
Abstract
Introduction
Although leaders can foster psychological safety by encouraging moral behaviors, the link between the two remains unclear. Despite its importance in clinical education and patient safety, empirical research has not adequately explored the unique impact of nursing leaders’ moral character and actions.
Objectives
This study not only examined the relationships between nursing leaders’ moral leadership, nurses’ psychological safety, team learning behaviors, and teams’ psychological safety but also assessed whether moral leadership and sample characteristics predict nurses’ and teams’ psychological safety.
Methods
A quantitative cross-sectional design was employed. After a pilot study, an online survey using Google Forms was conducted over 1 month in 2024. To assess the concepts studied, 365 nurses were recruited from different hospitals using convenience snowball sampling, yielding a response rate of 73%.
Results
Responses were rated on a 5-point Likert scale. Nurses rated their leaders as moral. Individualized means varied across variables. Most leaders showed high integrity and temperament, but moderate courage and prudence. Nurses’ respect was the highest moral subscale, followed by team learning. Teams’ psychological safety was high, especially in risk-taking and expectations, but moderate in learning from failure and support. Moral leadership correlated with nurses’ psychological safety and teams’ safety. Moral leadership and work area predicted nurses’ and teams’ psychological safety.
Conclusions
These findings suggest that although moral leadership is perceived positively, its impact on psychological safety may vary depending on contextual factors such as organizational culture and leadership style. Nursing leaders’ moral leadership and area of work were the shared determinants of nurses’ and teams’ psychological safety. Moral nursing leaders make a difference in the work environment. When nurses and nursing teams admire the qualities of their moral leaders, their psychological safety, including team learning behaviors, improves, resulting in several positive outcomes. Moral leadership contributes to psychologically safe environments by promoting openness, respect, and learning from failure. Future research should explore cross-cultural applications of moral leadership and its impact on team dynamics.
Introduction
Moral leadership has attracted increasing attention within the realms of organizational behavior and healthcare management (Gentry & Fleshman, 2020; Jackson & Lasthuizen, 2024; Meng & Guo, 2025; Newstead et al., 2020). Whereas ethical leadership revolves around a firm commitment to established ethical principles and guidelines, often shaped by external standards, moral leadership emphasizes personal values, integrity, and a deep awareness of right and wrong, stemming from one's internal moral compass (Ashley, 2025).
Moral leadership influences individual behaviors in various contexts and differs based on cultural values (Jackson & Lasthuizen, 2024). Although moral leaders foster psychological safety, their effectiveness is culturally contingent. Collectivist cultures, like that of Jordan, emphasize group harmony, which may discourage individual expression, potentially limiting the impact of moral leadership on psychological safety, whereas individualist cultures prioritize personal integrity and autonomy (Campion, 2019). This raises questions about whether moral leadership must be adapted to cultural norms to be truly effective (Sahlin et al., 2025). Moral leadership shapes how individuals behave by exemplifying moral characteristics, including courage, prudence, and integrity (Hackman et al., 2025).
Moral characters of leaders have been found to improve team outcomes through heightened commitment, reduced turnover intentions, and enhanced job performance (Newstead et al., 2020; Palanski et al., 2015). However, the processes through which moral leadership influences team climates, especially in nursing, remain insufficiently investigated (Jackson & Lasthuizen, 2024; Newstead et al., 2020).
Psychological safety—a belief that the team members are free to take interpersonal risks (Edmondson, 1999)—is essential in healthcare environments. Teams exhibiting high psychological safety report more transparent communication, a greater willingness to disclose errors, and stronger collaborative learning practices, directly affecting patient safety and the quality of care provided (Edmondson, 2018; Hessler et al., 2025).
Psychological safety builds trust and creativity, enabling team members to voice concerns and suggest innovations without fear (Edmondson, 1999). In nursing, it promotes help-seeking and experimentation, reduces errors, and boosts team performance (Edmondson, 1999; Zajac et al., 2021).
Moral leadership is a significant precursor to psychological safety (Alhaidan, 2024; Hendriks et al., 2020; Liu et al., 2025), as moral leaders foster trust and stimulate open communication (Hendriks et al., 2020), promoting fairness within their organizations and creating an environment where mistakes are viewed as learning opportunities rather than as reasons for punishment (Alhaidan, 2024). Nevertheless, to the best of our knowledge, no research has yet empirically explored how the moral actions of nursing leaders affect both individual nurses and entire teams. Therefore, the current study examined the relationships between nursing leaders’ moral leadership, nurses’ psychological safety, team learning behaviors, and teams’ psychological safety and assessed whether moral leadership and sample characteristics predict nurses’ and teams’ psychological safety.
Research Problem
Recent research in healthcare has defined moral leadership based on integrity, fairness, empathy, and justice. Hendriks et al. (2020) revealed that leaders who consistently demonstrate moral virtues report markedly higher levels of life satisfaction and job engagement among their subordinates. In nursing, Ahmad et al. (2023) reported that moral leadership contributes to enhanced psychological safety by enabling nurses to express concerns without fear, and Hessler et al. (2025) associated leader morals with improved team learning.
Research on psychological safety highlights its critical role in error reporting and collective learning within healthcare teams (Edmondson, 2018). The Global Survey of McKinsey (2021) identified supportive and consultative leadership behaviors as strong predictors of a psychologically safe environment.
Although psychological safety is well-established as vital for clinical learning and patient safety, empirical studies that isolate the distinct influence of nursing leaders’ moral character and behaviors are scarce, hindering comprehension of how specific moral traits and morally grounded decision-making processes create a secure environment for interpersonal risk-taking.
Significance of the Study
Effective leadership in nursing is dependent on moral characteristics that influence both individual and collective results, particularly in terms of nurses’ psychological safety and team learning behaviors (Edmondson, 2018; Pakizekho & Barkhordari-Sharifabad, 2022). This research it is unique because it (1) connects the moral actions of nursing leaders to psychological safety at both the individual (nurse) and group (team) levels; (2) it redefines moral leadership as a dynamic process where behavioral integrity and situational challenges collaboratively foster moral courage; and (3) it combines moral leadership, individual psychological safety (including team learning behaviors), and team psychological safety into a unified framework.
Although previous studies have indicated that moral courage mediates the relationship between integrity and performance/image (Palanski et al., 2015) and highlighted the impact of humility leadership on team safety (Mrayyan & Al-Rjoub, 2024; Rego et al., 2021), this study is the first within nursing and healthcare to integrate the three concepts of nursing leaders’ moral leadership on nurses’ psychological safety, and teams’ psychological safety.
Moral leadership enhances psychological safety, motivating nurses to express themselves and report errors without fear (Lee & Dahinten, 2021), fostering self-driven learning, innovation, and improved patient care (Lee & Dahinten, 2021). Nurses become self-driven to learn, enhance practices, and propose ideas that improve patient safety and care quality (Lee & Dahinten, 2021). Moral leaders cultivate a supportive environment, although the effectiveness of this support depends on their responsiveness to team feedback and adaptability in high-pressure situations (Ahmad et al., 2023). When nurses sense authentic support and emotional validation, their levels of stress and fatigue diminish, allowing for sustained engagement, proactive problem-solving, and ongoing improvement (Ahmed et al., 2023). By exhibiting moral courage in challenging situations, moral leaders strengthen nurses’ sense of professional purpose (Elhihi et al., 2025), thereby enhancing nurses’ moral motivation to navigate various patient care dilemmas (Elhihi et al., 2025). Finally, teams high in psychological safety exhibit greater cohesion, productivity, and retention, cultivating healthier workplaces and better care outcomes (Abbasivand-Jeyranha & Barkhordari-Sharifabad, 2025).
The findings can inform the design of moral leadership development initiatives, empowering nurse leaders to embody integrity and courage, cultivate psychological safety, and ultimately enhance team learning, staff well-being, and patient care.
Theoretical Framework
Although leadership theories that emphasize morals, ethics, and virtues highlight the connection between moral and effective leadership (Jackson & Lasthuizen, 2024; Newstead et al., 2020), few have critically examined how these values translate into measurable outcomes like psychological safety. This gap suggests a need to determine whether moral leadership alone suffices or if it should be complemented by structural and relational factors (Jackson & Lasthuizen, 2024; Newstead et al., 2020). The absence of morals such as justice, temperance, humanity, and wisdom can render human organizations incapable of survival (Newstead et al., 2020).
The theoretical framework employed in this study is the authentic leadership theory (Walumbwa et al., 2008). Authentic leadership focuses on ethical principles, self-awareness, and relational transparency. These elements are key elements for the culture of psychological safety within nursing teams (Almutairi et al., 2025).
Nursing leaders can significantly boost psychological safety by valuing openness and showcasing integrity, transparency, and honesty to build relational trust, creating a space where nurses feel comfortable expressing concerns, sharing ideas, and participating in ethical decision-making (Almutairi et al., 2025). They should also engage in balanced decision-making and shared ownership to encourage interpersonal risk-taking, thereby enhancing individual and collective psychological safety within nursing teams (Ip et al., 2025).
Literature Review
Morals are acquired and valued dispositions voluntarily demonstrated through habitual behaviors in relevant situations (Jackson & Lasthuizen, 2024; Newstead et al., 2020). Commonly reported antecedents of moral leadership are responsibility disposition and environmental (situational) cues (Pearce et al., 2006). Leaders can be socialized or personalized, with the former exhibiting a stronger sense of responsibility. Leaders with a high responsibility disposition align with moral standards, show concern for others, and pursue collective goals over personal gain. Situational strength provides behavioral cues, but does not guarantee moral behavior (Pearce et al., 2006).
The well-being of employees and other elements within the workplace is connected to the organization's moral standards and particular virtues, including the behavioral integrity of the leader (Hendriks et al., 2020; Jackson & Lasthuizen, 2024). Moral leaders promote equity and justice (Jackson & Lasthuizen, 2024), fostering shared leadership and empowering teams (Hendriks et al., 2020; Newstead et al., 2020; Pearce et al., 2006).
Psychological safety is essential for individuals to feel at ease when expressing their thoughts, sharing information, engaging in learning, and participating in ongoing conversations (Edmondson, 2018; Hessler et al., 2025; Newstead et al., 2020). Establishing clear moral boundaries can promote a safe workplace environment and facilitate psychological safety, leading to improved performance. When these boundaries are breached, leaders and colleagues can reflect on what went wrong and how morals can be utilized to repair, restore, or enhance the situation (Newstead et al., 2020). Thus, leaders must create a moral-based environment that allows individuals to thrive (Newstead et al., 2020).
The detrimental impact of team leaders’ authoritative leadership behaviors on psychological safety has been highlighted in the Global Survey of McKinsey (2021). Conversely, consultative and supportive leadership behaviors have been found to promote psychological safety. This correlation between leadership styles and psychological safety extends to moral leadership (Pearce et al., 2006), which influences followers’ innovative work behavior by fostering psychological safety (Ahmad et al., 2023). Moral leaders aim to improve the organization's well-being while balancing stakeholder interests and promoting shared leadership, thereby enhancing team problem-solving and creativity (Pearce et al., 2006).
Methods
Research Questions
This study addresses five research questions:
What are the levels of nursing leaders’ moral leadership? What are the levels of nurses’ psychological safety, including team learning behaviors? What are the levels of teams’ psychological safety? What are the relationships between nursing leaders’ moral leadership and nurses’ and teams’ psychological safety? Does nursing leaders’ moral leadership predict nurses’ and teams’ psychological safety?
Design
This study adhered to the STrengthening the Reporting of OBservational Studies in Epidemiology (STROBE) checklist (STROBE Group, 2014), employing a cross-sectional design utilizing an online survey to measure the studied concepts. This design facilitates the collection of data at a single moment in time, resulting in quicker and more cost-effective outcomes (Polit & Beck, 2019).
Settings and Sample
A convenience snowball sample of nursing academics, nurses, and nursing leaders from various hospitals was compiled after a pilot study with no necessary modifications. The first researcher utilized convenience sampling, announcing the study and allowing participants to voluntarily participate, and employed snowball recruiting by referring nurses.
This study focused on one major independent variable—leaders’ moral leadership—and nine demographic characteristics—gender, marital status, age, years of experience in nursing, years of experience in the current area of work, level of education, shift worked, work area, and sector. The two main dependent variables were nurses’ and teams’ psychological safety (Table 1).
Subject's Characteristics (n = 365).

Some totals did not equal 365 because of missing data.
The sample size was determined using the formula N = 10(k) + 50, where k represents the number of variables (9 + 1), and 50 cases were added to account for attrition. Polit and Beck (2019) recommend a minimum of 150 participants, but 365 nurses were recruited for this study. The inclusion criteria were proficiency with technological platforms and employment in hospital environments for at least 1 year. The exclusion criterion was diploma nurses who operate with a more restricted scope of practice, influencing their ability to engage with leadership dynamics and make ethical decisions (Meng & Guo, 2025).
Ethics
Approval was granted by the Institutional Review Board (IRB) of the first author's university (No. XXXX). All participant data were anonymized, with the coded responses securely stored in Google Drive; the researchers only shared the aggregates with nursing administrators at the designated hospitals.
Data Collection
Data were collected in 2024 and spanned 1 month. An online self-report survey was conducted in English using Google Forms. The survey link was shared on the Facebook pages of the Faculty of Nursing and the first researcher's colleagues. Nurses’ participation in the survey served as their consent. Nurses were prompted to invite their contacts to take the survey. A reminder was sent after 2 weeks to ensure that each nurse only took the survey once.
Instruments
Instruments were in English, Jordan's official language of nursing education. All the tools are available in the public domain; thus, no permissions were needed. The online survey amalgamated three tools.
Virtuous Leadership Scale
This scale measuring moral leadership was developed by Ou (2021). It comprises 29 items rated on a five-point Likert-type scale, with 1 indicating “strongly disagree” and 5 indicating “strongly agree.” Following Vagia'’s (2006) scoring, scores from 1 to 2.33 are considered low; 2.34 to 3.67, moderate; and 3.67 to 5, high. The Cronbach's alpha of the virtuous leadership scale was 0.94 in Ou (2021) and 0.95 in this study, indicating excellent reliability.
Nurses’ Psychological Safety
This 11-item scale developed by Edmondson (1999) evaluated the individual psychological safety of nurses, with responses ranging from “strongly disagree” to “strongly agree” on a scale of 1 to 5. This scale also followed Vagia'’s (2006) scoring. The Cronbach's alpha in this study was 0.89.
Team Psychological Safety
Teams’ psychological safety was assessed using a 19-item scale developed by Edmondson (1999). It was rated on a 5-point scale, with 1 indicating “strongly disagree” and 5 indicating “strongly agree.” This scale also followed Vagia'’s (2006) scoring. The Cronbach's alpha in this study was 0.94.
Data Analyses
Data were analyzed using the Statistical Package for the Social Sciences (IBM, 2017), with a significance level of 0.05. Leaders’ moral leadership, nurses’ psychological safety (including learning behaviors), and teams’ psychological safety were treated as interval variables. Descriptive statistics of means, standard deviations, frequencies, percentages, 95% confidence intervals of the mean, standard errors (SEs), and range were reported based on the types of variables. The independent variables in this study were the leaders’ moral leadership and sample characteristics. Nurses’ and teams’ psychological safety served as the dependent variables (Polit & Beck, 2019).
To examine the impact of leaders’ moral leadership on nurses’ and teams’ psychological safety, the general linear model (GLM) was employed (Polit & Beck, 2019). To gain further insights into the relationships between nursing leaders’ moral leadership and nurses’ and teams’ psychological safety, we conducted Pearson's correlation analysis, assessing the correlations between the total scores of the concepts and sample characteristics (Polit & Beck, 2019).
Results
Convenience snowball sampling was used to contact 500 nurses, of whom 365 responded, yielding a response rate of 73%. Most were young married women with Baccalaureate degrees who had approximately 4 years of experience in nursing and their current area of work. They worked on different types of shifts in government hospital units (Table 1).
Nursing Leaders’ Moral Leadership
To answer the first research question, nurses rated their nursing leaders highly in terms of moral leadership (mean = 3.80/ 5, SE = 0.033). The tool comprised six subscales: courage (4 items; mean =3.64, SE = 0.032), humanity (8 items; mean = 3.78, SE = 0.034), integrity (5 items; mean = 3.96, SE = 0.036), justice (5 items; mean = 3.82, SE = 0.040), prudence (4 items; mean = 3.59, SE = 0.058), and temperance (3 items; mean =3.95, SE = 0.044); the majority of nursing leaders had high integrity and temperament but moderate prudence and courage. The highest two means of moral leadership were for nursing leaders to do the right things even when they are unpopular (mean = 4.17, SE = 0.039) and acting as role models (mean = 4.04, SE = 0.053). The lowest were for nursing leaders expressing concerns for the misfortune of others (mean = 3.32, SE = 0.049) and everyone's needs (mean = 3.39, SE = 0.062) (Table 2).
Means, Standard Errors of the Means, Frequencies, Percentages, and 95% Confidence Interval (CI) of the Means of Nursing Leaders’ Moral Leadership (n = 365).

This Likert scale is rated from 1 (strongly disagree) to 5 (strongly agree). SE = Standard Error of the Mean; 95% Confidence Interval (CI) of the mean, using standard errors.
Nurses’ Psychological Safety
To answer the second research question, nurses rated their psychological safety, including learning behaviors in nursing teams, as high (mean = 3.78/ 5, SE = 0.038). The tool comprised three subscales: individual safety (4 items; mean = 3.71/ 5, SE = 0.046), individual respect (3 items; mean = 3.83/ 5, SE = 0.041), and team learning (4 items; mean = 3.82/ 5, SE = 0.044). Individual respect was the highest. The highest two means of nurses’ psychological safety were for workers welcoming others’ ideas and giving them time and attention (mean = 3.98, SE = 0.040), indicating high individual respect, and the ease with which the team could discuss difficult issues (mean = 3.94, SE = 0.041), indicating high individual safety. The lowest means were for nurses not facing retaliation or criticism when admitting to committing errors or mistakes (mean = 3.52, SE = 0.063), and for nurses raising concerns about team plans or decisions (mean = 3.66, SE = 0.062).
Regarding the third subscale, the highest means of nurses’ learning behaviors in the teams were for the ability to discuss mistakes and ways to improve and learn from them (mean = 3.89, SE = 0.048) and to identify underlying assumptions and seek counterarguments about issues being discussed (mean = 3.89, SE = 0.055). The lowest means were for their freedom to raise concerns about team plans or decisions (mean = 3.66, SE = 0.062) (Table 3).
Means, Standard Errors of the Means, Frequencies, Percentages, and 95% Confidence Interval (CI) of the Means of Nurses’ and Teams’ Psychological Safety (n = 365).
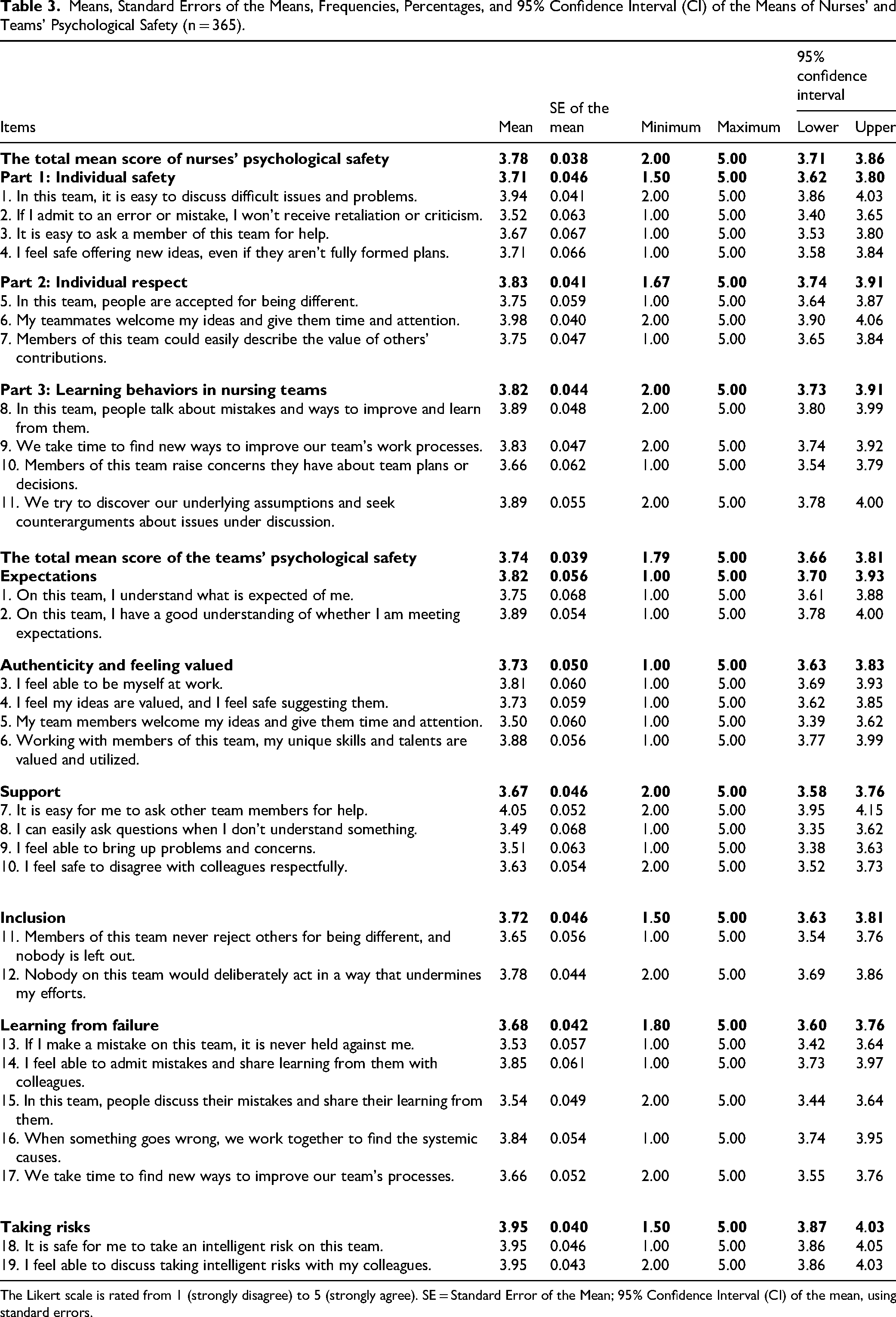
The Likert scale is rated from 1 (strongly disagree) to 5 (strongly agree). SE = Standard Error of the Mean; 95% Confidence Interval (CI) of the mean, using standard errors.
Nursing Teams’ Psychological Safety
To answer the third research question, nurses rated their teams’ psychological safety as high (mean = 3.74/ 5, SE = 0.039). The tool comprised six subscales: expectations (2 items; mean = 3.82, SE = 0.056), authenticity and feeling valued (4 items; mean = 3.73, SE = 0.050), support (4 items; mean = 3.67, SE = 0.046), inclusion (2 items; mean = 3.72, SE = 0.046), learning from failure (5 items; mean = 3.68, SE = 0.042), and taking risks (2 items; mean = 3.95, SE = 0.040). Nursing teams’ psychological safety was high in terms of taking risks and expectations but moderate in learning from failure and having support. The two highest means of nursing teams’ psychological safety were for feeling safe to take an intelligent risk on the team (mean = 3.95, SE = 0.046) and taking intelligent risks with colleagues (mean = 3.95, SE = 0.043). The lowest means were for the ability of nurses to easily ask questions when they did not understand something (mean = 3.49, SE = 0.068) and for team members welcoming each other's ideas and giving them time and attention (mean = 3.50, SE = 0.060) (Table 3).
Correlations of Nursing Leaders’ Moral Leadership and Nurses’ and Teams’ Psychological Safety
To answer the fourth research question, nursing leaders’ moral leadership was correlated significantly, positively, and moderately with nurses’ psychological safety—including learning behaviors in nursing teams (r = 0.609 at alpha 0.001)—and teams’ psychological safety (r = 0.635 at alpha 0.001). Nurses’ psychological safety correlated significantly, positively, and moderately with teams’ psychological safety (r = 0.697 at alpha 0.001) and significantly and positively but weakly with nurses’ marital status (r = 0.128 at alpha 0.005); all tests were two-tailed (Table 4).
Significant Correlations of Total Scores of Nursing Leaders’ Moral Leadership, Nurses’ and Teams’ Psychological Safety and Samples’ Characteristics (n = 365).

At significance level 0.05; bAt significance level 0.01.
Nursing Leaders’ Moral Leadership and Subjects’ Characteristics as Determinants of Nurses’ and Teams’ Psychological Safety
To answer the fifth research question, the GLM indicated that the determinants of nurses’ psychological safety were nursing leaders’ moral leadership (B = 0.32, p-value = 0.001), area of work (B = -1.87, p-value = 0.011), and type of hospitals (B = -2.06, p-value = 0.041). The model was significant (F(df = 9,1) = 401.04, p-value = 0.001, R2 = 0.631, Table 5) and explained 63.10% of the variance in the mean of nurses’ psychological safety score. The GLM indicated that teams’ psychological safety determinants were nursing leaders’ moral leadership (B = 0.60, p-value = 0.001) and area of work (B = -3.65, p-value = 0.003). The model was significant (F(df = 9,1) = 501.62, p-value = 0.001, R2 = 0.673, Table 5) and explained 67.30% of the variance in the mean of teams’ psychological safety.
General Linear Model (GLM) Model of the Total Score of Nursing Leaders’ Moral Leadership and Subject's Characteristics as Predictors of Nurses’ and Nursing Team Members’ Psychological Safety (n = 365).

* Indicates that B refers to unstandardized coefficients in the regression model.
** Refers to the total score of nurses' psychological safety, and denotes that the result is statistically significant at p < 0.001 (2-tailed). Additional descriptive statistics: mean = 41.99, standard deviation = 0.30, 95% confidence interval = [41.40, 42.58].
*** Refers to the total score of the team's psychological safety, and also denotes statistical significance at p < 0.001 (2-tailed). Additional descriptive statistics: mean = 71.20, standard deviation = 0.51, 95% confidence interval = [70.21, 72.18].
Covariates appearing in the model are evaluated at the following values: total score of leaders' moral leadership = 109.86, gender = 1.77, marital status = 1.60, age = 2.34, experience in nursing = 2.49, experience in the current area of work = 3.21, level of education = 3.00, shift worked = 1.50, area of work = 1.48, and the sector of work = 1.36.
Discussion
This study assessed whether nursing leaders’ moral leadership was associated with nurses’ and teams’ psychological safety. The findings suggest that although moral leadership is perceived positively, its impact on psychological safety may vary depending on contextual factors.
Nurses reported respect and team learning as the highest psychological safety subscales. Nursing teams had high psychological safety in terms of taking risks, but they needed to learn from failures, which was linked to having leaders’ support. Moral leaders foster nurses’ and teams’ psychological safety through integrity and transparency, enhancing trust, ethical risk-taking, and constructive feedback. Such environments encourage open communication and collaboration, enhancing psychological safety and team cohesion (as in Alilyyani et al., 2022).
The moral leadership of nursing leaders correlated with psychological safety by creating a supportive environment in which nurses feel appreciated and respected and building trust by encouraging them to engage in open communication and request support, especially when committing errors. This facilitates learning from failures, but only when leaders model vulnerability and treat error reporting as a developmental tool (Alhaidan, 2024; Liu et al., 2025).
The findings align with authentic leadership theory, but they also expose limitations. Although integrity and transparency were rated highly, moderate scores in courage and prudence suggest that moral leadership may not fully address the complexities of high-pressure clinical environments, necessitating a more nuanced understanding of how different moral traits interact with situational demands (Nanjundeswaraswamy et al., 2024).
Nurses recognized respect and team learning as the key aspects of psychological safety, aligning with the principles of authentic leadership theory, especially the elements of relational transparency and internalized moral perspective. As Walumbwa et al. (2008) noted, authentic leaders create environments based on trust, openness, and ethical consistency, fostering interpersonal respect, which enhances nurses’ confidence to participate in team-based learning and take interpersonal risks. Although nurses expressed confidence in risk-taking, the gap in learning from failure underscores the need for leadership support. Although authentic and moral leaders promote learning from failure, reinforcing psychological safety, future studies should critically examine whether moral leadership alone suffices or if complementary leadership styles are necessary to sustain psychological safety.
Nursing Leaders’ Moral Leadership
Nurses regarded their nursing leaders as exemplifying moral leadership. Virtue is a fundamental attribute for both nurses and nursing leaders (Hendriks et al., 2020; Jackson & Lasthuizen, 2024). Moral leaders demonstrate a strong commitment to their employees, patients, and clients (Jackson & Lasthuizen, 2024). Caldwell et al. (2015) expanded on the idea of the moral continuum to highlight the significance of a moral viewpoint in leadership. Such leaders foster positive relationships, subsequently improving organizational outcomes (Jackson & Lasthuizen, 2024). Participants’ high evaluations of their leaders’ virtues may be associated with their overall sense of well-being and trust (Hendriks et al., 2020).
Nurses rated nursing leaders highly on integrity and temperament but moderately on prudence and courage. Most participants were young, belonging to Generation Z (Gen Z), representing the most diverse and well-educated nurses entering the nursing workforce (Maravilla, 2021). Gen Z nurses valued courage and prudence (Maravilla, 2021) but rated leaders moderately on these traits, possibly because of high demand, low control, and poor staffing (Bolliger et al., 2022).
Nurses’ Psychological Safety
Nurses assessed their psychological safety, along with the learning behaviors exhibited within nursing teams, as high. Ayub et al. (2022) indicated that psychological safety mediates the connection between learning behaviors and students’ perceptions of their educational experiences; nurses with high individual psychological safety engage in critical reflection and foster interactions among peers, between leaders and nurses and in instructor–student interactions on students’ learning experiences.
The Individual Psychological Safety and Learning Behaviors in Working Teams scale comprises three subscales: individual safety, individual respect, and team learning. Nurses assessed their levels of individual respect and team learning as being higher than their perception of individual safety, potentially reflecting human nature, as self-respect often takes precedence over safety, serving as a crucial aspect of an individual's existence. Furthermore, self-respect can significantly enhance the learning experience. Although Maslow's hierarchy of needs points out that safety—encompassing security, stability, love, and belonging—is fundamental for psychological well-being, self-respect is actually better classified under esteem needs (McLeod, 2025). According to self-determination theory, self-respect is not a basic need but a result of satisfying essential psychological needs like autonomy, competence, and relatedness (Ryan & Deci, 2017). Self-respect, a component of esteem needs, may precede psychological safety (Wouters-Soomers et al., 2022). Leaders should foster environments that build self-respect (Rimon-Or et al., 2023).
Nurses reported high learning behaviors in their teams because they could discuss mistakes and ways to improve and learn from them. Nurses also sought to identify underlying assumptions and seek counterarguments about issues being discussed. Conversely, they felt constrained in voicing their concerns about team strategies and decisions. These findings relate to nurses’ high individual safety. They engaged in critical reflection (Ayub et al., 2022), enabling them to recognize the advantages of addressing the retaliation or criticism they faced, ultimately leading to a constructive learning experience. The benefits in such scenarios may surpass the drawbacks, reflecting findings by Pfeifer and Vessey (2019). Nurses with high individual psychological safety experience positive interactions among themselves and with their leaders (Ayub et al., 2022), enhancing their capacity to express concerns regarding team strategies and decisions.
Nursing Teams’ Psychological Safety
Nurses assessed their teams’ psychological safety as high, in contrast with the findings of Mrayyan and Al-Rjoub (2024) in Jordan. This outcome is expected, as psychological safety increases over time. The high psychological safety reported by nurses may contribute positively to the overall psychological safety of their teams. A systematic review by O’donovan and Mcauliffe (2020) identified several factors promoting psychological safety in healthcare teams. In our study, teams showed high safety in risk-taking and expectations (learning orientation) but moderate support and learning from failure (inclusiveness). As Murphree (2022) noted, leaders who foster inclusiveness can enhance psychological safety, encouraging team members to take risks and learn from any failures. Nevertheless, nurses in this study indicated that these risks are approached collectively and thoughtfully by their colleagues.
Correlations Between Nursing Leaders’ Moral Leadership and Psychological Safety
The moral leadership of nursing leaders was associated with the psychological safety of nurses (Abbasivand-Jeyranha & Barkhordari-Sharifabad, 2025), also correlating with the psychological safety of nursing teams. This relationship is indirectly supported by the findings of Kelemen et al. (2023), who noted that various forms of moral leadership are rooted in moral characteristics. Furthermore, Porter et al. (2023) highlighted the potential roles of psychological safety in fostering the adoption of these virtues. Thus, moral leadership may enhance positive learning behaviors and experiences within the team.
Nurses’ psychological emphasis on learning behaviors within nursing teams has a significant, positive, and moderate correlation with these teams’ psychological safety. Thus, nursing leaders should provide support to their teams and view failures as opportunities for growth and learning.
The psychological safety of nurses exhibited a significant yet weak positive correlation with their marital status. The majority of nurses, being women, may experience higher levels of psychological safety, including enhanced learning behaviors. Veale et al. (2023) emphasized the importance of psychiatric nursing in maintaining physical safety while also highlighting the ability of female nurses to effectively manage various patient situations owing to their elevated emotional or psychological safety. Conversely, Sadoughi and Hejazi (2023) reported no statistically significant differences in learning behaviors between male and female academics, a finding that did not align with our study.
Determinants of Nurses and Teams’ Psychological Safety
Although moral leadership is widely recognized for promoting ethical behavior and trust, its ability to foster psychological safety is often limited by systemic barriers such as rigid hierarchies and resource constraints (American Psychological Association [APA], 2024). These structures can suppress open communication and hinder inclusive practices, rendering moral leadership insufficient on its own (APA, 2024). Psychological safety thrives in environments where leadership is supported by organizational policies that promote mental health and growth opportunities, highlighting the need for structural reinforcement alongside moral intent (APA, 2024).
In this study, factors influencing the psychological safety of nurses, particularly in relation to learning behaviors within nursing teams, included the moral leadership of nursing leaders, specific work environment, and type of hospitals involved. Leaders who demonstrate moral integrity may foster both psychological safety and learning behaviors among their nursing staff. Hunt et al. (2021) noted that psychological safety and the promotion of learning behaviors are essential components to achieve success in healthcare teams. However, they do not emerge spontaneously; they require moral leaders who embody key virtues, such as trust, within their teams (Kelemen et al., 2023). This “virtuous cycle” suggests that trust enhances individual and team psychological safety (Cartland et al., 2022). Enhanced psychological safety has been linked to innovative learning behaviors (Hunt et al., 2021), including adapting to change (Cartland et al., 2022).
Nurses employed in governmental hospitals and units generally reported lower levels of psychological safety, which may adversely affect their learning behaviors compared to their counterparts in wards and private hospitals. In Jordan, government hospitals face significant challenges, including high patient demand, limited control over their work environment, and inadequate staffing, as evidenced during and following the COVID-19 pandemic. The effectiveness of units is often compromised owing to the nature of critical cases and insufficient staffing, raising concerns about nurses’ ability to learn without psychological safety. Research indicates that when nurses possess a degree of control, their psychological safety tends to increase, even amid the changes brought about by COVID-19 (Lee, 2021). Nurses with control may learn better, regardless of hospital type.
Moral leadership and work environment strongly shape nurses’ psychological safety. Individual nurses feel safe, and in turn it boosts team-wide safety. Key factors include learning orientation and inclusiveness (O’donovan & Mcauliffe, 2020). Furthermore, nursing teams operating in units generally exhibited lower levels of psychological safety than those in wards. Lower psychological safety in units may stem from limited control, poor staffing, and high stress.
Strengths of the Study
This study contributes to the advancement of nursing leadership research. It is among the first to investigate the impact of moral leadership on both individual and team psychological safety within nursing contexts, providing a unique and valuable perspective. The inclusion of learning behaviors further enriches the understanding of how ethical leadership influences team dynamics and performance. The study's large, diverse sample (N = 365) drawn from multiple hospital settings enhances the generalizability and robustness of the findings. Moreover, the use of validated instruments with high reliability, such as Edmondson's psychological safety scales, strengthens the credibility of the data (Edmondson, 1999, 2018).
The theoretical grounding of the study is reinforced by the integration of authentic leadership theory, providing a solid framework for interpreting the role of moral leadership in healthcare environments. Practical implications for leadership development and nursing education are evident in the importance of ethical leadership to foster safe, collaborative, and innovative care settings. The study also considered organizational nesting by calculating intraclass correlation coefficients, suggesting directions for future multilevel analyses. Additionally, recognizing team composition variables, such as diversity in experience and demographics, adds depth to the analysis of team functioning. The study proposes future research directions, including the use of digital communication analysis to capture real-time indicators of stress and collaboration and the expansion of research to include other roles such as nursing academics and leaders.
Limitations of the Study
Despite its contributions, the study's methodological limitations warrant consideration. The reliance on self-report measures introduces potential biases, including social desirability and common-method variance, potentially affecting the accuracy of the findings. Convenience snowball sampling limits the generalizability of the results across different healthcare settings and cultural contexts, particularly given the geographic constraints within Jordan (Polit & Beck, 2019). The cross-sectional design restricts the inference of causality or observation of changes over time, highlighting the need for longitudinal or mixed-method approaches in future research.
Cultural factors specific to Jordan, such as strong collectivism and vast power distance, may influence the interpretation of moral traits and limit the cross-cultural applicability of the findings. The absence of multi-source data and team-level variables, such as team type and composition, further constrains the analysis. Additionally, the use of interval psychology scales, which often yield non-normal residuals, may obscure associations when confounding variables such as organizational structure or leadership style are considered. The study did not differentiate between types of nursing teams, which could affect psychological safety and learning behaviors, as functional, self-managed, and task-force teams may experience these dynamics differently (Edmondson, 1999, 2018).
Moreover, the use of GLM may not be optimal for interval data, as it can produce imprecise estimates. Future research should consider structural equation modeling and functional linear models to better capture the complexity of these constructs (Beyaztas et al., 2022). Finally, although the study highlights the role of moral leadership, it remains unclear whether this alone can sustain psychological safety, or whether structural reforms and policy interventions must complement it. Future research should also examine mediating processes that link moral leadership to psychological safety and learning behaviors, while accounting for contextual factors (Wang et al., 2018).
By exploring these avenues, subsequent research can enhance our comprehension of how the ethical behavior of nursing leaders contributes to the creation of safer, more innovative, and more resilient care environments.
Implications for Practice
Although moral leadership is essential, its practical application may be constrained by systemic issues such as staffing shortages and hierarchical structures. Training programs must therefore extend beyond virtue cultivation to include strategies for navigating organizational barriers that inhibit psychological safety. Programs focused on leadership competencies, which include moral decision-making, advanced clinical leadership, and the promotion of a culture that values moral practices, are essential, as are those based on leadership theories, including authentic and transformational leadership, which offer a foundational understanding of the relationship between moral leadership and psychological safety. Such programs empower nursing leaders with the resources required to cultivate supportive environments, boost team performance, and improve patient care outcomes.
Nurses will not feel psychologically safe to take risks if they do not learn from failures or receive moderate or low support from their nursing leaders. To overcome nurses’ inability to ask questions when they do not understand something and the non-welcoming behaviors of team members toward each other's ideas, organizations should establish boundaries and welcoming work environments, reduce retaliation, and promote help-seeking and feedback (Wang et al., 2018).
Supportive environments cultivated by moral leaders improve team performance and care outcomes. Therefore, new training programs should emphasize moral decision-making and ethical consistency to enhance psychological safety. Moreover, ensuring a critical assessment of whether current leadership training programs adequately address the complexities of moral decision-making in high-pressure clinical environments is essential.
Implications for Education
Today's students are tomorrow's nurses and must learn various moral leadership behaviors such as integrity, temperament, prudence, and courage. They must also learn how to promote safety, respect, and learning behaviors within the teams. The best way to do so is to learn from a role model who would teach them how to discuss difficult issues and raise concerns without retaliation or criticism.
Nursing leaders’ moral leadership was correlated with nurses’ and teams’ psychological safety. Their moral leadership and area of work also predicted nurses’ and teams’ psychological safety. Nursing teams had high psychological safety in terms of taking risks, but they needed to learn from failures, especially when nursing leaders provided support. Thus, although moral leaders may help create a nurturing environment, the sustainability of such environments requires institutional backing and continuous leader development.
Moral leaders may contribute to promoting moral-shared leadership, which, in turn, promotes team psychological safety through enhanced organizational learning. This moral-shared leadership could encourage taking risks, learning from failure, and requesting help when needed. As moral nursing leaders are linked to positive changes in the work environment, moral leadership development programs are recommended, necessitating further research with a larger random sample and various research designs across different settings, cultures, and countries.
Educational curricula should not only impart moral traits but also foster critical thinking about ethical dilemmas and systemic challenges nurses may face. Students should be taught moral leadership through role models who encourage open discussion and calculated risk-taking. Integrating moral leadership traits into curricula fosters future nurses’ ability to promote psychological safety.
Conclusions
Moral leadership contributes to psychologically safe environments by promoting openness, respect, and learning from failure. Thus, moral leaders help create a nurturing environment in which nurses feel appreciated and respected, engage in open communication and request support—especially when committing errors—and learn from failures by promoting a “just culture,” viewing mistakes as opportunities for growth.
Future research should explore cross-cultural applications of moral leadership and its impact on team dynamics and assess whether moral leadership alone ensures psychological safety or requires structural support.
Footnotes
Acknowledgments
The researchers acknowledge the input of all subjects who participated in the study. Thanks are also conveyed to Dr. Ahmad, K. Alomari, for his help in providing insights on reviewers’ comments, which helped in the critical revisions of these comments.
Ethics Approval and Consent to Participate
All needed approvals were obtained before data collection, including an IRB No. 11/8/2021/2022 from the Hashemite University dated August 1, 2022. In the invitation letter, nurses were informed that their participation was their consent to participate in the study.
Consent for Publication
This article includes data obtained from individual participants. Written informed consent for publication was obtained from all participants. All authors hereby give their consent for the publication of the article, including all associated data published by Sage Publications.
Author Contributions
MTM involved in conceptualization, abstract, methodology, investigation, data analysis and writing, limitations, original draft preparation, writing, review, editing, and supervision. AIA involved in writing, review, and editing of discussion and implications.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of Data and Materials
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Authorship Statement
The authors listed meet the authorship criteria according to the latest guidelines of the International Committee of Medical Journal Editors, and the authors agree with the manuscript. The authors have approved the content before submission or resubmission. The authors have no conflicts of interest and no funding source.
Declaration of Generative AI and AI-Assisted Technologies in the Writing Process
During the preparation of this work, the authors used Grammarly to edit the language. After using this tool, the authors reviewed and edited the content as needed and took full responsibility for the content of the publication.