
Abstract
Background
Community nursing is crucial for health equity yet often underexposed in training. Perceptions were compared between first-year students and practicing community nurses to inform workforce strategies.
Objective
To compare the perceptions of nursing students and practicing professionals, moving beyond vocational preference to explore the meanings that shape professional identity in the community setting.
Methods
Through non-probabilistic intentional sampling, 67 participants were included (48 first-year students and 19 practicing professionals). Data collection occurred in October 2024 for Phase I, while implementation dates for Phase II were November to December 2024. Data collection methods comprised a self-administered questionnaire (SCOPE scale) for Phase I, and Photovoice (photography and guided discussions) for Phase II. Data analysis techniques involved descriptive and inferential statistics for quantitative data, and an iterative participatory thematic analysis for qualitative data. Integration used joint displays and a rigorous “follow-the-thread” technique to trace meta-inferences.
Results
Professionals scored significantly higher than students across all SCOPE domains (p < .001) and asset-mapping knowledge (84.2% vs. 27.1%). While 89.6% of students preferred hospitals, integration revealed a structural convergence: this statistical preference aligns with the qualitative theme of “The invisible nurse,” suggesting vocational choices are constrained by a lack of role models. Conversely, a divergence emerged between students’ high theoretical valuation of public health and their low affective scoring, revealing a “vocational dissonance” that contrasts with the professionals’ consolidated identity.
Conclusions
A marked perception gap separates students from community nurses. Theoretically, the study illustrates how professional identity is shaped by role visibility. At a policy level, findings suggest that ensuring workforce sustainability requires not only curricular reform but also institutional strategies that elevate the symbolic status of primary care to attract talent.
Background
Nursing has evolved from empirical practice to a university profession with a distinct scientific identity committed to public health (Donahue, 2011; Riegel et al., 2021). In Spain, legislative frameworks legally recognize Family and Community Nursing as a pivotal specialty (Real Decreto 2128/1977, 1997; Real Decreto 450/2005, 2005; Real Decreto 822/2021, 2021). This normative framework aligns with the principles of Alma-Ata (Davletov et al., 2018), and extensive literature linking strong primary care to reduced mortality and greater system efficiency (Starfield et al., 2005).
Despite evidence of their clinical efficacy, community nurses face structural invisibility and alarming staffing shortages. While the systemic need for robust primary care is well established, a significant research gap remains regarding the underlying causes of these shortages at the vocational and perceptual levels. Existing knowledge often focuses on the broader consequences of workforce deficits, yet it fails to adequately explore how the “perception gap” between future professionals and practicing community nurses actively undermines recruitment. Specifically, the symbolic divergence between how students imagine the community role and how professionals actually live it remains underexplored. Highlighting and analyzing this empirical gap is critical to strengthening the rationale for targeted interventions; failing to address these perceptual discrepancies poses a direct threat to nursing workforce sustainability and the long-term capacity of primary care systems. Therefore, this study addressed the critical gap between recognized workforce challenges and the unexplored symbolic barriers that hinder professional identity formation.
Review of Literature
The previous starting point fuels a “hospital-centric” bias among undergraduates, with over 70% preferring hospital placements due to perceived lower status. This hospital-centric bias is not a phenomenon exclusive to the Spanish context; international evidence suggests that the lack of early exposure to primary care is a systemic challenge for nursing education and workforce development globally (Van Iersel et al., 2016; Van Iersel, Latour et al., 2018). Although curricular redesigns exist, an empirical gap remains in understanding the symbolic divergence between the novices’ “imagined role” and the experts’ “lived role,” which this study addresses through a mixed-methods lens (Banegas et al., 2008; Consejo General de Colegios Oficiales de Enfermería de España, 2025; Laurant et al., 2018; Robles & Pozo, 1999; Van Iersel, Latour et al., 2018).
While curricular redesigns attempt to mitigate these stereotypes (Arrogante, 2017; Van Iersel et al., 2019, 2020), an empirical gap remains in understanding the symbolic divergence between the “imagined role” by novices and the “lived role” by experts. Addressing this perception gap is urgent to inform recruitment strategies and sustain the healthcare system's response to social inequalities (Valls Pérez et al., 2018). Therefore, this study aimed to compare the perceptions of nursing students and practicing professionals, moving beyond vocational preference to explore the meanings that shape professional identity in the community setting.
To address the complexity of this vocational gap, a mixed-methods approach is essential, as quantitative metrics alone cannot capture the latent symbolic associations driving “vocational dissonance” (Millán Klüsse, 2018; Olson et al., 2016). Grounded in the theoretical framework of professional identity formation, which posits that career orientation evolves through the interplay of initial perceptions and social learning experiences, this study employs an explanatory sequential design. Photovoice was specifically selected as the qualitative vehicle to allow participants to objectify their reality (Budig et al., 2018; Wang & Burris, 1997), overcoming the limitations of verbal discourse in exploring “invisible” roles (Bourgeault et al., 2010; Catalani & Minkler, 2010). This participatory method aligned with the study's aim by fostering critical reflection and empowering participants to visualize distinct professional identities.
Theoretically, this study was anchored in the framework of professional identity formation (PIF). PIF is defined as the transformative process through which an individual internalizes the values, behaviors, and norms of a profession, evolving from a layperson to a professional (Cruess et al., 2014; Cruess & Cruess, 2018). Key to this process is “anticipatory socialization” (Merton et al., 1957), whereby students conceptually “rehearse” future roles based on the visibility of role models and social feedback. In nursing, professional identity implies the integration of personal attributes and professional values derived from nursing education and practice (Ten Hoeve et al., 2014). This relies heavily on social validation and role visibility. When specific roles, such as community nursing, lack of visibility or are stereotyped as “low-tech” in the public and academic imagination, the student's ability to internalize this professional role is compromised, leading to the “perception gap” explored in this study.
Consequently, the specific objectives of this study were: (1) to quantitatively measure and compare affective and practical perceptions (Phase I); and (2) to qualitatively dissect the symbolic meanings of community practice through visual narratives (Phase II), integrating both datasets to inform educational policy and workforce strategies. Ultimately, this study aimed to clarify how the “vocational dissonance” arising from unresolved perceptual gaps contributes to recruitment failure, role invisibility, and professional burnout, ultimately weakening primary care systems from a nursing practice and policy perspective.
Materials and Methods
A sequential explanatory mixed-methods design was implemented to obtain a comprehensive understanding of perceptions of community nursing. The quantitative phase (Phase I) provided an overview, while the qualitative phase (Phase II) allowed for in-depth exploration. Phase II was connected to Phase I by inviting those who completed the questionnaire to participate. The final integration was achieved by merging findings (joint displays) and following threads (“follow-the-thread”) to explain convergences and divergences.
For the report, STROBE was followed during the quantitative phase (Von Elm et al., 2007) and COREQ for the qualitative phase (Tong et al., 2007), in addition to guidelines for the integration of mixed data (Draucker et al., 2020; Fetters et al., 2013; O’Cathain et al., 2010).
Scope and Context
The study was conducted in the Vigo Health Area (Spain), a region characterized by an aging population and high dispersion, which places significant pressure on community services. While the National Health System relies on Primary Care as its backbone, academic culture remains historically hospital-centric, creating a tension between public health mandates and educational traditions.
Participants, Eligibility and Sample Size
The study targeted nursing students and active professionals. Inclusion criteria were: (a) enrollment in a Spanish Nursing Degree (students) or employment in a Health Centre in the Vigo Health Area (professionals); (b) language proficiency; and (c) informed consent. Exclusion criteria were: (a) students with prior healthcare work or clinical placement experience; (b) professionals in non-community roles; (c) active leave of absence; and (d) inability to complete the 6-month study period.
First-year nursing students were conceptualized as novices based on theories of anticipatory socialization and early professional identity formation, which posit that students’ initial perceptions of the profession are shaped prior to extensive clinical exposure (Benner, 1984). At this early stage of training, students’ views of nursing roles are predominantly informed by pre-existing social representations and limited educational contact, making this group particularly suitable for exploring baseline perceptions of community nursing.
Sample size determination relied on “Information Power” (Malterud et al., 2016), rather than probabilistic representativeness. According to this model, a smaller sample is sufficient when the study aim is narrow, the participants hold high specificity, and the dialogue quality is strong. In this study, the specificity was maximized by selecting first-year students (novices) and established community nurses (experts) within a specific health area.
The quantitative sample (n = 67) provided sufficient power for non-parametric testing, while qualitative collection ceased upon reaching meaning saturation regarding role invisibility and technological use. This density of qualitative data compensates for the sample size, prioritizing depth of understanding over breadth.
Variables, Instruments, and Materials
Phase I Quantitative
A self-administered questionnaire was designed with three sections:
Sociodemographic variables such as gender, age, and year of commencement of studies (for students) or years of experience in primary care and route into employment (for professionals). Multiple-choice questions on knowledge and perceptions of community nursing, and preferences and attitudes toward this field. This section collected data on specific items regarding knowledge and preferences for community nursing. The content validity of these ad-hoc items was established by a panel of four independent experts, including two academic researchers and two community nurses. The panel reviewed the items for clarity and relevance, achieving a consensus on their final wording. The Scale on COmmunity care PErceptions (SCOPE), which assesses students’ perceptions of community nursing in three domains: affective perception, perception of practices, and location preferences (Van Iersel, de Vos et al., 2018). Each item is rated from 1 to 10, and mean scores are calculated for each domain and a total score. SCOPE achieved adequate reliability coefficients (Cronbach's α = 0.89 overall) in its original study. The original English version of the SCOPE scale was administered, as participants were required to have an adequate proficiency in English as an inclusion criterion. While no linguistic adaptation was performed, the internal consistency of the scale in this specific sample was assessed, yielding a Cronbach's α of 0.82, which indicates satisfactory reliability comparable to the original study.
Phase II Qualitative
Photovoice was used as a participatory methodology to explore meanings and practices in the community from the perspective of students and professionals. This technique enables participants to express and reflect on their experiences through photography (Catalani & Minkler, 2010; Wang & Burris, 1997). Three working groups were formed (two with students, one with professionals), each with four weekly sessions. The sessions combined framing and image ethics, photographic production by the participants themselves, guided discussion using the SHOWED guideline (“What do you see? / What is happening? / How does it relate to our lives? / Why does it exist? / What can we do?”), and a group synthesis with selection of photographs and construction of categories. Audio recorders and color printers were used for this part of the study (Catalani & Minkler, 2010).
Procedures
Participant recruitment was organized in October 2024 through the usual institutional channels for each group. Those interested received a link/QR code to an initial online questionnaire. Before the first question, a clear explanation of the purpose and conditions of participation was provided, emphasizing that participation was voluntary. To begin, participants had to tick a mandatory checkbox to accept the informed consent and privacy policy.
Quantitative data collection was administered by members of the research team who were not involved in participants’ academic assessment. Questionnaires were completed anonymously and on a voluntary basis, and participants were informed that their responses would have no impact on their academic evaluation. These procedures were implemented to reduce potential response and social desirability bias.
The questionnaire was self-administered and took approximately 10 min to complete. At the end, participants were given the option to express interest in participating in the qualitative phase, reminding them of the need to attend all four sessions to ensure continuity.
The qualitative phase was planned as a progressive four-week itinerary per group:
First session: The methodological and ethical framework was discussed, including safety guidelines for taking photographs (avoiding identifiable faces without consent) and handling materials. The photographic assignment was established. Second and third sessions: Participants presented their photographs and a critical dialogue was developed, guided by the SHOWED guideline. The conversations were audio recorded for analytical purposes, with no personal identifications in the transcripts. The images were printed to facilitate the work. Fourth session: This was devoted to collaborative synthesis. The group selected the most representative photographs and, based on these, constructed thematic categories and agreed-upon descriptors. With this material, the principal investigator developed an integrative analysis that preserved the participants’ voices.
Data Analysis
Quantitative analysis was performed using R (v4.3.1). Qualitative variables were summarized in absolute frequencies and percentages, while quantitative/ordinal variables were expressed as median and interquartile range (IQR) due to their non-parametric distribution. For the comparison between students and professionals, Pearson's chi-square test (χ2) was applied to categorical variables and the Mann–Whitney U test when appropriate. A confidence level of 95% was used, and p < .05 was considered the threshold for significance. The internal consistency of the SCOPE scale was calculated using Cronbach's α.
Following preliminary analysis of the quantitative data, key patterns and areas of ambiguity related to perceptions of community nursing were identified. These findings directly informed the development of the Photovoice discussion guide, which was designed to explore participants’ interpretations of role visibility, perceived professional value, and experiential influences underlying the quantitative trends. This sequential “connecting” process ensured that the qualitative phase functioned as an explanatory component of the mixed-methods design.
The qualitative analysis focused on the Photovoice products (photographs, narratives, recorded discussions, and agreed-upon thematic map). The relevant audio segments were transcribed verbatim in Microsoft Word. A participatory thematic analysis was developed, consolidating emerging categories defined by each group and producing a cross-sectional reading that connected them with the visual narratives and questionnaire patterns. The report was aligned with COREQ and criteria of credibility, transferability, dependability, and confirmability (Korstjens & Moser, 2018; Malterud, 2001; Tong et al., 2007).
Qualitative data from the Photovoice sessions were analyzed using an iterative thematic analysis approach. An initial phase of open coding was conducted independently by two members of the research team to identify meaningful units related to perceptions of community nursing. Codes were then compared, discussed, and refined through consensus, leading to the development of preliminary categories. In a subsequent phase, categories were grouped into broader themes through constant comparison, guided by the study's conceptual framework. Analytic decisions were documented throughout the process to enhance transparency and methodological rigor.
Integration of quantitative and qualitative findings occurred through an explicit “follow-the-thread” approach. Key quantitative results were first identified and used as analytical anchors. These results were then traced into the qualitative data to explore how participants’ narratives and visual representations helped explain, expand, or contextualize the quantitative patterns. Joint displays were developed to visually align quantitative findings with corresponding qualitative themes, facilitating systematic comparison and the generation of integrated interpretations. This process supported the development of meta-inferences that synthesized insights across both methodological strands.
The mixed integration (Fetters et al., 2013; Guetterman et al., 2015; O’Cathain et al., 2010) was articulated in three interconnected stages, visualized in Figure 1:
Connecting: The descriptive results of the questionnaire (Phase I) directly informed the sampling and the focus of the Photovoice discussion guide (Phase II), prioritizing topics where perception gaps were widest. Merging: Quantitative scores and qualitative themes were brought together using Joint Displays to identify convergences and expansions. Weaving (“follow-the-thread”): Finally, the narrative synthesis used the “follow-the-thread” approach, tracing statistical patterns to visual evidence to generate integrated meta-inferences.

Visual model of the explanatory sequential design and integration procedures.
Quality Assurance and Biases
To address information bias in the quantitative phase, the questionnaire was self-administered, with standardized instructions and a short response time to minimize fatigue. Anonymity and confidentiality were reinforced from the outset to reduce social desirability.
In the qualitative analysis, the risk of dominant group dynamics was addressed with a stable script for four sessions and the use of SHOWED to focus the analysis on common images and questions, ensuring the study's dependability. Recordings were deleted once used, and image rights were managed when identifiable people appeared in the photos. The consensual selection of photographs and the construction of categories in the final session underpinned the credibility of the analysis through participatory validation.
A key asset of the study was the plurality of researcher profiles. The principal investigator is a female nurse who was still a student at the time of the investigation. It was she who conducted the fieldwork occupying an “insider” position relative to the student participants. This horizontal relationship minimized power hierarchies, facilitating more authentic disclosure during Photovoice sessions. In contrast, the co-investigators adopted an “outsider” perspective, from an academic and “clinical” point of view, being a female nurse and a male occupational therapist ensuring methodological rigor and theoretical distance. Although gender perspective is not explicitly addressed in the study, it is important to mention that nursing is a highly feminized profession in Spain, and this has influenced the analysis of the results.
To mitigate potential biases—such as the student researcher over-identifying with the participants’ anxieties—the team implemented investigator triangulation. Regular debriefing sessions were held to cross-check coding and interpretations, ensuring that the findings reflected the data rather than the researchers’ preconceptions (confirmability). Finally, transferability was supported by the thick description of the sociocultural context and participants provided in the methodology sections.
Ethical Considerations
The study complied with the Declaration of Helsinki and local regulations and was approved by the IRB of the Nursing Management of the Vigo Health Area (with code 137-10-24). Informed consent, including specific permission for audio recording, was obtained via the online platform. The voluntary nature of participation, the possibility of withdrawal without repercussions, and the commitment to anonymity and confidentiality were emphasized. In Photovoice, specific consent was requested for audio recording, indicating its exclusive use for analysis and its subsequent deletion after transcription.
Beyond procedural compliance, the ethical framework of this study was grounded in the principles of inclusive research. By employing Photovoice, this study sought to shift the traditional power dynamic between researcher and subject, moving from an extractivist model to one of co-creation. Participants were not merely data sources but active agents who defined the narratives of their own professional reality. This approach fostered a form of “epistemic empowerment,” particularly relevant for a professional group that reported feeling “invisible.” By handing the camera to the participants, the study ensured that the representation of community nursing was self-determined, aligning scientific rigor with the ethical imperative of giving voice to the protagonists of care.
Results
The total sample consisted of 67 participants, divided into 48 first-year nursing students and 19 practicing community nurses. In both subgroups, females predominated (91.7% among students and 94.7% among professionals). The average age of the students was 19 years (IQR: 18–20), while among the professionals, the median age was 42 years (IQR: 36–52).
Phase I
Students expressed a generally positive but abstract assessment of community nursing (CN). While 75% reported intermediate knowledge and 68.8% acknowledged its public health importance, specific technical awareness was low; only 27.1% recognized “asset mapping,” and 89.6% expressed a clear preference for hospital placements (Table 1).
Summary of Characteristics and Perceptions of Community Nursing Among Students and Professionals (Phase I).

Note. n = number of participants; IQR = interquartile range; CN = community nursing; SCOPE = SCale on COmmunity care Perceptions.
In contrast, professionals displayed a consolidated identity. Nearly all (94.7%) rated CN as vital for public health, and 84.2% were familiar with asset mapping. Bivariate analysis confirmed significant divergences across all variables (Table 1). The most striking contrast appeared in placement preferences: while nearly 90% of students chose hospitals, only 5.3% of professionals did so (p < .001). Similarly, interest in future specialization was significantly lower among students (22.9% vs. 57.9%; p = 0.01).
Table 1 summarizes the main sociodemographic and perceptual variables collected in Phase I.
Regarding the SCOPE scale (Table 2), professionals scored significantly higher across all three domains (p < .001). The largest gaps were found in “Perception of Practices” and “Location Preferences,” confirming that students view the community setting as less attractive and technically versatile than their practicing counterparts.
Comparison of SCOPE Scale Scores Between Students and Professionals.
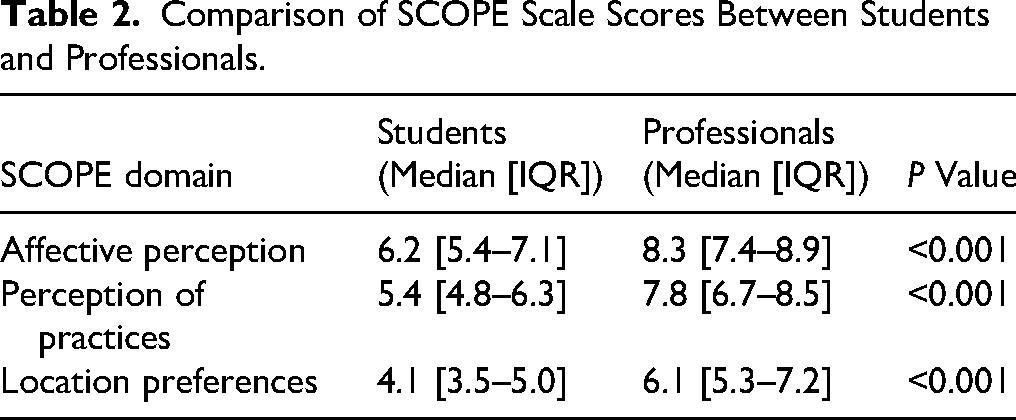
These quantitative results allowed for the identification of not only a difference in degree, but also a structural pattern of divergence between the two groups. While students tend to view CN from a more diffuse, emotional perspective and with less professional appeal, professionals build their perception on an experiential, critical, and strategic basis, which is evident in their recognition of the preventive, community and longitudinal value of this field.
In terms of convergence, both groups agreed in identifying academic deficits and low institutional visibility of CN as significant barriers to its development. This shared assessment was expanded in the qualitative phase.
Phase II
The qualitative phase, using Photovoice, allowed for an in-depth exploration of the representations and meanings associated with community nursing. Three working groups were formed (two of students, one of professionals) which generated 73 photographs, visual and verbal narratives, and a thematic map agreed upon by each group. From the integration of this material, seven main thematic categories emerged, shared to a greater or lesser extent by both groups.
“More Than Techniques”: Redefining Care from Proximity
Participants reconceptualized community care as a sophisticated relational practice rather than a mere absence of technical tasks. Through images of domestic spaces and neighborhood interactions, the visual narratives emphasized longitudinal accompaniment and adaptability. As one professional noted, the lack of rigid hospital protocols required a higher level of listening and contextual judgment. In hospital, everything is faster and more punctual. Not here. Here, you have to listen before you act. There isn't always a formula. (Professional) It's like accompanying people, not just healing them. That's nursing too. (Student)
This category challenged the stereotype that community nursing is “less clinical” or “more boring,” positioning it as a complex exercise in relational and contextual management.
“The Invisible Nurse”: Low Institutional Visibility of the Community Role
A pervasive sense of structural invisibility emerged. Visual data depicting closed doors and empty offices served as metaphors for the professionals’ perceived lack of institutional recognition. This mirrored the students’ confusion regarding the specific competencies of the role, often reducing it to basic tasks like vaccination. The data suggested a cycle where lack of visibility reinforces professional stereotypes. They see us as the ones who give injections and little else. But we do so much more. (Professional) Before this, I didn’t know that community nurses did health education or workshops. I thought they just gave vaccinations. (Student)
This category was linked to the quantitative findings regarding low scores in the dimension of perception of practices and location preferences.
“Technology with a Human Face”: Innovation Without Dehumanization
Contrary to the “low-tech” stereotype, professionals utilized photography to highlight digital tools (tablets, e-health apps) as strategic assets for maintaining continuity of care. While professionals viewed technology as an ally for connecting with patients outside the clinic, this instrumental dimension was notably absent from student narratives, reflecting a gap in their understanding of modern community practice. Community nursing adapts. It is not about white coats and clinics, it is about comfortable shoes and a mobile phone in hand. (Professional)
In contrast, female students did not discuss technology in any meaningful way, reflecting a still largely non-instrumental or non-applied view of their daily work.
“The Community as an Ally”: Networks, Support, and Environment
A key category shared by both groups was the recognition of community value understood as a network. The images showed parks, civic centers, neighborhood shops, and benches in a square. The emphasis was on interdependence and the role of the nurse as a “connector” between services, people, and resources. Here, everything is done with the people. It's not about imposing from above, it's about understanding what's going on and helping from there. (Professional) Sometimes the most important thing is not a cure, but knowing which association can help that person. (Student)
This finding reinforced the socio-political component of community care, which goes beyond the individual clinical act.
“Learning by Doing and Sharing”: The Need for Situated Training
The student group in particular highlighted experiential learning as a motivating factor. The images captured empty classrooms contrasting with bustling streets, symbolizing the gap between theory and practice. The students expressed a desire to learn through real contact with people and the local area. I don't know if I want to be part of the community because I haven't really experienced it. In class, everything is very general. (Student)
For their part, the professionals expressed that the development of community skills requires continuous training, reflection, and joint work. Sometimes you don't know if you're doing it right. There is no clear protocol, each case is different. (Professional)
“Be a Socializing Agent, Not Just a Healthcare Agent”
A specific category of professionals revolved around the figure of the nurse as a socio-cultural reference point and mediator. The photographs showed campaign posters, meeting spaces with groups, and handwritten notes from patients. This dimension involved taking on an educational, community-based, and sometimes activist role. We are often the only contact that person has with the system. We have to go beyond the diagnosis. (Professional)
This category broadened the scope of nursing work, showing it as a political and pedagogical practice as well.
“Caring as a Team”: The Value of Support among Professionals
Finally, both students and professionals valued teamwork as a protective factor against overload. The images included intertwined hands, whiteboards with shifts, and shared coffees. The importance of camaraderie and mutual recognition as a basis for sustaining care was emphasized. You can't care for others if you're broken. The team is what keeps you whole. (Professional) I imagine learning with someone to guide me. Not alone. (Student)
This category links to the need for mentoring, emotional support, and a healthy organizational culture.
Integration of Quantitative and Qualitative Results
To facilitate the comprehension of the convergence between phases, a Joint Display (Table 3) was developed following Guetterman et al.'s guidelines. This visual tool contrasts SCOPE scores with Photovoice narratives to reveal confirmation and expansion patterns.
Joint Display: Integration of Quantitative and Qualitative Results.
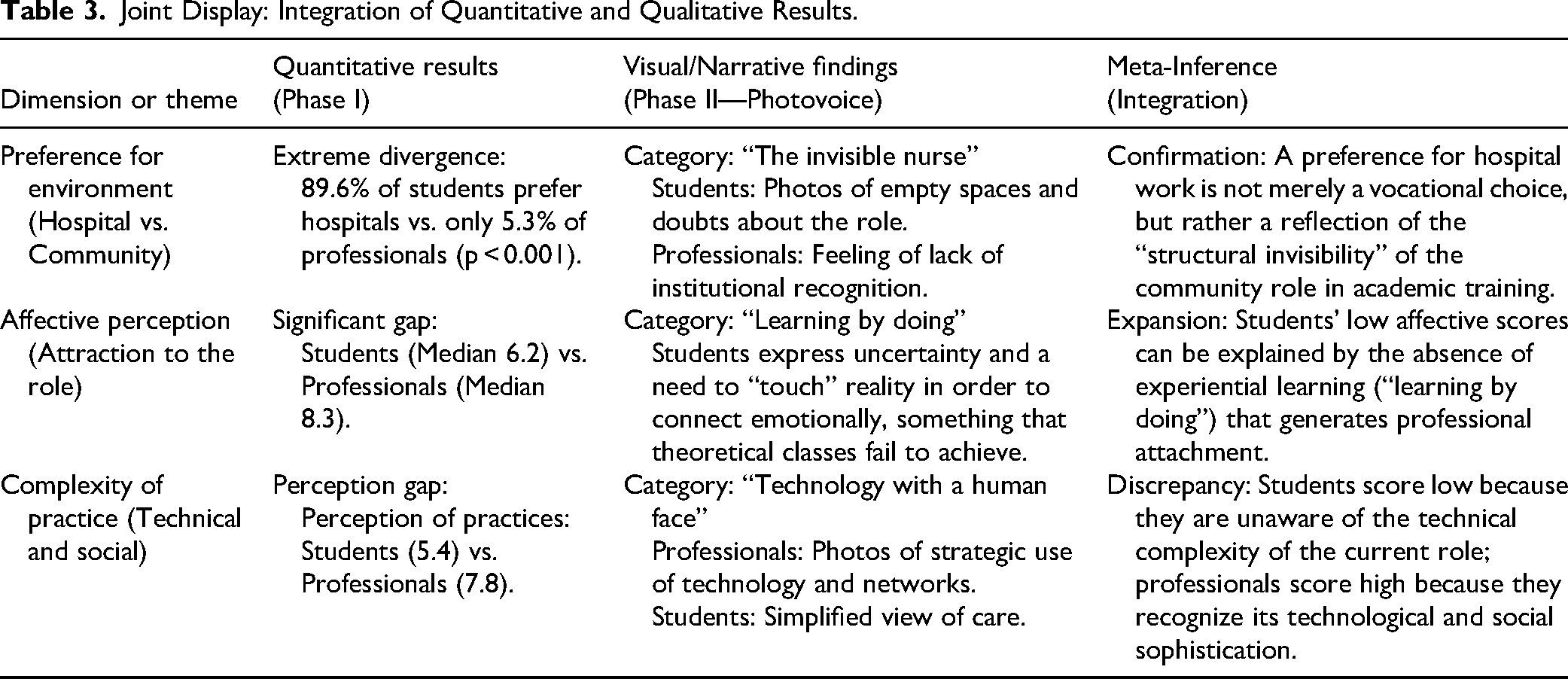
The integration of datasets revealed a clear pattern of “vocational dissonance.” The quantitative preference for hospital placements (89.6%) converged with the qualitative theme of “The invisible nurse,” suggesting that students’ choice was driven by uncertainty rather than disinterest. A significant divergence emerged regarding the complexity of the role: while students recognized the theoretical importance of community nursing, their Photovoice narratives revealed a superficial understanding, failing to capture the strategic and technological dimensions (‘Technology with a human face’) that professionals identified as central to their identity. This gap explained the discrepancy in the SCOPE “Perception of Practices” domain, where students scored significantly lower than professionals.
Discussion
This research revealed a substantial divergence in the construction of perceptions about CN between first-year students and practicing professionals. This gap transcends mere knowledge deficits; it affects the deep understanding of the role, vocational motivation, and the symbolic articulation of the community in the professional imagination. The findings suggest a systemic failure in the “anticipatory socialization” process for the community specialty. This confirms that professional identity development is hindered when students lack visible role models and symbolic anchors—such as specialized technology or clearly defined clinical hierarchies—which are ubiquitous in hospital settings but less tangible in community care.
Disrupted Anticipatory Socialization: The Gap in Professional Expectations
Quantitatively, the significant disparities in SCOPE scores—particularly in affective perception (Student Median: 6.2 vs. Professional: 8.3) and location preferences (4.1 vs. 6.1)—pointed to a deep-seated disconnection. While students theoretically valued the principles of public health, this valuation did not translate into a desire to practice in that setting. This disconnection reflects what PIF theory describes as “role ambiguity.” Unlike the hospital setting, which offers students clear, reinforced symbols of competence and status (Ten Hoeve et al., 2014), the community setting lacks these visible anchors in the undergraduate imagination.
Critically, this suggests that the “hidden curriculum” in nursing education continues to privilege acute care as the normative standard of practice. The low scores in “perception of practices” among students (5.4) indicate that, in the absence of experiential exposure, students fill the void with stereotypes rather than evidence. Consequently, they rely on abstract constructs rather than “experiential knowledge,” leading to the “vocational dissonance” identified in the integrated results. This echoes previous observations of hospital-centric (Van Iersel, Latour et al., 2018), but this data goes further by pinpointing the affective domain as the critical point of failure: students respect the role intellectually but do not feel emotionally connected to it.
Professional Identity Formation and the Lack of Symbolic Anchors
The qualitative phase, articulated through Photovoice, allowed for transcending the mere description of this ambivalence to approximate its symbolic roots. While previous survey-based studies have effectively quantified the low preference for community nursing (Van Iersel, Latour et al., 2018), this visual approach provides a phenomenological understanding of the latent causes of this gap. The visual metaphor of “empty classrooms” and “invisible nurses” serves as a powerful indictment of current pedagogical models. It suggests that student disconnection is not merely a passive lack of interest, but an active response to an educational environment that renders the community invisible.
Moreover, the contrast between student and professional discourses challenges the pervasive stereotype of community nursing as “low-tech” or “slow-paced.” Professionals in this study constructed an identity based on “Technology with a human face” and “Socializing agents,” revealing a complex, high-autonomy practice that contradicts the student view of CN as a subordinate or “retirement” role. This finding is crucial: it demonstrates that the “high-tech” allure of the hospital is based on a narrow definition of technology. By failing to showcase the complex relational and management technologies used in Primary Care, universities are inadvertently devaluing the specialty's epistemic authority. Consistent with Andina-Díaz et al. (2024), the use of Photovoice acted not just as a method, but as a critical intervention, forcing participants to confront and articulate these tacit biases.
Students’ limited exposure restricts their understanding of the community role to an abstract, subordinate figure. International research suggests that early, mentored experiences in real community projects catalyze vocational interest, highlighting the need for immersive pedagogies to challenge hospital-centric training (Buse et al., 2022; Mann et al., 2023).
In contrast, professionals displayed a consolidated identity forged in practice. Their discourses integrated clinical and social aspects, depicting nursing as an intersectoral and emotionally committed profession. Emerging categories like “Technology with a human face” and “Socializing agent” reveal a contemporary reinterpretation of the role, challenging student stereotypes of “outdated care” and broadening the horizon beyond the technical–clinical model. Similarly, “Caring as a team” emerged as a critical buffer against burnout.
Vocational Dissonance: Barriers to Internalizing the Community Role
Integrating these findings reveals a “vocational dissonance” that poses a structural threat to the healthcare system. The paradox is stark: while Spain's National Health System is founded on strong Primary Care, the academic and professional socialization of nurses remains aggressively hospital-centric. The low intention of students to specialize in PC (22.9%) despite valuing its social impact suggests that the “perception gap” is actually a “prestige gap.”
Beyond the training dimension, this study's findings reveal a structural invisibility of the role of the community nurse, both in the professional imagination and in organizational recognition. The qualitative category “The invisible nurse” illustrated this situation through images of impersonal spaces, reflecting the sense of anonymity that accompanies community work and the lack of representation in the media or institutional decision-making processes, despite their key roles in prevention, health promotion and intersectoral coordination. This perception is not anecdotal, but a constant documented in multiple healthcare contexts (Chee et al., 2024; Yoong et al., 2022). Furthermore, this invisibility is intertwined with precarious working conditions—such as lack of stability, overload, and excessive bureaucratization—which hinder retention and increase the risk of burnout (Halcomb et al., 2018). The low intention of students to specialize in PC (22.9%) and their clear preference for the hospital environment (89.6%) should not be interpreted as disinterest per se, but rather as the result of professional socialization that privileges the hospital as a model of clinical excellence, relegating the community to a secondary operational role that is poorly defined and has little symbolic weight. This trend has also been described in European studies (Van Iersel et al., 2016).
The central paradox that emerges is revealing: while primary care is recognized in institutional and academic discourse as the backbone of the healthcare system due to its decisive, preventive and community-based nature, its representation in training and the professional imagination remains marginal. This tension is empirically supported by students’ low preference for primary care as a training environment (only 10.4% chose this environment) and a low intention to specialize in it in the future (22.9%), despite valuing its social impact. This contradiction reflects a training logic that, by prioritizing hospital teaching as a benchmark of technical excellence, reproduces healthcare hierarchies that disadvantage the community. As the professionals’ discourses show, it is in actual practice—not at university—that community practice acquires meaning, agency, and legitimacy.
Ultimately, this dissonance acts as a barrier to internalizing the community role. If professional identity is formed through the integration of personal values and social validation (Cruess et al., 2014), the current system fails to provide the latter for community nurses. Addressing this requires more than curricular tweaks; it demands a re-engineering of how the “symbolic status” of Primary Care is projected during the formative years.
Future Research Directions
Regarding future inquiry, this study identified critical theoretical and methodological gaps. First, to understand the temporal evolution of “anticipatory socialization,” research must move beyond cross-sectional comparisons to longitudinal designs that track professional identity from university entry to clinical integration. Second, methodologically, this study proposed testing “Photovoice-mediated” clinical immersions as experimental interventions to determine if visual engagement can successfully generate the “symbolic anchors” currently missing in undergraduate training. Finally, replicating this mixed-methods design across different health systems would help distinguish between cultural specificities and systemic trends in the devaluation of community care.
Strengths and Limitations of the Study
From a methodological perspective, this study contributes a significant innovation to nursing education research in the Spanish context. The implementation of the “follow-the-thread” technique constitutes a central strength, as it allowed for a continuous analytical line from statistical data (the what) to visual evidence (the why). Unlike approaches that present qualitative and quantitative results in silos, this integration strategy forced the “weaving” of SCOPE findings with Photovoice narratives through joint displays. This ensured that final inferences, such as the paradox of institutional invisibility, were not mere juxtapositions of data, but robust meta-inferences validated across methods.
Another major strength lies in the explanatory sequential mixed-methods design. Unlike purely verbal techniques, the incorporation of Photovoice facilitated what Glaw et al. (2017) describe as access to “deep layers of meaning.” By using photography as an anchor for dialogue (visual elicitation), participants were able to communicate dimensions of “professional invisibility” that often remain hidden in traditional focus groups due to narrative saturation or social desirability. This triangulation not only validated the quantitative SCOPE data but enriched the interpretation of statistical discrepancies, confirming that visual methods are superior for exploring complex subjective phenomena in health settings (Wang & Burris, 1997).
However, the study also has significant limitations. First, the non-probabilistic and intentional sampling, limited to a single teaching unit and a small number of professionals, restricts the generalization of the results to other institutions or regions with different characteristics. Furthermore, the transferability of findings to other international contexts must be interpreted considering cultural and curricular differences. While hospital hegemony in nursing education is a global phenomenon, the perception of community nursing may vary substantially depending on the healthcare model. In nations with fragmented or insurance-based systems, the “institutional invisibility” of the community role might be exacerbated differently than in the present study, which is set within a National Health System with a strong historical orientation toward primary care. Conversely, in developing nations or resource-limited settings—where community nurses often assume more visible and autonomous clinical leadership by necessity—the perceptual gap among students might be narrower. Therefore, although the pattern of “vocational dissonance” identified here resonates with Western literature, its intensity may be modulated by the local curricular structure and the social status of public health in each region.
Second, voluntary participation in the qualitative phase may have introduced a self-selection bias toward more motivated profiles or those with more defined positions on the subject. Likewise, the presence of a researcher moderating the groups may have influenced the discursive dynamics, especially in the case of the students, potentially inhibiting the expression of more critical or emotionally vulnerable opinions. Finally, the limited representation of students in advanced courses restricts the possibility of establishing evolutionary inferences about the progression of perceptions toward community nursing throughout the degree program. Although exposure to this field tends to increase in higher-level courses, this study was unable to capture this longitudinal evolution. Despite these limitations, the robust methodological design and analytical depth give this study significant value for understanding the barriers and opportunities in community nursing education.
Implications for Practice and Recommendations
From an interpretive standpoint, the data indicates that the “hospital-centric” bias is less a rejection of community values than a symptom of educational disconnection, with profound implications for workforce sustainability. If the curriculum continues to present community nursing as a theoretical abstraction without the “experiential anchors” mandated by experiential learning theory (Kolb, 1984), recruitment for primary care will remain critical (Halcomb et al., 2018). Consequently, addressing this gap requires a multi-pronged approach that moves beyond traditional lecturing. It is recommended a curricular shift toward “service-learning” models that place first-year students in community centers to foster affective bonding (Yoong et al., 2022), alongside the integration of visual pedagogies like Photovoice to deconstruct stereotypes and make the “invisible” role visible before clinical rotations begin (Andina-Díaz et al., 2024).
However, educational efforts should be complemented by structural management strategies. Workforce sustainability benefits from addressing the organizational environment to mitigate “structural invisibility.” It is recommended that healthcare leaders foster supportive conditions in primary care—such as improving stability, streamlining administrative tasks, and recognizing nurse leadership in intersectoral coordination. Enhancing the symbolic status of the role within the health system is crucial to support educational interventions in balancing the current hospital-centric focus.
Regarding future research, this study identifies key areas for further inquiry. First, to understand the temporal evolution of “anticipatory socialization,” longitudinal designs tracking professional identity from university entry to clinical integration would offer valuable insights beyond cross-sectional comparisons. Second, replicating this mixed-methods design across different health systems would help distinguish between cultural specificities and systemic trends. Finally, intervention studies testing early “Photovoice-mediated” clinical immersions could provide empirical evidence for the curricular reforms proposed here.
Conclusions
This study moves beyond identifying a preference gap to exposing a systemic “vocational dissonance” that threatens the sustainability of primary care nursing. The findings challenge the assumption that theoretical knowledge is sufficient for professional identity formation; rather, they demonstrate that “symbolic visibility” and “experiential anchors” are non-negotiable prerequisites for anticipatory socialization.
Theoretically, this work extends the PIF framework by identifying “affective disconnection”—not cognitive deficit—as the primary barrier to community nursing specialization. Methodologically, the mixed-methods integration was decisive: while quantitative data confirmed the hospital-centric bias, only the visual narrative revealed its root cause, the structural invisibility of the role.
For nursing education and policy, the implication is clear: recruitment strategies that rely solely on informational campaigns will fail. Reversing the workforce crisis requires a dual approach: pedagogical interventions that provide early, high-visibility immersion in community settings, and organizational reforms that elevate the prestige and professional autonomy of the community nurse. Without restoring the symbolic status of the profession, the health system risks perpetuating a cycle of invisibility that alienates its future workforce.
Footnotes
Acknowledgments
The authors would like to thank all participants in this study for their cooperation and assistance.
Ethical Approval and Informed Consent Statements
The study was conducted in accordance with the Declaration of Helsinki. In accordance with current local regulations, the study was approved by the IRB of the Nursing Management of the Vigo Health Area (with code 137-10-24). Given that this is a qualitative research study with a special focus on the perceptions of the participants, special emphasis has been placed on ensuring their voluntary participation, anonymity and confidentiality, and written informed consent was obtained from all subjects involved in the study.
Author Contributions
Paz Muñoz Vidal: conceptualization, methodology, formal analysis, investigation, writing‒original draft preparation, and writing‒review and editing.
Macarena Chacón-Docampo: conceptualization, methodology, investigation, and writing‒review and editing.
Luis-Javier Márquez-Álvarez: writing‒original draft preparation, and writing‒review and editing.
Ana Isabel González Silva: writing‒review and editing, and supervision.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data presented in this study are available on request from the corresponding author due to participant's privacy.