
Abstract
Introduction
Experiencing birth trauma can result in various mental health issues, such as posttraumatic stress disorder, postpartum depression, anxiety, and challenges with bonding. Typical signs of traumatic childbirth include flashbacks, nightmares, avoidance of reminders, physical distress when triggered, loss of sexual intimacy, neglect of gynecological care, mood swings, anger, and social withdrawal. This study is novel and significant providing in-depth insights that are often absent from existing literature.
Objectives
To investigate the traumatic birth experiences of Saudi mothers, as well as their perceptions of and reactions to traumatic childbirth.
Methods
An interpretative phenomenological qualitative study was conducted in one government hospital in the eastern province of Saudi Arabia. This study employed a purposive sampling method to recruit participants. The data collection involved conducting semistructured interviews with 15 participants whose first childbirth occurred within the previous 18 months and who perceived their birth experience or their baby's arrival as traumatic.
Results
An interpretative phenomenological analysis was used to analyze the data. From the analysis, one core category was identified when birth turns from a happy event into trauma, along with three themes: (a) birth trauma, (b) experiences of obstetric mistreatment, and (c) unable to experience positive emotions.
Conclusion
This study explored mothers’ traumatic birth experiences and their emotional reactions, highlighting the need for better support and communication. The findings suggest that women should have the chance to share their childbirth experiences and should be assessed postpartum for signs of psychological distress. Implementing continuous, compassionate, and woman-centered care, involving partners, and understanding birth experiences can improve postnatal well-being. The findings suggest that midwives should focus on psychological health, with antenatal screening for birth-related fears, to identify at-risk women and tailor care to prevent trauma. Healthcare providers should prioritize continuous, woman-centered care as a vital part of organizational improvements to better address women's needs.
Keywords
Introduction
Pregnancy is a major landmark in a woman's life and heralds a time of happiness, anticipation, and making ready for the birth of a new family member. Women undergo a number of changes during pregnancy: physical, hormonal, and psychological (Watson et al., 2021). Birth trauma is the term used to describe the anguish a woman may experience both during and after giving birth (Keedle et al., 2022). It has been defined as the belief that there exists an “actual or threatened injury or death to the mother or her baby” (Beck & Watson, 2010). A number of factors are linked to traumatic birth, including obstetric complications, first-time birth, and emergency cesarean sections, alongside panic, lack of control, a negative assessment of earlier deliveries and healthcare professionals, interpersonal issues (Boorman et al., 2014; Wijma et al., 1997), medical intervention, and the type of birth (Ayers et al., 2016; Grekin & O'Hara, 2014; Modarres et al., 2012). Women who experience birth trauma may subsequently suffer from various mental health disorders, including posttraumatic stress disorder (PTSD), anxiety, postnatal depression, difficulties with postpartum bonding, and postpartum psychiatric disorders (Baldini et al., 2025; Keedle et al., 2022). PTSD is defined as a mental disorder that may develop after exposure to exceptionally threatening or horrifying events. However, many individuals demonstrate remarkable resilience and the ability to recover following such traumatic experiences (Bonanno, 2004).
Among the most common signs of traumatic childbirth are flashbacks, reliving some of the childbirth process, having nightmares, being unable to put the past behind, pushing aside memories of childbirth and anything connected with it, physical responses when being reminded of the pregnancy and the childbirth, rejection of sexual contact with one's partner, ignoring gynecological check-ups, mood swings, antagonism toward one's partner, stress, hostility, and disassociating from the environment (Byrne et al., 2017; Kranenburg et al., 2023). It is not unusual for women to experience mild or moderate fear of pregnancy: studies have found that 4% to 43% of women exhibit a degree of fear, while pregnant women overall have a pooled prevalence of 14% (O'Connell et al., 2017). The most common sources of fear are fear of the pain involved in giving birth, fear that one's body will be unable to survive labor, fear that the baby will be harmed, fear of the unknown, and fear that the pregnant woman will herself suffer harm (Slade et al., 2019). An extreme fear of pregnancy was first labeled tokophobia in the mid-to-late 1800s and defined as a high degree of fear of pregnancy and/or childbirth. The definition was subsequently modified to differentiate between primary and secondary conditions and to classify it as a symptom of depression (Slade et al., 2019). Primary tokophobia is the unhealthy fear of pregnancy in nulliparous women, whereas secondary tokophobia can arise after a traumatic birth, miscarriage, normal birth, stillbirth, or termination (Barton et al., 2024).
According to the World Health Organization (2024), maternal mental health must be considered a global health priority. It has been reported that 10% of pregnant women and 13% of new mothers suffer from an undiagnosed mental health disorder (World Health Organization, 2024). PTSD, which has a mid- and long-term impact on women's health, is among the most underdiagnosed but common mental health conditions (Vesel & Nickasch, 2015). PTSD is not limited to the perinatal period but can occur at the beginning of pregnancy and up to a year after childbirth (Ford et al., 2010; McKenzie-McHarg et al., 2015). Vision 2030 in Saudi Arabia emphasizes the importance of mental health as an essential component of overall well-being (Vision 2030 Kingdom of Saudi Arabia, n.d.); however, a gap remains in understanding how traumatic childbirth fits into the larger healthcare system, which this study seeks to address.
Review of Literature
Childbirth trauma has been defined as “Any event occurring during the delivery process that involves actual or threatened serious injury or death of the mother or her infant with the birthing woman experiencing intense fear, helplessness, loss of control, and horror” (Beck, 2004a, 2004b; Menage, 1993; Shiva et al., 2021).
In 2023, the total number of births in Saudi Arabian hospitals numbered 507,000, of which 60.3% were normal vaginal births, 36.7% were cesarean sections, and 2.95% were assisted births, including operative vaginal births, vaginal breech births, and other vaginal births outside the category of normal vaginal births (Ministry of Health, 2023). In total, 24.7% and 35.9% of Saudi women had experienced one or more mental health disorders in the preceding 12-month period and at least once during their lifetime, respectively. The most commonly reported 12-month and lifetime disorders were anxiety disorders, followed by mood disorders (Altwaijri et al., 2020).
A Saudi Arabian cross-sectional study carried out in Riyadh in 2020 found that 38.5% of the 174 women who took part reported having suffered from postpartum depression (PPD; Al Nasr et al., 2020). Furthermore, on the basis of data gathered from 279 Saudi women in 2022 during the postpartum period and 2 months after delivery, it was found that 32.8% had PPD (Alzahrani et al., 2022). Another study conducted in Riyadh in 2023, which included 187 women, set out to evaluate the prevalence of PPD and its linked factors and reported that 50.3% of the participants stated that they suffered from PPD a far higher figure than that of earlier studies (Aljaffer et al., 2023).
During the critical postpartum period, social support has a major impact on the physiological and psychological health of new mothers, who need the support of their partners and family members to avoid experiencing the “baby blues” and other postpartum complications that can threaten their health (Lefkovics et al., 2018; Wynter et al., 2014). Without this social support, new mothers can become stressed and anxious and start to feel incapable of fulfilling their maternal role (Weisman et al., 2010).
There is clear evidence to confirm that the psychological and emotional aspects of giving birth play a key role in determining women's overall birth experiences (Dixon et al., 2014; Olza et al., 2018). One of the major influences on how women feel during labor and birth is their interactions with intrapartum caregivers (Harris & Ayers, 2012; Oladapo et al., 2018). Several studies have examined the risks and protective factors associated with traumatic births. These studies have found that tokophobia, operative birth, and negative interactions with care providers are often contributing factors (Ayers et al., 2016; Soet et al., 2003). Martinez-Vázquez et al. (2021) determined that major protective factors include respecting the birth plan, continuity of care, and having skin-to-skin contact immediately after birth (Martinez-Vázquez et al., 2021). In addition, the quality of postnatal support received by women and their families after what is viewed as a traumatic birth can play a major role in determining whether a woman subsequently focuses on the distressing aspects of her experience of giving birth (Ayers et al., 2015).
Saudi Arabia's Vision 2030 and the Health Sector Transformation Program both set out ambitious goals designed to improve the country's healthcare services and highlight the importance of mental health and well-being (Vision 2030 Kingdom of Saudi Arabia, n.d.). Vision 2030 aims to improve citizens’ quality of life by emphasizing holistic health, of which mental health is a key component. The Health Sector Transformation Program supports this goal by focusing on modernizing the healthcare infrastructure, upgrading access to healthcare services, and raising the quality of care provided throughout the country. It is increasingly being acknowledged that addressing mental health issues and supporting mental well-being are important aspects of healthcare (Vision 2030 Kingdom of Saudi Arabia, n.d.).
At the time this study was conducted, there were no existing studies examining the experiences of mothers who have faced traumatic childbirth, particularly in the Middle East, and specifically in Saudi Arabia. This study aimed to investigate in detail the traumatic birth experiences of these mothers, as well as their perceptions of and reactions to such events.
Methods
Research Design
This study employed interpretative phenomenological analysis (IPA) to generate contextualized knowledge and novel insights into participant experiences (Smith et al., 2009). The data presented here were captured from in-depth face-to-face interviews with mothers. IPA emphasizes the importance of interpreting the data in the context of the individual's unique perspective and emphasizes the subjective meanings they attribute to their experiences. In this context, applying IPA aims to develop a rich and detailed account of the respondents’ experiences and gain insight into the challenges and expectations they have in managing their health conditions (Smith & Osborn, 2003). The central question guiding this research was as follows: “What are the experiences of the women who have suffered from traumatic births, and how do these experiences shape their health management?”
Population and Sampling
This study employed a purposive sampling method to recruit participants, which continued until no new ideas emerged in the interviews (n = 15). A key aspect of the study was the ethical treatment of the participants, and each participant provided written and verbal consent before their interview. The study's inclusion criteria were as follows: all participants were Saudi women aged 18 and older, with English fluency to understand the interview questions, and no pre-existing major medical conditions, who had recently delivered a full-term healthy or sick baby. Their first childbirth had occurred within the past 18 months, and they perceived their birth experience or their baby's arrival as traumatic; this timeframe was to allow for processing of the trauma to enable discussion around potential recovery, however, within recent memory. This study did not impose any exclusion criteria based on time, as women's memories of childbirth tend to remain vivid over the years (Simkin, 1992). They were selected from the largest government hospital in the eastern province of Saudi Arabia, which has a 450-bed capacity and more than 1,500 mothers visiting the antenatal clinic monthly, serving as a maternity and child hospital.
Data Collection
Participation in this study was entirely voluntary, and announcements were posted on hospital bulletin boards and sent to the target population via email. A word-of-mouth approach was also employed to aid recruitment. The sample size was determined using the data saturation approach, and data collection ceased when new individuals could not provide further insights into the phenomena (Al Nasr et al., 2020). Field notes were taken throughout the interview processes, and all interview data were compiled and analyzed until saturation was achieved. Each interview contributed to the overall understanding of the topic under study. Each participant was interviewed once between June 2024 and December 2024. To ensure the privacy and confidentiality of the information provided, each participant was interviewed separately. Before the interviews, it was crucial to ensure that the participants were at ease. The researchers verbally confirmed that the participants agreed to the requirements listed in the informed consent form. The participants were asked to provide their name, address, and phone number on a form before the interviews started, allowing the researcher to contact them if necessary. The interviews followed a semistructured format, with the researcher creating a set of questions and items to discuss (Table 1). The interview format was flexible and could be modified if needed (Weisman et al., 2010). This commitment to ethical research practices was paramount throughout the study.
Interview Guide.

The interviews took place in a counseling room in the hospital; only the researcher and the participant were present. The interview settings were chosen based on the environment in which participants felt most at ease, aiming to uncover the participants’ perspectives and obtain a greater perception of their experiences. The interviews lasted between 30 and 60 min. Audio equipment was also used to record the responses of the participants, as this method has been found to be the most accurate way to capture participants’ responses and ensure that no important information is missed. To elicit important information, probing questions based on the participants’ views were presented in the interview, including “Why?” “How?” or “What do you mean by this?”
Data Analysis
The interviews were transcribed verbatim from the audio recordings. The resulting written narratives varied in length, ranging from 10 to 12 pages, depending on each participant's unique experience. The interviews were conducted with the aid of specific research questions, ensuring focused and objective feedback. Revisions on the basis of initial interpretations were made as the interviews were analyzed and coded iteratively. Once the interviews were completed, they were transcribed, and an IPA was conducted. This analysis employed an idiographic and inductive approach to uncover the participants’ perspectives and gain a deeper understanding of their experiences. The idiographic method focuses on comprehending individual and distinct participants (Smith & Nizza, 2022). Table 2 outlines the steps involved in IPA, as proposed by Smith and Nizza (2022). Additionally, a qualitative research specialist was consulted to evaluate and validate the results and methods of analysis. The study is reported in accordance with the Consolidated Criteria for Reporting Qualitative Research (COREQ) checklist (Tong et al., 2007).
Step by Step to Conducting IPA.
Note. IPA = interpretative phenomenological analysis.
Trustworthiness
Four criteria were used to assess the quality of the data collected: credibility, dependability, confirmability, and transferability (Dixon et al., 2014). To ensure that the research had high credibility, the researchers worked with the interview subjects and asked for input on the transcripts. Dependability was ensured by verifying the results with the healthcare providers who were not part of the study. The participants were asked to confirm that the narratives had accurately expressed their real ideas and feelings in order to establish confirmability. Finally, to evaluate transferability, we looked at whether the findings could be applied to comparable populations, particularly those in another region of Saudi Arabia. The use of these techniques increased the rigor of the research findings. Reflexivity is essential for conducting high-quality, ethical research, as it establishes the credibility and validity of the research process (Cain et al., 2019). To uphold reflexivity, the authors have no connections to the selected hospital. Throughout the study, the authors consistently examined and discussed viewpoints and opinions, recognizing that beliefs, assumptions, and biases can influence thinking. The authors were acutely aware of the research roles, which guided the actions and decisions. To ensure rigor, the researchers remained grounded in the data, adopted a reflexive approach, and conducted intersubjective checks to minimize bias in the research outcomes (Newnham et al., 2021).
Ethical Considerations
This study was approved by the institutional review board Alahsa Health Cluster IRB MCH (No. H-05-HS-137) and King Saud University (Reference No. KSU-HE-24-570). The participants were fully informed about the study procedure and were given the opportunity to participate voluntarily, with the reminder of their right to withdraw at any time without any consequence. They were assured that their responses would be kept confidential and only accessible to the researchers in this study. To maintain confidentiality, participants were assigned codes to use instead of their names. Finally, all participants agreed to be audio recorded, and they were assured that all responses and transcripts would be securely destroyed. Informed consent was obtained from all participants. Lastly, Standards for Reporting Qualitative Research guidelines, which are a unified set of criteria for reporting qualitative research, were applied.
Results
Sample Characteristics
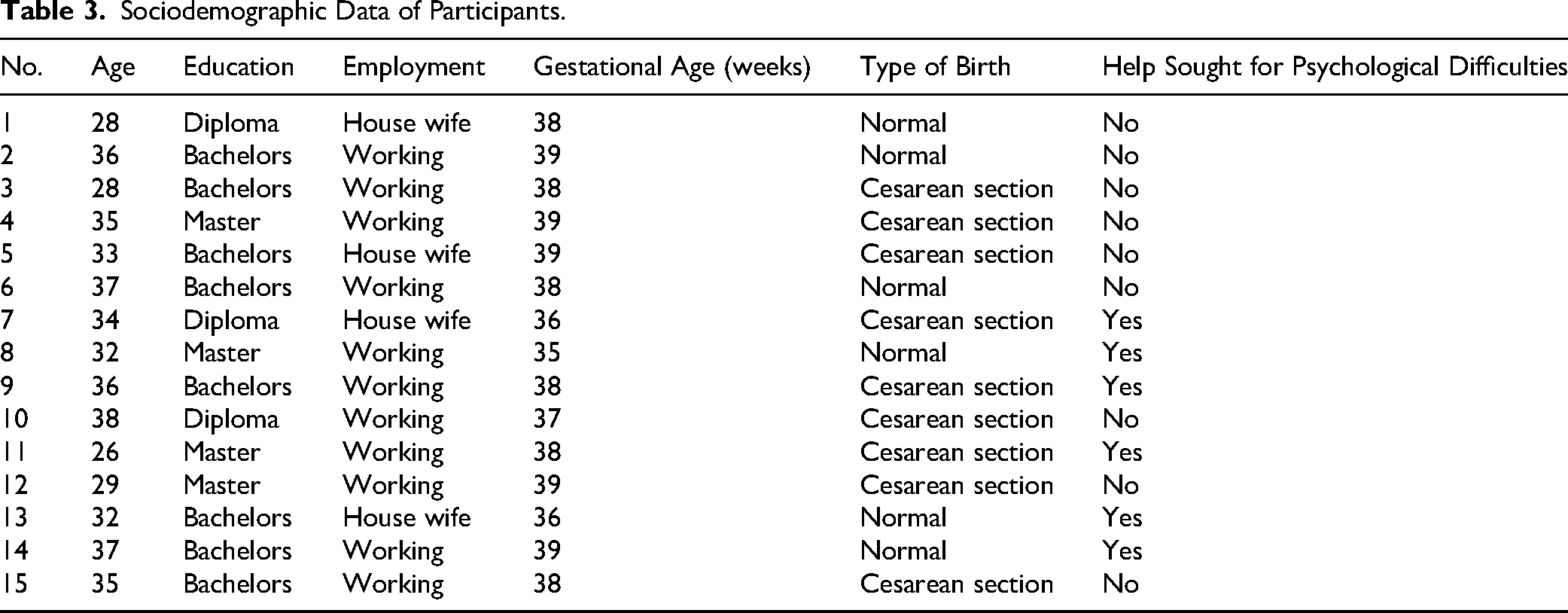
Fifteen postpartum women were included, with an average age of 33 years, and the majority were working (73%; n = 11). All the women who consented to participate in the interview sessions characterized their childbirth as traumatic. A significant 40% (n = 6) of the women had sought professional help for psychological difficulties, reinforcing the significant impact of their trauma. Additionally, 80% of the newborns were full-term, and most of the sample had a cesarean birth (60%). It is worth noting the diverse educational backgrounds of the participants, with 53% (n = 8) holding a bachelor's degree, as shown in Table 3.
Sociodemographic Data of Participants.
Findings from the Semistructured Interviews
The group's experiential themes can all be placed in the core category of “When birth turns from a happy event into trauma,” illustrating how women's childbirth experiences can shift from joyful milestones to sources of emotional distress. This transformation shows how unexpected challenges and negative interactions during childbirth can profoundly impact women's emotional well-being, turning what should be a joyous occasion into a traumatic event.
After the data analysis had been performed and the themes had been developed, three key themes associated with the research questions and focal points of this study were identified, as presented in Table 4. These three themes were revealed during the interpretative analysis of the transcribed interviews and are presented below alongside relevant contextual information that supports them.
Core Category with Themes and Subthemes.

Core Category: When Birth Turns from a Happy Event into Trauma
A detailed examination of the participant interviews enabled the researchers to make thematic conclusions, which are presented in detail below. The participants’ experiences are emphasized to support the outlined themes, using direct quotes representative of the experiential comments.
Theme 1. Birth Trauma
Women experienced traumatic births with emergency cesarean sections, severe tears, and little postpartum support. Hospital policies and lack of support deepened their trauma, affecting their emotional well-being and future pregnancies. The participants shared various traumatic childbirth experiences. Several women experienced emergency cesarean sections due to fetal distress or abnormal fetal conditions, leading to feelings of shock and fear. Others endured severe tears and inadequate postpartum support, which impacted their physical recovery and bonding with their babies. Hospital policies and lack of support further exacerbated their trauma, leaving lasting emotional scars and deep concerns about future pregnancies
This theme included three subthemes: traumatic childbirth experience, painful childbirth experience, and shocking news.
Traumatic Childbirth Experience. Several women experienced traumatic childbirth during emergency cesarean sections due to fetal distress, as several participants discussed: I endured three days of labor induction, and after those three days, the doctor informed me that my pelvis was too narrow when my baby experienced fetal distress. I was then taken to the operating room for a cesarean section. (Woman 1) During childbirth, it was traumatic to me. I suffered from severe tears, which caused my hemoglobin levels to drop, leading to the need for a blood transfusion. Because of this, I was unable to see my baby, hold her, or place her on my chest. (Woman 4) When my baby was born, her skin was bluish, and I did not hear her cry. At that moment, I knew that something was wrong with her health. She was then admitted to the intensive care unit for seven days, and I was not allowed to hold her. I was traumatized that I had to care for myself alone after a cesarean section. (Woman 5)
Painful Childbirth Experience. Some participants described their childbirth as painful and traumatic, particularly in cases involving congenital abnormalities or the loss of their baby. Example comments follow: I endured a painful journey throughout my pregnancy and delivery. My baby was diagnosed with congenital abnormalities during pregnancy. When I first received this news, I was physically, mentally exhausted. (Woman 6) This birth was one of the most painful experiences of my life. I can’t bring myself to go through pregnancy again. I no longer want to have children. I am mentally and physically exhausted. (Woman 9) My birth experience was incredibly painful, both physically and emotionally. It took me a long time to recover from the pain [with] difficulty sitting and bathroom struggles. (Woman 12)
Shocking News. Some women shared devastating news about losing their babies shortly after birth, describing their shock and inability to comprehend the loss. Example responses are as follows: Two days after birth, the pediatrician gave me devastating news—he told me that my baby would not live for long. He advised me to take her home because her time was limited. Just two hours after we arrived home, my baby passed away. I could not comprehend what had happened. (Woman 6) I was given the devastating news—my baby did not survive. The shock hit me like a storm. I couldn’t process what was happening. Was this real? Was I dreaming. (Woman 9)
Theme 2. Experiences of Obstetric Mistreatment
The second theme highlights the perception of obstetric mistreatment, harsh staff behavior, and miscommunications during childbirth. They felt their birth plans were ignored, leading to emergency cesareans and negative experiences. Several women reported that medical decisions led to severe complications, often caused by experiences obstetric mistreatment. Complaints about staff behavior were prominent, with reports of harsh and violent interactions, including yelling and forcing procedures. Many women felt they were misinformed. Additionally, numerous women expressed disappointment that their birth plans were not followed, often resulting in emergency cesareans and a sense that their wishes and expectations were ignored.
This theme included five subthemes: medical intervention, feeling neglected, staff behavior, feelings of being misinformed, and birth plan compliance.
Medical Intervention. Some women reported that medical interventions and obstetric decisions caused severe complications, pain, and long-term health issues.as several participants discussed: The medical interventions and decisions made by the doctors and staff led to severe complications, intense pain, and prolonged suffering for nearly six months after childbirth. (Woman 2) She suggested a C-section to speed up the process. I initially refused, but as the pain intensified, I called for the doctor and asked to have a C-section. By then, I was 7 cm dilated. (Woman 15)
Feeling Neglected. Many women felt unsupported during pregnancy and childbirth, relying on husbands who were often unprepared or unable to provide proper support. This left them feeling vulnerable and overwhelmed as most of the participants shared: The presence of my husband after birth was also essential. I suffered both physically and emotionally on my own, and they did not allow my husband to be by my side to help me move and cope with the pain. (Woman 1) To make matters worse, my husband was out of the country, and I had no support. I struggled to care for my newborn while barely being able to sit down. (Woman 12)
Staff Behavior. Many women experienced poor, harsh, and dismissive behavior from medical staff, feeling ignored, shouted at, or forced into procedures, worsening their distress, as some participants reflected: I entered the delivery room with a well-thought-out birth plan, but as labor began, everything changed. The behavior of the medical staff, including doctors and midwives, was extremely poor. (Woman 4) I tried to push, but I couldn’t. The midwife started yelling at me and forcing me to push, but I was unable to do so. (Woman 2)
Feelings of Being Misinformed. Many women felt unprepared and uninformed during childbirth, with unclear communication and sudden moves to the operating room, as some women highlighted: Suddenly, she brought out a hook-like tool and broke my water without informing me beforehand. I then heard her shouting and calling the nurses, telling them that the umbilical cord had prolapsed. (Woman 14) Without informing me or explaining anything, the doctor used a vacuum to extract my baby. I heard the medical team saying that I needed stitches due to a severe tear and excessive bleeding. I had suffered a third-degree tear that extended to my rectum and was taken to the operating room for suturing. (Woman 2)
Birth Plan Compliance. Many women's expectations of a positive birth were changed by emergencies and complications, leading to trauma, pain, and disrupted birth plans as many women discussed: My birth plan changed from a positive birth experience to one filled with suffering and prolonged pain. The trauma was deeply painful for me. (Woman 2)
Theme 3. Unable to Experience Positive Emotions
The third theme captures the profound emotional distress experienced by participants during and after childbirth. Many women reported feeling overwhelmed by fear for their own safety, the condition of their babies, and the uncertainties of labor. Feelings of loneliness and emotional exhaustion were particularly acute when they were left alone in the operating room or without support from their husbands and family. Several participants described crying, screaming, and experiencing emotional shock, struggling to cope with the trauma. For some, these experiences contributed to PPD, requiring medical intervention and long-term mental health support. Overall, the childbirth experiences left many women deeply wounded, both physically and mentally, with lasting impacts on their well-being, highlighting the emotional exhaustion and vulnerability inherent in such traumatic experiences.
This theme included three subthemes: mother's fear and anxiety, emotional exhaustion, and PPD.
Mother's Fear and Anxiety. Women felt intense fear, anxiety, and emotional exhaustion during childbirth, often without support. Many experienced tears, PPD, and lasting emotional and physical scars. This was highlighted by most of the women: At that moment, all I felt was fear and anxiety about what would happen to me and my baby. Would everything turn out fine or not? (Woman 1) I overheard them saying that my baby was in danger. At that moment, I broke down emotionally and started crying out of anxiety and fear. (Woman 14)
Emotional Exhaustion. Many women experienced emotional shock after childbirth, with feelings of grief, nerves, and loss of appetite, as most of the participants stated: I could not overcome my emotional shock. I was unable to eat or drink for four days; I had no appetite whatsoever. The experience left me deeply shaken. (Woman 7) My baby was gone. The child I had carried and fought for over 35 weeks was taken from me. I couldn’t control my emotions. I could still hear his voice in my mind, even when I closed my eyes. I couldn’t sleep. I couldn’t calm down. (Woman 9)
Postpartum Depression. Many women developed PPD after traumatic childbirths involving separation, pain, and emotional distress. They sought medical help and antidepressants, but depression often lasted months, causing shock and reluctance about future pregnancies, as most of the participants shared: I experienced postpartum depression and needed consultations with a psychiatrist and medication to cope with the trauma and depression I had endured. (Woman 7) Ahh … it hurts to even recall this story. It was a painful, heartbreaking birth. I developed postpartum depression, sought psychiatric help, and took medication. (Woman 13)
Discussion
The authors used an interpretative phenomenology research design to explore mothers’ traumatic birth experiences and their perceptions of and reactions to such events. The findings include a core category of when birth turns from a happy event into trauma with three themes: (a) birth trauma, (b) experiences of obstetric mistreatment, and (c) unable to experience positive emotions. The analysis yielded themes that provide insight into the importance of maternity care providers being aware of the risk factors for traumatic birth for women in Saudi Arabia.
The birth trauma shared by the participants was a central finding in this study. The findings show that the participants, with immense courage, shared various traumatic childbirth experiences that impacted their physical recovery and bonding with their babies. Hospital policies, lack of support, and restrictions further exacerbated their trauma, leaving lasting emotional scars and deep concerns about future pregnancies.
The birth trauma theme encompassed three subthemes: traumatic childbirth experiences, painful childbirth experiences, and shocking news. These findings align with previous research. Participants in earlier studies reported traumatic births, and factors associated with reporting birth as traumatic included a history of depression, induction of labor, instrumental deliveries, and postpartum hemorrhage (Nagle et al., 2022). In their literature review study, Simpson and Catling (2016) reported that risk factors included obstetric emergencies and neonatal complications; poor quality of provider interactions was identified as a significant risk factor for experiencing birth trauma. This reflects the findings of Nagle et al. (2022), who identified a prevalence of 18% of women experiencing birth as traumatic. Furthermore, an important feature of traumatic childbirth is the mother's perception of the traumatic event, which is defined by the feeling of fear about or the threat of severe damage to the mother or infant and/or their death during labor (Abdollahpour & Khadivzadeh, 2022; Beck, 2004a, 2004b; Kleiman & Wenzel, 2013). On the other hand, one study showed that some women who experience a traumatic birth do not necessarily have adverse physical or psychological outcomes (Elmir et al., 2010).
Experiences of obstetric mistreatment emerged as the second key theme. This highlights the perception of mistreatment and negative experiences associated with medical interventions during childbirth. Complaints about staff behavior were prominent, with reports of harsh, disrespectful, and violent interactions, including yelling, forcing procedures, and neglecting mothers’ emotional needs. Many participants felt they were misinformed or not informed at all about their treatment or what was happening, which heightened their trauma. This theme included five subthemes: medical intervention, feeling neglected, staff behavior, feelings of being misinformed, and birth plan compliance. This finding aligns with national research by Alghamdi et al. (2023), which shows that women who gave birth in the Kingdom of Saudi Arabia perceived their care as less respectful than those giving birth in Canada and the United States. The finding that having a traumatic birth can be linked to having a medicalized birth is not surprising, as it aligns with previous research by Kjerulff and Brubaker (2018), who found that women who had an unplanned cesarean delivery had negative feelings overall about their childbirth. This underscores the importance of respectful and humane treatment during childbirth, a responsibility that all healthcare professionals should be committed to. This study findings reflect the findings of Beck (2004a, 2004b, 2013), who explored the perceptions of mothers who perceived childbirth as a stressful event for various reasons, such as inadequate support, lack of respect and human dignity, and a sense of helplessness. Additionally, Zedan (2025) reports that women in the Middle East find giving birth stressful, with high rates of anxiety, trauma, and PTSD symptoms influenced by maternity care issues, which affect their perceptions and satisfaction with labor and birth experiences.
The inability to experience positive emotions emerged as the third key theme. The participants in this study reported profound fear and anxiety during childbirth. Several women described crying, screaming, and struggling to cope with the trauma. Others shared that they developed PPD, experiencing long-lasting emotional and physical distress, some requiring medication and mental health support. This theme included three subthemes: mothers’ fear and anxiety, emotional exhaustion, and PPD. This finding is consistent with Ertan et al. (2021), who found that childbirth experiences could be complicated and traumatic. Similarly, Shiva et al. (2021) emphasized that a negative childbirth experience has been associated with depression in the postpartum period. A study conducted in Saudi Arabia determined the prevalence of PPD in Riyadh and found a significant association between the occurrence of PPD and an unsupportive spouse, especially in those women with recent stressful life events, such as negative childbirth experiences (Al Nasr et al., 2020). These findings underscore the need for better support systems for mothers during and after childbirth, motivating us to be proactive in improving maternity care.
To understand the culture and context of maternity care in Saudi Arabia, it is important to note that the healthcare system is divided into two sectors: government hospitals, which are part of the public healthcare system overseen by the Ministry of Health, and private hospitals, which operate as for-profit entities with self-employed practitioners. Consequently, the competing nature of private and publicly governed healthcare has resulted in differing dynamics, information, and performance in the provision of care (Basu et al., 2012). Government hospitals, for example, provide maternity care services free of charge, while private hospitals charge pregnant women either by requesting cash payments or through private insurance schemes. Variations in women's experiences during childbirth between government and private hospitals have also been highlighted in previous international studies, suggesting that although private healthcare is more patient-/client-focused, health outcomes are often better in government hospitals (Hussain et al., 2020).
Taken together, the group of experiential themes can be categorized under the core category when birth turns from a happy event into trauma, women's experiences during childbirth are often impacted by birth trauma. This trauma can be caused by traumatic childbirth experience, painful childbirth, and shocking news; and by experiences of obstetric mistreatment, including medical interventions, feelings of neglect, staff behavior, misinformation, and noncompliance with birth plans. Such experiences can profoundly affect women's emotional well-being, leading to fears, anxiety, emotional exhaustion, and PPD as shown in Figure 1.

Women's perceptions of living a traumatic childbirth experience.
This study highlights the importance of offering high-quality intrapartum care, as well as respectful maternity care, to make sure that women have a positive experience of childbirth. It is essential for maternity care providers to be aware of the risks associated with traumatic births. Implementing a trauma-informed approach by midwives and maternity care providers during the postpartum period will help them identify emerging or already evident symptoms of maternal trauma. Women who are already experiencing subclinical postpartum symptoms of PTSD could benefit from undergoing a thorough investigation and diagnosis at a later point, potentially 6 weeks postpartum. In addition, Saudi Arabia's maternity services should provide ongoing support for women who have experienced birth trauma.
Strengths and Limitations of the Study
The study investigates women's perspectives on their traumatic birth experiences through qualitative interviews, aiming to uncover deep insights into their feelings and reactions. While this approach captures detailed personal meanings, it may involve subjectivity and interpretation biases. To reduce bias, women from diverse backgrounds were included, though the limited geographic scope remains a potential limitation. Further, as a qualitative study, our findings are based on participants’ perceptions and interpretations rather than statistical analysis; also, this study may not be universally generalizable due to its single-hospital focus. Moreover, while all participants consented to participate in the study, some expressed hesitation about sharing their thoughts and being recorded. We assured them that their responses would be kept confidential and accessible only to the research team, and that all data would be permanently deleted upon the study's completion, ensuring their privacy and respect.
Implications for Practice
Current findings recommend that the Saudi Ministry of Health must adopt respectful and supportive intrapartum care to ensure positive childbirth experiences. Midwives should concentrate on optimizing both maternal and infant health. This includes screening for tokophobia and birth-related anxiety during antenatal visits, which can help identify women at risk and allow for personalized care. Since many women struggle to discuss traumatic birth experiences, midwives should actively provide emotional support by asking open-ended questions and practicing empathetic listening. During labor, midwives should monitor for signs of excessive fear, irritability, frustration, and anger to enable early intervention. Continuous emotional support during labor and appropriate psychological follow-up after childbirth are vital. Tailored postpartum support is essential, considering the educational diversity among women. They should be allowed to discuss their birth experiences and be assessed during the postnatal period for signs of psychological distress to promote healing. Healthcare providers need training in understanding birth trauma, trauma-informed communication, and supportive care practices. Additionally, services should take into account women's coping styles and strengths, incorporating these into therapeutic approaches to promote recovery and foster posttraumatic growth.
Future Directions for Research
Very little quantitative evidence exists in Saudi Arabia on the effectiveness of debriefing and counseling interventions designed to assist women who experience traumatic births. Research should specifically investigate whether postpartum PTSD varies in terms of symptoms, progression, and duration compared to PTSD from other traumatic events. Additionally, studies should compare and contrast PPD and PTSD following childbirth to better understand their relationship and distinctions.
Conclusions
The research explores mothers’ traumatic birth experiences and their emotional responses, emphasizing the lasting psychological impact. It highlights the need for ongoing mental health support and better opportunities for women to voice their concerns. The study underscores the importance of a woman-centered approach, compassionate communication, and involving partners in postpartum care to improve emotional well-being and reduce long-term effects of childbirth trauma.
Supplemental Material
sj-docx-1-son-10.1177_23779608261417795 - Supplemental material for When Birth Turns from a Happy Event into Trauma: An Interpretative Phenomenological Analysis of Women's Perceptions of Living a Traumatic Childbirth Experience
Supplemental material, sj-docx-1-son-10.1177_23779608261417795 for When Birth Turns from a Happy Event into Trauma: An Interpretative Phenomenological Analysis of Women's Perceptions of Living a Traumatic Childbirth Experience by Anwar Nader AlKhunaizi, Areej Ghalib Al-Otaibi, Amani Alabdullah, Hibah Abdulrahim Bahri, Sarah Abdulaziz AlAbdalhai, Kholoud Mohammed Alhaji, Manal Awn Alharthi and Meral Jehad Al Zayer in SAGE Open Nursing
Supplemental Material
sj-docx-2-son-10.1177_23779608261417795 - Supplemental material for When Birth Turns from a Happy Event into Trauma: An Interpretative Phenomenological Analysis of Women's Perceptions of Living a Traumatic Childbirth Experience
Supplemental material, sj-docx-2-son-10.1177_23779608261417795 for When Birth Turns from a Happy Event into Trauma: An Interpretative Phenomenological Analysis of Women's Perceptions of Living a Traumatic Childbirth Experience by Anwar Nader AlKhunaizi, Areej Ghalib Al-Otaibi, Amani Alabdullah, Hibah Abdulrahim Bahri, Sarah Abdulaziz AlAbdalhai, Kholoud Mohammed Alhaji, Manal Awn Alharthi and Meral Jehad Al Zayer in SAGE Open Nursing
Footnotes
Acknowledgment
The authors extend their appreciation to the Deanship of Scientific Research through the Research Center at College of Nursing, King Saud University, for logistically supporting this study.
Ethical Considerations
This study was approved by the institutional review board Alahsa Health Cluster IRB MCH (No. H-05-HS-137) and King Saud University (Reference No. KSU-HE-24-570). The participants were fully informed about the study procedure and were given the opportunity to participate voluntarily, with the reminder of their right to withdraw at any time without any consequence. They were assured that their responses would be kept confidential and only accessible to the researchers in this study. To maintain confidentiality, participants were assigned codes to use instead of their names. Finally, all participants agreed to be audio recorded, and they were assured that all responses and transcripts would be securely destroyed. Informed consent was obtained from all participants. Lastly, Standards for Reporting Qualitative Research guidelines, which are a unified set of criteria for reporting qualitative research, were applied.
Consent for Publication
Participants gave their informed written consent for their data to be coded for analysis, and for certain anonymous citations to be included in the publication, while respecting their confidentiality.
Author Contributions
Conceptualization: ANA and AGA-O; methodology: ANA, AGA-O, and AAB; validation: AAB, HAB, and MAA; formal analysis: ANA and MJZ; investigation: ANA; resources: KMA, MJZ, and SAA; data curation: ANA and SAA; writing—original draft preparation: ANA and AGA-O; writing—review and editing: AAB, HAB, and KMA; visualization: AGA-O and MAA; supervision: ANA. All authors guarantee the integrity of the content and the study. All authors have read and agreed to the published version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of Data and Materials
In order to protect the privacy of participants, the individual dataset generated in this study is not publicly available. However, the final transcripts for data analysis are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.