
Abstract
Background
Plastic overconsumption and improper disposal pose growing threats to human health and environmental sustainability. Children are particularly vulnerable to plastic-related exposures, while mothers, strongly influence household consumption and waste management behaviors. Although nurse-led education effectively enhances health literacy, its potential to promote family-based sustainability practices remains underexplored.
Objective
To evaluate the effectiveness of a nursing-led, family-centered educational program in improving mothers’ and children's knowledge, attitudes, and practices regarding safe plastic use and recycling.
Methods
A quasi-experimental pretest–posttest study was conducted at X University Children's Hospital, Egypt, from March to August 2024. A total of 200 participants (100 mothers and 100 school-aged children aged 6–12 years) were recruited using simple random sampling. The intervention included two structured educational sessions delivered through lectures, group discussions, visual materials, and booklets. Five validated tools assessed outcomes: mothers’ demographic and knowledge questionnaire, mothers’ attitude scale, mothers’ practices checklist, children's recycling knowledge questionnaire, and children's recycling attitudes scale. Data were analyzed using IBM SPSS version 26. Statistical tests included McNemar, chi-square, and correlation analyses, with significance set at p < .05.
Results
Significant improvements were observed post-intervention. Mothers’ knowledge increased from 43% to 82%, attitudes from 58% to 91%, and practices from 54% to 88% (p = .001). Children's recycling knowledge improved from 34% to 89%, and attitudes from 33% to 82% (p = .001). Mothers’ education, residence, and occupation were positively associated with knowledge and practices (p < .05). Children's age and educational level correlated positively with knowledge (p = .010). Post-intervention findings indicated strong interrelationships among knowledge, attitudes, and practices.
Conclusion
Nurse-led, family-centered educational programs effectively foster sustainable household behaviors and reduce environmental health risks. Integrating sustainability education into school health services and community-based nursing initiatives may strengthen long-term behavioral change and contribute to broader public health and environmental sustainability goals.
Keywords
Introduction
Plastic has become inseparable from modern life due to its versatility, affordability, and extensive applications in packaging, storage, and daily household activities. Global production now exceeds 300 million tons annually, with nearly half manufactured for single use, thereby generating unprecedented levels of waste (Kumar et al., 2021). This overreliance on plastics is not merely an environmental concern but also a significant public health threat. Chemical additives leaching from plastic containers and bottles have been detected in human blood and tissue, with evidence linking exposure to cancer, reproductive anomalies, birth defects, and endocrine disruption (Mahmoud et al., 2023; Poojar et al., 2017).
The magnitude of this crisis is alarming. The World Health Organization estimates that plastics account for 10% of global waste generation (Dokl et al., 2024).Within the Mediterranean region, Egypt is the largest contributor, producing nearly 250,000 tons annually. These figures underscore the urgent need for interventions that are locally relevant yet globally significant, particularly in regions with high plastic dependency and limited waste management systems (Râpă et al., 2024).
Children constitute a particularly vulnerable group, as their early and repeated exposure to plastics amplifies lifelong risks. Persistent organic pollutants from plastics remain in the environment for decades, bioaccumulating in ecosystems and entering the human food chain (Lalrinfela et al., 2024). While the complete elimination of plastics is unrealistic, behavioral modification through awareness and safer practices offers a pragmatic pathway to mitigation (Ahmed, El-Kader et al., 2023). Critically, the formation of sustainable habits in childhood has been shown to predict environmental responsibility in adulthood (Kibria et al., 2023; Oludoye & Supakata, 2024).
Review of Literature
The growing concern about plastics is closely aligned with global Sustainable Development Goals (SDGs) (Mohamed et al., 2024), particularly SDG 3 (Good Health and Well-being), SDG 12 (Responsible Consumption and Production), and SDG 13 (Climate Action) (Ahmed, Abdulqadir et al., 2023). Addressing plastic use is not only about waste reduction but also about preventing disease, reducing toxic exposures, and protecting ecosystems (de Sousa, 2021; Stoett et al., 2024). Despite international efforts, recycling rates remain low, and awareness campaigns often fail to reach households where plastic use is most embedded in daily routines (Mohamed, Goktas et al., 2025). This highlights a critical implementation gap between global sustainability targets and individual or family-level practices (Ferronato et al., 2024; Islam et al., 2025).
Households and particularly mothers as primary caregivers play a decisive role in shaping children's daily habits and long-term behaviors (Ahmed et al., 2024). Evidence suggests that when environmental education is embedded within family routines, the likelihood of sustained behavior change increases (Luby et al., 2022). Mothers often influence decisions about food storage, water use, and waste disposal, making them powerful agents of sustainability within the home (Mohamed, Al-Yafeai et al., 2025). Targeting both mothers and children simultaneously creates a synergistic effect, where parental modeling reinforces children's learning, and children, in turn, influence family behaviors through peer-style advocacy within the household (Sihvonen et al., 2024).
Even with the recognized importance of environmental health, most interventions have been school-based or policy-driven, with limited attention to nurse-led family education (Sorour et al., 2026). Nurses are uniquely positioned at the intersection of health promotion, community trust, and environmental advocacy (Francis et al., 2025). They function not only as clinicians but also as educators, role models, and change agents, capable of translating complex sustainability concepts into actionable household practices (McKinnon et al., 2022). The American Nurses Association emphasizes environmental health as a professional responsibility, aligning nursing with global sustainability movements (Ahmed, Dabou et al., 2023). However, the potential of nurse-led interventions to promote recycling and safe plastic use among families remains largely underexplored in both research and practice (Moghbeli et al., 2024).
This study addresses that gap by developing and testing a nursing-led educational intervention designed to empower mothers and children to adopt safer plastic use and recycling behaviors. Unlike previous programs that have focused narrowly on school curricula or community campaigns, this intervention is family-centered and intergenerational, simultaneously equipping mothers with environmental health literacy while engaging children in participatory, hands-on learning. This dual-targeted approach ensures that knowledge transfer is reinforced at both caregiver and child levels, maximizing sustainability of behavior change. This innovative model advances an urgently needed paradigm shift: from individual awareness campaigns toward nurse-led, family-embedded interventions that strengthen resilience against environmental hazards while cultivating sustainable lifestyles from early childhood.
Study Objective
This study aimed to evaluate a nursing-led, family-centered educational program designed to improve mothers’ and children's knowledge, attitudes, and practices on safe plastic use and recycling. By engaging both generations, the intervention sought to foster sustainable household behaviors, reduce environmental health risks, and position nurses as key drivers of family-based sustainability in the Middle Eastern context.
Methods
Study Design
This study employed a quasi-experimental pretest–posttest design to evaluate the effectiveness of a nursing-led educational program on improving mothers’ and children's knowledge, attitudes, and practices related to safe plastic use and recycling. The design was selected to capture changes within the same participants before and after the intervention, thereby minimizing intergroup variability and allowing direct measurement of program impact.
Setting and Participants
The research was conducted in both inpatient and outpatient pediatric facilities at X University Children's Hospital, Egypt. Data were collected from the emergency unit, rehydration unit, medical wards, and outpatient clinics, where both mothers and their school-aged children were accessible.
A total of 100 mothers and their school-aged children (6–12 years old) participated in the study. Recruitment was performed using a simple random sampling method with a computer-generated list, where most of the participating mothers were housewives. To better understand the sources of information regarding the safe use of disposable plastic containers, data on the socioeconomic context of the area were considered, including access to the internet, availability and use of information technology, and engagement with social media. These factors were essential to interpret how mothers obtained knowledge and to guide the development of targeted nursing-led interventions for improving safe plastic use and recycling behaviors.
The inclusion criteria for the study required that mothers be willing to participate, that children fall within the age range of 6–12 years, and that both mothers and children be able to attend the two educational sessions and complete the pre- and post-assessments. Exclusion criteria were applied to families who were unwilling to participate and to children who were outside the specified age range. These criteria ensured that the study population was consistent and able to fully engage with the intervention and data collection process.
The sample size was determined using G*Power 3.1.9.7 (Heinrich-Heine-Universität Düsseldorf, Düsseldorf, Germany), informed by a pilot study. Based on an F-test with fixed effects, an effect size of f = 0.55, a significance level of α = 0.05, and a power of 0.95, the minimum required sample size was calculated as 60 participants per group. To enhance the study's statistical robustness and account for potential attrition, a total of 200 participants were recruited, comprising 100 mothers and 100 children. This sample size ensured sufficient power to detect statistically significant differences between pre- and post-intervention scores.
Intervention Procedure
The study was conducted over four phases from March 1 to August 30, 2024, each carefully structured to ensure methodological rigor and participant engagement (Figure 1).

Research flow chart: phases and procedures of the plastic hazards and recycling education study.
Preparatory Phase
The preparatory phase involved a comprehensive review of relevant literature and the development of the study protocol and data collection instruments. This included identifying the necessary socio-demographic information for participating mothers and children, adopting validated measures to assess mothers’ knowledge, attitudes, and practices regarding plastic container use, and adapting child-specific measures to evaluate knowledge and attitudes toward recycling habits.
The face validity of the child-specific measures (Measures IV and V) was evaluated by a committee of five community and pediatric nursing faculty members. The assessment focused on acceptability, clarity, length, design, wording, and overall appearance. Following approval, official permission for data collection was obtained from the manager of X University Children Hospital.
A pilot study was conducted prior to data collection with 10% of the total sample (10 mothers and their children) to assess the clarity, feasibility, and time required for data collection using the study instruments. The pilot participants were subsequently included in the main study, as no major modifications to the tools were necessary.
Assessment Phase
The assessment phase, conducted during March 2024, involved preparation of the nursing-led educational program. The program content was evidence-based, drawing on nursing textbooks, peer-reviewed journals, and verified online resources, covering safe plastic container use and sustainable recycling practices. Educational materials were presented in simple Arabic and included booklets with colourful illustrations, symbols, and supplementary videos.
Application Phase
The intervention phase spanned four months (April 1–July 31, 2024). During the first two months, participants completed baseline assessments. The following two months were dedicated to delivering the educational intervention to both mothers and children. Participants were organized into small groups of four mothers and their children. Researchers were assigned specific roles: some administered assessments to mothers, while others conducted educational sessions for children.
Mothers attended two 20-min sessions in seminar rooms located in emergency, medical, and rehydration units, as well as a teaching room near outpatient clinics, during regular clinic hours (9:00 AM–1:00 PM). Sessions included:
Session One: Pretest administration and discussion on the health hazards of plastic containers, identification of safe versus unsafe types, and interpretation of plastic symbols, reinforced through visual aids and group discussion. Session Two: Focused on practical strategies for safe plastic container use, with repeated reinforcement and distribution of a comprehensive educational booklet.
Group Two—Children's Education:
Children received two 20-min educational sessions in the same clinical settings, utilizing lectures, group discussions, videos, and visual aids:
Session One: Pretest assessment, introduction to recycling concepts, and identification of recyclable materials. Session Two: Promotion of positive recycling attitudes and creative reuse practices, reinforced with interactive visual materials. Each child received a colorful booklet with illustrations and symbols.
Appraisal Phase
The impact of the program was evaluated within two weeks following the completion of the intervention (August 2024). Evaluations were conducted via face-to-face interviews for inpatient participants, lasting approximately 20 min. Outpatient participants and those discharged were assessed through structured mobile phone interviews.
Quality Monitoring
To ensure data integrity, all collected measures including mothers’ knowledge, attitudes, reported practices, and children's recycling knowledge and attitudes were verified and cross-checked. Additionally, 10% of the questionnaires were randomly selected for detailed review as a quality control measure.
Instruments
Five measures were utilized to achieve the objective of this study.
Measure I: Demographic Characteristics and Knowledge of Mothers
This tool, adapted from El-Sayed et al. (2019), comprised two sections. The first section assessed socio-demographic characteristics, including the child's and mother's age, place of residence, mother's educational level, and occupation. The second section evaluated mothers’ knowledge regarding the hazards of plastic containers on children's health and the identification of safe versus unsafe types of plastics, including the recycling numbers commonly found on disposable containers. The knowledge assessment consisted of 23 items. Each correct response was scored 1 point, while incorrect or “don’t know” responses were scored 0. The total possible score was 21 points. Mothers scoring below 60% (fewer than 12 points) were classified as having unsatisfactory knowledge, whereas those scoring 60% or higher were considered to have satisfactory knowledge. The instrument demonstrated strong psychometric properties, with a content validity index (CVI) of 0.97 and a Cronbach's alpha of 0.812.
Measure II: Attitudes of Mothers
Also adapted from El-Sayed et al. (2019), this measure assessed mothers’ attitudes regarding the hazards of plastic containers (5 items), the use of plastic containers (11 items), and the use of plastic substitutes (3 items), for a total of 19 items. Responses were captured on a three-point Likert scale (agree = 3, uncertain = 2, disagree = 1). There were no negatively worded items. Total scores ranged from 19 to 57 points, with scores of 60% or higher classified as indicative of a positive attitude, and scores below 60% as a negative attitude. The measure demonstrated excellent validity and reliability, with a CVI of 0.96 and a Cronbach's alpha of 0.851.
Measure III: Practices of Mothers Regarding Plastic Container Use
This measure, adapted from El-Sayed et al. (2019), assessed mothers’ practices in using plastic containers through 10 items, including behaviors such as checking recycling symbols and reusing natural water bottles. Each item was scored dichotomously as “done” (1 point) or “not done” (0 points), with total scores ranging from 0 to 10. Scores below 60% (less than 6 points) indicated improper practices, whereas scores of 60% or higher indicated proper practices. The instrument demonstrated strong psychometric properties, with a CVI of 0.97 and a Cronbach's alpha of 0.701.
The practices assessed were a mix of proper and improper practices. Proper practices, for which participants received a point, included proactively checking the bottom of a plastic container for safety symbols before purchase, replacing an infant's feeding bottle or formula if it showed signs of degradation like a change in color or smell, and making a habit of identifying safe plastic symbols on food containers.
Conversely, the measure also identified several improper practices. Participants were penalized (score of 0) for engaging in these risky practices, which included: purchasing unsafe plastic containers solely due to their low cost; buying any plastic container or baby bottle that lacked a safety symbol; storing food in non-certified plastic containers in the refrigerator; placing hot food directly into unmarked plastic containers, which can accelerate chemical leaching; reusing single-use mineral water bottles; and buying plastic colored toys that did not have a safety symbol. Engaging in these practices reflects a lack of awareness regarding the potential health risks associated with chemical leaching from plastics.
Measure IV: Children's Recycling Knowledge Questionnaire
Adapted from Buil et al. (2019) and Decharat and Kiddee (2022), this questionnaire assessed children's knowledge about recycling. It consisted of two parts: socio-demographic information (child's name, age, sex, educational level) and knowledge about recycling (48 items covering the meaning of recycling, frequency, and types of materials recycled). Each correct answer was scored 1 point, and incorrect responses received 0 points. Total scores ranged from 0 to 48, with scores below 60% (less than 29 points) indicating unsatisfactory knowledge, and scores of 60% or higher indicating satisfactory knowledge. This measure demonstrated strong validity and reliability (CVI = 0.95, Cronbach's alpha = 0.719).
Measure V: Children's Attitudes Toward Recycling
This tool, also adapted from Buil et al. (2019) and Decharat and Kiddee (2022), comprised 21 items across four domains: children's opinions on recycling, knowledge about recyclable materials, ideas to facilitate recycling, and creative uses of recycled materials, illustrated with five images (A–E). Responses were recorded on a five-point Likert scale (strongly agree = 5 to strongly disagree = 1). Total scores ranged from 21 to 105 points, with scores of 60% (≥62 points) or higher indicating a positive attitude, and scores below 60% indicating a negative attitude. The measure demonstrated strong psychometric properties, with a CVI of 0.95 and a Cronbach's alpha of 0.719.
Data Analysis
The collected data were systematically organized, coded, and tabulated for analysis using IBM SPSS Statistics version 26. Descriptive statistics, including frequencies, percentages, means, and standard deviations, were used to summarize participants’ sociodemographic characteristics and study variables. For the pretest–posttest comparison, the McNemar test was applied to examine changes in categorical variables, while Pearson's chi-square test assessed associations between categorical variables at each time point. Statistical significance was set at p < .05. Data were presented in tables and figures to clearly illustrate changes in knowledge, attitudes, and practices following the intervention.
Results
Participant Characteristics
Table 1 presents the baseline characteristics of the studied mothers and children. More than half of the mothers (51.0%) were aged between 25 and less than 30 years. Additionally, 66.0% of the mothers resided in rural areas, and 38.0% had attained a secondary level of education. The majority of mothers (73.0%) were housewives, and 64.0% had three or more children. Regarding prior knowledge about the hazards and safe use of disposable plastic containers, 54.0% of the mothers reported that their primary source of information was relatives. As for the children, 75.0% were aged 10 years or older, and 61.0% were female. Moreover, 82.0% of the children were enrolled in grades 4 to 6 of primary school.
Sociodemographic Characteristics of Participating Mothers and Their Children (n = 200).

Pre- and Post-intervention
The results of Table 2 show a significant improvement in mothers’ total knowledge and practice levels regarding the hazards and safe use of disposable plastic containers after the educational intervention. The percentage of mothers with satisfactory knowledge increased from 43.0% in the pretest to 82.0% in the posttest. Similarly, proper practices improved from 54.0% before the intervention to 88.0% afterward. Both changes were statistically significant, with p-values of .001.
Pretest and Posttest Assessment of Mothers’ Knowledge and Practices on Disposable Plastic Container Hazards (n = 100).
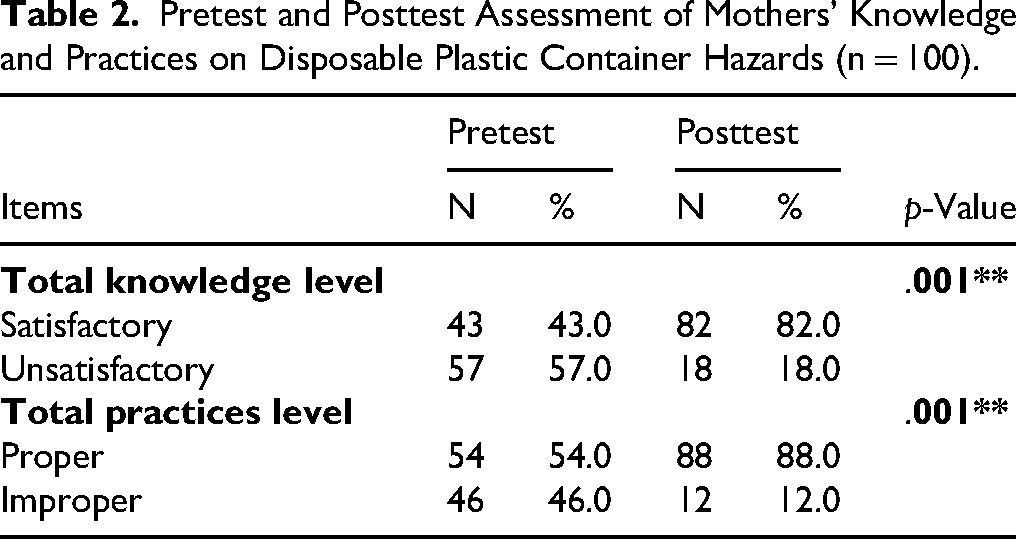
Figure 2 illustrates that there were highly statistically significant differences in pretest and posttest regarding total mothers’ attitudes toward disposable plastic containers hazards and safe use (p-value = .001). There was a significant increase in positive attitude from pretest (58%) to posttest (91%), and a corresponding decrease in negative attitude from 42% to 9%.

Mothers’ attitudes toward disposable plastic container hazards and safe use (n = 100).
Figure 3 demonstrates that there was a marked increase in the satisfactory knowledge, from 34% in the pretest to 89% in the posttest, and a corresponding decrease in unsatisfactory knowledge, from 66% to 11% with p-value = .001.
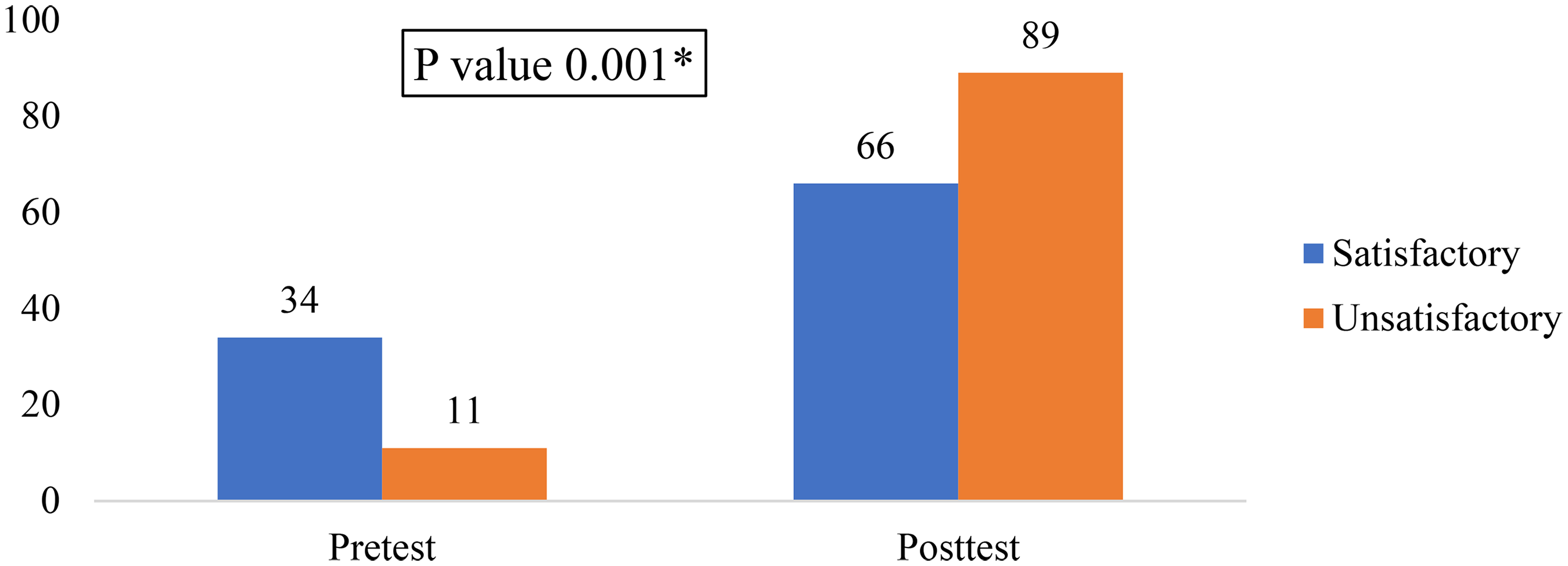
Pretest and posttest assessment of children's knowledge regarding recycling of disposable plastic containers (n = 100).
Figure 4 shows that positive responses increased from 33% to 82%, while negative responses decreased from 67% to 18%. This change is highly significant (p = .001).

Pretest and posttest assessment of children's attitudes regarding recycling of disposable plastic containers (n = 100).
Table 3 revealed that mothers’ education showed the strongest positive correlations with total knowledge (r = .481, p < .001), practice (r = .271, p = .006), and attitude (r = .229, p = .022). Residence and occupation were also significantly related to knowledge (r = .279, p = .005; r = .384, p < .001) and practice (r = .223, p = .026; r = .247, p = .013). Age correlated positively with practice (r = .306, p = .002) and marginally with attitude (r = .196, p = .050). Number of children showed no significant correlation. Pretest knowledge correlated with practice (r = .347, p < .001) and attitude (r = .306, p = .002), highlighting the influence of baseline levels on outcomes.
Correlations Between Mothers’ Sociodemographic Characteristics and Their Knowledge, Practices, and Attitudes in the Pretest (n = 100).

Pearson test; (*) statistical significant difference; (**) highly statistical significant difference.
Table 4 represents the relationship between age and total attitude is not statistically significant (R = .172, p = .088). Similarly, sex is significantly correlated with total knowledge (R = .238, p = .017). However, there is no significant correlation between sex and attitude (R = .136, p = .176). Lastly, child's education shows a significant positive correlation with total knowledge (R = .258, p = .010). The correlation between education and attitude is not significant (R = .106, p = .294).
Correlations Between Children's Personal Characteristics and Their Knowledge and Attitudes in the Pretest (n = 100).

Pearson test; (*) statistical significant difference; (**) highly statistical significant difference.
Table 5 shows a significant positive correlation between mothers’ total knowledge in the pretest and their total knowledge posttest (r = .476, p = .000) and total attitude (r = .210, p = .036). Similarly, total practices in the pretest are significantly correlated with both total knowledge (r = .435, p = .000) and total attitude (r = .353, p = .000). However, total attitude in the pretest shows no significant correlation with total knowledge (r = .105, p = .299) or total attitude (r = .000, p = 1.000).
Correlations Between Children's Knowledge and Attitudes and Mothers’ Knowledge, Practices, and Attitudes in the Pretest (n = 200).

Pearson test; (*) statistical significant difference; (**) highly statistical significant difference.
The educational intervention resulted in a significant strengthening of the correlations between knowledge, attitudes, and practices. At baseline, while strong significant correlations were found between knowledge and attitude (p < .0001, p = .0002, p = .0003), practices were not significantly correlated with the other domains (p = .255, p = .256). Post-intervention, all correlations became highly significant, with practices now strongly linked to both knowledge (p < .0001, p = .0002, p = .0003) and attitudes (p < .0001, p = .0002, p = .0003), indicating the intervention was effective in bridging the know-do gap and translating knowledge and positive attitudes into improved practices (Figure 5).
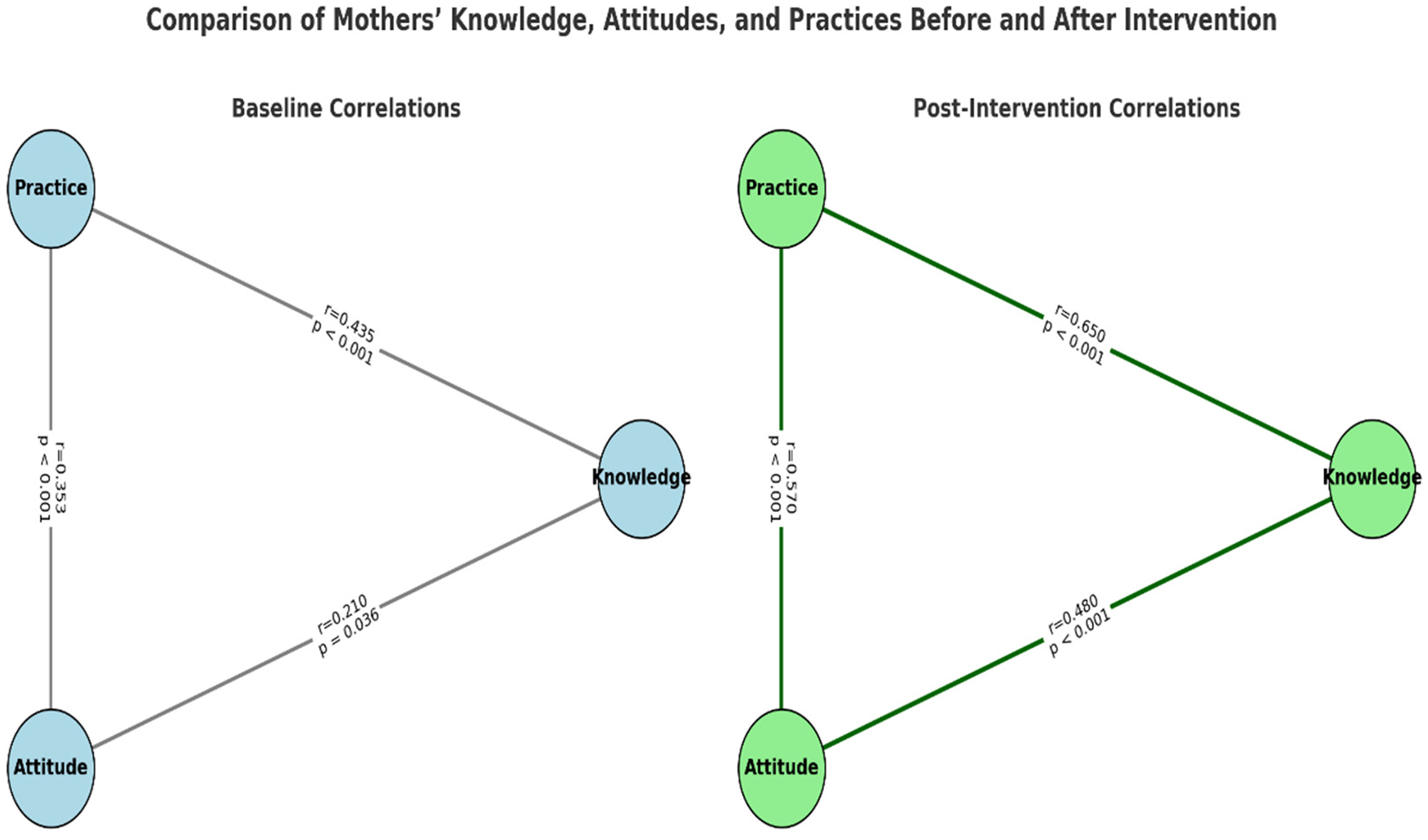
Changes in mothers’ knowledge, attitudes, and practices following the educational intervention.
Discussion
Research shows that we have not fully reached our goals on the path to a sustainable future. Rising inequality, climate change, biodiversity loss, and increasing amounts of waste from human activity continue to be pressing issues. So, there is a need to accelerate actions and successfully convey the message of sustainability to achieve these critical goals. It is increasingly recognized globally that education for sustainable development plays a critical role in creating a more just, peaceful, and sustainable world. To achieve this, individuals and societies need to be equipped with knowledge, skills, and values while developing heightened awareness (Sihvonen et al., 2024).
The present findings support global SDGs notably SDG 3, SDG 12, and SDG 13 by showing that nurse-led eco-education can improve responsible consumption and promote community sustainability. Such programs can be scaled to other regions, positioning nurses as key drivers of health and environmental goals.
The present study showed that more than half of the participating mothers were under 30 years of age, more than two-thirds were from rural areas, and over one-third had a secondary level of education. Additionally, the majority of the mothers were housewives, and more than half reported that their source of knowledge about the hazards and safe use of disposable plastic containers before the intervention came from relatives.
In contrast, the study by El-Sayed et al. (2019) reported that a high percentage of the participating mothers were aged 30 years and above, and about two-thirds were from urban areas. The study also showed that slightly more than half of the mothers were homemakers, and a high percentage reported that their main sources of information about the safe use of plastic containers were the internet and television. The current study also disagrees with the findings of El-Sayed et al. (2019) and Mahmoud et al. (2023), who reported that the internet and television were the main sources of information about the safe use of plastic containers.
This discrepancy may reflect differences in accessibility, content quality, or mothers’ trust in these sources. It suggests that being homemakers may influence mothers’ engagement with information on safe plastic use and highlights the need for tailored educational interventions to ensure accurate and practical guidance reaches them through the channels they use most.
The current study showed that more than half of the mothers had an unsatisfactory level of knowledge, nearly half demonstrated improper practices, and more than two-fifths had a positive attitude toward the hazards and safe use of disposable plastic containers. These findings are consistent with those of by El-Sayed et al. (2019), who reported that the majority of mothers had unsatisfactory knowledge and engaged in improper practices related to the safe use of plastic containers. Moreover, approximately half of the mothers in their study exhibited a negative attitude toward the use of such containers.
The findings indicate a substantial gap in mothers’ knowledge and practices regarding the safe use of disposable plastic containers, despite a considerable proportion having a positive attitude. This suggests that awareness alone may not translate into proper practices. The consistency with El-Sayed et al. (2019) reinforces the need for targeted educational interventions to improve both knowledge and behavior. Health education programs should focus on practical guidance and strategies to correct unsafe practices, particularly for mothers who are primarily responsible for food preparation at home.
The present study showed greater improvements than those reported by El-Sayed et al. (2019). This may be attributed to the nurse-led, interactive, and multimodal design of the program, which used videos and visual materials, compared with more traditional methods in El-Sayed's study. Additionally, the inclusion of both mothers and children may have promoted reciprocal reinforcement at home, amplifying learning. Finally, the predominantly rural sample in this study had lower baseline knowledge, creating greater scope for measurable improvement.
The present study also aligns with the findings of Mahmoud et al. (2023) who study the effect of health educational program about plastic use hazards on knowledge, attitude, and practice among study participants. They observe that, there was a statistically significant improvement in knowledge, attitude, and practices in all items of plastic products usage practices among studied participants before and 3 months after educational intervention as p less than .005. In the same line, the current intervention demonstrated that targeted, nurse-led education can effectively address these gaps, suggesting that inadequate baseline knowledge presents an opportunity for significant improvement when structured educational strategies are applied.
The present study illustrates that there were highly statistically significant differences between the pretest and posttest results regarding total knowledge level, total practice level, and overall maternal attitudes toward the hazards and safe use of disposable plastic containers (p = .001).
The significant improvements in mothers’ knowledge, practices, and attitudes suggest that the intervention program was highly effective. This underscores the importance of structured educational programs in promoting safe behaviors regarding the use of disposable plastic containers. The findings also highlight that when mothers are provided with clear guidance and practical information, they are capable of adopting safer practices and developing more positive attitudes toward health-related hazards.
Similarly, Kaur and Jeganathan (2019) studied knowledge about plastic-related health hazards among 30 participants. At pretest, two-thirds of the participants had poor knowledge, and none had good knowledge. After a structured teaching program, two-fifths had good knowledge, and more than half had average knowledge. They concluded that structured health education programs are effective in increasing participants’ knowledge about the hazards of plastic use.
Furthermore, Upendra et al. (2020), who assess knowledge on Hazards of Plastic Use among Residents of Selected Urban Community of Pune City, found that the majority of respondents have average knowledge (46.75%) and 3.5% respondents had poor knowledge on hazards of plastic use. This may be explained by the fact that urban communities are aware about the significant hazards of plastic use.
The present study also revealed a positive correlation between mothers’ age and total practice. The positive correlation between mothers’ age and total practice suggests that older mothers may have greater experience or awareness that contributes to safer practices regarding disposable plastic containers. Similarly, El-Sayed et al. (2019) reported a significant increase in total knowledge, attitude, and practice scores among mothers as age increased. However, this finding is inconsistent with Al-Khatib et al. (2015), who studied public perception of the hazards associated with municipal solid waste management. They found a significant association between age and knowledge regarding the health hazards of plastic use specifically among students, which may differ due to demographic or contextual factors.
Furthermore, the current study found positive correlations between mothers’ education level and their total knowledge, total practice, and total attitude scores. This aligns with findings by Srinivasan et al. (2019), who reported a significant relationship between respondents’ age, education level, and their knowledge, attitude, and practice concerning plastic usage. Their study also showed that the Knowledge, Attitude, Practice scores of mothers were directly influenced by their educational background.
The current findings also demonstrated a positive correlation between mothers’ total knowledge in the pretest and both total practice and total attitude, as well as between residence and mothers’ occupation with both total knowledge and total practice. These findings are supported by El-Sayed et al. (2019) who reported a highly statistically significant positive correlation between knowledge and both attitude and practice concerning the safe use of plastic containers in both pre- and posttests. Similarly, Srinivasan et al. (2019) confirmed a positive correlation between knowledge and practice, emphasizing that greater knowledge positively influences attitudes.
The significant correlations between mothers’ knowledge and practices and their children's knowledge and attitudes highlight the important role of family dynamics in shaping environmental behavior. This finding supports the concept of intergenerational learning, whereby parents’ attitudes and behaviors serve as influential models for their children. When mothers adopt proper practices and demonstrate awareness of safe plastic use, children are more likely to internalize these values and develop positive environmental attitudes. These results underscore the importance of designing family-centered educational interventions that engage both mothers and children simultaneously. Future programs could build on this relationship by incorporating joint learning activities or home-based assignments that encourage shared responsibility for environmentally safe practices.
The present study also revealed that the majority of children were aged 10 years or older, with more than half being female, and more than three quarters were in 4th to 6th primary grades. This differs from the findings of Aguilar-Jurado et al. (2019), who studied the effects of an educational glass recycling program in Spain and reported that nearly half of the students were girls and more than half were boys. However, both studies align in that the participants were elementary school students aged 6–12 years.
The current study also contrasts with Kaur and Jeganathan (2019), who examined the effectiveness of a structured teaching program on knowledge regarding the health hazards of plastic use among students. Their participants were female students aged 19–20 years, which differs from the age group in the present study. Nonetheless, both studies agree in that the majority of participants came from rural areas, and more than one-third parents had a middle school level of education.
Finally, the present study showed highly statistically significant differences between pretest and posttest results regarding children's knowledge of recycling disposable plastic containers (p = .001), reflecting the positive impact of the educational intervention. This finding aligns with Taghdisi et al. (2016), who studied the impact of education on empowering elementary school students to perform source separation for recycling. They found that, after the intervention, recycling activities significantly increased in the intervention group, with more than two-fifths participating and a statistically significant difference (p < .001) between the test and control groups. Also, study made by Buil et al. (2019) about creating the habit of recycling in early childhood: a sustainable practice in Spain regarding the aim of this study, which was to define and implement a teaching unit on sustainability for early childhood education by focusing on concrete sustainable practices (aluminum packaging recycling), the results allowed the researchers to declare that the activities achieved very positive results, both with the children and with all of the agents who contributed to the program and are very motivated to continue recycling.
Strength and Limitation
The present study demonstrated several strengths, including the effective empowerment of both mothers and children by enhancing their knowledge, practices, and attitudes regarding the safe use of plastic materials, while fostering sustainable recycling habits through a creative and engaging approach. By assessing actual intended behavioral, the study provided valuable insights into how educational interventions influence daily habits, directly supporting global SDGs, particularly SDG 3 (Good Health and Well-Being), SDG 12 (Responsible Consumption and Production), and SDG 13 (Climate Action), by linking health education with environmental sustainability. Moreover, the success of this nurse-led program underscores its potential for scalability, positioning nurses as key agents in advancing both public health and sustainability agendas.
However, several limitations should be noted. First, the study involved a relatively small sample, raising concerns regarding the validity and generalizability of the results. A larger sample size would be necessary to more confidently support the conclusions drawn. Second, the study employed a quasi-experimental design without a control group, limiting the ability to attribute observed improvements solely to the intervention. Important influencing factors, such as socio-economic status, access to recycling facilities, and prior sustainability knowledge, were not fully assessed. Additionally, the reliance on self-reported data may introduce potential bias, including social desirability effects, as participants might have provided responses they perceived as more favorable rather than reflecting their true behaviors or opinions. Moreover, the absence of subgroup analyses restricts a nuanced understanding of how environmental or contextual factors influence behavior change. Future research should examine various demographic and contextual subgroups to identify specific determinants of knowledge, attitudes, and practices. Finally, a longer follow-up period would provide a stronger assessment of the sustainability of behavioral improvements in recycling practices.
Implications for Practice
The outcomes of this intervention signal a high-value opportunity to institutionalize nurse-led educational strategies within community and school-based health programs. Embedding recycling and safe plastic usage education into routine primary care, school health activities, and maternal–child health services may transform environmental awareness into habitual behavior, strengthening both public health outcomes and ecological responsibility.
Frontline nurses are well-positioned to operationalize sustainable behavioral change by integrating health education with environmental stewardship, using tailored learning modules that engage children and caregivers simultaneously. Community outreach platforms—including school classrooms, primary healthcare centers, maternal and child health clinics, universities, and public community spaces provide strategic touchpoints for scalable implementation. Educational materials such as illustrated guides, interactive workshops, booklets, pamphlets, posters, and hands-on recycling demonstrations can reinforce message retention and promote long-term habit formation.
Expanding structured educational programs targeting caregivers and healthcare providers, particularly community and school nurses, can further enhance awareness of safe plastic use and recycling practices. Family-based learning strategies that actively involve both parents and children should be encouraged to foster intergenerational transfer of environmental responsibility and healthy behaviors.
At a policy level, healthcare administrators and decision-makers should consider integrating standardized recycling education curricula into school health frameworks and community-based nursing initiatives. Cross-sector collaboration among health, education, and environmental agencies may accelerate sustainability efforts, enhance community engagement, and support measurable ecological benefits.
Additionally, further research involving larger and more diverse samples of school-aged children is warranted to identify the primary sources through which students acquire recycling knowledge and to examine how these sources influence attitudes toward pro-environmental behaviors and long-term sustainability practices.
Conclusion
The nurse-led educational program effectively empowered mothers and their children to adopt safer practices regarding plastic use and to develop sustainable recycling habits. Statistically significant improvements were observed in mothers’ knowledge, attitudes, and practices following the intervention, demonstrating the program's effectiveness. The initiative also fostered environmentally responsible behaviors among children by enhancing their knowledge and attitudes toward recycling, thereby promoting sustainability within households and the wider community. Additionally, significant correlations were noted between children's age and total practice, as well as between children's education level and total knowledge. Mothers’ residence and age were positively associated with both total knowledge and total practice, highlighting key demographic factors that influence learning outcomes and intended behavioral improvement.
Footnotes
Acknowledgments
The authors wish to thank the participating patient and the administrative support provided by Hospital manager for facilitating data collection.
Ethics Statement
Ethical approval for this study was granted by the hospital ethics committee and the Institutional Nursing Ethics Board under approval number 1120220509. Written informed consent was obtained from mothers, and assent was secured from children aged ≥7 years. Confidentiality and anonymity were maintained throughout the study.
Author Contributions
Amira Hassan Abd-Alfatah contributed to data collection, investigation, and manuscript review. Mona Gamal Mohamed was responsible for methodology, project administration, and manuscript drafting and editing. Safaa R. Osman provided supervision, formal analysis, and critical review of the manuscript. Nahed Abd Elazeem Abd Elsalam contributed clinical input and manuscript review. Nora Abdelhamid Zaki supported methodology development and manuscript validation. Walaa Hassan Abd-Alfatah assisted with data collection, resource management, and manuscript editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.