
Abstract
Introduction
Peripheral artery disease (PAD) is a chronic condition caused by atherosclerosis, leading to limb ischemia and reduced quality of life. While surgical interventions like angioplasty improve vascular patency, postoperative exercise rehabilitation is critical but often sees low adherence, with dropout rates over 60%. Research often overlooks patients' subjective experiences and barriers to rehabilitation.
Aim
This study explores postoperative exercise rehabilitation behaviors in PAD patients, aiming to identify influencing factors and inform targeted intervention strategies to enhance recovery and quality of life.
Methods
A qualitative study involved 18 PAD patients (mean age 63.1 ± 13.1 years, 77.8% male) from Shanghai Jiao Tong University School of Medicine, Shanghai Ninth People's Hospital, engaged in exercise rehabilitation for ≥2 months. Semi-structured interviews (40–60 min) were conducted from December 2024 to February 2025 until data saturation. Data were analyzed using NVivo 12, with themes identified through peer debriefing and an audit trail to ensure credibility.
Results
Patients reported partial walking improvements, though recovery varied by age and compliance. Low-intensity exercises like walking were preferred. Facilitators included medical guidance, perceived functional gains, social/familial support, and digital tools. Barriers were physiological (pain, weakness, ulcers) and psychological/social (lack of support, isolation, limited knowledge).
Conclusion
Exercise rehabilitation in PAD patients is shaped by diverse facilitators and barriers. Personalized interventions leveraging medical guidance, social support, and digital tools can boost adherence and outcomes. Addressing physiological and psychological barriers is essential for patient-centered rehabilitation. Future efforts should explore scalable, technology-driven solutions to optimize recovery.
Introduction
Peripheral arterial disease (PAD) is a chronic condition that significantly impacts the arteries of the lower extremities (Gornik & Beckman, 2005). With global aging and the rising prevalence of risk factors, including hypertension, diabetes, and smoking, the incidence of PAD has increased significantly (Fowkes et al., 2017). The prevalence of PAD ranges from 15% to 20% among individuals aged over 65 years (Fowkes et al., 2017). Atherosclerosis is the primary pathological mechanism of PAD, causing vascular stenosis or occlusion and subsequent limb ischemia. Patients commonly present with intermittent claudication, lower limb pain, and reduced skin temperature, among other symptoms (McDermott, 2015). Severe PAD may progress to limb ulcers, gangrene, and potential amputation, imposing significant physical, psychological, and socioeconomic burdens on patients, families, and society (Fowkes et al., 2017).
Surgical and endovascular interventions, including vascular bypass grafting, percutaneous transluminal angioplasty (PTA), and stent implantation, are vital for improving vascular patency and restoring limb perfusion in patients with PAD (Beckman et al., 2021). However, clinical evidence indicates that surgical interventions alone are insufficient to fully address postoperative rehabilitation challenges in patients with PAD (Vartanian & Conte, 2015). Patients with PAD post-surgery often experience impaired limb function recovery and an elevated risk of recurrent cardiovascular events (Smith et al., 2019). Studies indicate that, despite successful revascularization, some patients with PAD experience limited improvements in exercise capacity and quality of life (Vartanian & Conte, 2015).
Review of Literature
As a non-pharmacological intervention, exercise rehabilitation is pivotal in enhancing postoperative recovery for patients with PAD (Hamburg & Balady, 2011). Regular exercise promotes collateral circulation, enhances vascular endothelial function and muscle strength, alleviates intermittent claudication, and improves exercise endurance and self-care ability in patients (Gornik et al., 2024). Despite its benefits, postoperative exercise rehabilitation in patients with PAD exhibits low participation and adherence rates. International guidelines recommend exercise rehabilitation as the first-line treatment for PAD, with evidence demonstrating significant improvements in walking capacity and quality of life (Morcos et al., 2018). Despite the physiological benefits of exercise rehabilitation, long-term adherence among patients with PAD remains low, with information dropout rates exceeding 60% (McDermott, 2018). Current research on exercise rehabilitation for PAD primarily focuses on physiological outcomes, often overlooking patients' subjective experiences, psychological barriers, and social support needs (Signorelli et al., 2020).
This study aims to thoroughly investigate postoperative exercise rehabilitation behaviors in patients with PAD, identify influencing factors, and provide evidence for developing targeted intervention strategies. Nursing significantly influences postoperative mobility; thus, this study examines its impact on rehabilitation outcomes. By addressing rehabilitation barriers and optimizing a personalized rehabilitation navigation system, this research seeks to enhance recovery, improve quality of life, and advance intelligent, patient-centered rehabilitation medicine.
Methods
Aim of the Study
This study explored postoperative exercise rehabilitation behaviors in PAD patients, aiming to identify influencing factors and inform targeted intervention strategies to enhance recovery and quality of life.
Study Design
A descriptive qualitative study was conducted using in-depth semi-structured interviews. This article adhered to the Consolidated Criteria for Reporting Qualitative Research (COREQ) guidelines (Booth et al., 2014).
Participants and Recruitments
This study selected 18 patients diagnosed with PAD who had participated in structured exercise rehabilitation programs from Shanghai Jiao Tong University School of Medicine, Shanghai Ninth People's Hospital.
We utilized a purposeful sampling strategy, recruiting participants from an established peripheral artery disease (PAD) follow-up database at our institution. Potentially eligible patients, who were all undergoing continuous outpatient follow-up, were first identified by their treating surgeons. A dedicated research nurse subsequently screened this database weekly to confirm eligibility based on the study criteria.
Inclusion criteria required patients to: (1) have a history of hospital-based interventional vascular reconstruction (e.g., percutaneous transluminal angioplasty or stent implantation); (2) be in the early to mid-recovery stage, defined as 3 months to 3 years post-surgery; and (3) have completed at least 2 months of structured, hospital-supervised exercise rehabilitation to ensure active engagement in the rehabilitation process. We excluded patients who were currently hospitalized or in the early postoperative period (<2 months post-surgery), which we defined as the transition phase from hospital-based rehabilitation to self-management.
During a scheduled outpatient visit, the research nurse contacted confirmed eligible patients, explained the study objectives, and obtained written informed consent. Following consent, we collected their data. Semi-structured interviews were conducted by trained researchers between December 2024 and February 2025. Interviews continued until data saturation was achieved, defined as the point at which additional interviews yielded no new elements or relevant information regarding participants’ perspectives (Klompstra et al., 2024).
Data Collection
Interviews were conducted by a qualitative research expert unaffiliated with the participants. The semi-structured interview guide was developed by the research team, informed by clinical expertise, and finalized through consensus with vascular surgery specialists.
Data Analysis
All interviews were conducted using a guided patient description protocol. This study employed a descriptive qualitative design, with data collected through in-depth semi-structured interviews focusing on patients' experiences, challenges, and needs related to exercise rehabilitation for PAD. Each interview, lasting 40–60 min, was audio-recorded and transcribed verbatim. Data were analyzed using NVivo 12 software to code and identify core themes and subthemes.
Rigor
Interviews were audio-recorded and transcribed verbatim by H.J.P. and Y.F. Transcripts were verified against recordings for accuracy and anonymized to ensure participant confidentiality (PAD patient replacing names with codes like P01–P18).
To ensure the trustworthiness of our findings, we incorporated several validation strategies. Credibility was enhanced through peer debriefing; the three primary analysts (Y.F, Y.J.W., and S.Y.H.) regularly discussed the coding process and interpretive decisions. In cases of disagreement, additional authors (X.W.L, W.W.B., and Y.C.) with expertise in vascular surgery and qualitative research were consulted to reach a consensus, enriching the analytical depth. Furthermore, an audit trail, consisting of detailed records of procedural and analytical decisions from transcription to final theme development, was maintained within NVivo to ensure dependability and confirmability.
Results
Sample Characteristics
18 PAD patients comprised predominantly males (77.8%) with older age (mean age 63.1 ± 13.1 years), with most participants married (72.2%) and covered by urban medical insurance (61.1%). Among them, 66.7% were current smokers and 16.7% current drinkers, indicating health risks. Clinically, 44.4% exhibited severe lower limb ischemia (maximum walking distance < 300 m), underscoring significant disease burden, with moderate (33.3%) and mild (22.2%) cases less prevalent (Table 1).
Demographic and Health Characteristics of the Sample.
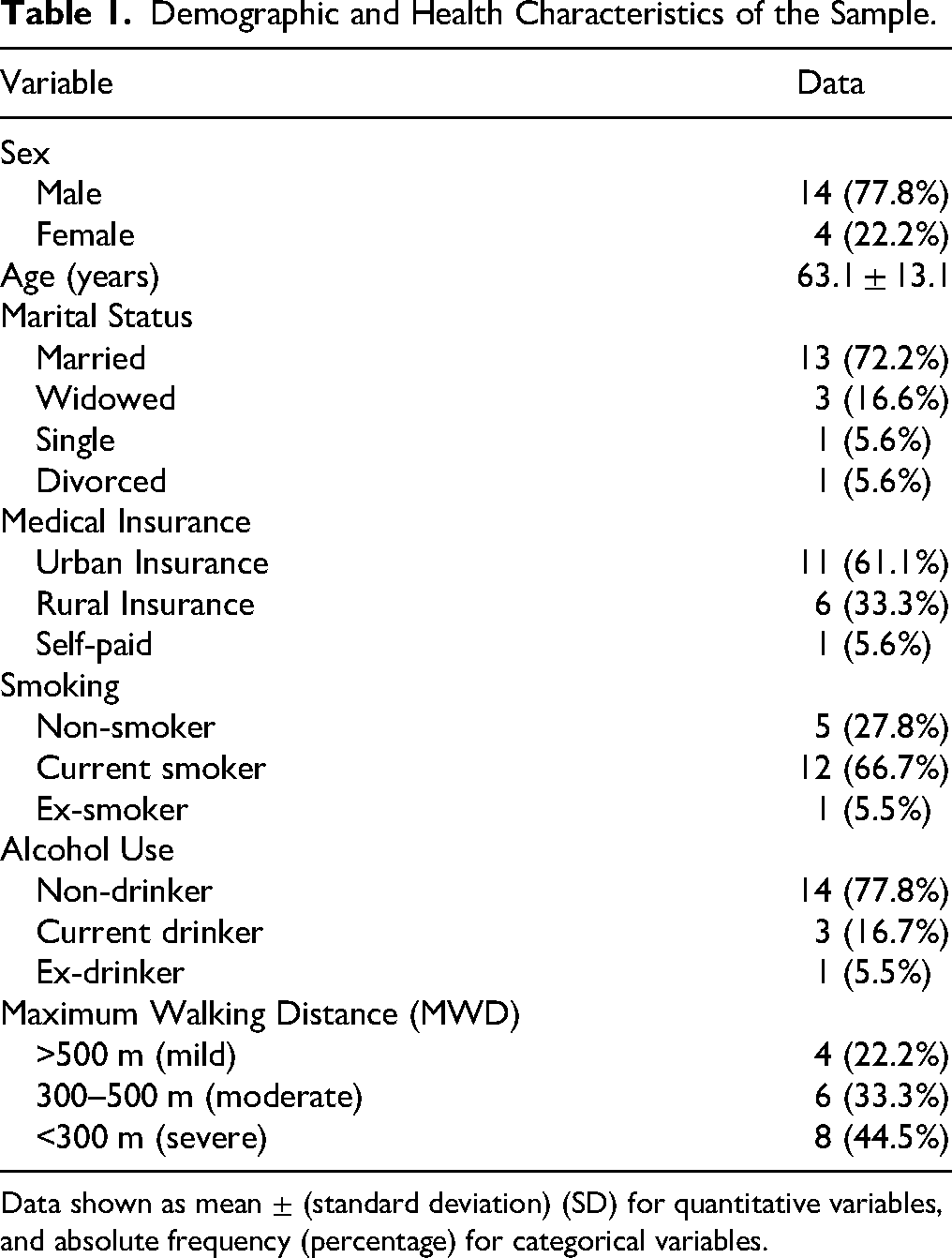
Data shown as mean ± (standard deviation) (SD) for quantitative variables, and absolute frequency (percentage) for categorical variables.
Study Themes
Postoperative Rehabilitation Experience, Needs, and Changes in Patients With PAD
Based on in-depth interviews with 18 patients with PAD, the study revealed that the postoperative exercise rehabilitation behaviors of these patients exhibited multi-dimensional experience, which could be specifically divided into the following two sub-themes:
Most patients (10 participants) reported a partial improvement in walking ability post-surgery, though recovery speed varied significantly by age, comorbidities, and compliance.
A patient who had undergone the surgery 1 year ago stated:
“Now I can walk around the community, much better than before the operation!.” (Male, 61 years old, underwent the surgery 1 year ago)
However, four patients were dissatisfied with the rehabilitation outcome due to the insignificant alleviation of limb ischemia symptoms (MWD < 300 m). They believed that the improvement in their quality of life after surgery was limited.
“The pain in my leg became unbearable when I walked less than 100 metres and was relieved only by painkillers.” (Female, 76 years old, underwent the surgery 1 year ago)
65% of patients prioritized safe, accessible exercises (for example: low-intensity Activities: walking), while only one participant engaged in resistance training.
"Walk slowly against the wall and feel more secure.” (Male, 79 years old, underwent t

Categories and subcategories for the facilitators to exercise rehabilitation and the multifaceted nature of rehabilitation barriers.
Facilitators to Exercise Rehabilitation
In this category, four facilitators were found, and four subcategories were performed: (i) Guidance from Medical Teams; (ii) Perceived Functional Improvement; (iii) Social and Familial Support; (iv) Digital Rehabilitation Tools
All patients mentioned the significance of doctors’ advice in formulating rehabilitation plans. A patient 1 year after surgery said:
"The doctor developed a detailed walking goal for me, which gave me a sense of direction in my rehabilitation process. They told me to walk 10 minutes a day, then gradually increased it to 30 minutes according to the results of the examination. Now the pain in my leg is not worse." (Male, 44 years, underwent the surgery 6 months ago)
11 participants reported that they saw visible progress as motivation.
“I walk from 200 meters to 1000 meters, watching the numbers rise, the heart has motivation.” (Male, 56 years, underwent the surgery 1 year ago).
7 participants relied on family encouragement for safety and adherence.
“My wife pushed me to stick to exercises. My husband walks with me every day, and he helps me when I can't walk.” (Female, 66 years, underwent the surgery 3 years ago).
Patients commonly called for tracking their rehabilitation progress through digital tools (such as apps). 7 patients suggested adding a home - based remote monitoring function.
“An app could remind me to exercise at home. And used wearables for real-time feedback, like sports bracelet” (Male, 58 years, underwent the surgery 3 months ago).
The Multifaceted Nature of Rehabilitation Barriers
Physiological Limitations
Pain (four participants), lower limb weakness (five participants), and complication was occurred ulcer (one participant) were the primary obstructive factors. A patient 3 months after surgery described:
“When I walk, my legs feel heavy. I can only walk a few hundred meters and then I have to stop.” (Male, 58 years, underwent the surgery 6 months ago)
Insufficient Psychological and Social Support
Four patients interrupted their exercise due to the lack of family supervision and rehabilitation knowledge. One patient gave up group sports because of a sense of social isolation. Lack of a final decision-maker.
“No one in the village understands this disease. The doctor asks me to move more, but I'm afraid I'll make a mistake.” (Male, 66 years, underwent the surgery 1 year ago).
Discussion
This study elucidates the postoperative exercise rehabilitation behaviors of patients with peripheral artery disease (PAD), highlighting facilitators and barriers that shape their experiences. The findings underscore the necessity of tailored exercise prescriptions and goal-setting, which provide clarity and motivation for patients. Nurses play a pivotal role in advocating for standardized, individualized rehabilitation protocols and ensuring continuity of care through regular follow-ups. However, modern healthcare increasingly relies on multidisciplinary teams to address the multifaceted barriers to rehabilitation, including physiological, psychological, and social challenges (Treat-Jacobson et al., 2019).
Physiological limitations, such as pain, lower limb weakness, and complications like ulcers, remain central challenges, consistent with PAD's pathophysiology (Hiatt et al., 2015). These barriers necessitate adaptive exercise protocols that balance intensity with symptom tolerance, such as interval walking programs to mitigate discomfort while maintaining therapeutic benefits. Kinesiologists and exercise specialists can contribute by designing evidence-based exercise regimens tailored to patients' physical capacities and symptom profiles, ensuring safe progression. Nurses, in collaboration with these specialists, can enhance patient education on exercise safety, self-monitoring techniques, and pain management strategies to address knowledge gaps that contribute to non-adherence.
Psychological barriers, including fear, anxiety, and social isolation, were reported by patients as significant obstacles to sustained engagement. Psychologists can play a critical role in addressing these barriers by providing cognitive-behavioral interventions, motivational interviewing, and coping strategies to build patients' confidence and resilience. For instance, addressing fear of pain or reinjury through psychological support can complement nursing-led education and encouragement. Social support deficits, such as lack of family supervision or community understanding, further highlight the need for rehabilitation professionals to facilitate peer support groups or community-based programs, fostering a sense of connection and accountability among patients.
The demand for digital rehabilitation tools, such as apps for remote monitoring and progress tracking, reflects a shift toward patient-centered, technology-driven care (Bull, 2023; Koebe et al., 2023). Nurses can lead the design and implementation of these tools, ensuring usability for older adults and incorporating features like real-time feedback, reminders, and virtual peer communities (Alruwaili et al., 2023). Collaboration with rehabilitation professionals and technology specialists is essential to integrate these tools into comprehensive care plans, ensuring they complement human interaction rather than replace it. Nurses remain central in interpreting data, adjusting plans, and providing empathetic support, while multidisciplinary input enhances the holistic nature of care.
The study's findings emphasize the need for a holistic assessment framework to address physiological and psychological barriers. Nurses, in partnership with psychologists, kinesiologists, exercise specialists, and rehabilitation professionals, can optimize pain management, adjust exercise intensity, and foster social support, thereby improving adherence (Tao et al., 2017). For example, integrating psychological counseling with tailored exercise plans can address both physical and emotional barriers, creating a synergistic effect.
While this study enriches understanding of PAD rehabilitation behaviors, its single-center design and small sample limit generalizability. Future research should explore diverse populations using longitudinal mixed-methods approaches to capture evolving patient needs. Testing the proposed rehabilitation navigation system in clinical settings, with input from multidisciplinary teams, will be crucial to validate its efficacy in improving adherence and outcomes.
Strengths and Limitations
This study provides valuable insights into the postoperative exercise rehabilitation behaviors of patients with PAD; however, several limitations must be acknowledged. The single-center design, conducted at from Shanghai Jiao Tong University School of Medicine, Shanghai Ninth People's Hospital, may limit the generalizability of findings to other healthcare settings with differing resources, patient demographics, or rehabilitation protocols. The small sample size of 18 participants, while sufficient for achieving data saturation in this qualitative study, restricts the ability to capture a broader range of experiences and may not fully represent the diversity of PAD patients. Additionally, the use of purposive sampling may introduce selection bias, as participants were required to have participated in a structured exercise rehabilitation program for at least two months, potentially excluding those with lower adherence or different rehabilitation experiences. The cross-sectional nature of the study limits insights into the long-term evolution of patients' rehabilitation behaviors and needs. Future research should address these limitations by incorporating multi-center designs, larger and more diverse samples, and longitudinal approaches to better understand the dynamic nature of postoperative rehabilitation in PAD patients.
Implication for Practice
Exercise rehabilitation in PAD patients is shaped by diverse facilitators and barriers. Addressing physiological and psychological barriers is essential for patient-centered rehabilitation. Future efforts should explore scalable, technology-driven solutions to optimize recovery.
Conclusion
This study highlights the critical role of nurses in developing personalized exercise programs and leveraging technology-based monitoring systems to enhance postoperative rehabilitation for PAD patients. By integrating comprehensive health education and tailored interventions, nurses can improve patient adherence and quality of life. However, large-scale, multi-center clinical trials are needed to validate the proposed intelligent rehabilitation navigation system and ensure its broader applicability in clinical practice. This research provides a foundation for advancing patient-centered, technology-driven rehabilitation in PAD care.
Supplemental Material
sj-docx-1-son-10.1177_23779608261421741 - Supplemental material for Qualitative Research on Postoperative Exercise Rehabilitation Behavior of Patients With Peripheral Artery Disease (PAD)
Supplemental material, sj-docx-1-son-10.1177_23779608261421741 for Qualitative Research on Postoperative Exercise Rehabilitation Behavior of Patients With Peripheral Artery Disease (PAD) by Yan Fu, Yanjie Wang, Hongji Pu, Peng Qiu, Xinwu Lu, Yong Cheng, Siyi Huang and Weiwei Bian in SAGE Open Nursing
Supplemental Material
sj-docx-2-son-10.1177_23779608261421741 - Supplemental material for Qualitative Research on Postoperative Exercise Rehabilitation Behavior of Patients With Peripheral Artery Disease (PAD)
Supplemental material, sj-docx-2-son-10.1177_23779608261421741 for Qualitative Research on Postoperative Exercise Rehabilitation Behavior of Patients With Peripheral Artery Disease (PAD) by Yan Fu, Yanjie Wang, Hongji Pu, Peng Qiu, Xinwu Lu, Yong Cheng, Siyi Huang and Weiwei Bian in SAGE Open Nursing
Footnotes
Ethical Statement
All were performed in accordance with the procedures of the Declaration of Helsinki. Ethical approval was obtained from the Shanghai Ninth People's Hospital, Shanghai JiaoTong University School of Medicine Ethics Committee (Approval Number: SH9H-2024-T344-2). All participants provided written informed consent prior to participating in the study.
Author Contributions
Yan Fu (investigation, formal analysis, methodology, writing—original draft preparation, writing—review and editing), Yanjie Wang (conceptualization, formal analysis, methodology, writing—original draft preparation, writing—review and editing, supervision), Hongji Pu (investigation, formal analysis, methodology, writing—original draft preparation, writing—review and editing), Peng Qiu (investigation, writing—review and editing, supervision), Xinwu Lu (investigation, conceptualization, writing—review and editing, supervision), Yong Cheng (conceptualization, formal analysis, conceptualization, writing—review and editing, supervision, project administration), Siyi Huang (investigation, formal analysis, conceptualization, writing—review and editing, supervision, project administration), Weiwei Bian (conceptualization, data curation, writing—review and editing, supervision, project administration). All authors have read and agreed to the published version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Original Exploration Project of Shanghai Ninth People's Hospital, Shanghai Municipal Health Bureau Project, Shanghai Ninth People's Hospital Nursing Fund Project, Clinical Research Program of 9th People's Hospital, The National Natural Science Foundation of China (grant nos. JYYC004, 20224Y0170, 202240145, JYHL2023MS05, JYHL2024ZD01-Z3, JYLJ202204, 82300540, 82170509, 82370494, 82170411).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
The data that support the findings of this study are available from the corresponding authors upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.