
Abstract
Introduction
Catheter-associated urinary tract infections (CAUTIs) remain a major healthcare-associated concern despite being largely preventable. They contribute to prolonged hospital stays, increased antimicrobial resistance, and higher healthcare costs.
Objective
This study evaluated the effectiveness of a structured CAUTI prevention bundle combined with a nursing empowerment program in a tertiary care hospital in Makkah, Saudi Arabia. The objective was to update evidence-based practices, improve compliance with urinary catheter insertion and maintenance protocols, and enable nurses to independently discontinue catheters without a documented clinical indication.
Methods
Conducted between October 2023 and May 2024, the prospective single-arm intervention included 247 adult patients requiring indwelling urinary catheters across medical, surgical, and neurosurgical wards. CAUTI rates were measured according to CDC/NHSN (Centers for Disease Control and Prevention/National Healthcare Safety Network) criteria, and bundle compliance was monitored using standardized audits.
Results
The intervention led to a 73% reduction in CAUTI incidence, from 5.4 to 1.41 per 1,000 catheter-days. Nursing compliance improved markedly, rising from 56% to 93%, while catheter utilization remained stable. Additionally, the average catheter days per patient decreased by 41%.
Conclusion
These findings highlight the critical impact of structured protocols and nursing empowerment on reducing infection rates and enhancing clinical efficiency. The results support broader implementation of similar strategies in alignment with Saudi Vision 2030's healthcare improvement goals.
Introduction
Catheter-associated urinary tract infections (CAUTIs) represent a significant share of Healthcare-Associated Infection (HAIs), resulting in adverse clinical outcomes, prolonged hospitalization, rising antimicrobial resistance, and escalating healthcare costs. Although largely preventable, CAUTIs continue to pose a serious threat to patient safety (Rubi et al., 2022; Werneburg, 2022). According to Centers for Disease Control and Prevention (CDC) estimates, approximately 75% of nosocomial urinary tract infections are attributable to the use of urinary catheters. Moreover, an estimated 12% to 16% of hospitalized adults require an indwelling urinary catheter, with the risk of developing a CAUTI increasing by roughly 3% to 7% for each additional day the catheter remains in place (Centers for Disease & Prevention, 2025).
The prevalence and burden of CAUTIs remain considerable, especially in intensive care units (ICUs), where invasive devices are frequently utilized (Sleziak et al., 2025; Yajun et al., 2025). Across the globe, healthcare systems are increasingly adopting structured, evidence-based strategies like care bundles to minimize infection risks and enhance consistency in clinical practice. Each bundle consists of a concise set of targeted interventions designed to address the needs of specific patient populations and care settings. When implemented collectively and consistently, these interventions lead to significantly better patient outcomes than when applied individually (Ruscitti & Puro, L'utilizzo dei bundle nella pratica clinica./2008; Sebastiani et al., 2024).
Literature Review
In the context of preventing CAUTIs, care bundles typically include aseptic catheter insertion techniques, selection of appropriate catheter materials, daily assessment of catheter necessity, rapid removal of unnecessary catheters, and strong adherence to hand hygiene and maintenance protocols (Huang et al., 2025; Rosenthal et al., 2025). Clarke et al. reported a substantial reduction in CAUTI rates from 5.2 to 1.5 per 1,000 catheter-days following the implementation of a care bundle comprising four low-cost, evidence-based practices. These include use of silver-alloy catheters, catheter stabilization, prevention of tubing-floor contact, and early postoperative removal (Clarke et al., 2013). This model has since been widely recognized for its cost-effectiveness and sustainability, providing a foundation for care bundle design across diverse healthcare systems.
The Saudi Ministry of Health has addressed the growing need for CAUTI prevention through strategic national initiatives, including the “CAUTI out of nation” (CAUTIoN) project. The initiative has shown encouraging results, with a recent study reporting a 3.6 percentage point reduction in CAUTI rates across national healthcare facilities from mid-2022 to early 2024 (Aldalbehi et al., 2025). A 6-year surveillance study conducted across six hospitals in Saudi Arabia, Bahrain, and Oman reported an overall CAUTI rate of 3.2 per 1,000 catheter-days, with a catheter utilization ratio of 0.78. Despite achieving an approximate 80% reduction in CAUTI rates over the study period, adherence to catheter care bundles remained limited, with a compliance rate of only 65%. When benchmarked internationally, CAUTI rates in the Gulf Cooperation Council (GCC) hospitals were 32% higher than those reported by the U.S. National Healthcare Safety Network (NHSN), yet 39% lower than rates documented by the International Nosocomial Infection Control Consortium (INICC) (Al Nasser et al., 2016), indicating both challenges and progress in regional infection control practices.
Critically, the success of any care bundle is heavily reliant on nursing empowerment, as nurses are the primary providers responsible for catheter insertion, maintenance, monitoring, and patient education. Empowered nursing teams supported through continuous education, decision-making authority, interdisciplinary collaboration, and accountability frameworks are more likely to adhere to bundle protocols and proactively identify deviations from best practice (Saade et al., 2024; Zhang et al., 2024). Supporting this, a quality improvement project by Yatim et al. in Singapore demonstrated that a nurse-driven catheter removal protocol reduced CAUTI rates from 4 to 0 per 1,000 catheter-days over 6 months, despite a slight increase in catheter use. Staff compliance with the protocol reached 89%, underscoring the effectiveness of nurse-led interventions in enhancing patient safety (Yatim et al., 2016).
Despite the wealth of international and national evidence, consistent implementation of CAUTI prevention strategies remains a challenge due to variable training, resource limitations, and institutional cultures (Al Nasser et al., 2016; Aldalbehi et al., 2025; DePuccio et al., 2020; Werneburg, 2022). While several Saudi hospitals have independently adopted care bundles, data-driven evaluations of their cumulative impact, particularly when integrated with structured nursing empowerment programs remain limited. Bridging this gap is essential for developing scalable and sustainable models for healthcare quality and patient safety.
To address this issue, this study aims to assess the combined impact of prevention care bundles and nursing empowerment on CAUTI rates in a large tertiary hospital in Saudi Arabia by evaluating local outcomes within the broader context of international best practices.
Methods
Study Design and Setting
This pilot prospective, single-arm, open-label study was conducted to assess the effectiveness of an updated CAUTI prevention care bundle in lowering infection rates compared to standard routine care. The study was conducted from October 2023 to May 2024 at a government tertiary hospital, Makkah, Saudi Arabia, with a capacity of over 500 inpatients bed and 40 emergency department beds. The hospital was staffed by more than 300 registered nurses (RNs) working in adult care units. These nurses had qualifications such as bachelor's degree in nursing and had relevant clinical experience. The majority of patients admitted during the study period presented with multiple comorbidities, including diabetes, hypertension, peripheral vascular disease, neurological disorders, heart failure, and those requiring dialysis.
Catheters were inserted in various adult care units, including general medical (52%), surgical (35%), extended care (8%), and neurosurgical wards (5%). The total study duration was 7 months, 1 month was allocated for training RNs on the updated CAUTI prevention bundle, followed by 6 months dedicated to implementation and CAUTI incidence data collection.
Baseline Information
Baseline data were obtained retrospectively from the hospital's Nursing Quality Indicator records over a 6-month period (January–June 2023) preceding the intervention. These records consist of aggregate indicators used for internal hospital quality monitoring and do not include individual patient-level demographic or clinical information. As a result, potential confounding variables could not be controlled in the baseline analysis. During this pre-intervention period, the average CAUTI incidence was 5.4 per 1,000 catheter-days. This rate served as the benchmark for evaluating the effectiveness of the bundle intervention introduced in the study. Notably, this rate was significantly higher than the NHSN and national CAUTI benchmarks (Aldecoa et al., 2022).
Inclusion and Exclusion Criteria
All patients admitted to adult care units including general medical, surgical, extended care, and neurosurgical wards, who had urinary catheters, were included in the study, with no exclusions.
Procedure
Following ethical approval, an authorization letter from the nursing administration was distributed to all clinical nursing directors. Investigators conducted daily visits to each ward to screen, recruit participants, and collect data. All patients were followed during the study period (6 months), or until discharge or death, whichever occurred first.
Since the intervention required full adoption by the selected wards, RNs in the intervention group were educated on the CAUTI prevention bundle through in-service sessions, meetings, and one-on-one bedside training provided by the investigators. The education and training program employed multiple strategies, including detailed explanations of each bundle component, the supporting evidence base, and demonstrations of proper catheter insertion and maintenance techniques during in-service training. Moreover, consultation and clarification with the investigators continued throughout the study. This program was provided extensively in the first month of the study period.
To assess the accuracy of implementation and identify any deviations, spot checks were conducted collaboratively by investigators and head nurses during daily ward visits. These evaluations used a standardized CAUTI prevention bundle checklist audit tool, which included all components of the bundle, including both insertion and maintenance elements. Each patient was monitored for a total of 24 h during their hospital stay, either continuously or in intervals across different shifts, to capture variations in practice. Catheter insertion was performed by physicians, while maintenance was the responsibility of the nursing staff. Maintenance indicators were jointly supervised by the head nurses and investigators and were assessed every 12 h to ensure adherence. Compliance was determined using an all-or-none approach. Failure to meet even one bundle component was classified as noncompliant. The incidence rate of CAUTI was recorded by investigators in collaboration with infection control practitioners, who also contributed to ongoing outcome monitoring. In addition, monthly audit data served as a group-level compliance indicator. Furthermore, a root-cause analysis was performed for each new CAUTI event to identify contributing factors. This structured, multidisciplinary approach ensured consistent oversight of clinical practice and infection prevention throughout the study.
Modified CAUTI Prevention Bundle
The CAUTI prevention bundle was developed to reduce CAUTI incidence, be practical for RNs to implement, and empower them to remove urinary catheters unless clinically indicated. The intervention comprised a set of evidence-based practices derived from guidelines issued by the CDC and the General Directorate of Infection Prevention and Control under Saudi Arabia's Ministry of Health (Centers for Disease & Prevention, 2025; Ministry of Health & Control in Healthcare, 2025).
In addition to the essential practice of timely removal of indwelling urinary catheters, the literature also highlights the effectiveness of strategies such as automatic stop orders after 72 h, daily reviews, mandatory renewal with documented indications, and reminders, all of which have been shown to reduce catheter duration and CAUTI rates (Gupta et al., 2023; Meddings et al., 2010; Saint et al., 2013). Specifically, in our study, the 72h interval served as a defined checkpoint for nursing staff to assess the continued need for catheterization. While physicians may update or discontinue catheter orders at any time based on clinical need, nurses are authorized, under the protocol, to remove the catheter if no renewed physician order is present after 72 h. This structured review empowers nurses and ensures catheter use remains clinically justified.
These measures were implemented in tandem with the CAUTI prevention bundle. A multidisciplinary team including nurses, physicians, infection control practitioners, and quality improvement professionals was involved in modifying the bundle and adapting it to the context of adult care units.
The Intervention
Pre-insertion phase— CAUTI prevention (CAP)
► Verify the physician's order: Ensure the order includes catheter type, size, and indication. ► Assess clinical necessity: Evaluate if catheterization is medically justified based on the patient's current condition. ► Prepare the patient: Collect supplies and clearly explain the procedure to the patient.
Insertion phase—CATHETER INSERTION
► Competent staff only: Catheterization must be performed by trained personnel. ► Aseptic hand hygiene before procedure: Perform proper hand hygiene before starting. ► Thorough perineal cleaning: Clean perineal area with sterile or antiseptic solution. ► Handle sterile equipment only: Use sterile catheters and insertion tools. ► Use sterile gloves: Wear sterile gloves throughout the procedure. ► Apply topical sterile lubricant: Use a sterile, single-use lubricant. ► Establish a closed drainage system: Attach a sterile closed drainage system. ► Position drainage bag correctly: Place the drainage bag below bladder level and ensure it does not touch the floor. ► Secure catheter to prevent movement: Immobilize the catheter by securing it to the patient's thigh to prevent trauma. ► Perform hand hygiene after procedure: Wash hands thoroughly after completing the procedure.
Maintenance phase—SECURE FLOW
► Secure the catheter: Prevent movement and urethral trauma. ► Evaluate daily need: Review whether catheter is still indicated. ► Maintain a closed system: Do not disconnect the catheter unless clinically necessary. ► Use personal protective equipment (PPE) and clean hands thoroughly before contact: Follow infection control protocols. ► Remove PPE and hand hygiene after handling: Ensure safety postprocedure. ► Elevate hygiene standards (meatal care): Provide daily perineal and meatal care. ► Ensure unobstructed flow: Check tubing for kinks and verify proper drainage. ► Position drainage bag below bladder: Ensure the bag is correctly placed. ► Use one container per patient when emptying: Prevent cross-contamination. ► Monitor and empty drainage bag regularly: Watch output closely and document as needed.
Catheter removal phase—REMOVE
► Review catheters order every 72 h: Ensure a renewed physician order exists. ► Establish communication with the physician: Inform the physician if renewal is due. ► Monitor documentation: Check for timely updates and accuracy in patient records. ► If no order renewal, prepare for removal: Initiate removal process if no valid order is present. ► Verify patient readiness and educate: Ensure clinical stability and explain the procedure to the patient. ► Execute safe removal procedure: Follow aseptic technique and document the catheter removal properly.
Measurements
The primary outcome measure of this study is the rate of CAUTIs, as defined by the CDC criteria. A CAUTI is characterized as the development of infection in individuals who have had an indwelling urinary catheter in place for over two consecutive days and exhibit at least one clinical sign or symptom indicative of infection, such as fever exceeding 38°C, suprapubic tenderness, costovertebral angle pain or tenderness, urinary urgency, increased frequency, or dysuria. Confirmation of the diagnosis requires a urine culture yielding no more than two microbial species, with at least one being a bacterial organism present at a concentration of 10⁵ colony-forming units per milliliter (CFU/mL) or higher (Centers for Disease & Prevention, 2025; Potugari et al., 2020).
The secondary outcome is compliance with each element of the prevention bundle. Compliance was defined as adherence to all components of the bundle; missing even a single element was considered noncompliance. This was measured using a CAUTI prevention bundle checklist audit tool, which encompassed both catheter insertion and maintenance practices.
Statistical Methods
SPSS version 25 (Chicago, IL) was employed to perform descriptive statistics and correlation analysis and the CAUTI rate was determined using the following formula: (Number of CAUTIs/Number of catheter days) × 1000. To compare incidence rates between groups, a Poisson regression model was utilized with 95% confidence intervals. The chi-square (χ²) test of independence was used to assess differences between the pre- and postintervention groups.
Results
Participant Characteristics and Baseline Data
A total of 247 patients with indwelling urinary catheters were assessed in this single-center study conducted at a tertiary care hospital in the Makkah province of Saudi Arabia. The cohort primarily comprised older adults (mean age: 68.9 years) with a high burden of chronic comorbidities, including hypertension (46.6%), insulin-dependent diabetes (23.5%), and peripheral vascular disease (17.8%). The majority of patients were male (67.6%), and most admissions were for medical-related illness (58.7%), followed by postsurgical care (29.6%) and trauma-related treatment (11.7%). Prior to the intervention, the mean hospital stay for catheterized patients was 14.2 days, indicating prolonged bed occupancy and elevated risk of infection (Table 1).
Demographic characteristics of patients (N = 247).

The study was conducted from October 2023 to May 2024 at a government tertiary hospital in Makkah, Saudi Arabia, with a capacity of over 500 inpatient beds and 40 emergency department beds. Patients included in the study were those admitted to adult care units, including general medical, surgical, extended care, and neurosurgical wards, who had indwelling urinary catheters.
Impact of Intervention on CAUTI Rate
The CAUTI rate dropped from 5.4 to 1.41 per 1,000 catheter-days following bundle implementation. Across all patients, the total duration of catheterization was 2,124 catheter-days, with a mean catheter dwell time of 8.6 days per patient. During the pre-intervention period, the mean dwell time was higher, at 14.2 days. The incidence rate ratio (IRR) was 3.62 (95% confidence interval: 1.06–12.44), and the reduction was statistically significant (p = .0407), suggesting that prevention care bundles are effective in achieving a meaningful reduction in infection rates (see Figure 1). These findings highlight the positive impact of the intervention bundle on both catheter management and infection control.
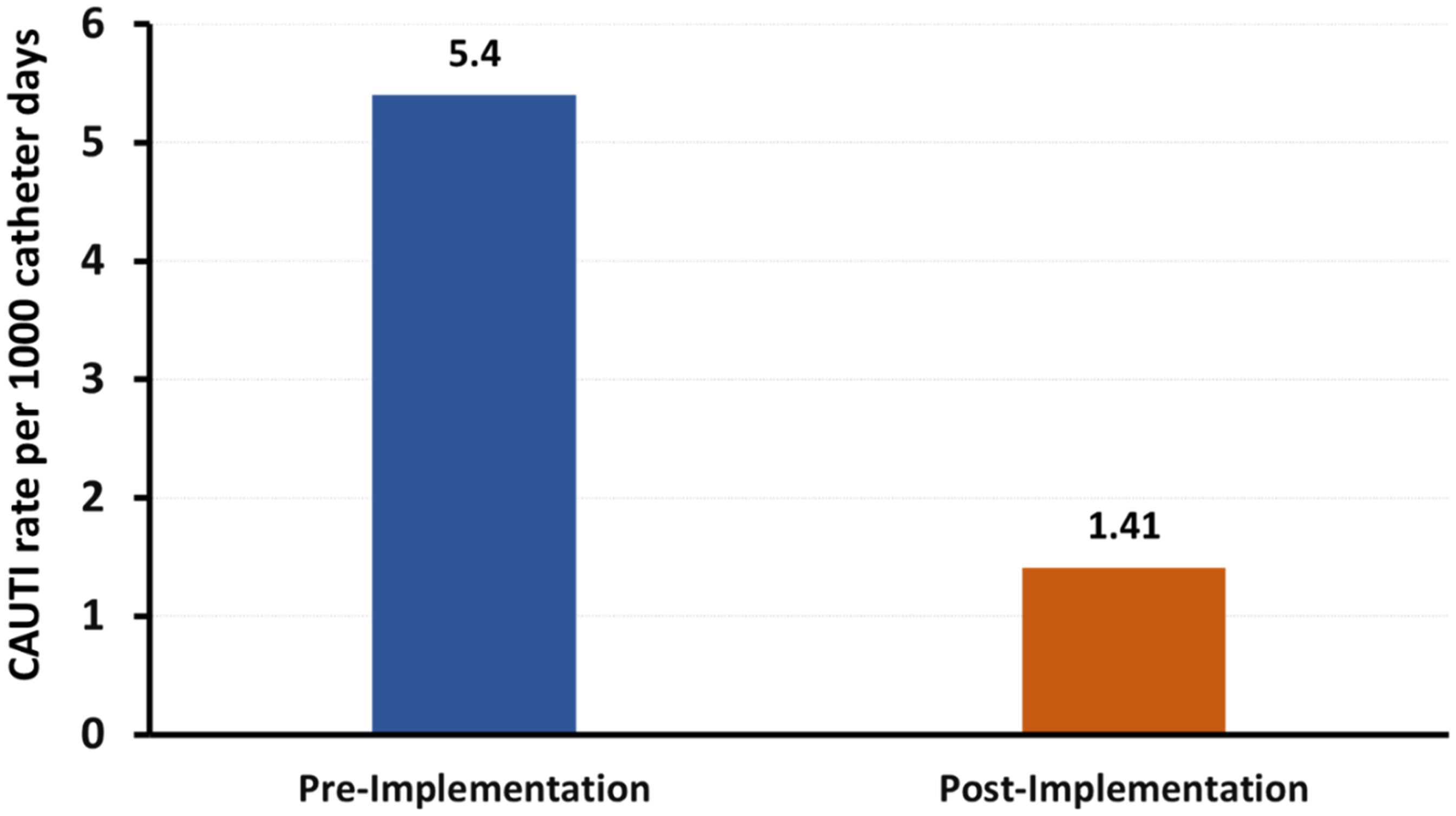
The difference in the CAUTI rate before and after implementation of the CAUTI prevention bundle. The pre-intervention period includes data from January to June 2023, obtained from hospital records where the study was conducted. The postintervention period includes data from November 2023 to May 2024. CAUTI: catheter associated urinary tract infection.
Nursing Compliance Following Intervention
The success of the intervention was also reflected in the significant improvement in RN compliance with the CAUTI prevention bundle. Monthly audits revealed a substantial increase in compliance from 56% in the initial month to 93% in subsequent months. This 37% absolute improvement was statistically significant (p < .001), highlighting a strong association between the intervention and enhanced adherence to evidence-based CAUTI prevention practices. Improved compliance likely contributed to the observed reduction in hospital stays.
Discussion
This prospective, single-arm interventional study demonstrates the transformative effect of combining evidence-based CAUTI prevention bundles with nursing empowerment strategies. In this study, we implemented an updated CAUTI prevention bundle designed to reduce infection rates, be practical for RNs to implement, and empower them to remove catheters unless clinically indicated. The bundle incorporated evidence-based practices aligned with CDC and Saudi Ministry of Health guidelines, including daily catheter reviews, automatic stop orders, and renewal requirements with documented indications. This bridging of global evidence with local health policy ensured contextual relevance and feasibility.
A distinguishing feature of our intervention was its emphasis on nursing empowerment, an often-overlooked element in infection prevention efforts. It has been reported previously that behavioral changes, such as empowering nurses and ensuring full adherence to care bundles, can lead to substantial and sustained reductions in CAUTI rates (Bartlomé et al., 2015; Gupta et al., 2023). Our prevention model expanded on this by involving nurses in daily safety rounds and audit processes, fostering real-time accountability and problem-solving. Qualitative feedback from participating nurses revealed that their adherence was motivated by “feeling trusted to act” and “seeing data on how their actions prevented infections,” reflecting core principles of transformational leadership.
We achieved an approximate 73% reduction in CAUTI incidence, along with a 37 percentage-point improvement in compliance with care protocols highlighting the synergistic role of standardized practices and nurse autonomy in advancing patient safety. These findings align with results from other studies implementing evidence-based prevention strategies. For instance, Clarke et al. demonstrated a significant decline in CAUTI rates in US hospitals using a four-component bundle, emphasizing catheter stabilization and early removal (Clarke et al., 2013). Similarly, a study conducted in the high-dependency unit of a tertiary hospital in Saudi Arabia highlighted that behavioral change, when combined with long-term implementation of prevention models, played a key role in reducing CAUTI incidence rates (Mazi et al., 2024). The national CAUTIoN project in Saudi Arabia also demonstrated a notable decrease in CAUTI rates through structured, evidence-based protocols (Aldalbehi et al., 2025). Importantly, this reduction in CAUTI incidence was achieved without a corresponding change in catheter utilization rates, indicating that improved maintenance and adherence to care protocols rather than change in device utilization rate were key drivers of success. This aligns with CDC guidelines, which emphasize that while appropriate catheter use is essential, it must be combined with meticulous maintenance to effectively prevent CAUTIs, particularly in high-acuity populations (Centers for Disease & Prevention, 2024; Van Decker et al., 2021).
Interdisciplinary teams play an equally vital role in sustaining CAUTI reduction efforts. Our root-cause analyses of each CAUTI event fostered close collaboration among nurses, infection preventionists, and physicians, enabling timely and targeted corrective actions. This collaborative approach mirrors the strategies employed in other studies, which successfully reduced CAUTI rates through daily interdisciplinary rounds (Arora et al., 2014; McClusky & Steenland, 2019). Additionally, experience from a community academic medical center during the COVID-19 pandemic reinforces the value of a multidisciplinary, multipronged strategy. By integrating daily catheter necessity reviews, standardized order sets and insertion checklists, and promoting external urinary diversion devices, the center reduced its NHSN standardized infection ratio for CAUTI from 0.37 in 2019 to 0.00 in 2021 (Whitaker et al., 2023).
These results demonstrate that even under the strains of a global health crisis, structured, team-based interventions grounded in evidence-based practice can yield substantial reductions in hospital-acquired infections. Future initiatives should prioritize data transparency and shared accountability to address persistent challenges, such as variable compliance in high-acuity settings.
Strength and Limitations
The use of a single-arm intervention design was a key strength of this study, as it enhanced the practical relevance and external validity of the CAUTI prevention bundle. Moreover, implementing a standardized, evidence-based bundle empowered nurses to deliver high-quality, consistent care and strengthened their clinical decision-making skills. The study also exemplifies the successful translation of research evidence into clinical practice, demonstrating the feasibility, applicability, and sustainability of the CAUTI prevention bundle in improving patient safety and nursing performance within healthcare settings.
While promising, our study had several limitations. The single-center setting, while enabling detailed workflow analysis, restricts the generalizability of findings. Future multicenter trials are warranted to evaluate the scalability and applicability of the intervention across Saudi Arabia's diverse hospital infrastructure. The single-arm design also limits causal inference. However, rigorous Poisson regression adjusting for comorbidities and diagnosis helps strengthen the validity of the observed associations.
Another key limitation is the reliance on retrospective data from nursing quality indicators collected over a 6-month period. These indicators are aggregate measures used for internal hospital quality monitoring and did not include individual-level demographic or clinical data. Consequently, we were unable to adjust for all potential confounders that may influence outcomes. Moreover, the 6-month postintervention duration may not be sufficient to capture long-term sustainability of the observed improvements. Extended longitudinal follow up is recommended to assess the durability of effects over time.
Lastly, the study did not include documentation of the clinical indications for catheterization, as this was beyond the original scope. This limits contextual interpretation of catheter-use patterns. Future research should consider incorporating this information to enhance clinical insight.
Implications for Practice
The marked reduction in CAUTI incidence following the implementation of a nurse-empowered, all-or-none CAUTI prevention bundle highlights the critical role of structured, multidisciplinary interventions in infection control. Granting nurses the autonomy to assess and remove urinary catheters based on clear criteria not only enhanced accountability but also streamlined patient care. These findings underscore the need for healthcare institutions to prioritize education and support mechanisms that reinforce best practices in infection prevention.
Therefore, we recommend that education on prevention bundles be incorporated into nurse training and staff orientation, along with regular refresher courses for practicing nurses. This approach is crucial for promoting adherence to evidence-based practices aimed at reducing healthcare-associated infections. Hospital management and infection control teams should conduct routine audits and provide feedback to ensure consistent bundle implementation and to identify gaps in practice. Multidisciplinary collaborations, such as among nurses, physicians, infection control teams, and quality improvement staff must be fostered to strengthen accountability, facilitate knowledge transfer, and ensure comprehensive catheter care. Additionally, ongoing professional development opportunities and access to updated clinical guidelines can empower nurses to maintain high standards of care and effectively prevent CAUTIs.
Conclusion
This study demonstrates that nurse-empowered CAUTI prevention bundles can significantly reduce catheter-associated urinary tract infections and improve adherence to care standards. By integrating global evidence with locally tailored implementation, the approach highlights how standardized protocols can be effectively adapted to regional healthcare contexts. Although conducted at a single center, scaling such evidence-based models across diverse settings may further refine prevention strategies and contribute meaningfully to infection control, workforce development, and patient safety.
Footnotes
Abbreviation
Acknowledgments
We extend our heartfelt appreciation to the hospital staff for their generous support and collaboration during the conduction of our study. We are especially grateful to the nursing staff, whose active participation, professionalism, and unwavering commitment greatly contributed to the success of this research. Our sincere thanks also go to the entire healthcare team, particularly the Infection Control and Quality Departments, for their valuable support, guidance, and dedication throughout the study.
Ethics Approval and Consent to Participate
The necessary permits and approvals for this study were obtained from the Research Ethics Committees one of the large metropolitan hospital, Ministry of Health, Saudi Arbia and Umm Al-Qura university Research Ethics Committees
Funding
The present study did not receive any dedicated financial funding from public, commercial, or not-for-profit funding organizations.
Competing Interests
The authors declare no competing interests.
Data Availability
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.