may even elicit a euphoric feeling not just from the drug itself but also from getting away with performing deviance within the group context (Katz 1988). Thus, the motivation to use substances within these peer contexts of socializing may reinforce substance use by individuals within the peer network.
The Case of Prescription Drug Misuse
The misuse of prescription drugs such as painkillers, sedatives, and stimulants has been documented as a significant problem, especially among young adults. The National Survey on Drug Use and Health revealed that prescription drug misuse continues to be second only to marijuana use among the 18 to 25 age group (Substance Abuse and Mental Health Services Administration 2014). Patterns of prescription drug misuse among young people have been quite varied. While swallowing pills was the most common method among college students, alternative administration, such as intranasal misuse, was reported by a significant minority (Garnier-Dykstra et al. 2012). Moreover, prescription drug misuse has been associated with a number of harmful health outcomes as well as increased use of other substances, including tobacco, marijuana, and other illicit drugs use, and binge drinking (Boyd, McCabe, and Teter 2006; Catalano et al. 2011; Garnier-Dykstra et al. 2012), which exacerbates consequences. While prescription drugs have an array of negative outcomes, they are considered by young people to be less harmful and less stigmatizing than illicit drugs (Quintero, Peterson, and Young 2006).
Given the relative recency of the trend, peer effects on prescription drug misuse have been less well studied than other substances. Studies have identified that adolescents who have peers who misuse prescription drugs are more likely to misuse prescription drugs themselves (Ford 2008). Other research has identified the importance of peers in shaping prescription drug misuse through social learning processes but indicated that social learning may be less influential than for illicit drug use (Schroeder and Ford 2012). Peers may be more weakly associated because favorable definitions of prescription drugs circulate widely due to their legitimate medical uses, and thus peers’ use may not be as important for the internalization of positive definitions of prescription drug misuse. Nonetheless, it remains important to consider multiple ways that peers may shape patterns of prescription drug misuse, particularly with respect to escalating drug practices and symptoms of dependence.
Sources for prescription drugs acquisition have been extremely varied, from doctors and pharmacists to dealers (Inciardi et al. 2007), although the evidence points toward friends serving as important points of access to prescription drugs. The most common suppliers of prescription drugs for misuse are within the peer network (Boyd et al. 2006; Garnier-Dykstra et al. 2012; McCabe and Boyd 2005; McCabe, Boyd, and Young 2007). Beyond providing a source of access, peer acquisition networks may enable normalization and encourage curious individuals to take advantage of the availability through peers (Parker 2005). This may occur especially in a context where suppliers are selling the drugs as a favor, not as a means to obtain profit (Parker, Aldridge, and Egginton 2001). One of the manifestations of normalization of this drug trend is the ease with which drugs are obtained for free from friends (Garnier-Dykstra et al. 2012). One study shows that almost half of active users obtained their drugs not by purchasing them but through peer network sharing (Hurwitz 2005). As with other forms of deviance, research on the phenomenon of prescription drug misuse demonstrates that peers play a role. Thus, given its prevalence among young people, we utilize prescription drug misuse as a vehicle to further understand the mechanisms through which peer effects operate.
Methods
Our data set contains multimethod study assessments with 404 prescription drug misusers who were involved in nightlife scenes. The data were collected between 2011 and 2013. As young adults active in nightlife scenes are a venue-based population, we used venues as our basic unit of sampling to systematically generate a sample of nightlife-involved young adults. Time-space sampling (Stueve et al. 2001) was used in eight different nightlife scenes in New York to recruit participants. Time-space sampling has proven useful to recruit venue-based samples in studies via the randomization of the venues attended and the days/times attended (Parsons, Grov, and Kelly 2008). Through extensive social mapping fieldwork, the research team generated a list of venues across a range of nightlife scenes: indie rock clubs, gay clubs, lesbian party scenes, electronic dance music scenes, jam band shows, college bars, hip hop clubs, and alternative scenes such as warehouse parties. We documented days and hours of operation for venues and assigned all venues an individual number for each viable day. From this enumerated list of venues, we sampled venues and shift day/times using a random digit generator, which produced a series of numbers corresponding to venues on days of the week throughout the month. This random digit process generated the recruitment schedule.
At each venue, project staff attempted to screen as many individuals as possible, aiming to survey all young adults at the venue. Staff approached a patron, identified themselves, described the screening survey, and requested verbal consent for participation in the anonymous brief survey conducted on an iPod Touch designed using iFormBuilder software. For those who provided consent, trained staff administered the beginning of the brief survey (age and NYC residency), and respondents self-reported other information (race, sexual orientation, gender, and substance use) directly onto the iPod Touch. Individuals received no compensation for completing the screening survey. Field staff members were trained not to administer surveys to individuals who were visibly impaired by intoxication. Response rates to the screening survey (75.0 percent) were relatively high given the difficult conditions of surveying young adults in dimly lit, loud nightclub settings and the lack of compensation for participating.
Upon completion of the survey, the software determined whether the individual was eligible for the study (9.4 percent of those screened met eligibility criteria). If eligible, they were provided a brief description of the study and asked to provide contact information if they were interested in participating. A majority of those eligible (77.4 percent) provided contact information for further study participation.
Venue recruitment was supplemented by scene-targeted recruitment via online groups associated with nightlife scenes of interest to reach those who go out less frequently. The research team developed a list of online groups relevant to nightlife scenes of interest. Group members between the ages of 18 and 29 who resided in the NYC metropolitan area saw an advertisement for the study; if they clicked on the ad, they were directed to a Qualtrics survey that screened for study eligibility and, if eligible, collected contact information. A small proportion (<15 percent) of the sample was recruited via this supplemental method. 1
Research staff contacted all eligible participants by phone to provide more information about the study, confirm eligibility, and schedule the initial assessment. Eligibility criteria were as follows: (1) age 18 to 29, (2) reported misuse of prescription drugs at least three times during the past six months, and (3) reported misuse during the past three months. The subjects could report misuse of any of three prescription drug classes—pain killers, sedatives, and stimulants—and many reported the misuse of multiple classes. A threshold of three recent occasions of misuse excluded individuals who simply experimented with a single occasion of misuse while also avoiding enrolling only heavy users. Once participants completed the assessment, including the informed consent process, they were compensated $50. All procedures received Institutional Review Board approval.
We recognize that our sampling method, although allowing us to examine an understudied and rarer phenomenon of a hard to reach population, only permits us to generalize to socially active young prescription drug users. As we argue previously, however, the role of peer influence in the continuation of deviance is understudied, such that we view our methods as advantageous in that a sample of the general population would yield too few active misusers of prescription drugs to assess these outcomes. As shown in the following, both quantitatively and qualitatively, these peer processes still play a role in distinguishing these patterns in continuation. Thus, our sample permits us to test theory while being careful not to generalize the findings beyond this drug using population. We return to this point in the discussion.
Measures
Within the survey, we provided the following operational definition of misuse to subjects: “using prescription drugs obtained from a non-medical source, using more than the prescribed dose, or using prescription drugs for a non-medical or recreational purpose.” We modeled three dependent variables. The first outcome is the number of prescription drug misuse instances during the previous 90 days, ranging from 1 to 340 total instances and skewed to the right (mean = 37.8, SD = 47.8). All drug use behaviors were assessed using a 90-day recall period as a three-month recall period has been shown to produce reliable data (Napper et al. 2010). Second, we measured escalating patterns of misuse by assessing the misuse of prescription drugs through modes of non-oral administration (i.e., sniffing, smoking, or injecting). Finally, we examine symptoms of prescription drug dependence. Via a measure adapted from the Composite International Diagnostic Interview (CIDI) Substance Abuse Module (Cottler and Keating 1990; Cottler, Robins, and Helzer 1989), seven items assessed symptoms of dependence such as tolerance, urges, and increasing use. The measure was tailored to assess the misuse of prescription drugs, and we utilized a cut-off score of 3 or greater to identify youth displaying symptoms of dependence on prescription drugs.
We utilized several measures of peer effects to address the four factors discussed previously. We used two measures for network-based access to prescription drugs. We assessed the total number of sources subjects indicated that they could use to acquire prescription drugs (Inciardi et al. 2007). Moreover, since the majority of prescription drugs misused by young adults come from peer sources (McCabe and Boyd 2005), we also assessed whether or not individuals specifically received prescription drugs from friends (yes/no). Peer drug associations emphasize the importance of the social benefits and costs to drug use that influence individuals’ use (Oetting and Beauvais 1987). Sixteen items from the Peer Drug Associations (PDA) scale 2 assessed perceptions of the peer normative context of prescription drug misuse and its influence, with a Cronbach’s alpha of .726, indicating good internal reliability. Finally, we selected two subscales from the Inventory of Drug Taking Situations (IDTS) to assess peer pressure and use within social peer contexts. The IDTS was designed to gauge the situational antecedents of drug use and has been widely utilized in studies of drug use (Turner, Annis, and Sklar 1997). We used the social pressure subscale and the pleasant times with others subscale; the subscales each had five items, and their Cronbach’s alphas were .833 and .872, respectively.
We include numerous personal characteristics as covariates. Participants self-reported all demographic information in the survey portion of their assessment. Specifically, they reported age, gender, sexual identity, race/ethnicity, and highest education completed. We included measures of total illicit drug use 3 and alcohol use during the past 90 days since previous studies found a strong association between prescription drug misuse and illicit drug use (Catalano et al. 2011; Ford 2008; Ford and McCutcheon 2012; McCabe and Boyd 2005; McCabe et al. 2007) as well as other risky behaviors (McCabe 2005). Descriptive statistics for all variables are available in Appendix Table A1.
Statistical Analyses
The statistical analysis performed on frequency of misuse was a zero-truncated negative binomial regression due to the nature of the data—count variable, with overdispersed values, with zero not being an acceptable value. The other two dichotomous outcomes, meeting prescription drug dependence criteria and having used alternative route of administration during the past 90 days, were analyzed through a series of logistic regressions. Full models with all variables for all outcomes are available in Appendix Tables A2–A4.
Qualitative Interviews
The 70 qualitative interviews analyzed for this article were drawn from 214 qualitative interviews conducted among the 404 young adults in this project. Given that 214 interviews well exceeds a viable sample size for qualitative analysis (Guest, Bunce, and Johnson 2006; Small 2009), we drew a random subset to provide a sufficient yet manageable sample size (n = 70) for the analyses within this article. Our qualitative analytic sample consists of 14 gay/bisexual men, 19 lesbian/bisexual women, 20 heterosexual women, and 17 heterosexual men. Mirroring the survey cohort, 67 percent of the qualitative sample was white, and the median age was 25.
The semi-structured interview utilized critical incident measures to draw out specific event narratives about participants’ prescription drug misuse practices. Critical incident measures reduce recall bias and provide context for behaviors rooted within specific events (Leonard and Ross 1997). Centering on patterns and trajectories of prescription drug misuse among young adults and the role that social contexts play, the interview guide tapped into several relevant issues: social norms and subcultural contexts of misuse, assessment of risk perceptions of prescription drugs in relation to each other and other substances, and the experiences of initial misuse and most recent misuse of each prescription drug class and their social contexts.
We analyzed the qualitative data through an iterative process. Interviews were coded initially using a combination of inductive and deductive perspectives (Strauss and Corbin 1998). We approached the data through a process of multiple readings, coding, and assessing emerging concepts and themes relevant for peer-related mechanisms (Rubin and Rubin 2005). Inductively, the multiple readings of the data allowed for the discovery of any emerging themes to permit contrasting experiences to the peer mechanisms identified. Yet, as argued by Strauss (1987), we also applied deductive approach, making theoretically sensitive coding an important component, keeping in view the results of our quantitative analysis (Strauss and Corbin 1998). A specific goal was to identify the ways in which the mechanisms analyzed within the quantitative analysis resonated within the experiences of young people. In this respect, we evaluated the ways in which young adults described the peer dynamics of their social networks and how these related to prescription drug misuse. As such, the coded themes were discussed and evaluated in light of the literature on peer influences.
The theoretical considerations specified in the peer processes outlined within the introduction were considered and specifically coded for during the data analysis process. Subsequent application of codes in consideration of these theoretical frameworks ultimately cohered with that of a thematic analysis, a qualitative analytic technique utilized to identify and analyze patterns in the description of particular a phenomenon. Our approach cohered with standard qualitative analytic techniques that enable the distillation of wider common themes on peer influence from the narratives provided while leaving outlying individual assertions aside. Consequently, the reported results reflect the themes endorsed by multiple respondents and are exemplified with direct quotes from interviews. Qualitative analyses were performed with the use of NVIVO.
Results
Quantitative Findings
Table 1 provides concise findings for each of the factors individually (labeled single peer effect) as well as the full model inclusive of all peer factors simultaneously (labeled all peer effects). Columns 1 and 2 present the models assessing the number of instances of prescription drug misuse in the past 90 days. The number of drug sources was a significant predictor for prescription drug misuse, initially showing that for every additional source of drugs, the frequency increases by 23 percent (p < .001); it remains significant in the final model, predicting an increase of 16 percent in frequency for every additional source (p < .001). Interestingly, having gotten drugs from friends is not a significant predictor for the frequency of misuse outcome, a point to which we return in the discussion. Peer drug associations are also a consistent predictor, initially increasing the frequency of prescription drug misuse by 4 percent with each unit increase on the PDA scale (p < .001) and by 2 percent in the final model (p < .05). Whereas social pressure was initially significant when alone, it reduces to nonsignificance in the final model containing other peer factors. By contrast, greater desire to have a pleasant time with others increases the number of instances of prescription drug use; for every unit increase on this scale, frequency increases by 9 percent (p < .001). The findings of these models suggest the importance of social networks for acquisition, group normative context, and social reinforcement of drug use in the frequency of personal use. Noteworthy, however, is that social pressure does not impact frequency of use once accounting for other peer effects.
Regressions Predicting Prescription Drug Outcomes with Peer Effects.

Note: Exponentiated coefficients are displayed. Frequency of prescription drug misuse is fit with a truncated negative binomial model, with incident rate ratios displayed. The other two outcomes are fit with a logistic regression model, with odds ratios displayed. The first column for each outcome includes only one theoretical peer mechanism (“Got Rx from friends” and “Number of Rx sources” are included in one model because they both test network access, while all others are the sole peer predictor). The second column reflects a model with all peer predictors. All models include the controls described in the text, and the negative binomial regression contains a dispersion parameter. Full models are available in the Appendix.
p < .05. **p < .01. ***p < .001.
Columns 3 and 4 present models for the alternative administration of prescription drugs. The number of sources is significant in both the single peer effect and the final models. In the final model, for every additional prescription drugs source, the odds of having non-orally consumed prescription drugs increases by 29 percent (p < .05). We find that individuals scoring one unit higher on the peer drug associations scale experience an increase in the odds of alternative administration, which maintains significance in the final model, an increase of 5 percent (p < .05) after the inclusion of all peer factors. For the misuse of prescription drugs to have a pleasant time with others, for every one unit increase, the odds of the outcome increase by 8 percent, net of the other variables (p < .05). Similar to the first outcome, although initially significant on its own, social pressure is not a significant predictor when considered with other peer factors. Similar to previous discussion, we deduce that peers manifest their influence on the individual’s escalated misuse through sources of acquisition, a perceived peer normative context that favors misuse, and a motivation to misuse prescription drugs to enjoy times with peers, but the peer influence on escalation is not attributable to social pressure within a wider peer context.
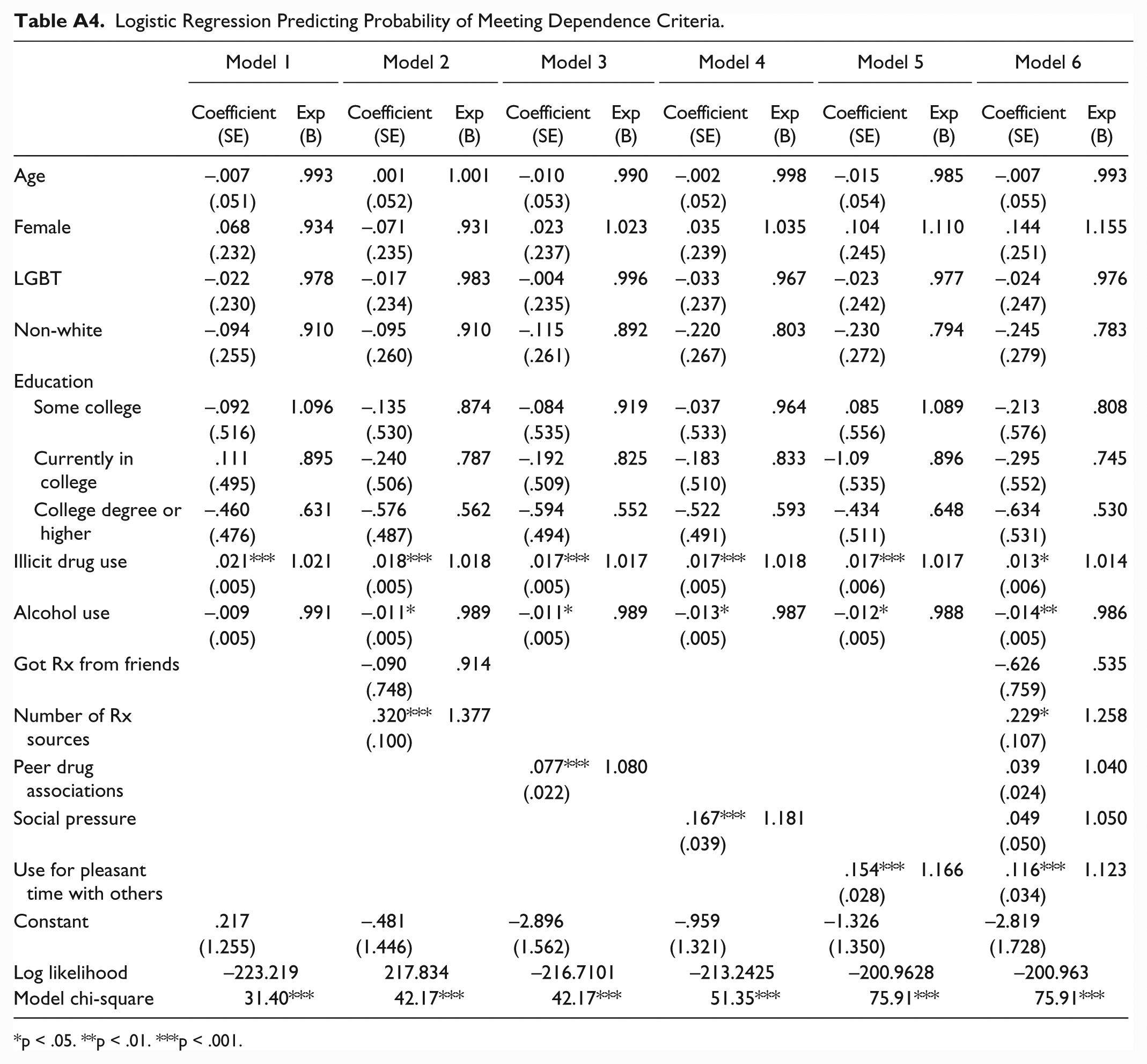
We analyze dependence symptoms as the outcome in Columns 5 and 6. Again, there is a significant effect of sources of acquisition; each additional source increases the odds of symptoms of dependence by 26 percent in the final model. Peer drug associations initially demonstrate a significant association with the outcome; for a one unit increase in the scale, the odds of dependence on prescription drugs increase by 8 percent (p < .01); however, this mechanism’s effect is reduced to nonsignificance in the final model. Misusing prescription drugs for pleasant times with others increases the odds of dependence symptoms by 12 percent for each unit increase on the scale (p < .001) in the final model. Social pressure continues to be nonsignificant in predicting this outcome when other sources of peer influence are included. This last model suggests that the connection between peers and emerging symptoms of dependence is not due to social pressure, but sources of acquisition and use to have good times with peers remain important.
Qualitative Findings
We elucidate the survey results with qualitative interview data from prescription drug misusers. These interviews provide nuanced support for the main components of the statistical analysis: peer network drug acquisition, normative context, and pleasant times with others as influencing misuse, with less support for peer pressure.
Peer sources of acquisition
Relative to dealers and family members, the prevalence of peers as sources for prescription drugs acquisition stands out in interviews. The ways in which these groups provide prescription drugs, however, are diverse. First, peer drug acquisition often involved getting drugs for free as close friends are willing to share their own supply. As Julia (23) described, “like, literally having someone go, ‘do you want a Vicodin?’ is not that uncommon.” Prescription drugs for free, as a minor favor, or even as a gift from a friend emerged as a widespread practice: I feel like it’s really weird to keep saying that they’re easy to get, but they’re so easy to get. And, I feel that when you’re buying illegal drugs, you have to text this weird guy. And then get in his car. And it’s, like, stressful. People are weird about it and it’s unreliable. But . . . everyone has a friend who has good health insurance and gets their pills for free or whatever, and will trade you for a drink, or like, you’ll get them back or something. It’s just really easy. (Julia) These couple of new friends that I recently met have them at all times. Like, all the time within their immediate close group of friends. And they just have them, and they just do them all the time. I’m not even sure of how many they do, but on any given night, if I’m hanging out with them for four or five hours, they’re taking maybe three to four pills each, so it’s just kind of having them there. And they’re just giving them away. They’re not asking for any money. I’m not asking them for them, but they’re giving them to me, so I’m just kind of, like, taking them and hanging out. I’ve had a couple nights hanging out with these specific people and just combining it with drinking. (Nathan, 27 years old)
Additionally, beyond sharing or giving prescription drugs for free, friends acted either as dealers themselves (in the sense that there is an exchange) as well as liaisons to other friends within the wider network who are experienced in drug diversion. The descriptions of these diverse options provide support for our finding that users often have multiple prescription drug sources. Although often receiving drugs directly from friends, interviewees also described processes of buying drugs through friends of friends: This particular guy, it’s my boyfriend’s friend. He, I believe, has a prescription. But we buy so much, it wouldn’t fill one prescription. So I don’t really know. I’m not sure if he has multiple doctors. Whatever, but my friend will, you know, take the order, make the call. For Xanax, that one guy who I’ve never met. Had to go through my friend to get, that’s the only person I know to find them. (Emma, 24 years old) She’s like a friend of a friend. This is how I’ve gotten Adderall in the past. Basically, since I’ve moved to New York, there was some party at which she announced that if anyone wanted to buy some, she had some. ’Cause she has her own prescription, but she’s prescribed way more than she takes, and she sells the rest for extra money. (Jenny, 26 years old)
Overall, peers provide critical points of access to prescription drugs both via the widespread sharing of prescription drugs occurring within peer networks and connecting friends to individuals for purchases.
Peer normative context
Many participants discussed the extent to which prescription drug misuse was normative in their peer networks. Typical remarks highlighted ubiquitous use in their networks, putting an emphasis on the role of the collective character of consumption within their peer groups: “Adderall is just so available, I have so many friends who are prescribed it, so people just, when they’re stressed out they just, that’s what they turn to . . . I think college students especially. I think that’s pretty common now” (Carrie, 20 years old). The group commonly creates a context and opportunity to misuse prescription drugs:
It’s generally something that happens within the night. It’s not something that I say, “We’re gonna go out and we’re gonna do Adderall tonight.”
Gotcha, it’s just sort of something that just pops up?
Right, and I know a few people that are sort of around most of the time who have them pretty frequently. (Daniel, 21 years old)
Not only are group norms favorable toward misuse, but the practice is commonly executed within the peer group and becomes routine. Participants mentioned approaching peer group members for information and advice related to prescription drugs, who often help them without hesitation and give them tips. “When I don’t know about it, I go to her and she knows when it’s something I just shouldn’t do, and she can tell me what it’s supposed to look like, and she can tell me how much to take, and what to make sure I have” (Jake, 20 years old). Moreover, groups sometimes served as an opportune environment to experiment with methods of administration: “I was with a friend. We were in his bedroom, and I was like, ‘I heard it’s even better if you sniff them.’ So we were like, ‘Alright, let’s do it!’ So we crushed it out . . . we had no idea what we were doing” (Ben, 26 years old).
We generally found that peers are tolerant of recreational misuse even when they do not use drugs and even create a favorable normative context and encourage positive peer drug associations: I have a really diverse group of friends. They’re kind of all over the map. It’s like there’s some that just don’t do it, that would never do it. Then there’s some that do. For the most part, though, it’s a general relaxed attitude towards just recreational. I don’t really have drug people—I don’t have friends who do drugs like every day. That’s just not a part of my life. But in terms of like recreational using, I think they’re totally okay with it. Most of them recreationally use. I think. I’m the one like, “Oh, you want to take this Vicodin?” and “Oh yeah, sure.” They don’t ever seek it out, though. I have like, two friends that have their own prescriptions to things, and that’s it. You know? Everyone else is kind of like, “Oh, you have one? Okay, sure, I’ll take it.” But . . . otherwise it’s, like, not a big deal. (Ed, 24 years old)
Peer pressure
Social pressure among peers was complicated in participant narratives. Many youth stated that they did not experience explicit social pressure to misuse yet acknowledged that their friends subtly encouraged use in certain circumstances. Young adults described peer pressure as relatively rare and perceived it as inconsequential when it occurred. As Zack described, I usually think the peer pressure thing is bullshit. Like, these imaginary people, who are walking around, that want you to do their drugs. However, this is a rare occurrence where these people were walking around and they wanted me to do their drugs, and they gave them to me, so I took them. That usually isn’t my persona, but it was my best friend. So I was like, “Oh alright, I’ll take this.” (Zack, 27 years old)
Yet others specifically described feeling not pressured but enabled to misuse because the drugs were consistently available and attainable through romantic partners or friends: Most of my friends have Adderall or some kind of Adderall-like prescription because they have health insurance and all these pills. Like, one of my roommates, she’s pretty much a pharmacy—she has sleeping pills, Xanax, Adderall, Klonopin, . . . everything imaginable. And so, when we go out, if I don’t have coke, I’ll take some Adderall. My friends will do whatever is available with me. But, the situation never was like, “Do you ever feel pressured to take it?” or anything. But it’s always, people give them out like candy in my social group. Like, if I want to take some—”Do you want some? ’Cause that would be—I’m willing to share, like, for free.” It’s not something really attached to, I don’t know, some kind of monetary thing. It’s not a commodity. It’s just like, you know, if you have an extra pizza, you’d give to someone else. (Helen, 22 years old)
On rare occasions when having experienced peer pressure, respondents described primarily their initiation experiences instead of situations in which they continued or escalated use. The initiation experiences, typically occurring at a younger age, were situations they did not expect, and although they did not plan on taking prescription drugs, everyone else was doing it, so they felt compelled by the social circumstances rather than explicit pressure: Beforehand, I was actually kind of nervous to take it, but taking it, it was pretty mild for all of us involved. That was probably one of those situations where I felt socially pressured to do so. Even though it was my best friends and I could have pretty easily said no, it was everybody else was kinda doing it and having fun, so I did it too. (Sophie, 22 years old)
Others often expressed not perceiving groups of friends trying to pressure others to misuse prescription drug, but the social context was one that suggested use was acceptable and enabled, which speaks back to the peer drug associations.
Pursuit of good times with friends
Individuals commonly expressed inclinations to use prescription drugs to have a more interesting, pleasing, or relaxing time. Such interviews supported survey findings that individuals take pills to increase enjoyment during social occasions, whether it is just to “hang out” or go out at a bar, club, or party: You just laugh, like everything is goofy. It usually starts that she picks me up, then we go to her place. We are hanging out in the apartment, maybe we have a snack, I don’t know, we’re just shooting the shit. And then she gives me a Lorry [Lorazepam]. We call it Lorry . . . then we roll a spliff and we walk to the park to smoke. And by the time we are done with the spliff, we walk back to her apartment. We just laugh the whole way. It’s a good time, but, I mean, but that’s all it is. I mean, and it doesn’t last that long. I don’t even know what’s that for. It must be for anxiety, which, I mean, it helps. Like, it’s just you don’t care. (Jake, 20)
What makes a good night was said to be “hanging out with a group of friends, you know, whether it’s a small group or a large group, and just shooting the shit, telling stories and laughing” (Tessa, 21 years old). Such descriptions illustrate why party contexts were often particularly appropriate settings for collective alcohol and drug use and distribution of pills: If I decide to pop Xanax when I’m drinking, it’s usually because I’m in a group of friends and we’re all just having this awesome time, and I just kind of want to push it to that next level of all being happy, and we all end up just popping them. (Anne, 25 years old)
Discussion
As the literature on peer effects has accumulated considerable strength in examining substance use, the case of prescription drug misuse comes as an opportunity to apply the acquired body of knowledge to this emerging drug trend and through it, further explanations of the role of peers in deviance. The association of peers’ deviance with individual deviance, especially in the case of substance use, is one of the most robust findings in sociology. Yet, classic theories such as those by Sutherland, Becker, and Akers describe a more complex process than simply imitation; rather, peer influences are multifaceted and, as we contend, intertwined. As opposed to merely measuring peer use, we argue that various mechanisms of action by which peers shape individual drug use must be studied together to provide a comprehensive assessment of the role of peers. Through the examination of four distinct mechanisms, this article provides an opportunity to extend previous literature by considering multiple dimensions of peer effects. It also allows us to consider the continuing role peers play in deviance beyond considerations of whether or not individuals engage in a behavior.
Overall, this article identifies several dimensions of peer effects on prescription drug misuse among regular misusers—via the frequency of misuse, the odds of non-orally administering the medication, and odds of reporting symptoms of dependence. The individual peer models suggest that each peer factor is important. However, within the full model, we identified that network accessibility, perceived peer normative context, and motivation to misuse drugs to have a pleasant time with peers each played some role in shaping patterns of prescription drug misuse while peer pressure did not. Moreover, the findings deepen our understanding of the processes underlying these behaviors because even though we know peers are a great influence of behavior, identifying the mechanisms behind their influence still represents a challenge (Warr 2002). The qualitative findings not only illustrate these processes but also highlight the manner in which these peer processes are intertwined.
Reminiscent of Becker’s (1955, 1963) early work on access to marijuana, the number of network sources individuals used to obtain prescription drugs is a significant factor in all three outcomes, confirming the importance of peer networks in the continuation of drug practices. The interviews reinforced the existence of a network in which peers have extensive access to prescription drugs and diversion is normalized and unproblematic among them. These findings highlight the central role of peers in prescription drug access, whether through monetary or bartered transaction or extensive sharing within peer networks (Garnier-Dykstra et al. 2012; Hurwitz 2005). The data, however, showed that whether a person has gotten prescription drugs from friends is not a significant predictor of misuse, potentially because the sheer ubiquity of this response (97.4 percent) leads to little variability, which is perhaps less surprising among a sample of active misusers. Although we cannot assess this predictor for this reason, the commonplace sharing among friends demonstrates its level of importance for young adults.
Peer drug associations, which account for contexts of peers’ positive and negative reinforcement of drug practices, were associated with the frequency of prescription drug misuse as well as transitions to non-oral routes of administration, such as smoking or sniffing. Peer drug associations serve as a way of measuring not only perceptions of peers’ involvement with the substances but also their active role in conditioning the individual to use drugs or discouraging the individual. The peer network context acts to subtly condition the individual to adhere to peers’ beliefs, attitudes, and norms. Thus, our findings indicate that the perceived benefits and costs of misuse within the peer network shape the frequency of misuse as well as how young people administer drugs. By contrast, symptoms of dependence were not influenced by this peer mechanism. By the time an individual reaches levels of misuse indicative of dependence, the perceived normative context may be less important.
Our results indicate that peer influence does not extend to individuals experiencing direct pressure to misuse. This finding parallels those of Bot and colleagues (2007), who concluded that modeling (measured as the imitation of others’ drinking) is a significant predictor of individual drinking, whereas persuasion (drinking resulting from being offered drinks) is not (also Overbeek et al. 2011). Though significant when considered as the lone source of peer influence, peer pressure was reduced to nonsignificance for all three outcomes once the other sources of peer influence were accounted for. Instead, peers play a role in personal misuse via more subtle forms of encouragement as well as deterrence from discontinuation, but pressure does not affect the outcomes under study. One additional consideration is that peer pressure may play no role in continuing patterns of deviance in the manner it may in decisions to initiate deviance. The qualitative analysis highlighted that participants recalled instances of social pressure during initiation into misuse, albeit rarely, while not doing so or expressing skepticism of its influence for continuing or escalating patterns of misuse. We also note that peer pressure may be a more significant factor for teenagers in comparison to young adults. Important differences exist between these unique stages of the life course, whereby pressure to conform may be more significant for adolescents (Warr 2002).
Rather than peer pressure, the results highlight that misuse is motivated by a desire to enjoy pleasant times with friends. The interviews further support this finding; participants argued the drug properties provide for additional enjoyment in social situations. Katz (1988) identified the experience of group-based pleasure as a key component of deviance and risk taking, and our findings suggest that the group context may amplify the experience of pleasure from deviant acts, leading to higher probabilities on all three outcomes. Overall, the findings strengthen the argument that a key connection between peers and personal use is the desire to have pleasant times with friends in social situations.
In terms of limitations, this study relies on a sample with particular characteristics, which presents some issues of generalizability. First, our sample purposefully examines active prescription drug misusers, and as such, we focused on peer effects in continuing patterns of use, namely, frequency of misuse, escalation, and dependence. While a strength in many respects given the overwhelming focus on initiation or “any use” in the sociological literature, this limitation implies that we cannot generalize to a wider population of young adults. Second, as we sampled from nightlife venues with a time-space sampling method, we may have oversampled people who are more frequent nightlife participants. Though advantageous for accessing a hard to reach population, the nightlife-based sample creates some restrictions in our ability to fully extend our results to other populations and contexts. Third, prescription drugs represent the second most illicitly used category of drugs other than marijuana, demonstrating its importance. Yet, while we believe that our results are likely applicable to other drug types, we cannot be certain that the same results will hold for all illicit substances or teenagers. We encourage future tests of these processes for teenagers, other drugs, and young adults more generally.
Beyond the issue of the sample generalizability, we recognize the potential for issues of self-selection. Network scholars have identified methods for disentangling the processes of influence and selection (Snijders and Baerveldt 2003; Steglich et al. 2010), yet such analytic methods have only been applied to assessments of network properties of whether or not peers use (Knecht et al. 2010; Mencken et al. 2010). Future research could apply such methods to study selection and influence processes related to mechanisms of action such as those examined here. While cognizant of the inability to fully disentangle selection from influence with ego-based survey data, to address possible issues of temporal order, we reran our models using outcomes from the 12-month follow-up survey. We present the baseline cross-sectional models for two reasons. First, we avoid the (~20 percent) attrition that occurred by the 12-month follow-up. Second, we are unable to run the model for non-oral administration from the 12-month follow-up due to perfect prediction for one factor. Specifically, those who did not acquire prescription drugs from friends at baseline did not escalate to non-oral administration at 12 months among subjects followed up. For the other outcomes at the 12-month follow-up, we find nearly identical results for peer-related variables. The lone exception is that the PDA scale in the analogous model with all peer effects for frequency of misuse is only marginally significant (p = .060). Additionally, while these analyses do not eliminate the possibility of selection, several aspects of our research attenuate this concern. First, our goal was to examine competing peer mechanisms, which are still of interest even in the face of self-selection. That is, even if individuals seek out particular peers, we remain interested in the components of that peer relationship associated with continued use, escalating patterns of use, and dependency. Second, the null findings for social pressure and significant findings for a desire to have a pleasant time with others are less likely to be influenced by self-selection. Even if selecting into a peer group on the basis of their favorability to prescription drug use, we do not find that those peer definitions manifest themselves in the form of pressure. Additionally, one’s desire to enhance time spent with friends through substance use is an egocentric measure related to the peer group experience. Lastly, our use of qualitative interviews to identify how young people understand these mechanisms gives further credence to the role that peers play regardless of self-selection. In fact, most of our interviewees reported that misuse and escalation, while supported by peers, is relatively unsystematic, as opposed to a process whereby peers seek each other out expressly for the purpose of prescription drug misuse.
Conclusions
The strength of this article lies in the opportunity to separate multiple strands of peer effects on deviance and clarify distinctions between access, normative context, peer pressure, and desire to have pleasant experiences with others. Additionally, rather than focus on whether these mechanisms shape any use, we provide evidence for the role of peers in continued patterns of deviance. In strong association with the efforts of scholars to connect peers’ deviance to individual deviance, we find that the peer context strongly affects the continuation of deviance, in this case, patterns of prescription drug misuse. The major implications are that the intertwined peer processes must be evaluated holistically to distill out their influence. Additionally, rather than being motivated by friends’ pressure to sustain or increase personal use, individuals are motivated by a broader peer context, especially by a positive normative context, desires to enhance experiences with friends, and network-based accessibility that facilitates misuse.
Footnotes
Appendix
Logistic Regression Predicting Probability of Meeting Dependence Criteria.
| Model 1 |
Model 2 |
Model 3 |
Model 4 |
Model 5 |
Model 6 |
|||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Coefficient (SE) | Exp(B) | Coefficient (SE) | Exp(B) | Coefficient (SE) | Exp(B) | Coefficient (SE) | Exp(B) | Coefficient (SE) | Exp(B) | Coefficient (SE) | Exp(B) | |
| Age | –.007 | .993 | .001 | 1.001 | –.010 | .990 | –.002 | .998 | –.015 | .985 | –.007 | .993 |
| (.051) | (.052) | (.053) | (.052) | (.054) | (.055) | |||||||
| Female | .068 | .934 | –.071 | .931 | .023 | 1.023 | .035 | 1.035 | .104 | 1.110 | .144 | 1.155 |
| (.232) | (.235) | (.237) | (.239) | (.245) | (.251) | |||||||
| LGBT | –.022 | .978 | –.017 | .983 | –.004 | .996 | –.033 | .967 | –.023 | .977 | –.024 | .976 |
| (.230) | (.234) | (.235) | (.237) | (.242) | (.247) | |||||||
| Non-white | –.094 | .910 | –.095 | .910 | –.115 | .892 | –.220 | .803 | –.230 | .794 | –.245 | .783 |
| (.255) | (.260) | (.261) | (.267) | (.272) | (.279) | |||||||
| Education | ||||||||||||
| Some college | –.092 | 1.096 | –.135 | .874 | –.084 | .919 | –.037 | .964 | .085 | 1.089 | –.213 | .808 |
| (.516) | (.530) | (.535) | (.533) | (.556) | (.576) | |||||||
| Currently in college | .111 | .895 | –.240 | .787 | –.192 | .825 | –.183 | .833 | –1.09 | .896 | –.295 | .745 |
| (.495) | (.506) | (.509) | (.510) | (.535) | (.552) | |||||||
| College degree or higher | –.460 | .631 | –.576 | .562 | –.594 | .552 | –.522 | .593 | –.434 | .648 | –.634 | .530 |
| (.476) | (.487) | (.494) | (.491) | (.511) | (.531) | |||||||
| Illicit drug use | .021*** | 1.021 | .018*** | 1.018 | .017*** | 1.017 | .017*** | 1.018 | .017*** | 1.017 | .013* | 1.014 |
| (.005) | (.005) | (.005) | (.005) | (.006) | (.006) | |||||||
| Alcohol use | –.009 | .991 | –.011* | .989 | –.011* | .989 | –.013* | .987 | –.012* | .988 | –.014** | .986 |
| (.005) | (.005) | (.005) | (.005) | (.005) | (.005) | |||||||
| Got Rx from friends | –.090 | .914 | –.626 | .535 | ||||||||
| (.748) | (.759) | |||||||||||
| Number of Rx sources | .320*** | 1.377 | .229* | 1.258 | ||||||||
| (.100) | (.107) | |||||||||||
| Peer drug associations | .077*** | 1.080 | .039 | 1.040 | ||||||||
| (.022) | (.024) | |||||||||||
| Social pressure | .167*** | 1.181 | .049 | 1.050 | ||||||||
| (.039) | (.050) | |||||||||||
| Use for pleasant time with others | .154*** | 1.166 | .116*** | 1.123 | ||||||||
| (.028) | (.034) | |||||||||||
| Constant | .217 | –.481 | –2.896 | –.959 | –1.326 | –2.819 | ||||||
| (1.255) | (1.446) | (1.562) | (1.321) | (1.350) | (1.728) | |||||||
| Log likelihood | –223.219 | 217.834 | –216.7101 | –213.2425 | –200.9628 | –200.963 | ||||||
| Model chi-square | 31.40*** | 42.17*** | 42.17*** | 51.35*** | 75.91*** | 75.91*** | ||||||
p < .05. **p < .01. ***p < .001.
Acknowledgements
The authors acknowledge the contributions of Jeffrey Parsons and members of the project team, especially Brooke Wells, Amy LeClair, and Mark Pawson. The views expressed in this paper do not expressly reflect the views of the National Institute on Drug Abuse or any other governmental agency.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a grant from the National Institute on Drug Abuse (Brian C Kelly, P.I.). Funding Sources National Institute on Drug Abuse, (Grant / Award Number: R01DA025081).
1
Individuals recruited through online groups were more likely to be gay, non-white, and less well educated. There were no significant differences in the frequency of misuse for each of the three prescription types.
2
We removed an item that assessed social pressure to use to avoid overlap with the conceptualization and operationalization of social pressure.
3
The frequency of illicit drug use is a variable formed by adding the number of instances the respondent reported having used the following substances in the past 90 days: MDMA, LSD, methamphetamine, cocaine, crack, heroin, methadone, ketamine, and “other drug.” We excluded marijuana since use was ubiquitous among respondents.