
Abstract
The Sickle Cell Data Collection program reported maternal death rates in California (2004–2014) of 629 per 100,000 for Black women with SCD, 12 per 100,000 for Black women without SCD, and 6 per 100,000 in the general population. Yet little is known about the lived experiences of pregnant Black women with SCD, or their perceptions of nurses as advocates. To explore how social structures shape maternal health, the complexities of pregnancy while living with SCD, and nursing's role in care and advocacy, a qualitative study using semi-structured interviews was conducted. An interpretive framework centered participants’ voices and revealed key themes: (1) Trauma During Childbirth; (2) Dismissal, Disbelief, and Inadequate Pain Management; (3) Self-advocacy; and (4) Emotional and Psychological Impact. Together, these themes highlight the intersecting challenges of pregnancy faced by Black women with SCD and the transformative potential of compassionate, informed, and equitable care.
Background
Most research is reported not from the perspective of the population directly impacted, but rather from that of surrounding personnel such as healthcare professionals. When Black women participate in studies, research is often centered on White groups as the standard of reference. Findings are then generalized and applied to other groups, leaving Black women marginalized and rendered “other” (Thomas, 2022).
Review of Literature
According to the Centers for Disease Control and Prevention (2023) over 80% of pregnancy-related deaths of Black women in the United States are preventable. From 2004–2014 the CDC conducted a state-level surveillance of California's in-hospital maternal mortality rate among women with sickle cell disease (SCD) compared to all women and Black women without SCD (Raider et al., 2016). During these eleven years, the Sickle Cell Data Collection program found the maternal death rate for SCD was 629 per 100,000 compared to 6 per 100,000 maternal deaths in the general population, and 12 per 100,000 maternal deaths for Black women.
In society, the voices of Black women are often underrepresented or overlooked, a pattern that can also be observed within healthcare settings. While maternal health outcomes for Black women with SCD is improving, what remains lacking is the intentional engagement of women with SCD in shaping and informing the understanding of this maternal health experience. Identifying literature that specifically centered Black women as the study population proved challenging. The underrepresentation of the voices of Black women with SCD remains a critical gap in research that must be addressed (Le et al., 2022).
Black women experience racism, biases, stereotyping, and other forms of discrimination that cause disparities which negatively impact maternal health (Patterson et al., 2022). The negative impact of disparities in maternal health for Black women results in increased levels of stress, which has physiological ramifications on the body (Brantley, 2023). Additional SCD related racial disparities, implicit biases, and stigma compound the health disparities that are already evident in maternal health for Black women (Anderson & Roberts, 2019).
The lived experiences of pregnant Black women with SCD have not been prioritized in healthcare improvement or research, despite their significantly higher risk of severe maternal morbidity and mortality. Gaining insight into how these women perceive their maternal health experiences can inform efforts to improve outcomes. Thus, the purpose of this study is to explore the maternal health experiences of Black women with SCD.
Methods
This study was conducted using a Hermeneutic phenomenological approach. Hermeneutic phenomenology aids the researcher in finding the deeper meaning and understanding of the experiences related to the phenomenon, by employing deep listening and openness, to allow the participants to discuss their experiences and perceptions (Creswell & Creswell, 2017). A constructivist interpretive framework was used to center the discussion of the topic around the participants’ experiences. In doing so, the essence of the lived experiences gathered is used to generate or develop a theory or pattern of knowing (Creswell & Creswell, 2017).
Ethical approval for this qualitative study was obtained from the authors’ institutional review board before recruitment and data collection commenced. A target sample size of 5 to 15 participants of Black women with SCD who are or have been pregnant within the last ten years were invited to participate in this study. Recruitment occurred using purposeful sampling of participants who have experience with the phenomenon through the Sickle Cell Care Center at the author's institution, and snowballing technique.
After obtaining informed consent, virtual interviews were conducted using a key informant interview guide. Participants were interviewed from February 2025 and April 2025. Each interview ranged between 20 and 90 min. All the interviews were audio-recorded and transcribed by the researcher. Verbatim transcripts of audio recordings were initially coded using handwritten notations on a wide column on the right-hand side of the transcribed interviews. As coding continued emerging themes and patterns were identified.
An interpretive summary of every interview was completed. The researcher continued with data immersion by reading and rereading notes and transcripts, listening to audio recordings, and recalling observations and experiences. This process consisted of a continuous circular and reflexive process where common meanings and interpretations were presented. This led to the researcher summarizing and listing patterns or emerging themes from all the interviews.
Results
The participants consisted of nine Black women ages 18 years and older who are or have been pregnant within the last ten years in the United States. While conducting the nine interviews and parallel analysis, a point was reached when no new themes emerged, thus reaching the point of data saturation. The study focuses on the maternal health experiences and perceptions of the participants throughout pregnancy and child-birth, as well as the role and impact nursing advocacy had on their hospital encounters and childbirth experiences.
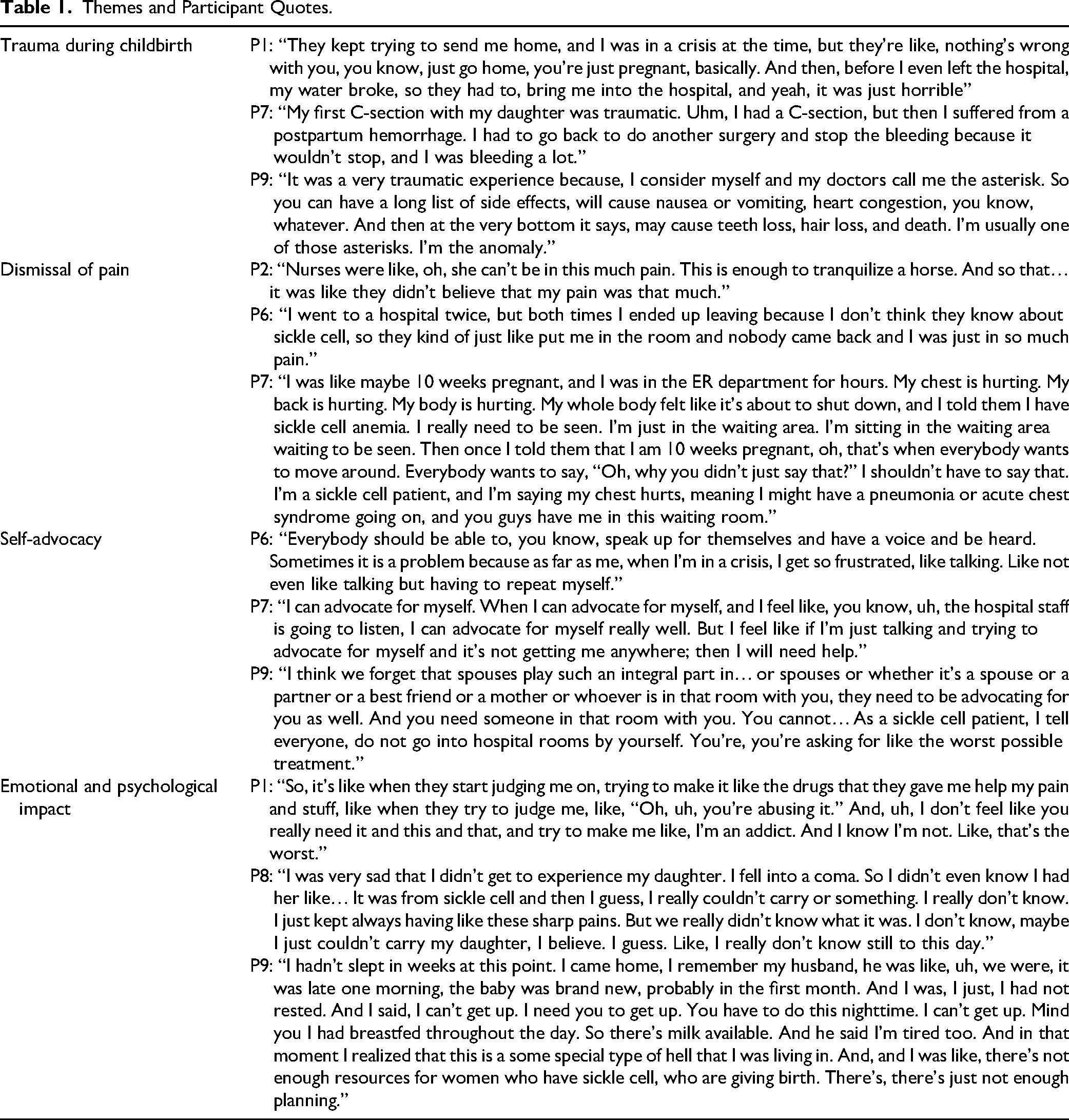
After completing thematic analysis, four major themes emerged representing the participants’ maternal health and birthing experiences as Black women with SCD: (1) trauma during childbirth; (2) dismissal of pain; (3) self-advocacy; (4) emotional and psychological impact. See Table 1 for themes and exemplar participant quotes.
Themes and Participant Quotes.
Theme 1: Trauma During Childbirth
More than five participants described experiencing trauma during childbirth, often shaped by a combination of medical complications, inadequate responsiveness on the part of healthcare providers, and the intersection of SCD with pregnancy. Both physical and emotional trauma were revealed, as well as a pervasive sense of being dismissed, unheard, and disbelieved at critical junctures of care.
Participant 1 recounted a profoundly traumatic labor experience in which she, already in sickle cell crises, was not recognized as being in active labor despite prior notification to the hospital. Upon arrival at the hospital, as a primigravida she recognized that the baby “was about to come out in the car.” She was directed to go to the emergency room where she informed staff that she was about to deliver. Her admission to the labor and delivery unit was only expedited after her mother intervened on her behalf, disclosing her SCD diagnosis.
Despite the baby being delivered within hours of her arrival the participant found herself having to convince the healthcare team that she was in labor which impacted the remainder of the time she had left where her birthing plan could have been implemented. She remained hospitalized for a week after delivery due to ongoing sickle cell crisis, and described the experience as emotionally devastating, citing feelings of being silenced and dismissed, causing further mental distress, stating, “it really mentally messed me up.” Other participants similarly reported complications and trauma experienced during childbirth.
Participant 8, for example, experienced postpartum hemorrhage requiring multiple blood transfusions and surgery during her first pregnancy. Her second pregnancy was not only high risk but was marked by frequent pain crises. She was hospitalized at eight months and diagnosed with acute chest syndrome and pneumonia, resulting in early induction.
Participant 9 described the traumatic delivery of her first child, during which she was in a coma and unable to remember the experience. Her second pregnancy brought fear, with the past trauma resurfacing. She recalls telling her provider, “I hope I don’t die,” reflecting her deep-seated fear due to prior complications experienced.
Participant 10 experienced severe psychological and physical distress during childbirth. At six months gestation, she began to feel a persistent fear of dying. Accustomed to experiencing adverse effects to medications, she initially planned for a birth without an epidural. However, after consenting to an epidural at 8 cm dilation, her baby's heart rate dropped, necessitating an emergency caesarean section. She experienced intense fear, pleading with her husband to advocate for her survival, saying, “Oh, God, surgery, they're going to cut me open. Oh, I'm going to die for real,” “please don't let them kill me. Please don't let them kill me. Please don't let them kill me. Please, please advocate for me. Please fight for me.”
Collectively, these narratives illustrate how childbirth experiences for women with SCD can be marked by medical complexity, compounded fear, and emotional trauma. Participants consistently emphasized a lack of provider responsiveness, cultural sensitivity, and individualized care—factors that not only may have influenced the clinical outcomes but also left lasting psychological impacts.
Theme 2: Dismissal, Disbelief, and Inadequate Pain Management
Approximately two thirds of the participants reported that their pain, whether due to sickle cell crisis or labor, was dismissed or disbelieved by healthcare providers, leading to inadequate pain management. This lack of validation and appropriate response not only intensified their physical suffering, but contributed to emotional distress and medical mistrust.
Participant 1 recounted a stark contrast in pain treatment while sharing a hospital room with a patient who reported similar pain levels. The other patient received timely and effective medication with expressed relief, whereas Participant 1 was prescribed a markedly different and ineffective pain regimen. Describing another encounter, she recalls going to a hospital unfamiliar with her condition and was left waiting in the emergency room lobby for 10 to 12 h, despite having identified herself as high-risk, due to SCD.
Participant 2 expressed the differences in care she received at a general hospital vs. a university affiliated medical center with OB-GYN specialists familiar with high-risk pregnancies and SCD. Staff in the general hospital were reluctant to administer pain medication for her sickle cell crisis due to misconceptions about opioid use during pregnancy. The doctor told her, “but the book says-you can't be on opioids and pregnant, so we can't give you this pain medicine.” While the nurses told her “Oh, I don't want to give you this. I don't want to harm your kids.” In contrast, once she was transferred to the university hospital the care she received attentive care and she felt well taken care of. Nonetheless, during her 65-day admission, she recalls inadequately managed pain, and felt that her post-delivery concerns were dismissed. Staff insisted that she was ready to be discharged, despite her fear of crisis due to the physical strain of labor.
Participant 6 echoed a common sentiment of racial bias, stating that her identity as a Black woman appeared to make the nurses “skeptical about my pain level and had assumptions about drug behavior.” Similarly, Participant 8 described disparities in care depending on whether she was at a hospital that specializes in high-risk pregnancies or a general hospital, reiterating the broader trend of inadequate and inequitable treatment across varying healthcare settings. She experienced going to the general hospital at 10 weeks gestation and reported to the nursing staff: My chest is hurting. My back is hurting. My body is hurting. My whole body feels like it's about to shut down, and I told them I have sickle cell anemia. I really need to be seen. I'm just in the waiting area. Then once I told them that I am 10 weeks pregnant, oh, that's when everybody wants to move around. ‘Oh, why you didn't just say that?’ I shouldn't have to say that. I'm a sickle cell patient, and I'm saying my chest hurts, meaning I might have a pneumonia or acute chest syndrome going on, and you guys have me in this waiting room.
Participant 9 shared a particularly distressing encounter with providers who interpreted her extended periods of sleep as a side effect of the narcotics, instead of a coping mechanism for severe pain. She recalls a provider remarking, “Oh, I got to get her off of that,” based on an assumption of overmedication instead of ongoing suffering. This misinterpretation reflected a fundamental misunderstanding of her pain experience and led to skepticism about the legitimacy of her condition. Going to the hospital is her last resort. She said, I go to the hospital when I can't take it anymore, like my pain medicine's not working, the heating pad, me taking baths, me drinking a whole bunch of fluids, stuff like that. That's why I fight it for the longest that I can.
Participant 10 recounted regularly being met with healthcare providers’ disbelief when reporting her pain as 10 out of 10 on the pain scale. She noted that because she does not “look” like she is in pain with objective signs that providers expect (such as screaming or appearing visibly distressed), her reports are often dismissed or her pain underestimated. As a result, she finds herself compelled to educate healthcare workers about the subjective nature of pain, particularly in the context of SCD, where patients may develop high pain tolerance and/or express pain in non-stereotypical ways. I have to ask this person who I do not know, nor do I trust, for help. And to be turned away and told no, or I don't think you need what you're asking for even though I know me better than you will ever know me. I think that it's respecting and understanding that every person is different. There's no two humans alike. So, what you saw before, right? You saw that person who came in, who was in serious chronic sickling pain, who was dancing around their room, and on TikTok and laughing and giggling. Maybe that's how they cope.
These accounts illustrate the critical role of specialized care in improving outcomes for high-risk pregnant patients with SCD, as well as the pervasive impact of provider misjudgments on patient trust and pain management.
Theme 3: Self-Advocacy
A recurring theme across participant narratives was the necessity of self-advocacy in navigating the healthcare system. Several participants reported that advocating for themselves was frequently required to ensure appropriate care, especially in the context of inadequate communication, racial bias, and disbelief of patient-reported symptoms.
Participant 2 described feeling entirely alone in her care, to the point where she assumed the role of her own advocate and care coordinator while hospitalized, stating, I was advocating even in that hospital bed, I was calling the attendings. I was setting up meetings. I was setting up multidisciplinary meetings every Thursday at three o'clock.
Participant 7 similarly expressed frustration at having to repeatedly explain and clarify her needs, often while in the throes of a sickle cell crisis. An example of this was after undergoing a Cesarean section when she was given only Tylenol and ibuprofen for pain management despite being in crisis and post-operative pain. She had to explicitly state her condition and surgical history to receive appropriate attention. In such moments, her fiancé also acted as an advocate when she was too debilitated to speak for herself.
Participant 8 reported frequently feeling the need to advocate for herself when she perceived being treated differently based on race. She described confronting staff when disparities were evident, stating, I feel like it's getting racist, I call them out. Like, I don't like being treated like this. I will prefer you to treat me the way you just treated the other patient.
Participant 9 recalled a particularly troubling encounter when a provider told her “Okay. I'm going to do a pill count for you,” implying suspicion of misuse. She challenged the provider by saying… “you’re not doing a pill count for the White people.” This confrontation exemplifies how perceived racial bias prompted her to self-advocate and resist discriminatory treatment.
Participant 10 similarly experienced skepticism from providers regarding her knowledge of pain management and opioids. When questioned, “Why do you know so much about opioids?” she explained that her understanding stemmed from decades of managing her condition. Since I've been on them since I was five, maybe I may have read something about them over the last 40 years.
These accounts underscore the emotional labor patients with SCD—particularly Black women—must expend to be heard, believed, and appropriately treated. The findings point to common failure in provider communication, cultural responsiveness, and patient-centered care, placing an undue burden on individuals to navigate and rectify their own care in the midst of complex and debilitating health challenges.
Theme 4: Emotional and Psychological Impact
A majority of participants described experiencing a profound emotional and psychological toll associated with managing pregnancy and chronic illness, specifically SCD. The cumulative burden of pain, pervasive bias, and prolonged hospitalizations contributed to overwhelming feelings of frustration, exhaustion, depression, and fear.
Participant 2, who was hospitalized for 65 days during her pregnancy, articulated the emotional weight of enduring repeated negative interactions with healthcare staff. I don't want to be here dealing with attitude from the nurses and doctors. And I just felt like every shift, there was always someone who had that weird stank attitude towards me. And it got to a point where I was going through like almost like a depression, you know, because of it. Because it was just so overwhelming.
Participant 3 emphasized how taxing pregnancy is on the body, and emotionally draining for women with SCD. She found it easier to communicate with the nurses than the doctors, indicating a possible lack of empathetic or accessible communication from providers.
Participant 4 expressed that the cumulative impact of racial discrimination and lack of support resulted in a lasting mistrust of the healthcare system. Her reluctance to seek care stemmed from a fear of experiencing repeated mistreatment, noting “the same treatment will happen again.” This sentiment underscores how negative encounters can deter individuals from accessing critical medical support.
Participant 7 shared an emotional account of an unscheduled hospital admission just two weeks before her due date, prompted by a potential sickle cell crisis. She was overwhelmed by the disruption of her birth plan and absence of her support system, leading her to break down in tears. She wanted her sister to be there and her hair to be nicely done to feel good, not this sudden change of plans. Her story highlights the emotional toll of lost autonomy and unmet expectations during pregnancy and childbirth.
Participant 8 described intense physical and emotional exhaustion during both of her pregnancies, each marked by severe sickle cell crises. She was hospitalized for extended periods after each birth—several weeks with her first child and two months with her second—making it difficult to care for her first born and contributing to feelings of isolation and emotional distress. She also reported feeling stigmatized and harassed by medical providers, who she believed viewed her as a drug seeker, compounding her psychological burden.
Participant 10 shared a distressing account of persistent premonitions of death during the last four months of her pregnancy. After giving birth, she experienced disorientation and a dissociative state marked by sensory distortion. This culminated in a striking encounter with a lactation consultant who prayed for her, affirming the participant's long-standing fear that something was seriously wrong, saying “the spirit of death is here.” Participant 1 agreed to prayer and stated “because no one else in here believes me that I’m going to die. I’ve been saying it for weeks.” When the lactation consultant finished praying her hair and scrubs were physically drenched with sweat.
The very next day a different lactation consultant came into her room, whom she immediately sensed was unfamiliar and unsettling. When she expressed concern to her husband, he noted that this individual had been caring for her for days. However, when the original consultant returned and was told the name of the earlier visitor, she informed the participant that no such person was on staff. The participant stated, I have to say the supernatural side of it because supernatural side of it played such a role in how I felt, that feeling of death.
These narratives reflect how the intersection of chronic illness, pregnancy, and systemic inequities generates substantial psychological strain for individuals with SCD. The emotional toll, often exacerbated by inadequate care and invalidation, can have lasting mental health implications that extend well beyond the clinical setting.
Discussion
The purpose of this study was to explore the experiences of Black women with SCD during childbirth and perinatal care. Addressing this gap required centering the voices of pregnant Black women with SCD, who remain underrepresented in clinical research despite being disproportionately affected by the disease (Le et al., 2022). Several themes discussed in this manuscript can be found in the current literature. Specifically, SCD stigma, racial bias, and inadequate pain management experienced during traumatic childbirth. Social, racial, and institutional disparities impact maternal health of Black women and contribute to poor health outcomes.
Disparities in maternal healthcare access and quality contribute to adverse pregnancy outcomes due to implicit biases, stereotyping, racism, and lack of cultural competencies in maternal health and medical treatment (Byrd et al., 2022; Eapen et al., 2023; Montalmant & Ettinger, 2023). Providers may dismiss patient concerns, limit information, and spend considerably less time with Black women compared to Non-Hispanic White women (Adebayo et al., 2022; Montalmant & Ettinger, 2023).
These inequities increase risks of postpartum complications, including unnecessary caesarean sections, infections, and hemorrhage (Brantley, 2023; Early et al., 2023). Structural racism and implicit bias further elevate maternal mortality risks, even among highly educated and economically secure Black women (Byrd et al., 2022; Montalmant & Ettinger, 2023).
For women with SCD, pregnancy and the postpartum period often intensify pain crises, requiring aggressive pain management (Parrish & Morrison, 2013). Yet providers frequently question the legitimacy of reported pain, perpetuate stereotypes of “drug seekers,” and overlook patient concerns (Wu et al., 2024). These misconceptions force women to self-advocate, despite evidence showing no adverse effects to mother or fetus (Brantley, 2023; Byrd et al., 2022).
A key contribution of this study is presenting these themes from the firsthand perspective of women with SCD. Beyond existing literature, participants described dismissal and disbelief of pain; the burden of self-advocacy; and the emotional and psychological toll of biased care. Such experiences erode trust in providers and reflect systemic patterns where patient-reported pain is validated only when it aligns with provider expectations.
Together, these findings provide a comprehensive understanding of the compounded challenges faced by Black women with SCD in perinatal care. Their accounts reveal how stigma, mismanagement, and racial bias exacerbate both physical and emotional burdens, underscoring the urgent need for compassionate, culturally competent, patient-centered care. Ensuring respect, dignity, and equitable treatment is essential to improving maternal health outcomes for women with SCD.
Strengths and Limitations
A key strength of this study is its focus on centering the experiences of pregnant Black women with SCD. The voices of Black women provide much needed insight into what it is like to experience pregnancy and childbirth while having SCD, a group that is often underrepresented in research. By prioritizing the voices of these women, the study offers invaluable insight into the unique challenges they face during pregnancy and childbirth while managing a chronic illness. These lived experiences provide a crucial perspective on how race, healthcare disparities, and SCD intersect in clinical settings, informing the broader discussion on improving care for this population.
However, the study is not without limitations. One limitation is the method of participant recruitment. Although snowball sampling is an effective tool for reaching specific, hard-to-reach populations, it was not the only recruitment technique used. In this study, a significant amount of time was utilized in screening participants who were interested in participating for the incentive of a gift card, as noted on recruitment flyers. Upon screening it was determined that some provided phone numbers were invalid or “subscriber” numbers. This created delays in recruitment and may have impacted the diversity of the sample.
Additionally, this study used a qualitative approach that emphasizes depth and context rather than statistical comparison. Its purpose is to provide a nuanced understanding of participants’ lived experiences, not to generate generalizable findings. The target sample size of 5 to 15 participants is consistent with phenomenological Research, where the goal is transferability—the extent to which insights resonate across contexts—rather than statistical representation (Creswell & Creswell, 2017). A smaller sample supports “thick description” of the research context and allows the researcher to explore the unexpected and uncover the “why” behind the “what.” In phenomenological studies, sample size is guided by data saturation, the point at which no new themes or insights emerge (Creswell & Creswell, 2017). Thus, the strength of this design lies in its capacity to yield rich, meaningful interpretations rather than broad generalizations.
The qualitative framework remains consistent with the study's conceptual framework, prioritizing the voices and lived experiences of the participants. The narratives shared by the nine participants offer meaningful contributions to the ongoing maternal health conversation. Gaining insight and understanding into their experiences is an important step towards improving maternal health outcomes for Black women with SCD.
Implications for Practice
The experiences of women with SCD reveal persistent healthcare challenges, including racial discrimination, inadequate pain management, and limited provider knowledge, all of which compound physical and emotional burdens. Participants’ narratives underscored how the intersection of race, gender, and chronic illness heightens vulnerability during childbirth. These findings show that systemic inequities, disbelief, and stigmatization affect not only the clinical but also the emotional and psychological well-being of affected women. Self-advocacy becomes necessary, yet burdensome, as they navigate a system that frequently fails to recognize their unique needs.
Nurses must move beyond procedural care toward relational, equitable, and advocacy-based approaches. Integrating patient narratives into practice and scholarship ensures that Black women with SCD are central—not peripheral—to advancing maternal health and reshaping nursing ethics, research, and education. Future research should employ community-engaged qualitative methodologies (e.g., participatory action research, narrative inquiry) to amplify patient voices. Patient-centered care requires individualized pain assessments that prioritize verbal reports and contextual understanding over stereotypical visual cues, while embedding empathy and advocacy into routine practice to rebuild patient trust and reduce fear-driven avoidance of care.
Nursing education must critically examine how curricula address systemic racism and bias in maternal health, evaluate the impact of training on cultural competence and SCD care, and explore policy-level strategies for implementing standardized pain management and accountability in hospital systems. Strengthening provider education—particularly for nurses—and fostering a culture of compassion and patient-centered care are essential steps toward improving healthcare experiences and outcomes for women with SCD.
Conclusion
Black women with SCD encounter healthcare environments often marked by mistrust, inadequate pain management, and systemic bias. Their need to self-advocate highlights both strength and persistent gaps in equitable, culturally responsive care. Addressing these challenges requires structural and educational reform, including provider training on implicit bias, cultural humility, and SCD-specific knowledge.
Centering the voices of Black women in maternal health research and clinical practice provides essential insight for reshaping policy and advancing culturally competent interventions. Elevating these perspectives is critical to building inclusive, patient-centered care models that actively dismantle bias and improve maternal outcomes.
Footnotes
Acknowledgments
I would like to acknowledge Loma Linda University Health Sickle Cell Center staff and Cayenne Wellness for recruitment assistance, and the participants for their valuable contributions.
Ethical Approval and Informed Consent
Institutional review board approval #5240549; informed consent is received from each participant prior to data collection.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was partially funded by Health Resources and Services Administration (HRSA) of the U.S. Department of Health and Human Services (HHS) (grant number UR6MC50347-01-00), Maternal Health Research Network (MH-RN) for MSIs–Research Awards to LOMA LINDA UNIVERSITY, Loma Linda, California. This content and conclusions are those of the authors and should not be construed as the official position or policy of, nor should any endorsement be inferred by HRSA, HHS, or the U.S. Government.
Declaration of Conflicting Interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data are not made publicly available to protect the confidentiality of participants.