
Abstract
Do public health policy interventions result in prosocial behaviors? The Patient Protection and Affordable Care Act’s Medicaid expansions were responsible for the largest gains in public insurance coverage since its inception in 1965. These gains were concentrated in states that opted to expand Medicaid eligibility, and they provide a unique opportunity to study not just medical but also social consequences of increased public health coverage. The authors examine the association between Medicaid and volunteer work. Volunteerism is implicated in individuals’ health and well-being, yet it is highly correlated with a person’s existing socioeconomic resources. Medicaid expansions improved financial security and a sense of health, two factors that predict volunteer work, for a socioeconomic group that has had low levels of volunteerism. Difference-in-difference analyses of the volunteer supplement of the Current Population Survey (2010–2015) find increased reports of formal volunteering for organizations as well as informal helping behaviors between neighbors for low-income nonelderly adults who would have likely benefited from expansions. Furthermore, increased volunteer work associated with Medicaid was greater among minority groups and narrowed existing ethnic differences in volunteerism in states that expanded Medicaid eligibility.
Keywords
Large-scale reforms to public health insurance coverage can be viewed as policy interventions affecting population health. Past health reforms to Medicaid, the Children’s Health Insurance Plan, and Medicare have had a significant and widespread impact on health behaviors and outcomes (Baicker and Finkelstein 2011; Currie and Gruber 1996; Finkelstein 2007; Sommers and Oellerich 2013). The Oregon Health Insurance Experiment, for example, randomized Medicaid coverage for low-income adults and found evidence of increased health utilization, improved physical and mental health status, and reduced mortality for those participants receiving Medicaid compared with the control group (Baicker et al. 2013; Finkelstein et al. 2012).
Observers expect that the recent Medicaid expansions as part of the Patient Protection and Affordable Care Act (ACA) will have similarly widespread health effects. Among the various provisions of the ACA, states’ Medicaid expansions were the largest drivers of improved insurance coverage between 2013 and 2015. More than 60 percent of insurance coverage gains have been attributed to Medicaid, providing health insurance to about 13 million Americans under age 65 (Frean, Gruber, and Sommers 2016). States opting into the federally funded Medicaid expansion made all individuals with household incomes below 138 percent of the federal poverty level (FPL) eligible for Medicaid coverage regardless of family and pregnancy status, constituting the most comprehensive and far-reaching set of changes to Medicaid since its inception in 1965 (McDonough 2011). The Medicaid expansion has thus rendered an increased population eligible for health insurance, which will likely translate in greater health care utilization (Baicker and Finkelstein 2011) and better health outcomes (Currie and Gruber 1996).
In addition to direct health effects, social scientists are interested in the indirect effects of health care reform (McKay and Timmermans 2017; Stone and Bryant 2012). The Oregon Medicaid experiment shows that Medicaid enrollment not only improved self-reported health and well-being but also stabilized incomes (Baicker and Finkelstein 2011). Greater financial stability and better health may allow individuals to take on more social engagement activities. Volunteering is one critical prosocial activity beneficial not only for communities but also for individuals. Despite concerns raised about a decline in civic engagement (Putnam 2000), Americans lead other countries in volunteer work (Dekker and Halman 2003). Prior studies consistently demonstrate that individuals with greater resources such as income, education, and health are more likely to engage in volunteer work (Wilson and Musick 1997). The benefits of volunteering due to public health insurance, however, may accrue differently for various social groups: in addition to socioeconomic resources, gender, race, and ethnic background are major determinants of volunteerism (Musick and Wilson 2008). An increase in volunteering among groups less likely to volunteer in the past may be socially significant because volunteering may also produce health benefits as well as provide access to social, political, and human capital (Wilson 2000).
Building on this literature, in this article we address the following research questions. First, is increased access to public health insurance through Medicaid expansions as part of the ACA associated with increases in formal volunteering and informal helping? Second, do increased levels of volunteering and helping differ by gender and race? Recent health reforms provide a fortuitous research opportunity to study this relationship. A Supreme Court decision in June 2012 made the ACA’s Medicaid expansion mandate optional for states. Although states did not randomly expand Medicaid, the variation in policy adoption allows a comparison of the effects of Medicaid expansion on volunteering.
We find increased reports of formal volunteering for organizations as well as informal helping behaviors between neighbors for low-income nonelderly adults living in states that decided to expand Medicaid. Medicaid expansion, however, did not close the gender gap in volunteering. Increased volunteer work associated with Medicaid was greater among Latino/as and narrowed ethnic differences in volunteerism in states that expanded Medicaid eligibility.
Health Insurance and Volunteering
To explore how health insurance may indirectly stimulate prosocial behavior such as volunteering, we review research literature indicating that gaining health insurance is associated with improvements in individual health and household financial stabilization. Both of these effects, better health and financial security, have been associated with an increased likelihood in volunteering. Because the Medicaid expansion under the ACA has benefited certain groups more than others, any increases in volunteering among the poor may be moderated by race and gender.
Medicaid is a means-tested government insurance program for families and individuals with limited income and resources to pay for health care. Title II of the ACA sought to bring about the largest reform to the Medicaid program since its inception in 1965 (McDonough 2011). Historically, states had considerable freedom to set their eligibility rules and the benefits that they offered through Medicaid. The ACA’s original design would have made all persons in households earning effectively up to 138 percent of the FPL eligible for Medicaid coverage and set uniform standards on benefits and care across all states (McDonough 2011). However, the July 2012 Supreme Court decision in National Federation of Independent Business v. Sebelius limited the federal government’s ability to enforce state compliance. Greatly influenced by political factors, state economic conditions, administrative capabilities, and prior policies toward low-income residents and the uninsured (Jacobs and Callaghan 2013), 24 states and the District of Columbia opted to expand Medicaid eligibility in January 2014. Michigan and New Hampshire joined soon after in April and August 2014, respectively. Pennsylvania and Indiana decided to expand during the first quarter of 2015, and Alaska, Montana, and Louisiana joined thereafter within another 18 months. This turn of events resulted in an opportunity to compare states that proceeded Medicaid expansions against states that did not.
Generally, Medicaid expansions were deemed responsible for more than 60 percent of health insurance coverage gains in 2014 and led to increased health care utilization and self-reported health (Frean et al. 2016). Several studies have exploited the variation in policy change between states. Using a difference-in-difference approach, researchers have estimated changes in insurance coverage, migration patterns, and health outcomes associated with Medicaid expansions (Courtemanche et al. 2016; Schwartz and Sommers 2014; Sommers et al. 2015). Early studies after the rollout of the ACA in 2014 show that Medicaid expansions was associated with significant reductions in uninsurance between late 2013 (the pre-ACA period) and early 2015, a little more than a year after the ACA went into effect. As expected, the research shows that states with Medicaid expansions to low-income adults were associated with reduced mortality as well as improved coverage, access to care, and self-reported health (Sommers et al. 2015). The research showed that few people migrate from states without to states with Medicaid expansion to obtain Medicaid insurance. Medicaid expansion also reduced uncompensated hospital care in states that opted for expansion compared with nonexpansion states (Dranove, Garthwaite, and Ody 2016). Still, participation of health care providers in Medicaid because of relatively low reimbursement rates and “churning” or eligibility changes that render individuals no longer eligible for Medicaid when their income changes limit the effectiveness of the Medicaid expansion on improving population health indicators (Collins et al. 2015; Polsky et al. 2015).
Beyond health effects, providing health insurance to a previously uninsured population improves the financial stability for those gaining health insurance. One of the major primary economic functions of health insurance is to protect financial assets against expensive medical bills. Research shows that previous expansions of public insurance coverage provided financial benefits to uninsured families and individuals who gain coverage (Wherry, Kenney, and Sommers 2016). For low-income adults, the Oregon Medicaid experiment demonstrated that coverage reduced financial strain on several self-reported measures such as out-of-pocket medical payments, borrowing money or skipping bills to pay for medical expenses, and the incidence of catastrophic expenditures (Baicker et al. 2013; Finkelstein et al. 2012). A quasi-experimental study showed that a 10 percent increase in Medicaid eligibility was associated with an 8 percent decrease in household bankruptcy (Gross and Notowidigdo 2011). The ACA has stabilized the out-of-pocket health expenses of newly covered young adults (Busch, Golberstein, and Meara 2014). Also, the 2014 Commonwealth Fund Biennial Health Insurance Survey found that for the first time since the survey started in 2001, fewer people reported financial barriers to care, and fewer people reported problems paying their medical bills or debts (Collins et al. 2015).
Better health and greater financial security, in turn, may stimulate social behaviors. One such critical prosocial behavior is volunteering, when people give their time freely for the benefit of others. In 2013, 62.8 million Americans (25.3 percent) volunteered more than 7.9 billion hours of service, for a value of $184 billion (Corporation for National and Community Service n.d.). Volunteering encompasses both formal and informal dimensions (Wilson 2000; Wilson and Musick 1997): formally, volunteering includes the unpaid provision of services, political activism, and community representation, while informal volunteering includes helping out in communities and intervening in emergencies. Informal helping is distinct from informal caregiving arrangements, which are associated with time- and resource-intensive obligations rather than an opportunity to do well for oneself and others (Post 2005). We limit our analysis to specific types of formal volunteering and informal helping: participating in volunteer organizations and helping a neighbor to fix or improve things.
Research shows that volunteering is affected by both health and financial factors. In their profile of American volunteers, Musick and Wilson (2008) argued that people require cultural, human, and social resources to engage in volunteer work. “Poor health,” they wrote, “raises the cost of doing volunteer work” (p. 164). Self-rated health is positively related to volunteering (Day and Devlin 1996). A study of elderly Europeans in 10 countries found that those that rated their health as good or better were twice as likely to volunteer as those rating their health as fair or worse (Erlinghagen and Hank 2006). Thoits and Hewitt (2001) also found that people who reported being happier and healthier volunteered more hours and that self-reported mental health and physical problems may be barriers to volunteering.
Volunteering also depends on a range of human capital factors, including financial resources. Volunteer work may impose opportunity costs because it is unpaid work. Especially for people with low income, barriers to volunteering include incidental expenses of volunteering such as transportation, membership dues to volunteering organizations, and even decent clothing (Reitsma-Street, Maczewski, and Neysmith 2000). Wealthier people are also more likely to be a member of volunteering organizations, more likely to be asked to volunteer, and may be more likely to bear the risks and costs of volunteering, suggesting a positive relationship between volunteering and income (Musick and Wilson 2008). The research shows indeed that higher income leads to a higher likelihood of volunteering (Day and Devlin 1996; Menchik and Weisbrod 1987), although higher income does not explain the number of hours volunteered (Woolley 1998).
Differences in socioeconomic resources only partially explain differences in volunteerism between racial and ethnic groups in the United States (Musick and Wilson 2008). Whites tend to volunteer more than African Americans, but racial differences in volunteering decrease after controls for education, income, occupational status, and neighborhood conditions (Clary, Snyder, and Stukas 1996; Cutler and Danigelis 1993; Wuthnow 1998). Racial solidarity and response to the needs of the local community motivate African Americans to engage in formal and informal volunteer work (Latting 1990), although data from a national representative survey show little difference in motivation for volunteering (Clary et al. 1996). Religious organizations serve as foci of formal volunteer work among more African Americans than other ethnic groups (Hall-Russell and Kasberg 1997), and their greater informal social interactions increase opportunities to help within their communities. Still, disparities in socioeconomic resources result in fewer African Americans engaging in volunteer work than whites. Latino/as also face social disadvantage and exclusion similar to that of African Americans. Unfamiliarity with the language, social customs, and civil practices that recent immigrants face may create further barriers for many Latino/as (Musick and Wilson 2008), although few studies examine rates and motivations for volunteer work among Latino/as. How race and ethnicity moderates the relationship between socioeconomic resources and volunteerism is not immediately apparent. On one hand additional resources may make a greater difference to minority groups that had the least to begin with. Yet the impact of these resources may be muted in the presence of structural barriers that cannot be overcome by short-term endowments onto individuals (Rotolo and Wilson 2014).
Volunteer work has also been viewed as an extension of women’s caretaking role (Negrey 1993; Scott 1991), and donating time for the needs of the community was socially acceptable and often desirable for wives of upper- and middle-class men (Stephan 1991). Although increasing female labor force participation in recent decades has made volunteer work less gendered, women are still more likely to volunteer, both formally and informally, than men (Wilson and Musick 1997). Women are still more likely to be the primary caretakers of children whose schools and extracurricular organizations often recruit parents for help. In addition, women are more likely to express prosocial norms that lead to greater volunteerism (Marini et al. 1996). These structural and cultural forces suggest that socioeconomic resources may matter less for women than men when it comes to volunteer work (Musick and Wilson 2008). Some studies show gender as a significant moderator of the relationship between socioeconomic resources and volunteering, whereas others do not find significant effects of gender (Barkan 2004; Schlozman, Burns, and Verba 1994). Taniguchi (2006) found that part-time work encourages women’s volunteer work but not men’s, while unemployment inhibits men’s volunteering. Men may also be more likely to hold the jobs that provide the civic skills on which volunteering depends (Schlozman et al. 1994). Most recently, Musick and Wilson (2008) did not find any interaction effects of gender on the relationship between socioeconomic resources and volunteering.
In sum, state-based Medicaid expansions facilitated by the ACA may have effects on formal volunteering and informal helping by providing to key predictors of increased volunteering: better health and greater financial stability. We would expect that states that expanded Medicaid will show an increase in volunteers, especially among African Americans and Latino/as, who previously faced greater socioeconomic barriers to volunteering. Conversely, we expect gender to have similarly small moderating effects on the association between Medicaid, a socioeconomic resource, and volunteer work. An increase in volunteering among populations less likely to volunteer would be socially significant because volunteering is associated with better physical and mental health, political engagement, and socioeconomic resources (Wilson 2000).
Data and Variables
The analyses use the volunteering supplement to the Current Population Survey (CPS). The CPS is a monthly survey of approximately 60,000 households conducted by the Bureau of Labor Statistics and the Census Bureau. The survey is a probability sample of the civilian, noninstitutionalized population of the United States. The volunteering supplement is conducted once a year in September. The CPS offers several advantages. It is one of the largest probability samples of the United States and has high response rates, and the volunteering supplements have response rates that exceed 80 percent (according to CPS technical documentation) and have been used as benchmarks to evaluate biases in other surveys on volunteerism (Abraham, Helms, and Presser 2009). The CPS also collects consistent economic and sociodemographic information year after year, enabling researchers to study trends over time. Our data spans the period from 2010 to 2015, and our primary analyses are limited to respondents aged 18 to 64.
Formal Volunteering
We measure formal volunteerism in both likelihood of having volunteered for an organization and the total number of hours volunteering for those organizations in the past 12 months. The CPS asks two questions to determine whether a respondent engaged in formal volunteering. The first asks, “Since September 1st of last year, have you done any volunteering activities through or for an organization?” The second asks, “Sometimes people don’t think of activities they do infrequently or activities they do for children’s schools or youth organizations as volunteer activities. Since September 1st of last year, have you done any of these types of volunteer activities?” We consider those who answered “yes” to any of these two questions as having volunteered in the past 12 months.
Informal Helping
In addition to detailed questions on volunteering, the CPS asks, “Since September 1st of last year, have you worked with people in your neighborhood to fix or improve something?” Following Wilson and Musick’s 1997) conceptualization of volunteer work, we consider this variable a form of informal helping.
Analytical Strategy
The main analyses exploit the variation in states’ participation in Medicaid expansions. Twenty-four states and the District of Columbia decided to expand Medicaid in January 2014. Four more joined by 2015. As of the end of our study period, 22 states had not adopted Medicaid expansions. We use a difference-in-difference approach to estimate changes in volunteerism associated with Medicaid expansions. The CPS volunteer supplement was surveyed in September of each year. Therefore, 2014 is considered the first postexpansion period for the first 24 states and the District of Columbia that joined Medicaid and Michigan, which joined in April of that year. The first postexpansion period for New Hampshire, Pennsylvania, and Indiana is 2015, as they adapted Medicaid expansions in August 2014, January 2015, and February 2015, respectively. The remaining three expansion states—Alaska, Montana, and Louisiana—joined after September 2015 and feature in the analyses as nonexpansion states. The analyses compare difference in volunteer work between expansion and nonexpansion states before and after adoption.
Medicaid expansions predominantly affected low-income households. Thus, we expect changes in volunteerism associated with Medicaid to be the greatest among lower income households and the smallest, if any, among higher income households; we focus our analyses on individuals in households in the bottom quartile of the income distribution (determined within each year). The September supplement of the CPS includes a 16-category variable that indicates an individual’s total household income. We use this measure to categorize respondents into income quartiles. Total household income ranged from less than $5,000 a year to $19,999 a year. The second quartile’s income ranges from $20,000 to $49,999 a year. One hundred thirty-eight percent of the FPL for a single-adult household ranged from $15,029 in 2010 to $16,243 in 2015 (U.S. Department of Health and Human Services).
We use multivariate logistical regressions to estimate changes in likelihood of formal volunteering and informal helping associated with Medicaid expansions. We calculate estimates first for the entire low-income population; then we add interaction terms with gender and race to examine their moderating effects. We also estimate changes in likelihood of volunteering for the top half of the income distribution to show that changes associated with Medicaid were present only among the low-income group.
All our multivariate models control for possible confounding factors: age, gender, race, ethnicity, marital status, employment status, educational attainment, presence of children under 18 in the household, family income, and urban or rural residence. We also include state and year fixed effects in all our models and use robust standard errors clustered by state.
Results
The low-income sample included 74,211 nonelderly adults across six years from 2010 to 2015. A total of 43,251 individuals resided in the 28 states that expanded Medicaid as of early 2015, and the remaining 30,960 resided in the 22 states that did not (Table 1). Residents in Medicaid expansion states were more likely to be college graduates living in urban areas. Although the proportion of whites was roughly equal between Medicaid expansion and nonexpansion states, nonexpansion states accounted for a greater proportion of African Americans.
Descriptive Characteristics of Low-income Sample.
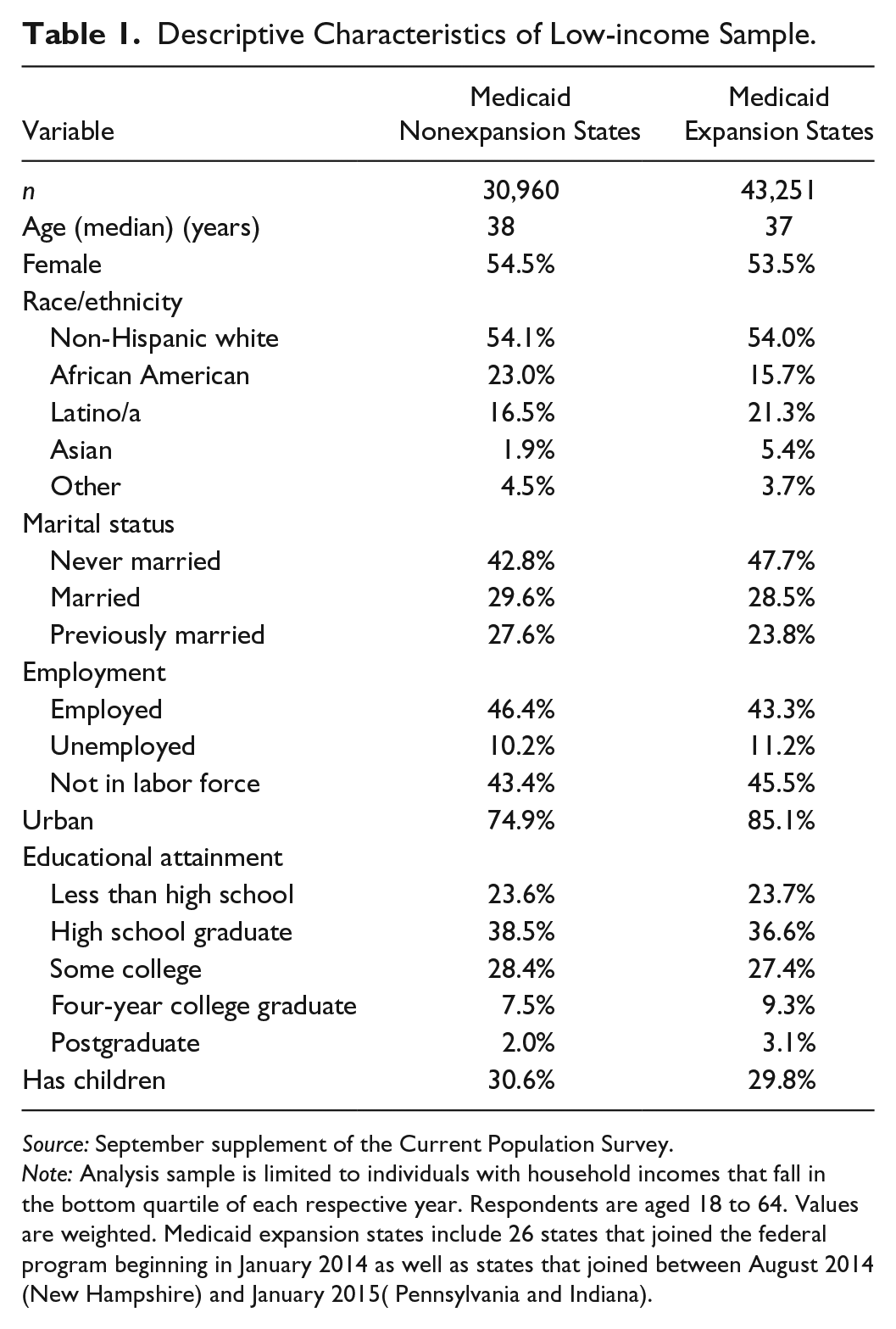
Source: September supplement of the Current Population Survey.
Note: Analysis sample is limited to individuals with household incomes that fall in the bottom quartile of each respective year. Respondents are aged 18 to 64. Values are weighted. Medicaid expansion states include 26 states that joined the federal program beginning in January 2014 as well as states that joined between August 2014 (New Hampshire) and January 2015( Pennsylvania and Indiana).
Figure 1 presents the percentage of respondents who volunteered for organizations and the percentage of respondents who informally helped neighbors in the past 12 months by state Medicaid expansion status (as of 2015) between 2010 and 2015. Prior to 2014, the proportions having volunteered formally and informally appear to be similar between expansion and nonexpansion states. A formal test of means confirms that the proportion of respondents engaged in both types of volunteer work is not statistically different. After 2014, the prevalence of volunteering for an organization in nonexpansion and expansion states diverged. The difference grew from Medicaid expansions states having more volunteers by 0.2 percentage points between 2010 and 2013 to having more volunteers by 2.8 percentage points in 2014 and 3.3 percentage points in 2015.
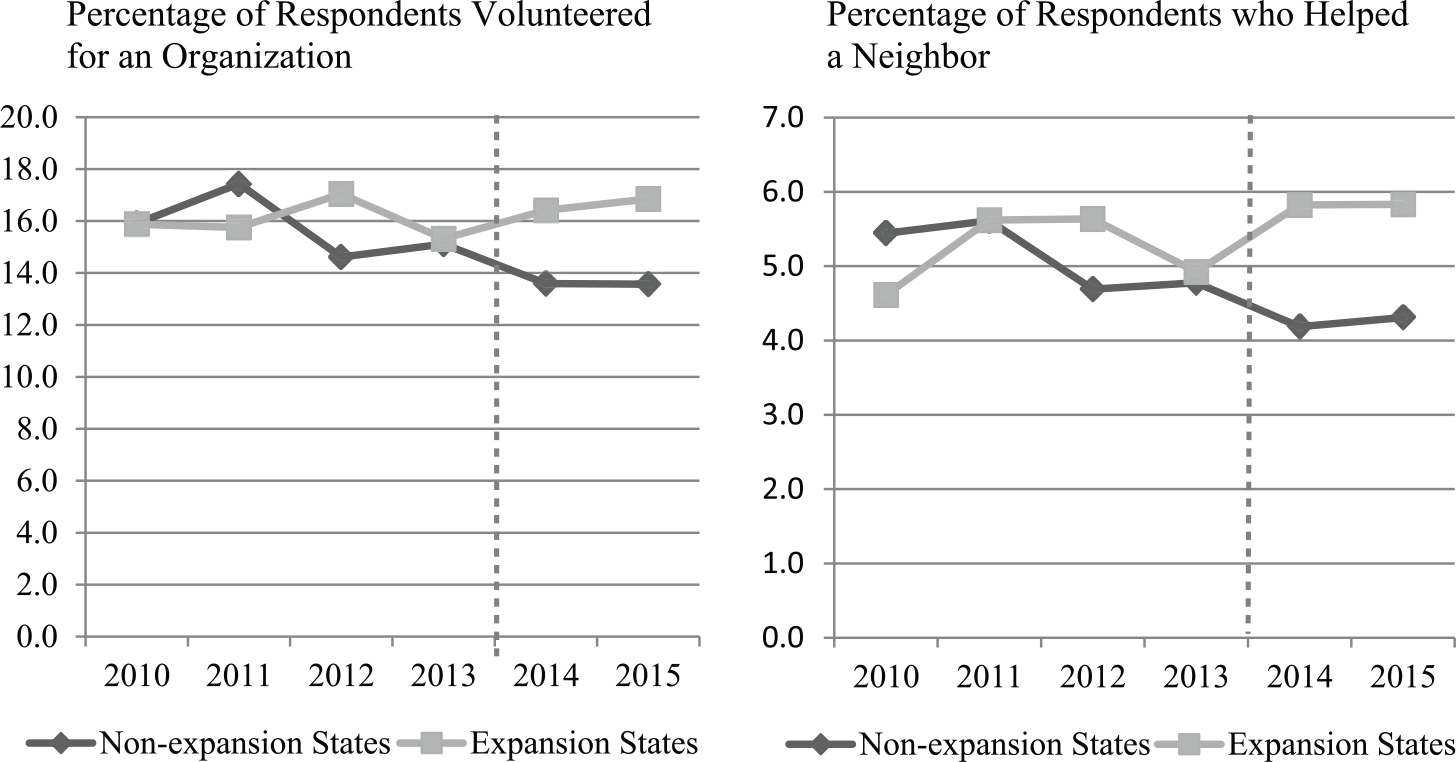
Unadjusted percentage of low-income respondents who engaged in formal volunteer work and informal helping during the past 12 months by state Medicaid expansion status.
The patterns observed in formal volunteer work are echoed in patterns of informal helping. After 2014, the gap in proportion of people engaging in informal helping increased noticeably. The difference in prevalence between expansion and nonexpansion states was 0.1 percentage points during the four years leading up to the ACA. This difference increased to 1.6 the year after ACA.
Trends in volunteer work among higher income residents in Medicaid expansion states did not differ from those in nonexpansion states after 2014. Figure 2 shows the unadjusted levels of formal and informal volunteering among those in the top half of the income distribution. A greater proportion of higher income individuals volunteered than low-income individuals. However, volunteer work among the higher income group declined in both expansion and nonexpansion states between 2010 and 2015. This is the general trend for all income-state expansion status groups except those that likely benefited from the ACA’s Medicaid expansions.

Unadjusted percentage of higher income respondents who engaged in formal volunteer work and informal helping during the past 12 months by state Medicaid expansion status.
Table 2 present the results from the difference-in-difference analysis of Medicaid expansion among low-income residents on the two measures of volunteer work: likelihood of volunteering for an organization and likelihood of working with a neighbor to improve or fix things. They collectively demonstrate that levels of volunteerism, both formal and informal, increased among those who most likely benefited from Medicaid expansions. These estimates formally test differences observed among low-income nonelderly adults in Figure 1. They are also adjusted for age, gender, race and ethnicity, marital status, employment status, urban residence, educational attainment, presence of own child under 18 in household, state, and year. Robust standard errors are clustered by state. Prior to Medicaid expansions, low-income adults living in expansion states were less likely to volunteer for organizations than low-income adults living in nonexpansion states (relative odds = 0.91). After expansions took effect, the relative odds of formal volunteering increased to 1.31 for those living in expansions states. In comparison, the relative odds for those living in nonexpansion states increased from 1.0 to 1.14 after 2014. The difference-in-difference estimates show relative odds of 1.27 associated with Medicaid expansions.
Changes in Formal and Informal Volunteer Work among Low-income Adults in Medicaid Expansion versus Nonexpansion States.
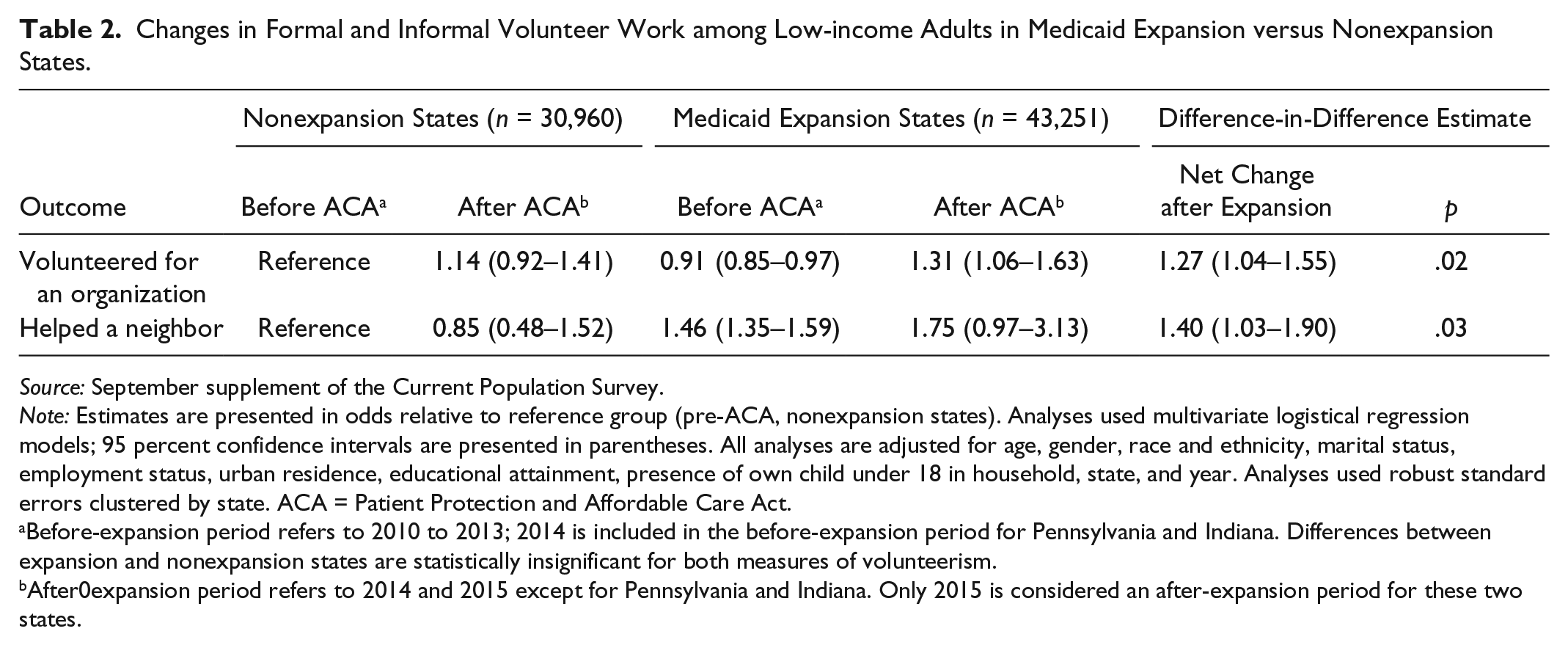
Source: September supplement of the Current Population Survey.
Note: Estimates are presented in odds relative to reference group (pre-ACA, nonexpansion states). Analyses used multivariate logistical regression models; 95 percent confidence intervals are presented in parentheses. All analyses are adjusted for age, gender, race and ethnicity, marital status, employment status, urban residence, educational attainment, presence of own child under 18 in household, state, and year. Analyses used robust standard errors clustered by state. ACA = Patient Protection and Affordable Care Act.
Before-expansion period refers to 2010 to 2013; 2014 is included in the before-expansion period for Pennsylvania and Indiana. Differences between expansion and nonexpansion states are statistically insignificant for both measures of volunteerism.
After0expansion period refers to 2014 and 2015 except for Pennsylvania and Indiana. Only 2015 is considered an after-expansion period for these two states.
Low-income adults living in expansion states were more than twice more likely to help a neighbor after the ACA went into effect in 2014 than their nonexpansion state counterparts (1.75 vs. 0.85). This is a notable increase in difference from relative odds of 1.46 and 1.00 for expansion and nonexpansion states, respectively, prior to Medicaid expansions. Increases in both forms of volunteer work associated with Medicaid expansions were statistically significant at an α level of .05, with robust standard errors accounting for clustering within states.
Figure 3 shows the relative odds of volunteering among the higher income groups in expansion and nonexpansion states. Unlike the low-income group, individuals in the top half of the income distribution living in Medicaid expansion states did not experience an increase in volunteer work. Repeating the patterns in Figure 2, volunteerism dropped after 2014 among all groups in the higher income category. Likewise, another group that was not directly affected by Medicaid expansions, individuals over age 65, did not experience an increase in volunteer work. A parallel difference-in-difference analysis of low-income adults aged 65 to 80 (Appendix Table A1) confirms that both measures of volunteerism did not change with Medicaid expansions. Adding more to the connection between Medicaid expansions and volunteer work, individuals who likely gained new eligibility showed a statistically stronger association. Low-income single parents were more likely than non–single parents prior to the expansions, and the ACA explicitly targeted all low-income individuals regardless of family status. Low-income individuals who were not single parents showed a stronger relative increases in both formal and informal volunteer work in expansion states after the ACA than similar single parents (Appendix Table A2).
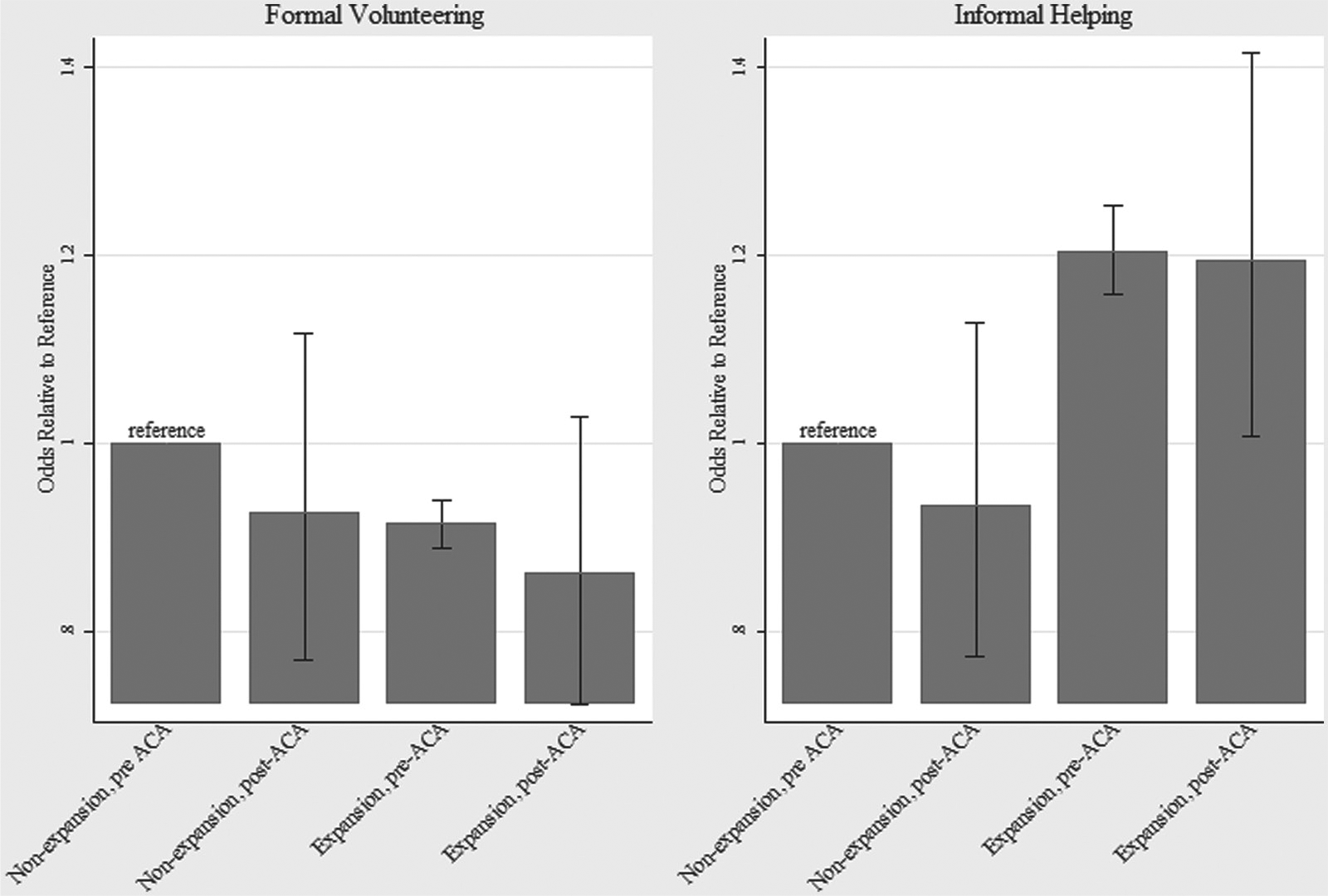
Adjusted relative odds of having volunteered formally and informally for the higher income group in expansions and nonexpansion states before and after the ACA.
Table 3 shows volunteerism between Medicaid expansion and nonexpansion states before and after the ACA by gender and race. The rates of formal and informal volunteer work mirror the pattern seen in Table 2. Residents living in expansion states were less likely to volunteer for organizations prior to the ACA but exceed their nonexpansion state counterparts after the ACA. Informal helping was more prevalent in expansions states prior to the ACA, and the gap further increased after the ACA. Women are more likely to volunteer for organizations than men prior to 2014, and the gender difference persisted after Medicaid expansions. The analysis shows less significant gender difference in informal helping. Increases in formal and informal volunteer work associated with Medicaid were similar between men and women.
Changes in Formal and Informal Volunteer Work among Low-income Adults in Medicaid Expansion versus Nonexpansion States by Subgroup.

Source: September supplement of the Current Population Survey.
Note: Estimates are presented in odds relative to the reference group. Analyses used multivariate logistical regression models. Ninety-five percent confidence intervals are presented in parentheses. All analyses are adjusted for age, gender, race and ethnicity, marital status, employment status, urban residence, educational attainment, presence of own child under 18 in household, state, and year. Analyses used robust standard errors clustered by state. ACA = Patient Protection and Affordable Care Act.
Before-expansion period refers to 2010 to 2013; 2014 is included in the before-expansion period for Pennsylvania and Indiana.
After-expansion period refers to 2014 and 2015 except for Pennsylvania and Indiana. Only 2015 is considered an after-expansion period for these two states.
Prior to the ACA, minority groups, especially Latino/as, were less likely to have formally volunteered for organizations. After the ACA, formal volunteerism converged toward that of whites for minority groups living in states that expanded Medicaid. The race and ethnic gap in formal volunteer work appears to have increased in states that did not expand Medicaid.
Consistent with past research, African Americans were equally likely to give informal help as whites before Medicaid expansions took place in 2014. Informal helping among African Americans living in states that expanded Medicaid exceeded that of whites after the ACA. Latino/a residents were significantly less likely to engage in informal volunteering than whites prior to Medicaid expansions. Although the difference persisted after the expansions, the gap between Latino/as and whites narrowed for residents who lived in states that expanded Medicaid. This gap widened in states that did not expand Medicaid.
Although all groups living in Medicaid expansions states experienced increases in volunteer work, changes associated with Medicaid expansions were significantly larger among Latino/a respondents. Medicaid expansions were associated with an increase in formal volunteer work by 1.72 (relative odds of volunteering) among Latino/as compared with 1.11 among white respondents. This difference (1.55) was statistically significant at α = .01. Increases in informal helping associated with Medicaid were also the largest among Latino/a respondents although the difference compared to whites was not statistically significant.
Discussion
Our analysis shows an association between volunteer work—both formal volunteering for organizations and informally helping a neighbor—and states’ Medicaid expansions following the ACA. Likelihood of volunteer work increased among low-income individuals when their home states expanded Medicaid eligibility to all whose household incomes fell below 138 percent of the FPL. Similar low-income respondents living in states that did not expand Medicaid did not experience such a rise in volunteerism. That volunteer work increased among the low-income group is especially notable; income has been a strong predictor of volunteerism and those with the least income were also less likely to volunteer (Wilson 2000).
Medicaid expansions did not close the gender gap in volunteering. Men were less likely to volunteer for organizations and help neighbors prior to the ACA than women, and although both genders increased their participation in Medicaid-expansion states, the gender difference remained. Prior research suggests that gender differences in volunteer work stemmed more from structural and cultural differences related to gender role expectations and opportunities that are difficult to overcome by giving more resources to some individuals (Marini et al. 1996; Musick and Wilson 2008; Negrey 1993; Scott 1991). Thus, it is unsurprising that Medicaid did not affect one gender significantly more than the other.
Echoing the findings of prior work, the analysis also showed that minority groups were less likely to volunteer for organizations than their white counterparts. This gap in rates of formal volunteerism narrowed among those who living in states that expanded Medicaid. Medicaid expansions were associated with the largest increases in formal volunteer work among Latino/as, suggesting that greater access to public insurance mitigated some of the barriers—financial insecurity and perception of poor health—that they disproportionately faced. Medicaid expansions were also associated with greater informal helping among minority groups. After accounting for sociodemographic differences, African Americans living in states that expanded Medicaid were significantly more likely to help a neighbor than their white counterparts. Differences in informal volunteering between Latino/as and whites also narrowed in Medicaid expansion states.
This analysis is not without limitations. The cross-sectional data also limit casual inference between public health insurance and volunteerism. The supplement of the CPS does not contain respondents’ health insurance coverage history which would have allowed direct examination of Medicaid coverage gain under the ACA and volunteerism. Yet sensitivity analyses bolster the relationship between Medicaid expansion and volunteerism. The relationship between expansions and volunteer work was not present in groups that did were not directly affected by Medicaid expansions. Volunteer work did not change with expansions for higher income adults as well as adults above age 65. Furthermore, low-income adults who were unlikely to have qualified for Medicaid prior to the ACA—those who were not single parents—showed a significantly greater relationship between expansions and volunteer work. Triple difference analyses show stronger association between Medicaid expansions and volunteerism among minority groups. However, the analysis cannot distinguish whether the findings are due to greater effect of public insurance per se or to Medicaid expansions resulting in more new coverage among minorities. Nonetheless, our results suggest that the gap in volunteerism between income and racial groups have narrowed in states that expanded public insurance coverage.
Nonrandom assignment of Medicaid expansions across states also limits the analyses from establishing a causal relationship with volunteerism. States that decided not to expand Medicaid are roughly clustered in the South and the Midwest. These states were also generally late in adopting Medicaid when it was first introduced in 1965. However, difference in volunteerism between expansion and nonexpansion states prior to the ACA had no statistical significance, while after the ACA, such differences in volunteer rates and hours have emerged.
Despite these limitations, this study suggests that changes in public health insurance policy have accompanied changes in social behaviors. Such prosocial behavior may circle back to produce improved population health outcomes. Although this goes beyond the scope of the data, an extensive literature has found that even a limited amount of volunteer work is associated with decreased psychological distress (Thoits and Hewitt 2001), higher life satisfaction, reduced risk behavior, better physical health, and lower mortality (Konrath 2014). The narrowing of racial and ethnic differences in volunteerism that followed Medicaid expansions suggests then that greater availability of insurance coverage may be reducing health inequalities in indirect ways. Should these health dividends return to the groups that experienced the largest increases in volunteerism—low-income minorities—with Medicaid expansions, the recent health reforms’ impact on health disparities may be even greater than what recent studies find.
Footnotes
Appendix
Changes in Formal and Informal Volunteer Work among Low-income Adults in Medicaid Expansion versus Nonexpansion States by Subgroup.

| Nonexpansion states |
Medicaid Expansion States |
Triple-Difference Estimates |
||||
|---|---|---|---|---|---|---|
| Before ACA a | After ACA b | Before ACA a | After ACA b | Between-group Difference in Change after Expansion | p | |
| Relative odds of volunteering for an organization | ||||||
| Single parent | Reference | 1.37 (1.06–1.76) | 1.13 (0.97–1.3) | 1.33 (1.08–1.63) | Reference | |
| Non–single parent | 0.95 (0.85–1.07) | 1.04 (0.83–1.31) | 0.82 (0.72–0.94) | 1.25 (1–1.56) | 1.60 (1.34–1.92) | .000 |
| Relative odds of helping a neighbor | ||||||
| Single parent | Reference | 1.08 (0.53–2.17) | 1.94 (1.65–2.29) | 1.68 (0.84–3.38) | Reference | |
| Non–single parent | 1.0027 (0.87–1.15) | 0.81 (0.44–1.48) | 1.39 (1.2–1.6) | 1.73 (0.95–3.16) | 1.93 (1.11–3.33) | 0.019 |
Note: Estimates are presented in odds relative to the reference group. Analyses used multivariate logistical regression models; 95 percent confidence intervals are presented in parentheses. All analyses are adjusted for age, gender, race and ethnicity, marital status, employment status, urban residence, educational attainment, state, and year. Analyses used robust standard errors clustered by state. ACA = Patient Protection and Affordable Care Act.
Before-expansion period refers to 2010 to 2013; 2014 is included in the before-expansion period for Pennsylvania and Indiana.
After-expansion period refers to 2014 and 2015 except for Pennsylvania and Indiana. Only 2015 is considered an after-expansion period for these two states.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project benefited from facilities and resources provided by the California Center for Population Research at the University of California, Los Angeles, which receives core support (R24-HD041022) from the Eunice Kennedy Shriver National Institute of Child Health and Human Development.