
Abstract
Introduction
Climate change poses a major threat to the health and well-being of people around the world, especially vulnerable groups such as pregnant women. Nurses need to be actively involved in addressing the health impacts of a changing climate. It is very important to help and take care of people who are pregnant. Knowing about and dealing with how climate change affects towns and pregnant women is extremely important.
Objective
To assess how nurse education modules about climate change affect pregnant women's reported practice and quality of life (QoL).
Method
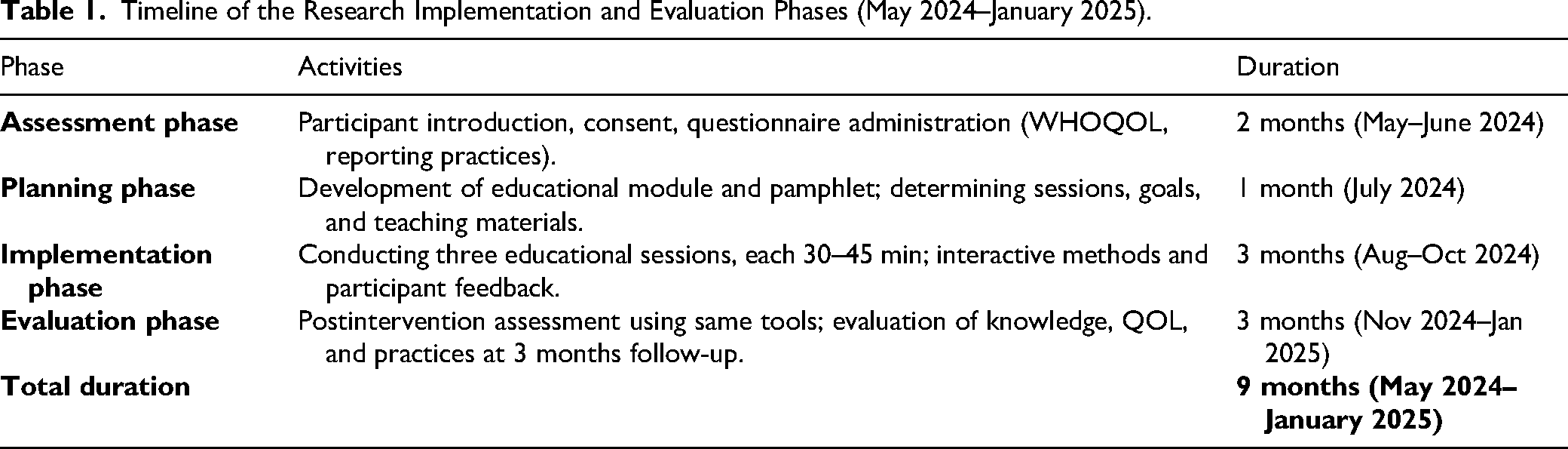
A quasi-experimental (one-group pre–posttest) design was utilized. The obstetrics and gynecological outpatient clinic at Benha University Hospitals served as the study's site, a purposive sample of 128 pregnant women. Four instruments were employed to gather data: tool (a) Structured interviewing questionnaire, tool (b) Maternal knowledge questionnaire, tool (c) Maternal reported practices, and tool (d) World Health Organization QoL. Nurses received structured training prior to implementing the educational modules, the training included orientation on the module content, demonstration of teaching steps and supervised practice to ensure standardization. Nurses’ competency was evaluated using a checklist before applying the modules with participants.
Results
Comparing the postintervention phase to the preintervention phase revealed a highly statistically significant difference in knowledge, QoL, and practices regarding heat stress and climate change (p ≤ .000). The results clarified that, about one third of the studied sample had adequate knowledge regarding climate change and heat stress in the preintervention compared to two-thirds at postintervention phase. The mean score of the overall QoL was increased from 61.91 ± 7.46 prior intervention to 96.42 ± 11.39 postintervention, as well as, the total mean score of reported practices was improved from 41.28 ± 7.27 prior intervention to 63.15 ± 5.24 postintervention. The results confirming the impact of the educational module in improving the studied sample's knowledge, reported practices and QoL regarding climate change and heat stress.
Conclusion
The study showed that the nursing educational module on climate change had a positive effect on pregnant women’ QoL and their reported practices. To maintain these improvements over time, it's recommended to integrate the module into routine nursing training and maternal and maternal care programs. Incorporating this approach in to daily practice could help ensure sustainable benefits and promote healthier outcomes for mother and their babies in the context of environmental changes.
Introduction
In recent decades, climate change has become a major global threat with serious implications for human health. It greatly impacts our surroundings, natural systems, and the health of people, unfairly adding more problems to those who are already at risk, such as older adults, people who are always sick, kids, and women expecting babies, as well as the babies they are carrying (Watts et al., 2019).
Pregnant women are particularly vulnerable to the negative health effects associated with climate change, driven by alterations in human physiology that affect their thermoregulation, cardiovascular function, and immune response. When pregnant women are subjected to extreme heat and harsh outdoor environments, they may face considerable fluid depletion, endure heat-related health issues, and confront a range of medical complications, which could ultimately lead to early delivery, insufficient fetal development, birth defects, or even death. Also, the health of both the mother and her baby might get worse because of worry and strain caused by events related to changes in the climate (Bekkar et al., 2020). Climate change's health repercussions are expected to cause approximately 250,000 fatalities each year between 2030 and 2050. It is thought that as the climate changes, we will see more climate-related events that are both more common and more intense, such as periods of very hot weather, fires in the wild, and severe storms like hurricanes and times of very little rain, which will likely result in problems during pregnancy, such as low iron, babies with low birth weights, eclampsia, births that happen too early, and possibly even the death of the baby (Glaser et al., 2022).
In the context of Egypt, climate vulnerability is intensified by a combination of hot summers, minimal rainfall, expansive desert terrain, and densely populated urban areas. These natural surroundings cause the nation to be one of the most at risk to worldwide climate change consequences, which makes life even harder for women who are pregnant (Elshahed et al., 2021).
Educational interventions, particularly nursing-led modules, have a central role in empowering pregnant women with the knowledge and strategies needed to respond effectively to health challenges linked to climate change. The educational intervention program assist women during pregnancy in making informed decision and adopt preventive health behaviors which can contribute to better quality of life (QoL) and favorable fetal health outcomes (Fasanghari & Keramat, 2023 ).
Therefore, this quasi-experimental study aims to assess the short-term effect of a structured nursing educational module on pregnant women's QoL and their reported health practices in response to climate change and heat stress in Egypt.
Review of the Literature
Egypt's triple effect of hot summers, limited rainfall, and the country's extensive desert, heavily populated cities, and terrain rank it among the top five countries most at risk from climate change worldwide (Akhtar, 2024). The United Nations Intergovernmental Panel on Climate Change (IPCC) clarifies that climate change is accelerating beyond previous projections, with widespread and intensifying impacts across sectors and regions (IPCC, 2022). Vulnerable and marginalized populations, including pregnant women, are among those most affected due to physiological and socioeconomic vulnerabilities (IPCC, 2022; Romanello et al., 2023).
The Egyptian Ministry of Health reports in 2021 that since the onset of the heat wave, there are 95 heat-related deaths and 1,914 injuries (MOH, 2021). During pregnancy, women experience various bodily changes that heighten their susceptibility to illnesses involving fever, consequently elevating their vulnerability and the risk of mortality. Women who are pregnant are found to be at a greater health risk everywhere, and studies show that they can have bad outcomes if they are exposed to really hot weather while they are pregnant (Bekkar et al., 2020; Hess et al., 2012; Kuehn, 2017). A lot of people affected by high temperatures suffer from preexisting health conditions such as persistent high blood pressure or weakened heart muscles, which can exacerbate heat exposure risk.
In addition, climate change results in lasting shifts in weather patterns and temperature levels. Such alterations may happen naturally as a result of significant volcanic eruptions or sun activity fluctuations. The main cause of climate change since the 19th century has been human activities, especially the combustion of conventional fuels such as coal, oil, and natural gas (Wright et al., 2023). The use of the Nursing Educational module is an officially acknowledged curriculum offering a comprehensive and solid foundation rooted in the behavioral, life, and nursing sciences for the overall practice of nursing (Gustini et al., 2024). The focus on pregnancy is the gestational period in which a fetus grows within the mother's uterus, usually spanning 40 weeks (Acar & Öter, 2024). The QoL, that is refers to the idea of the QoL, aims to measure the welfare of a population or an individual concerning both beneficial and detrimental elements of their overall life at one particular time (T, 2024).
Climate change has diverse and detrimental impacts on the QOL of pregnant women. Furthermore, heat exposure can cause fetal metabolism to shift from anabolic to catabolic pathways and increase maternal oxytocin and antidiuretic hormones, both of which decrease uterine blood flow. Pregnancy-related emotional stress is also linked to extremely high or low temperatures, which can worsen placental, endothelial, and endocrine dysfunctions (Yadav, 2023). In addition, excessive heat can impair placental function, induce dehydration and endocrine dysfunction, and overwhelm a pregnant woman's thermoregulatory system, particularly during labor. Hypertensive disorders, preterm birth, gestational diabetes, and stillbirth are examples of clinical sequelae (Kabir et al., 2023).
Water supplies are being influenced by climate change in several ways. Gastrointestinal and other ailments may arise from coming into contact with untreated polluted water, especially for pregnant women who are more vulnerable. Premature birth and pregnancy loss are possible outcomes of these conditions in extreme situations. Food production, availability, transportation, safety, and quality are all at risk during floods and droughts. Listeria and toxoplasma are examples of foodborne infections that can be fatal and raise the risk of stillbirth, miscarriage, or early delivery (Ashrafuzzaman et al., 2023).
All dimensions of pregnant women's QoL, both physically, emotionally, psychologically, and socially, are negatively affected by heat stressors and climate change. Ground-level ozone, smoke from wildfires, and dust from droughts are among the outdoor air pollutants that could rise as a result of climate change. Women who are pregnant are especially vulnerable to the negative consequences of vehicle emissions. They should take further care to limit their exposure to vehicle smoke, as this may affect the fetus's development and raise the possibility of premature labor and poor birth weight (Raihan, 2023). Extreme weather occurrences have been shown to raise emotional stress in pregnant women, worsen mental diseases, and cause psychological stress. Furthermore, these incidents may interfere with access to therapy, behavioral health resources, and support systems, all of which may impair women's capacity for coping (Kaya et al., 2025).
One kind of active learning that helps expectant mothers become more conscious of their particular requirements is an educational module. It's an efficient approach to learning where pregnant women receive information and practice to grasp knowledge and apply it in practice through educational modules. Before showcasing professional abilities, it can also be useful in imparting concepts and detailed instructions that positively affect QoL (ElSayed et al., 2024). Furthermore, continued teaching helps pregnant women to apply healthy practices to cope with climate change, which in turn improves the QoL (Shalaby Awad Mahmoud et al., 2023). Nurses are able to assist in advancing renewable energy sources, protecting the Earth's natural assets, and helping to decrease the release of harmful gases. Furthermore, they have the capacity to champion policy reforms on both community and global scales (Hudon et al., 2023).
Climate change is now considered one of the most pressing warnings to global health, and its disproportionate impact on pregnant women has drawn increasing concern from the international scientific community. Pregnant people tend to be more susceptible to harsh weather, polluted air, and not having enough food or clean water, and all of these issues are likely to get worse in the coming years (Romanello et al., 2023). Egyptian mothers are finding life tougher as they grapple with hotter weather patterns, sparser precipitation, and the density of city living. Pregnant women often experience multiple pressures which can increase vulnerability. Despite this, relatively limited educational and preventive interventions are specifically designed to address their needs in both practice and research.
This study responds to the identified gap by implementing nursing educational module targeting pregnant women. The module designed to enhance pregnant women’ knowledge and encouraging appropriate behavioral responses for managing heat stress and climate associated health risks. By assessing QoL alongside self-reported practices, the study examines how health education can function as a feasible preventive approach. This research is significant as it addresses a critical issue in public health and underscores the essential role that nurses play in the advancement of communities, as well as in motivating vulnerable populations to embrace methods for adjusting to alterations in the climate. The findings may contribute to the development of maternal health policies and community-based intervention planning in Egypt and other settings affected by climate related challenges.
The purpose of this present research is to assess the impact of nursing educational modules on climate change in enhancing the QoL and reported practices of pregnant women. This study hypothesized the following:
Method
Tools of Data Collection
Scoring System
Every knowledge variable was weighted based on the items in each multiple-choice question. Each item was given a value of 1 for correct answers and 0 for incorrect ones or unknown responses. To obtain the final score, the scores of each question were combined.
▪ > 60% correct responses are considered (good). ▪ 50 ≤ 60% correct responses are considered (average). ▪ < 50% correct responses are considered (poor).
The WHOQOL-BREF is an adapted version of the
The questionnaire consisted of 26 items: two items assessed overall QoL and general health, while the remaining 24 items were divided into four domains: physical health (seven items), psychological well-being (six items), social relationships (three items), and environmental factors (eight items; Ali et al., 2025).
Scoring System
The survey utilized a “5-point rating scale” ranged from 1 to 5 points: the higher the number of points, the superior the QoL. Average values were represented in each domain and computed following the key and guidelines.
Scoring System
Every practice variable was weighted based on the following items: never (0), sometimes (1), and always (2). The following categories apply to the total practice score:
▪ Satisfactory level: ≥60%–100%. ▪ Unsatisfactory level: < 60%.
Timeline of the Research Implementation and Evaluation Phases (May 2024–January 2025).
Results
Table 2 showed the general characteristics of the studied sample. It was clear that 56.3% of the studied sample were in the age group <25 years with a mean age of 25.95 ± 4.89 years. As regards the residence, 60.2% of the studied women lived in rural areas. Regarding the educational level, 33.6% of them had a university education. Furthermore, 56.3% of them were housewives.
Distribution of the Studied Sample according to Their General Characteristics (n = 128).

In terms of distribution of the studied sample regarding their obstetrical history, 56.3% of the participants were Primigravida (n = 72), 56.3% were Nulliparous (n = 72), and more than half of them were in their second trimester 54.7% (n = 70) with a mean gestational age of (16.32 ± 5.44) weeks. More details are presented in Table 3.
Distribution of the Studied Sample Regarding Their Obstetrical History (n = 128).

Table 4 showed a very notable statistical difference between the results from the time after the intervention and those from before the intervention, supporting the postintervention in all elements of the sample's understanding regarding climate change and heat stress, with p ≤ .001.
Distribution of the Studied Sample Regarding Knowledge About Climate Change and Heat Stress at Preintervention and Postintervention Phases (n = 128).

Figure 1 displayed that (31.2%) and (72.7%) of the studied sample had adequate knowledge regarding climate change and heat stress in the preintervention and postintervention phases, respectively.

Percentage distribution of the studied sample regarding total knowledge score about climate change and heat stress at preintervention and postintervention phases (n = 128).
Table 5 demonstrated that, in the phase prior to the intervention, the mean scores for overall QoL revealed a reduced QoL among the women analyzed (61.91 ± 7.46). However, postintervention, the mean difference score for overall QoL among the examined women was (96.42 ± 11.39), showing a highly significant statistical difference (p ≤ .001). There were significant variations across all dimensions of QoL, which included physical health, mental well-being, social relationships, and environmental factors, as well as two components relating to overall QoL and general health (p ≤ .001).
Total Mean Cores of Quality-of-Life Domains of Studied Women Toward Climate Change and Heat Stress at Preintervention and Postintervention (n = 128).

Note. Wilcoxon signed ranks test.
**A highly statistically significant p ≤ .001.
Table 6 revealed that there was a highly statistically significant difference in total mean scores of the studied women's reported practices toward climate change and heat stress at preintervention and postintervention phases, with p ≤ .001. The total mean score of reported practices was improved from 41.28 ± 7.27 to 63.15 ± 5.24.
Mean Scores of Studied Women's Reported Practices Toward Climate Change and Heat Stress at Preintervention and Postintervention (n = 128).

Note. Wilcoxon signed ranks test.
**A highly statistically significant p ≤ .001.
Figure 2 displayed that, (33.6%) and (77.3%) of the studied sample had satisfactory levels of reported practices regarding climate change and heat stress at pre- and postintervention phases respectively.

Percentage distribution of the studied sample regarding total reported practices scores toward climate change and heat stress at pre- and postintervention phases (n = 128).
Table 7 clarified that there was a highly significant statistically positive correlation between total knowledge score and (total reported practices and total QoL) scores regarding climate change and heat stress at preintervention and postintervention phases (p ≤ .001).
Correlation Between Total Knowledge, Total Reported Practices, and Total Quality of Life Scores of the Studied Sample Regarding Climate Change and Heat Stress at Pre- and Postintervention Phases (n = 128).

Discussion
The study addresses the urgent but neglected problem of the effect of climate change on pregnant women in Egypt, who are more vulnerable to heat and other environmental stressors, and the effectiveness of a structured nursing educational module to increase awareness and encourage healthier practices, in contrast to the majority of previous studies that focus on risks, showing how targeted education can enable women to safeguard their health and enhance their QoL, and highlighting the important role of nurses in assisting pregnant women to adjust to climate change in areas such as Egypt with particularly harsh environmental conditions.
Findings from this research pertaining to the general characteristics of the studied pregnant women showed that the mean age is 25.95 ± 4.89 years, and over half of the sample was under 25 years old.
Concerning residents, rural and urban areas were defined according to the
This finding closely mirrors results from India, where a large retrospective maternal-newborn health registry study (Belagavi, Nagpur, Thatta sites) found similar demographic patterns among pregnant women exposed to heat stress (Shankar et al., 2023). In that study, mean maternal ages clustered around the mid-20s, and a substantial proportion resided in rural areas, with varied education levels. As well as this finding aligns with Kaya et al. (2025), who carried out their study in Turkey and found that over two-thirds of pregnant women were under 25 years old, with an average age of 25.80 ± 3.43 years, and that approximately three-quarters lived in rural areas. Additionally, Acar and Öter (2024), studying pregnant women in Turkey, reported that over half of the participants originated from rural areas. Furthermore, the present study's results are consistent with findings by Rekha et al. (2024), whose research in India also highlighted similar demographic patterns among pregnant women.
Analysis of obstetrics history revealed that, over half of the studied women were experiencing their first pregnancy and had no previous deliveries, with a mean gestational age of “16.32 ± 5.44 weeks.” These findings are consistent with those reported by ElSayed et al. (2024), in an Egyptian study, which found that over one-quarter of women were nulliparous, over two-thirds of the women were primigravida and more than two-thirds in the second trimester of pregnancy.
Also, findings from other studies conducted in Egypt differ from those of the current research. Farg et al. (2024) reported that all participants were multigravida and two-thirds were multipara. Additionally, Afifi et al. (2024) observed that fewer than two-thirds of women in both the study and control group were multigravida. Furthermore, more than two-fifth of the control group and less than two-thirds of the study group were multiparous.
The findings of the current research showed a highly statistically significant enhancement across the knowledge of the pregnant women under study, with postintervention scores surpassing preintervention scores across all items related to climate change and heat stress. Similar results were reported by Ahmed et al. (2023), in Egypt, who found that the majority of pregnant women demonstrated in adequate knowledge regarding climate changes prior to the educational intervention, f0llowed by a noticeable improvement in their knowledge after its implementation. Moreover, the finding is consistent with Andreae et al. (2024), whose study in Germany indicated that only about 10% of participants had a high level of knowledge regarding climate change. The majority exhibited low knowledge, and fewer than one-third showed a moderate understanding. Additionally, Acar and Öter (2024) reported in their Turkish study that participants showed insufficient knowledge regarding the impact of climate change on maternal and infant health.
Pregnant women’ insufficient awareness of climate change and heat stress prior the intervention may be linked to their socioeconomic and residential circumstances. Many participants were unemployed and resided in rural areas, limited their access to information on current global issues such as climate change. Additionally, unemployment may have provided some protection from heat exposure, sunburn and other adverse consequences of climate change, which could explain participants limited interest in climate related issues (Heberlein et al., 2024). In contrast Ngwenya et al. (2018) reported that the majority of participants in Bulawayo, Zimbabwe, had adequate knowledge of climate change, where as only a few had limited understanding.
Concerning the QoL of the pregnant women analyzed before any intervention, the present research indicated that their overall QoL was adversely affected by climate change and thermal stress. This was reflected in their average QoL scores, which stood at 61.91 ± 7.46. In contrast, after the intervention, the average score for their overall QoL rose to 96.42 ± 11.39, showing a significant difference. The results of this study align with those of Menon (2024), who conducted the study in Kerala, India, and came to the conclusion that focused educational initiatives can enhance perceptions of health risks associated with climate change, which in turn can motivate expectant mothers to embrace healthier lifestyle choices that lessen the effects of climate change, aligns with existing evidence that structured prenatal education can significantly boost maternal well-being. Similarly, Lee et al. (2022) in 2022 found that structured antenatal education on environmental health risks led to a significant increase in both QoL and self-efficacy among pregnant women in urban South Korea. In another study for instance, Özkan et al. (2018) conducted a quasi-experimental study in Turkey using the Scale of Complaints during Pregnancy and their Effects on QoL and found that pregnant women who received structured prenatal education had significantly lower complaint scores and therefore higher QoL compared to a control group in both second and third trimesters (p < .05).
Concerning the documented behaviors related to climate change and heat stress, the results of the present study indicated a statistically significant difference in the overall average scores of the women's reported behaviors regarding climate change and heat stress before and after the intervention, with p ≤ .001. The overall mean score for reported behaviors changed from 41.28 ± 7.27 to 63.15 ± 5.24. This advancement in behaviors may be attributed to the enhanced awareness among pregnant women, and the majority of participants engaging with the educational module likely contributed to this improvement in practices. Additionally, when pregnant women have sufficient information and have adapted healthy practices, and can effectively adapt to climate change, they can achieve a better QoL in all dimensions, physically, psychologically, socially, and spiritually.
This finding aligns with previous research demonstrating the effectiveness of targeted health education interventions in enhancing maternal practices in response to environmental health risks. For instance, a quasi-experimental study conducted in Egypt among pregnant women working in outdoor environments reported a significant increase in knowledge and preventive practices related to heat stress after participating in a structured educational intervention (Mohamed & Hassan, 2024).
In addition, this result agreed with ElSayed et al. (2024), who conducted their study in Alexandria, Egypt, and reported that only a few numbers of women had a satisfactory level of practice before the implementation of the nursing educational module, and improved to two-thirds of the women after implementation. As interpreted by the researcher, the climate change educational module can have a positive impact on improving practices among pregnant women by increasing knowledge and promoting a better understanding of the potential maternal and fetal health risks associated with climate change. This program can support pregnant women in making proactive decisions to protect themselves and their unborn fetuses.
This result is congruent with Dewidar et al. (2023) who conducted their study in Alexandria, Egypt, and reported that there was a highly positive statistical correlation between total knowledge and total health-related behaviors of the studied women. In addition, this result was supported by a study by Lykins et al. (2024) whose research in California, USA, demonstrated that structured awareness programs increase knowledge and empower women to make informed decisions about their health and environmental practices during pregnancy.
Strengths of the Research
This study has several advantages. Validated scales were used to collect data. Numerous studies have so far emphasized the need to find evidence-based ways to mitigate the negative effects of climate change on the health of groups like young adults and college students. Our research may be unique in that it aims to establish a foundation for assessing how climate change education affects the awareness, QoL, and adaptive practices of expectant mothers.
Limitations of the Research
The researchers recruited participants from Benha University Hospital using a purposive sample. The study results might therefore not be typical of all expectant mothers in other regions of the world. One limitation of this study is the lack of a control group, although the sample size was large enough to allow for group division. The program was applied to all participants for ethical reasons, since the content was related to important health practices. It was not acceptable to prevent any participant from receiving this information. This may reduce the ability to confirm that the improvement was only due to the intervention, but the before-and-after comparison still gives useful results.
Due to the limited availability of research that directly addresses the effect of nursing educational modules on pregnant women's QoL in relation to climate change, particularly within the Egyptian context, some studies included in this research were chosen for their partial or conceptual relevance. Although these references may differ in location, population, or exact intervention type, they share a common focus on the role of education in improving health awareness and behaviors among vulnerable groups, especially pregnant women. Therefore, these studies were used to support the general framework of the current research and to provide theoretical and practical insights that help interpret the findings.
Implications for Nursing Practice
The findings of this study carry several important implications for nursing practice. The evidence strongly indicates that achieving a healthy pregnancy largely depends on women's ability to develop the necessary skills to effectively address their evolving needs. It may also help in better informing the job of professionals who take care of women in the hospital during pregnancy. Additionally, nurses can advocate for policies that mitigate climate change's effects on vulnerable populations, including pregnant women. By leveraging their expertise, they can push for climate-smart healthcare practices.
Conclusion
Maternal knowledge of pregnant women, QoL, and reported practices regarding climate change and heat stress were improved as a result of the nursing educational module. In addition, a statistically significant positive correlation existed between the total knowledge score and both QoL and reported practices, before and after the intervention scores for climate change and heat stress. Thus, the study's goal was accomplished, and the research hypotheses were supported.
Footnotes
Acknowledgments
The authors would like to express their sincere gratitude to Riyadh Elm University, College of Pharmacy, Nursing and Medical Sciences, for their support and assistance throughout this research.
Ethics Approval and Consent to Participate
The Scientific and Ethical Research Committee at Benha University, Faculty of Nursing was addressed (RES-OBSN-p77). All Women who participated in this study gave their oral consent to participate in the study, and confidentiality was guaranteed. Procedures were strictly aligned with applicable standards and laws, including the Declaration of Helsinki.
Author Contributors
FA: conceptualization, methodology, formal analysis, validation, investigation, writing—original draft preparation, visualization, writing—reviewing and editing; AA, RH, AM, and AA: conceptualization, methodology, data collection, writing—reviewing and RH and AA: conceptualization, methodology, writing—reviewing and editing. The authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
The datasets generated and/or analyzed during the current clinical trial are not publicly available as they have not been published but can be gained from the corresponding author upon reasonable request.